
Abstract
Background:
Physical activity has been associated with better cognitive function and better sleep quality. Yet, whether the beneficial effect of physical activity on cognitive function can be explained by an indirect pathway involving better sleep quality is unclear.
Objective:
To investigate whether sleep quality mediates the association between physical activity and cognitive function in adults 50 years of age or older.
Methods:
86,541 community-dwelling European adults were included in the study. Physical activity and sleep quality were self-reported. Indicators of cognitive function (immediate recall, delayed recall, verbal fluency) were assessed using objective tests. All measures were collected six times between 2004 and 2017. The mediation was tested using multilevel mediation analyses.
Results:
Results showed that self-reported physical activity was associated with better self-reported sleep quality, which was associated with better performance in all three indicators of cognitive function, demonstrating an indirect effect of physical activity on cognitive function through sleep quality. The mediating effect of sleep quality accounted for 0.41%, 1.46%, and 8.88% of the total association of physical activity with verbal fluency, immediate recall, and delayed recall, respectively.
Conclusion:
These findings suggest that self-reported sleep quality partly mediates the association between self-reported physical activity and cognitive function. These results need to be confirmed by device-based data of physical activity and sleep quality.
INTRODUCTION
Worldwide, 35.6 million people have dementia, with a new case every four seconds [1, 2] and a prevalence that doubles every five years [3]. Thus, promoting cognitive health in aging is a public health priority [1] and non-pharmacological lifestyle interventions play a central role in this promotion [2]. Specifically, adopting a physically active lifestyle is considered a protective factor against cognitive decline and dementia [4–9]. For example, randomized controlled trials have shown that fitness training improves cognitive function [10]. Prospective cohort studies have suggested that engaging in regular physical activity reduces the risk of dementia by 28% [11] and that meeting the recommended 150 min/week of moderate-to-vigorous physical activity could reduce up to 18% the prevalence of Alzheimer’s disease cases among older adults [8]. Moreover, a recent Mendelian randomization study drawing on large-scale genome-wide association studies revealed that moderate physical activity improves cognitive functioning [6]. Overall, these findings consistently demonstrate how essential physical activity is for maintaining cognitive function in later life.
Multiple mechanisms can explain the protective effect of physical activity on cognitive function [12]. For example, at the molecular and cellular level, it has been suggested that physical activity induces an increased availability of growth factors such as the brain-derived neurotrophic factor, insulin-like growth factor-1, and vascular endothelial growth factor, which have been associated with increased brain plasticity, synaptogenesis, and neurogenesis [13–16]. At the brain level, cross-sectional and experimental studies have shown that physical activity is associated with an increase in hippocampus [17, 18], prefrontal cortex [19], and caudate nucleus volume [20]. Further, better white matter integrity [21, 22] and functional connectivity [23–25] are thought to explain the positive effect of physical activity on cognitive function [21, 22]. However, less is known about the behavioral factors that may underlie the relationship between physical activity and cognitive function.
An indirect pathway through sleep quality is a potential candidate mechanism. For example, previous studies showed that greater engagement in physical activity can improve sleep quality [24, 26–31]. In turn, better sleep quality can promote cognitive health [32–35]. Moreover, the deterioration in sleep quality often observed in older adults [36–38] could contribute to age-related cognitive decline [32, 39–41]. However, at the time of writing, only few cross-sectional studies have tested the potential mediating role of sleep quality on the association between physical activity and cognitive function [40, 43]. Some studies showed that sleep quality [43], sleep efficiency [42], and total sleep time [44] mediated the association between physical activity and executive functions. Other studies showed no evidence of a mediation by sleep quality [40, 45]. In sum, current evidence for the potential mediating role of sleep on the relationship between physical activity and cognitive function in later life fully relies on cross-sectional studies and is inconclusive. Studies using experimental designs did not conduct mediation analyses to examine the relationship between exercise, sleep, and cognition, and there is no longitudinal study testing this relationship [41].
To address this gap, the objective of this large-scale longitudinal study was to examine the associations between some indicators of physical activity, sleep quality, and cognitive function in adults 50 years of age or older. Based on the literature [42, 43], we hypothesized that sleep quality partly mediates the relationship between physical activity and cognitive function.
METHODS
Study design
Data were drawn from the Survey of Health, Ageing and Retirement in Europe (SHARE), a longitudinal population-based study on adults 50 years of age or older living in 27 European countries and Israel [46]. Data were collected every two years between 2004 and 2017 for a total of 7 measurement waves using computer-assisted personal interviewing (CAPI) in participants’ homes. Physical activity, sleep quality, and cognitive function (immediate recall, delayed recall, and verbal fluency) were assessed at all measurement waves except wave 3 (2008-2009). Physical activity and sleep quality were self-reported, whereas cognitive function was assessed using objective tests. SHARE was carried out in accordance with the Declaration of Helsinki and has been approved by the Ethics Committee of the University of Mannheim (waves 1–4) and the Ethics Council of the Max Plank Society (waves 4–7). All participants provided a written informed consent. To be included in the present study, participants had to be 50 years or older and have at least one measure of physical activity, sleep quality, and cognitive function. To reduce reverse causation bias, we excluded individuals with suspected dementia at baseline, as indicated by a score above two on the time orientation question [47], and people who reported more than two limitations in activities of daily living (ADL) at baseline.
Measures
Outcome: Cognitive function
Cognitive function was assessed at wave 1, 2, 4, 5, 6, and 7 using validated tests of verbal fluency, immediate recall, and delayed recall. The semantic verbal fluency test implemented in SHARE [48] was used to assess executive functioning [49] and cognitive impairment [50]. However, verbal fluency is also associated with verbal skills and may not solely reflect executive functioning [51]. In the verbal fluency test [50], trained interviewers asked participants to name as many different animals as they could think of in one minute. The score was the total number of correctly named animals, with a higher score indicating better performance. In addition, memory abilities [49] were derived from immediate and delayed recall performance in a 10-word delayed-recall test [52] adapted from the Telephone interview of Cognitive Status-Modified (TICS-M) [53]. In the immediate-recall test, participants listened to a 10-word list that was read out aloud by the interviewer. Immediately after reading the list, participants were asked to recall as many words as possible. At the end of the cognitive testing session, participants were asked to recall the words from the list again, which captured delayed recall [54], an indicator of cognitive impairment and dementia [52]. Both recall scores ranged from 0 to 10 with a higher score indicating better performance. All these cognitive tests have been widely used to measure cognitive function in later life [47, 55–58].
Independent variable: Self-reported physical activity
Self-reported physical activity, assessed using CAPI at wave 1, 2, 4, 5, 6, and 7, was derived from two questions: “How often do you engage in vigorous physical activity, such as sports, heavy housework, or a job that involves physical labor?” and “How often do you engage in activities that require a low or moderate level of energy such as gardening, cleaning the car, or doing a walk?” [59–61]. Participants answered using a four-point scale: 1 = Hardly ever, or never; 2 = One to three times a month; 3 = Once a week; 4 = More than once a week. Participants who did not answer “more than once a week” to either item were classified as physically inactive. As described in previous research [62–64], this strategy reduces the potential misclassification bias that could lead to physically inactive participants being incorrectly classified as physically active.
Mediating variable: Self-reported sleep quality
Self-reported sleep quality, assessed using CAPI at wave 1, 2, 4, 5, 6, and 7, was derived from the question: “Have you had trouble sleeping recently?” Participants who answered “Trouble with sleep or recent change in pattern” were classified as having poor sleep quality, whereas participants who answered “No trouble sleeping” were classified as having good sleep quality [65, 66].
Covariates and potential confounders
The following covariates were included in the analysis: measurement wave (1 to 7), age group (50–64, 65–79, 80–96 years), sex (male, female), body mass index (underweight: < 18.5, normal: ≥18 and < 25, overweight: ≥25 and < 30, obese: ≥30 kg/m2), education (7 categories based on the International Standard Classification of Education) [67], ability to make ends meet (with great difficulty, with some difficulty, fairly easily, easily), birth cohort [war (1914–1918, 1939–1945), great depression (1929–1938), no war nor economic crisis (before 1913, 1919–1928, after 1945)], country of residence (Austria, Belgium, Croatia, Czech Republic, Denmark, Estonia, France, Germany, Greece, Hungary, Ireland, Israel, Italy, Luxembourg, Netherlands, Poland, Portugal, Slovenia, Spain, Sweden, Switzerland), attrition [no dropout, dropout (participants who responded to neither wave 6 nor wave 7), death (participants who died during the follow-up)], partnership status (alone, in couple), and number of chronic diseases. These variables were adjusted for in the models because they have been identified as potentially confounding factors in the associations between physical activity, sleep quality, and cognitive function.
Statistical analyses
Data were analyzed using linear and logistic mixed-effects models that account for the nested structure of the data (i.e., repeated measurement over time within a single participant) and provide acceptable Type I error rates [68]. Participants with missing observations were included as mixed-effects models do not require an equal number of observations from all participants [69]. Specifically, to investigate the mediating role of sleep quality on the relationship between physical activity and cognitive function, we used two complementary approaches. First, we conducted the distribution-of-the-product coefficients approach using the RMediation package [70], which produces confidence intervals around the indirect effects. Second, as recommended [71], we used the component approach, which tests individual model parameters to confirm the significance of the indirect effects [72]. The component approach operates by demonstrating that the two components of the indirect effect (i.e., from the independent variable to the mediator [the first component] and from the mediator to the outcome [the second component]) are both significant (Fig. 1). This test, referred to as the joint-significant test [73] or the causal steps test [74], has proven to perform better in terms of Type I error rates than other tests, such as bootstrap-based methods [72].
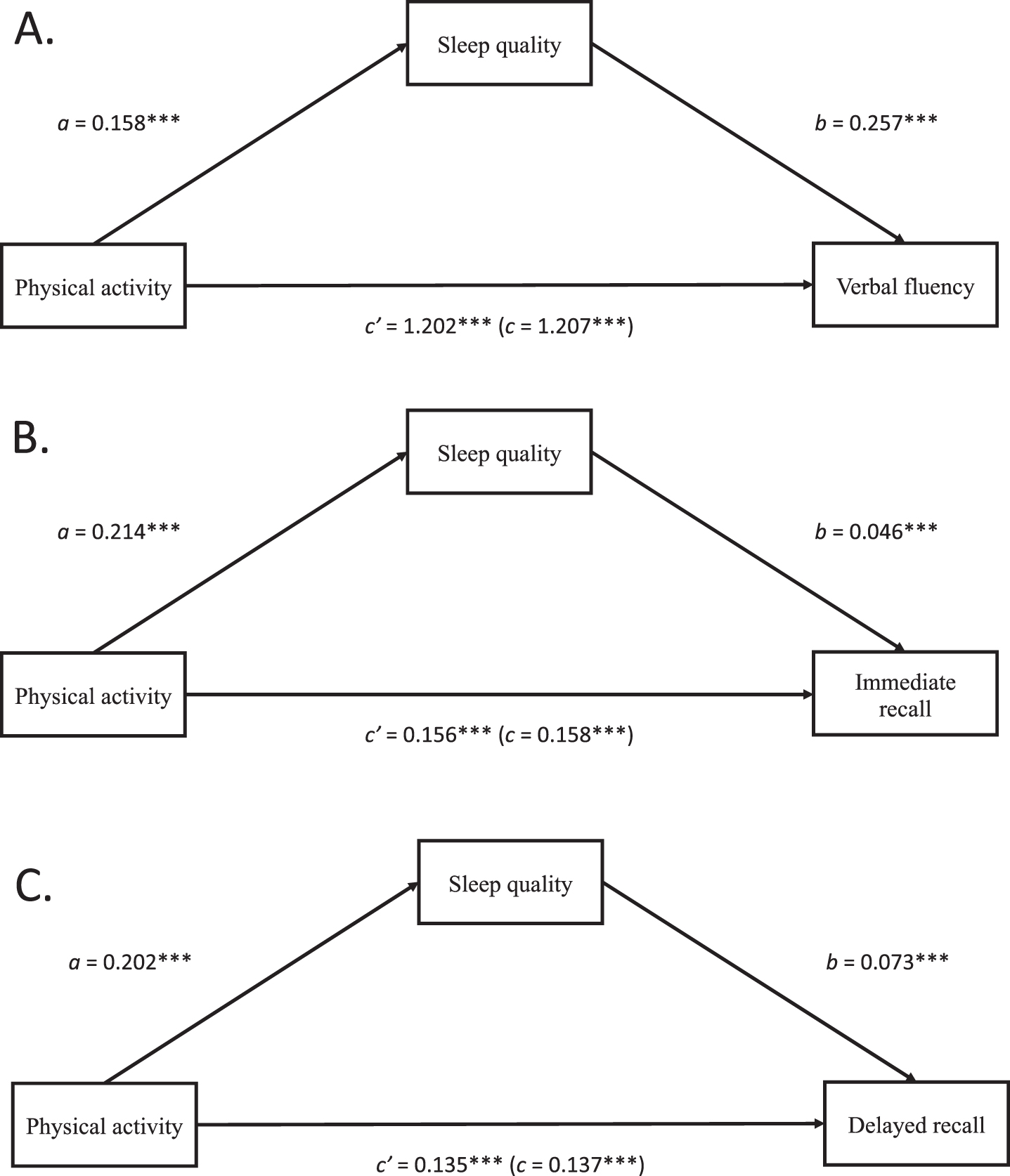
Mediation models. Coefficients are unstandardized regression coefficients obtained from the mixed-effects models. a represents the association between the exposure (i.e., physical activity) and the mediator (i.e., sleep quality). b represents the association between the mediator (i.e., sleep quality) and the outcome (i.e., cognitive function), c’ represents the direct effect of the exposure on the outcome, after adjustment for the mediator. The unstandardized regression coefficient representing the total association (c) between physical activity and cognitive function is in parentheses. ***p < 0.001. A) Results of the models for verbal fluency. B) Results of the models for immediate recall. C) Results of the models for delayed recall.
For each of the three cognitive outcomes, two mixed-effects models were computed to test the mediating role of sleep quality on the associations between physical activity and cognitive function. Model 1 tested the association between physical activity (i.e., exposure) and sleep quality (i.e., mediator) and was adjusted for the covariates. Model 2 tested the association between sleep quality (i.e., mediator) and cognitive function (i.e., outcome), adjusted for physical activity (i.e., the exposure) and the covariates. In the distribution-of-the-product method of the Rmediation package, an indirect effect is established when the confidence intervals around the indirect effects obtained from Model 1 and Model 2 do not cross zero. In the component approach, an indirect effect is established if both the association between physical activity and sleep quality (i.e., first component, Model 1) and the association between sleep quality and cognitive function (i.e., second component, Model 2) are significant. The total effect is estimated by summing the indirect effect and the direct effect. Finally, the proportion of the total effect explained by the mediator was calculated as follows: (total effect – direct effect)/total effect. Estimates of the effect size for fixed effects were reported using the marginal and conditional pseudo-R2 computed with the MuMin R package [75].
Sensitivity analyses
Five sensitivity analyses were conducted. The first sensitivity analysis relied on a sample of participants with at least two self-reported measures of physical activity, two self-reported measures of sleep quality, and two measures of a given cognitive function. The second sensitivity analysis excluded participants who reported poor sleep quality at baseline. The third sensitivity analysis excluded participants who dropped out during the survey (i.e., participants who responded to neither wave 6 nor wave 7). The fourth sensitivity analysis excluded participants who died during the survey. The latter two sensitivity analyses tested whether attrition due to dropouts and deaths affected the results. The fifth sensitivity analysis adjusted for the level of depressive symptoms at baseline because higher level of depressive symptoms may reduce the energy and motivation to be physically active and may affect the relationships between physical activity, sleep quality, and cognitive function.
Robustness analyses
We performed a robustness analysis in which a time lag was created between the predictors (i.e., physical activity and sleep quality) and the outcome (i.e., cognitive function). Specifically, for a given wave (except for wave 1) the predictors were assigned the value of the preceding wave [76]. This approach aimed to minimize the impact of reverse causation bias on the observed associations.
RESULTS
The study sample included 86,541 individuals (46,480 women). Table 1 summarizes the characteristics of the participants stratified by self-reported physical activity status at baseline. Simple association tests indicated that physically active (versus physically inactive) participants showed better cognitive function (i.e., on all three indicators), better self-reported sleep quality, higher education, higher ability to make ends meet, and were less likely to be a woman, to be older, to have a chronic condition, and to be obese. Moreover, performance on the three cognitive tasks were significantly correlated with each other (verbal fluency – delayed recall, r = 0.47; verbal fluency – immediate recall, r = 0.49; immediate recall – delayed recall, r = 0.71; ps < 0.001).
Baseline characteristics of the participants by physical activity status
Baseline, the first measurement occasion for each participant; SD, standard deviation; p values are based on the analysis of variance and chi-square tests for continuous and categorical variables, respectively, testing the effect of physical activity status at baseline (physically active versus physically inactive) on these variables. The descriptive statistics are based on the larger sample size (i.e., 86,541 from the models testing verbal fluency).
Results of the mixed-effects models
CI, confidence interval at 95%; OR, odds ratio. Results are derived from mixed effects models. Results of the Model 1 are derived from logistic mixed-effects models, while results of the Model 2 are derived from linear mixed-effects models. Models are adjusted for wave of measurement, age, sex, birth cohort, body mass index, education, ability to make ends meet (satisfaction with household income), attrition, country of residence, and number of chronic diseases.
Verbal fluency
Results of the mediation analysis based on the distribution-of-the-product approach showed a significant indirect effect of physical activity on verbal fluency through sleep quality (b = 0.054, 95% confidence interval [95% CI] = 0.039–0.068). Results of the mediation analysis based on the component approach showed that physically active individuals had better sleep quality than physically inactive individuals (b = 0.16, odds ratio [OR] = 1.17, 95% CI = 1.14–1.21, p < 0.001) (Model 1). In Model 2, results showed that better sleep quality was associated with better verbal fluency (b = 0.26, 95% CI = 0.17–0.28, p < 0.001). Since the two components of the mediation were significant, these results were consistent with the results of the mediation analysis based on the distribution-of-the-product method and further supported a significant indirect effect of physical activity on verbal fluency through sleep quality. After adjusting for sleep quality (Model 2), results showed the association between physical activity and verbal fluency remained significant (b = 1.20, 95% CI = 1.14–1.26, p < 0.001), suggesting that the effect of physical activity on verbal fluency was not fully mediated by sleep quality. The proportion of the total effect that was mediated by sleep quality was 0.41%. The model explained 28.3% of the marginal variance and 60.1% of the conditional variance in verbal fluency.
Immediate recall
Results of the mediation analysis based on the distribution-of-the-product approach showed a significant indirect effect of physical activity on immediate recall through sleep quality (b = 0.010, 95% CI = 0.007–0.012, p < 0.001). Results of the mediation analysis based on the component approach showed that physically active individuals had better sleep quality than physically inactive individuals (b = 0.21, OR = 1.24, 95% CI = 1.20–1.28, p < 0.001) (Model 1). In Model 2, results showed that better sleep quality was associated with better immediate recall (b = 0.05, 95% CI = 0.04–0.06, p < 0.001). Since the two components of the mediation pattern were significant, these results were consistent with the results of the mediation analysis based on the distribution-of-the-product method and further supported a significant indirect effect of physical activity on immediate recall through sleep quality. After adjusting for sleep quality (Model 2), results showed that the association between physical activity and immediate recall remained significant (b = 0.14, 95% CI = 0.12–0.15, p < 0.001), suggesting that the effect of physical activity on immediate recall was not fully mediated by sleep quality. The proportion of the total effect that was mediated by sleep quality was 8.9%. The model explained 25.5% of the marginal variance and 50.4% of the conditional variance in immediate recall.
Delayed recall
Results of the mediation analysis based on the distribution-of-the-product approach showed a significant indirect effect of physical activity on delayed recall through sleep quality (b = 0.015, 95% CI = 0.011–0.018, p < 0.001). Results of the mediation analysis based on the component approach showed that physically active individuals had better sleep quality than physically inactive individuals (b = 0.20, OR = 1.22, 95% CI = 1.18–1.27, p < 0.001) (Model 1). In Model 2, results showed that better sleep quality was associated with better delayed recall (b = 0.07, 95% CI = 0.06–0.08, p < 0.001). Since the two components of the mediation pattern were significant, these results were consistent with the results of the mediation analysis (distribution-of-the-product method) and further supported a significant indirect effect of physical activity on delayed recall through sleep quality. After adjusting for sleep quality (i.e., Model 2), results showed that the association between physical activity and delayed recall remained significant (b = 0.14, 95% CI = 0.12–0.15, p < 0.001), suggesting that the effect of physical activity on delayed recall was not fully mediated by sleep quality. The proportion of the total effect that was mediated by sleep quality was 1.5%. The model explained 23.5% of the marginal variance and 51.1% of the conditional variance in delayed recall.
Sensitivity and robustness
The sensitivity (Supplementary Tables 1–5) and robustness analyses (Supplementary Table 6) yielded similar results as the main analyses. Specifically, physically active individuals self-reported a better sleep quality than physically inactive individuals, and better sleep quality was associated with better performance on all three measures of cognitive function. This effect was also observed in participants with a least two measurements, regardless the type of tested attrition, and after adjustment for depressive symptoms at baseline. Moreover, physical activity and sleep quality were independently associated with all three measures of cognitive function, which suggested the association between physical activity and cognitive function was not fully mediated by sleep quality. Results of the robustness analysis showed the same partial indirect effect, although the magnitude of the associations of physical activity and sleep quality with cognitive function were smaller.
DISCUSSION
Our results showed that physical activity was positively associated with sleep quality and that sleep quality was positively associated with cognitive function, indicating a significant indirect effect of physical activity on cognitive function through sleep quality. Moreover, the proportion of the indirect effects was 0.41%, 1.46%, and 8.88% for verbal fluency, immediate recall, and delayed recall, respectively. Physical activity remained significantly associated with all three domains of cognition after adjustment for sleep quality. Hence, our study lends support for a partial mediating role of sleep quality on the relationship between physical activity and cognitive function, although additional studies using more objective measures of physical activity and sleep parameters are needed to confirm our findings.
Comparison with other studies
Our results showed an association between physical activity and sleep quality that is consistent with earlier evidence indicating that physical activity improves sleep quality [24, 26–31]. To explain this association, at least three complementary explanations have been proposed [27, 77]. First, a higher level of physical activity may improve affective states and mental health [63, 79]. Second, physically active individuals may have a better weight management than inactive individual [80–82]. Third, physically active individuals may exhibit better physical function [83]. All these factors could contribute to sleep quality [84–88]. Consequently, the conjunction of these three explanations can lead to better sleep quality in physically active than physical inactive individuals.
Our results also aligned with the mounting evidence showing that better sleep quality is associated with better cognitive function [42, 89–91]. Specifically, we observed that poor sleep quality was significantly associated with lower cognitive performance, thereby confirming the robustness of this association. Several biological mechanisms have been proposed to account for the link between sleep and cognitive function [32]. Specifically, studies suggested that sleep disturbance may favor cognitive impairment through increased amyloid-β concentrations [92], neurodegeneration [93, 94], or the alteration of specific neurotransmitter systems [95]. In sum, our findings confirm that sleep quality could contribute to maintaining cognitive health across aging. Nonetheless, it should be noted that the sizes of the observed associations in our study were small. For example, compared with participants who reported sleep problems, participants without sleep problems named on average 0.25 more words for verbal fluency, 0.10 for immediate recall, and 0.05 for delayed recall. The significance of the observed effects should thus be interpreted in the context of the large-scale dataset.
These two previous results (i.e., significant links between physical activity and sleep quality, and between sleep quality and cognitive function) may suggest that physical activity has an indirect effect on cognitive function through the mediating role of sleep quality. The mediating effect of sleep quality was 0.41%, 1.46%, and 8.88% of the total association of physical activity with verbal fluency, immediate recall, and delayed recall, respectively. Furthermore, after adjustment for sleep quality, physical activity was still significantly associated with cognitive function. This result is consistent with the literature suggesting that the protective effect of physical activity on cognitive health in later life is also largely independent from sleep quality [4–9]. Therefore, other mediators could be considered such as mood, anxiety, body composition, cardiorespiratory system, gut microbiome, or social support. In other words, sleep quality mediates the association between physical activity and cognitive function in later life, but additional mechanisms need to be also considered.
Strengths and weaknesses
Among the strengths of the present study are the large sample size of community-dwelling middle-aged and older individuals living in 21 European countries, the reliance of a statistical approach suited to formally test mediation, and the use of three indicators of cognitive function providing consistent results. Moreover, the results remain similar across the sensitivity and robustness analyses. However, our findings need to be considered in light of the following features that limit the conclusions that can be drawn from our study. First, physical activity was assessed using a self-reported questionnaire, which may have reduced measurement validity and produced issues in the classification of active versus inactive individuals [96]. In addition, the questionnaire measured the frequency with which individuals usually engaged in physical activity in their daily-life, which lacks granularity. Future studies should include more objective measures such as accelerometer-based levels of physical activity. Second, sleep quality was assessed using a single self-reported item, which did not allow to examine whether different aspects of sleep (e.g., timing, quality, and duration) may have a specific influence on cognitive function. Moreover, this single item included the notion of “recent change in pattern”, which may have misled some participants, such as those who had a sleep disorder for several years. Yet, the sensitivity analysis excluding participants with poor sleep quality at baseline provided consistent results with those of the main analysis. Although the psychometrics of a single-item sleep-quality scale were reported to be good [97], future studies using more comprehensive questionnaires combined with a device-based measure of sleep are needed to replicate the current findings. Third, the fact that sleep quality and physical activity were self-reported may have introduced a shared method variance bias, which may have inflated the observed association between the exposure and the mediator. However, this bias unlikely explains the overall mediating pattern given that our cognitive measures (i.e., outcomes) are based on validated tests, not on questionnaires. Fourth, general cognitive function is thought to be underpinned by many cognitive domains, including but not limited to spatial ability, memory, processing speed, and reasoning [98, 99]. However, the current study is based on two measures that primarily reflect memory performance (i.e., immediate and delayed recall) [49], and one measure thought to mainly capture executive functions [100]. Since the effect of physical activity and sleep quality on cognitive function is likely dependent on the cognitive domain, future studies should include a wider range of cognitive domains. Fifth, we did not examine whether and how the country of residence moderate the observed effects. For example, the characteristics of the overall mediation mechanism may differ depending on the country characteristics, such as its welfare regime (i.e., Scandinavian, Bismarckian, Southern European, and Eastern European) or social protection expenditure [101–103]. Future studies could examine whether the relationships between physical activity, sleep, and cognitive function differ across countries. Finally, our analyses are based on correlational data. Therefore, we cannot exclude reverse causality and thus cannot infer a causal relationship between our variables. For example, better sleep quality can favor engagement in physical activity, which in turn may improve cognitive function [104, 105]. Similarly, higher levels of cognitive function can increase the engagement in physical activity [59, 106–108]. This finding can be explained by recent theoretical and empirical studies associated with the theory of effort minimization [109–114]. Specifically, this theory claims that cognitive function plays a key in role in counteracting their automatic attraction to effort minimization. Altogether, bidirectional relationships between physical activity, sleep quality, and cognitive function are likely and should therefore be explicitly examined in future randomized controlled trials.
Conclusion
This study highlights that the protective effect of physical activity on cognitive function in middle-age and older adults may be partly explained by sleep quality. Specifically, physically active individuals had better self-reported sleep quality than physically inactive individuals, which was partly explained by an indirect pathway through cognitive function. However, less than 10% of the total effect of self-reported physical activity on cognitive function was explained by sleep quality, thereby suggesting that physical activity also has an independent effect on cognitive function. These findings need to be confirmed using device-based measure of physical activity and actigraphy-based measurement of sleep parameters (e.g., sleep onset latency, sleep duration, sleep efficiency). Our results suggest that public health policies and clinicians should continue to promote physical activity and good sleep quality to delay cognitive decline.
DATA SHARING
The SHARE dataset is available at http://www.share-project.org/data-access.html
Footnotes
ACKNOWLEDGMENTS
This paper uses data from SHARE Waves 1, 2, 3 (SHARELIFE), 4, 5, 6, and 7 (DOIs: 10.6103/SHARE.w1.600, 10.6103/SHARE.w2.600, 10.6103/SHARE.w3.600, 10.6103/SHARE.w4.600, 10.6103/SHARE.w5.600, 10.6103/SHARE.w6.600, 10.6103/SHARE.w7.711). The SHARE data collection was primarily funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812) and FP7 (SHARE-PREP: no.211909, SHARE-LEAP: no.227822, SHARE M4: no.261982). Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see ![]() ).
).
B.C. is supported by an Ambizione grant (PZ00P1_180040) from the Swiss National Science Foundation (SNSF). M.P.B. is supported by the Natural Sciences and Engineering Research Council of Canada (RGPIN-2021-03153) and the Banting Research Foundation.