
Abstract
Older adults with significant cognitive impairment require help with activities of daily living. The BASIC-Cognitive Project, set in Nueces County, Texas, is a community-based study examining trends in cognition among Mexican Americans and non-Hispanic Whites. Using cross-sectional data from a cohort study, we found that at least 7% of individuals aged 65 and older with a Montreal Cognitive Assessment (MoCA) score of < 20 (or < 15 for telephone MoCA), did not receive any caregiving help. This conservative estimate highlights an important community need for those with significant cognitive impairment and has implications regarding safety and care for older adults.
INTRODUCTION
People with dementia require help with activities of daily living. Alzheimer’s disease and other dementias affect 50 million people globally and 3.5 million people in the United States [1]. Little is known about the proportion of these individuals that have no one to help them as their cognitive impairment progresses. There are serious implications for safety and access to healthcare for people with severe cognitive impairment who are isolated. Lack of any caregiving may also lead to early institutionalization, resulting in an increase of societal healthcare costs. For providers, barriers to providing services to those with dementia include physician level confusion about who is to provide services, lack of a stable relationship between the caregiver-patient dyad and provider, time constraints, and poor communication [2]. Mexican Americans are more likely to have cognitive impairment and dementia, and they report financial resources as a higher priority than non-Hispanic Whites [3]. Subsequently, there could be greater unmet caregiving needs among Mexican Americans. There is also a demonstrated ethnic disparity in self-reported health-related quality of life for Latinx individuals above the age of 65 with probable dementia compared with non-Hispanic Whites [4].
The BASIC-Cognitive project is an ongoing, community-based cohort study of participants with cognitive impairment and dementia. In the current paper, we sought to make a conservative estimate of the number of people who have significant cognitive impairment and do not have anyone with normal cognitive function to help them with activities of daily living, as well as to examine the prevalence of substantial social isolation in this community. Social isolation may be a key component of cognitive impairment [5].
METHODS
We prospectively obtained cross sectional data from a cohort study. The BASIC-Cognitive methods were previously reported [6]. Briefly, households in Nueces County, Texas, were randomly identified from a two-stage area probability sample. Residents in the community aged 65 years and older were recruited using door-to-door case ascertainment from May 1, 2018–March 15, 2020, and through phone calls between April 20, 2020 and July 21, 2021 due to COVID-19 restrictions. To identify participants with dementia, age-eligible participants completed the Montreal Cognitive Assessment (MoCA). Based on previous studies, dementia was defined as a MoCA score of < 20 for the neighborhood sample, and < 15 for the telephone MoCA (tMoCA) [7]. Participants were asked to identify an informal caregiver for further involvement in the study through an iterative process. We asked people if they have a caregiver, and depending on their response, press further to determine if there was anybody who provided any level of care for them. We defined “informal caregiving” very broadly and conservatively; anyone who provides even minimal support to help the older adult with any activity that they were not able to complete on their own could be identified as a caregiver. This could include anyone from a neighbor who helps them take out their trash, to a relative who lives with them. To participate in the study, we require the caregiver to have a certain level of cognitive function and pass a screening test before enrollment. We assessed the cognitive function of the caregiver named by participants by administering a MiniCog (in person) or tMoCA short (phone) and determining if the score was greater than two or nine, respectively.
This study took place in Nueces County, Texas. The population estimate in 2020 was 340,233, with 14.9% of that population age 65 and older. Of the population aged 65 and older, 50.7% are of Hispanic/Latinx ethnicity, and 43.4% are non-Hispanic White. This county is predominantly urban with residents living in the city of Corpus Christi. Most of the Hispanic/Latinx population are non-immigrant US citizens of Mexican American heritage [8].
Eligible study participants from the BASIC-C door-to-door screening (MoCA < 20) and the telephone screening (tMoCA < 15) were pooled to form a single analysis data set. Univariate descriptive statistics were estimated and bivariate analyses were performed to investigate the rates of caregiving support and to study the association between caregiving support and the demographic characteristics of the study sample.
The study was approved by the University of Michigan IRB. De-identified data are available based on reasonable requests according to IRB regulations and informed consent. Interested parties should contact the corresponding author.
RESULTS
In the neighborhood random sample, 432 respondents (338 Mexican American, 67 non-Hispanic white, 15 Other, 12 Unknown) with MoCA scores of less than 20 were asked to identify a caregiver. In our sample, 18 respondents (4.2%) were unable to identify any caregiver. A caregiver who lived with the respondent but also had probable cognitive impairment was identified in an additional 14 (3.2%) respondents. In the telephone random sample, 129 respondents with tMoCA scores of less than 15 were asked to identify an informal caregiver. Seven respondents (5.4%) were unable to identify any caregiver. An additional three (2.3%) identified a caregiver who lived with them but also had probable cognitive impairment. Table 1 provides the demographics of the total sample. There was a combined total in both sampling procedures of 25 respondents (4.5%) who were unable to identify a caregiver, and 17 (3.0%) who only had a caregiver with probable cognitive impairment. In sum, 42 of 561 (7.5%) of participants with significant cognitive impairment did not have a cognitively normal person to help them with even minimal needs (Fig. 1). Participants with higher MoCA scores were less likely to have a caregiver than those with lower MoCA scores (Fig. 2).
Demographics
MA, Mexican American; MoCA, Montreal Cognitive Assessment; tMoCA, Telephone Montreal Cognitive Assessment; CI, confidence interval; SD, standard deviation; y, years. *Years of education was capped at 17 years. **The respondents who waived assent do not have a MoCA or tMoCA score. They were excluded from the distribution of MoCA score or tMoCA score reported in this table.
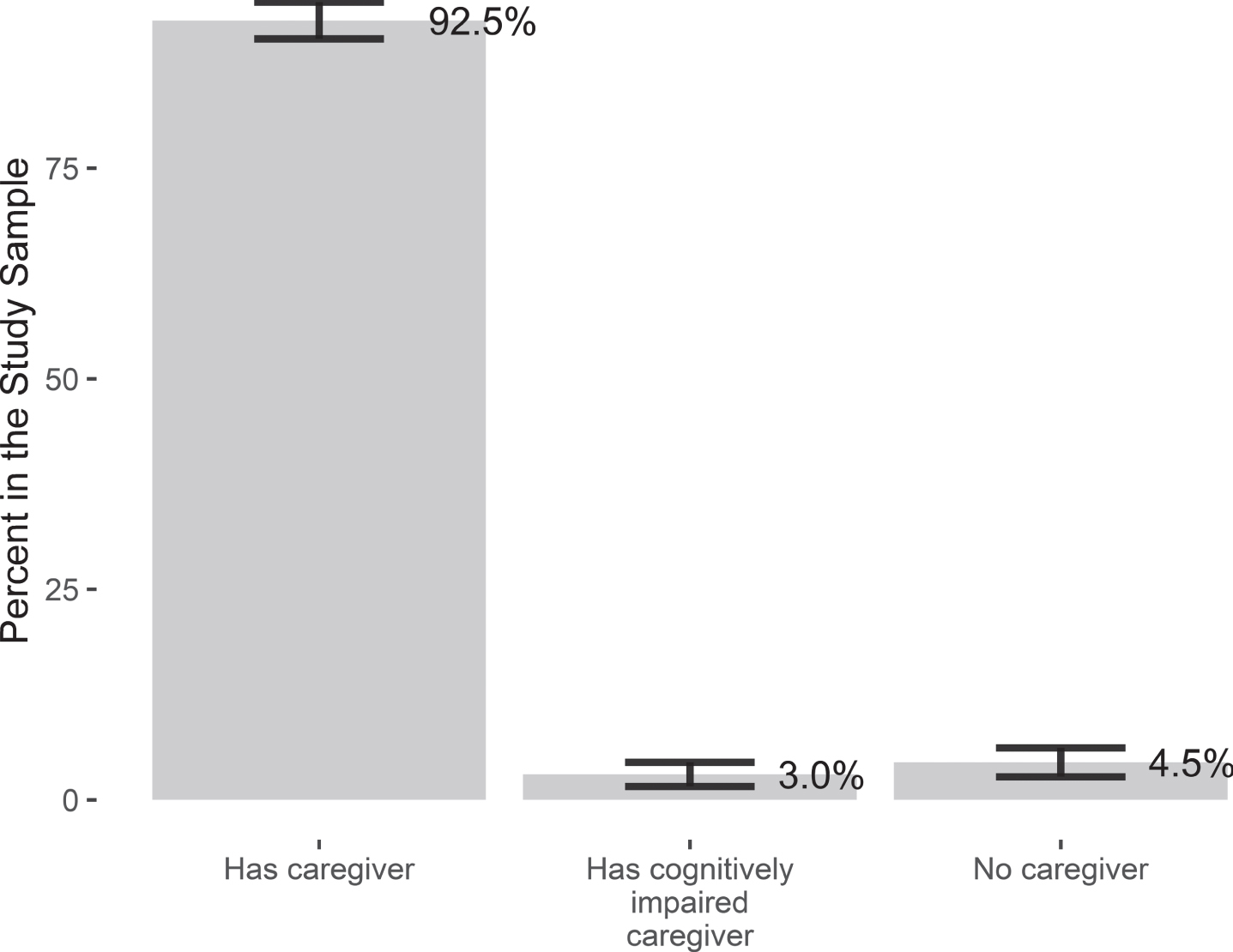
Percentage (and 95% confidence intervals) of sample with caregivers, no caregivers, or impaired caregivers.
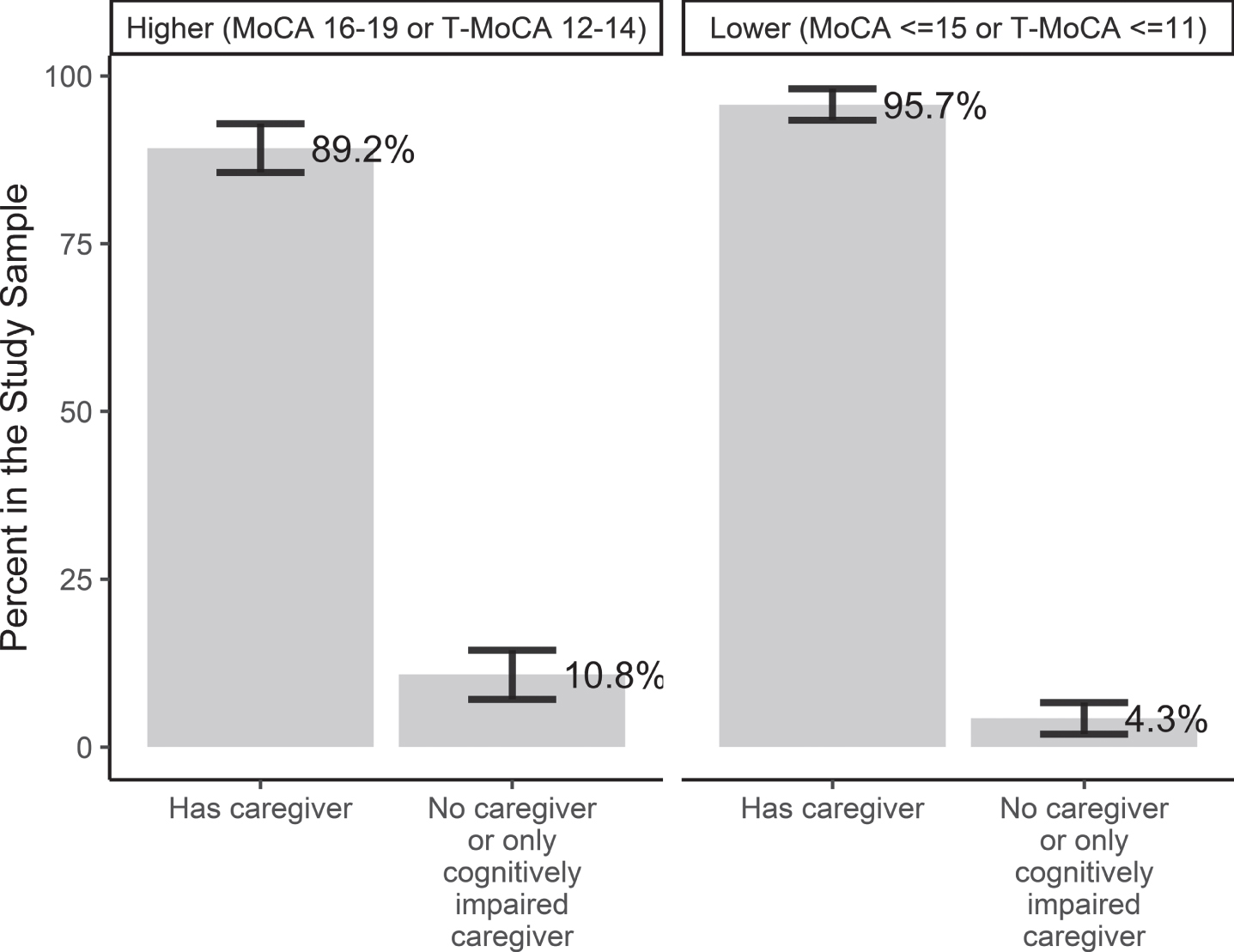
Percentage of sample (and 95% confidence intervals) with caregiver or no caregiver/impaired caregiver by participant MoCA/T-MoCA score.
DISCUSSION
This study found that 7.5% of participants with dementia could not call upon anyone with normal cognition to help them with the simplest tasks like rolling their garbage can to the curb once per week. This is a very conservative estimate of unmet needs; the true proportion of people with dementia who have no one to provide all their needs is likely much higher. The people who more commonly had informal care did have lower MoCA and tMoCA scores on average; however, both groups have median scores low enough to require caregiving help (Table 1). The literature demonstrates an association between dementia and social isolation, where social isolation is objectively defined as low contact with others in both quality and quantity [9]. This connection could be the result of a bidirectional causal link, with cognitive decline impeding one’s ability to maintain social connections, or, conversely, with a lack of close relationships further impairing one’s cognitive health. In either case, social isolation is closely linked to the manifestation of mental and physical health problems in aging populations. One meta-analysis found that social isolation among older adults was associated with a 29% increase in mortality, and that living alone corresponded to a 32% increase in mortality [10]. A prospective study conducted in Finland found that “loneliness” was a predictor of cognitive decline over a 10-year period among an older adult sample population [11]. Similar results are found worldwide, indicating a universal connection between aging, isolation, and cognitive decline. In a study conducted in South Korea, depression, loneliness, lack of a social-network, and difficulty completing daily activities were all risk factors for dementia [12]. In a cohort study conducted in Sweden, elderly adults living alone or without any close social relationships were demonstrated to be 1.5 times more likely to develop dementia over a 3-year period than those living with another person [13]. Further, a longitudinal study of older adults in Spain found that poor social engagement was significantly associated with cognitive decline and dementia even when controlling for other risk factors, including age, education, and baseline cognitive function [14].
As their cognitive function worsens, people with dementia are likely to become more reliant on caregivers for daily activities and decision-making. Examples of these may range from providing aid in health promoting behaviors such as physical exercise [15] to overseeing the transition to driving cessation. The absence of any person who can provide even a minimal level of care highlights these decisions as areas of concern. Those with dementia without caregiving support may be more likely to continue driving past when they can do so safely, may be vulnerable to household dangers such as engaging in potentially dangerous activities without supervision (e.g., use of stove, power tools) or falling [16, 17], may have poor medication compliance or misunderstand medication instructions [18, 19], and have a quicker timeline to institutionalization [20], which is expensive to both the individual as well as society. One study observed that living alone was a significant predictor of a shorter average time to institutionalization as compared to those that lived with someone else [20]. The yearly cost per person attributed to dementia in 2010 dollars was $33,329 ($41,700 today) for formal care (including out-of-pocket spending, Medicare spending, formal home care, and nursing home care) [21]. The value estimated for the replacement of informal caregiving with the cost of a home health agency is $30,839 ($38,600 today) [21]. We found that Mexican Americans were more likely to receive informal care than Non-Hispanic Whites (Table 1). Future analysis of ethnic differences could provide a comparison of unmet needs between Mexican Americans and non-Hispanic Whites and give insight into cultural differences in caregiving trends.
This study has limitations. Our findings are from one specific community and may not be the same in other locations. We used the MoCA to define dementia and used a cutpoint of < 20 and < 15 for tMoCA. While there is literature support of this [7], a more thorough cognitive assessment is needed to accurately define dementia. Since the COVID-19 pandemic, we switched from door-to-door recruitment to phone recruitment. In addition to the high concordance between in-person and telephone scores observed in the current study, the literature suggests that cognitive assessments by telephone can be successfully utilized when there are barriers to in-person evaluation [22]. At the initial recruitment phase, we did not gather information on living situation or marital status, so we do not know if those who had no caregiver may live with someone. However, due to our broad definition of care, we find it unlikely that someone could have no one to name if they lived with others. Out of the 25 participants who could not identify an informal caregiver, only one had a formal paid caregiver. There could also be hesitancy among older adults to disclose to the research team that they receive caregiving. A strength of this study, however, is that over 450 people have provided names of caregivers in our cohort. Our study is well-established in the community; therefore, the likelihood of potential hesitancy would have only a small effect on recruitment. This study also included a rigorous sampling methodology.
This study found that 7.5% of individuals in Nueces County with significant cognitive impairment do not obtain even minimal assistance with their daily needs, which raises important hypothesis-generating questions. Further study is required to determine whether there is an even larger gap between needs and services for people who have greater cognitive impairment and whether the absence of caregiving accelerates cognitive decline. More research can help determine whether policy development is necessary to try to close this gap, which could include the promotion of accessible transportation, at-home care services, and resources to facilitate social network support.