
Abstract
Background:
White matter hyperintensities (WMH) are a known risk factor for cognitive decline. While the ɛ4 allele of apolipoprotein E gene (APOE4) is another risk factor for cognitive decline, it remains unclear how APOE4 affects the relationship between WMH and cognitive decline, specifically in the prodromal stage of dementia.
Objective:
To determine how APOE4 moderates the relationship between WMH and cognition in prodromal dementia.
Methods:
Two-hundred-sixteen participants with prodromal dementia underwent magnetic resonance imaging (MRI), neuropsychological testing (global and domain wise), cardiovascular risk factor assessments, and APOE genotyping. Visual ratings for WMH as well as total and lobar WMH volumes were quantified. Moderation analysis was performed to determine the influence of APOE4 on the relationship between WMH and performance on global and domain-specific cognitive measures. The role of confluent and non-confluent WMH on cognition was additionally studied using logistic regression.
Results:
APOE4 carriers (n = 49) had poorer memory and higher global WMH (10.01 mL versus 6.23 mL, p = 0.04), temporal WMH (1.17 mL versus 0.58 mL, p = 0.01), and occipital WMH (0.38mL versus 0.22 mL, p = 0.02) compared to APOE4 non-carriers (n = 167). Moderation analysis revealed that APOE4 positivity strengthened the relationship between higher global as well as lobar WMH burden and poorer episodic memory. Furthermore, APOE4 carriers with confluent WMH were 4.81 times more likely to have impaired episodic memory compared to non-confluent WMH and non-APOE carriers.
Conclusion:
The impact of WMH on memory may be strongest among APOE4 carriers. Clinicians targeting WMH would need to consider the APOE4 allele and WMH severity status to strategize cognitive interventions.
INTRODUCTION
White matter hyperintensities (WMH) have been demonstrated to be a reliable surrogate measure for cerebral small vessel disease on T2-weighted FLAIR magnetic resonance imaging (MRI) [1]. WMH are a significant risk for cognitive impairment and Alzheimer’s disease (AD) [2–4]; however, the specific relationship between the severity of WMH and impairment in cognitive measures require further clarification [5]. A number of studies suggest association between WMH and cognition in mid to later stages of dementia [4, 6]. However, for prodromal dementia and early stages of dementia, there still remains a knowledge gap due to conflicting findings on WMH versus cognition relationship [6]. Given that, a quarter of the general elderly population may display moderate to severe WMH, the factors that influence the impact of WMH on cognition would have high clinical relevance [7]. It is known that a wide range of factors moderate the effect of WMH on cognitive outcomes, including aging, cardiovascular disease risk factors (CVRF), as well as the upstream pathways that result in WMH, which include cerebral small vessel disease, cerebral amyloid angiopathy, genetic vulnerability to neurodegeneration, or a combination of these [4, 9]. In addition to volumes of WMH, studies have demonstrated that type of WMH lesion (confluent versus non-confluent) may also have different impact on clinical outcomes [10, 11]. Confluent WMH has been demonstrated to result in significant functional connectivity changes as well as increase the risk of progression from MCI to dementia [10, 11].
One of the strongest known genetic risk factor for sporadic AD and vascular dysfunction is the apolipoprotein ɛ4 allele (APOE4) [8, 13]. The APOE4 allele has been associated with cognitive decline via pathways that include the amyloid cascade as well as vascular mechanisms [9, 12]. Importantly, in participants with high WMH burden, the APOE4 has been associated with increased risk of domain-specific cognitive decline in episodic memory and executive function in AD and Lewy body dementia [13]. However, it remains unclear how APOE4 affects the relationship between WMH and cognition at the early or prodromal stage of dementia. To our knowledge, previous studies investigating this relationship have not examined the effects of region-specific WMH burden on domain-specific cognitive performance. Hence, we sought to investigate whether APOE4 moderates the association between region-specific WMH and cognition in prodromal dementia. We hypothesized that higher WMH burden would be more strongly associated with poorer cognitive performance in domains of episodic memory and executive function in APOE4 carriers than non-carriers as the neurodegeneration in the frontal and temporal brain regions in AD is known to affect these domains [14–16].
MATERIALS AND METHODS
Participants
The study included 216 participants with subjective cognitive impairment (SCI, n = 78) and mild cognitive impairment (MCI, n = 138) recruited between August 2013 and January 2018 at National Neuroscience Institute, Singapore. Participants with SCI reported subjective symptoms, did not have objective deficits on cognitive evaluation and had a Clinical Dementia rating (CDR) score of 0 [17]. A diagnosis of MCI was based on the National Institute on Aging-Alzheimer’s Association (NIA-AA) and Petersen criteria [18, 19]. Participants with MCI had cognitive symptoms, objective deficits on cognitive evaluation, and a CDR of 0.5. For both SCI and MCI, we excluded participants where the cognitive symptoms may be best explained by other conditions such as depression, sleep impairment, or medication use. The data collected included the MRI, neuropsychological testing (global and domain wise), cardiovascular risk factor assessments, and APOE genotyping. The study inclusion criteria included presence of WMH, either punctate or confluent lesions on the T2-weighted fluid-attenuated inversion recovery (FLAIR) MRI sequence and APOE genotyping. The presence of ɛ4 allele, either homozygotes or heterozygotes, was used to stratify participants into APOE4 carrier (including 15 SCI and 34 MCI) and non-carrier (including 63 SCI and 104 MCI) groups. The number of SCI and MCI participants in the APOE group composition were matched for their cognitive status (χ2 p = 0.36). The SingHealth Centralized Review Board approved this study. Informed consent was obtained according to the Declaration of Helsinki from participants or their next of kin if they were incapable of giving consent, as deemed appropriate by the clinician.
Neuropsychological assessments
All the neuropsychiatric tests were administered and rated by trained psychologists at baseline. The neuropsychological battery included tests of global cognition, attention, executive function, memory, and language. Global cognition was assessed on the Montreal Cognitive Assessment (MoCA) [20]; executive function was assessed on the Frontal Assessment Battery (FAB) and Color Trails 2 [21, 22]; attention was assessed with Wechsler Adult Intelligence Scale version 4 using Digit Span Forward, Digit Span Backward and color trails 1 [22, 23]; episodic memory was assessed on Wechsler Memory Scale version immediate and delayed Story Recall and Alzheimer’s Disease Assessment Scale Cognitive Subscale (ADAS-Cog) immediate and delayed recall tests [24, 25]; and language was assessed using Boston naming test [26], and subcomponents of MoCA and FAB animal fluency task.
MRI protocols
The T1-weighted magnetization-prepared rapid gradient-echo (MPRAGE) and T2-weighted FLAIR MRI sequences were acquired on a 3T Tim Trio system (Siemens Erlangen, Germany) scanner. The T1 structural MRI sequence was acquired with repetition time of 2300 ms, echo time 2.28 ms, inversion time 900 ms, flip angle 8, 1 mm slice thickness, 192 number of slices, and 1×1×1 mm voxel size. The FLAIR MRI sequence was acquired with repetition time of 5000 ms, echo time 387 ms, inversion time 1800 ms, flip angle 120, 1 mm slice thickness, 192 slices, 1×1×1 mm voxel size.
Quantification of grey matter and WMH volumes
We used the Computational Anatomy Toolbox (http://dbm.neuro.uni-jena.de/cat12/), an statistical parametric mapping (SPM12 version 7487) based tool [27], to process the T1 images and extract total intracranial volume (TIV) and grey matter (GM) volumes. Default Cat12 segmentation routine was applied in the expert mode to control for WMH lesions being misclassified as GM tissue during T1-segmentation routine. We used Lesion Segmentation Toolbox (LST version 2.0.15) to quantify WMH volume based on previously published routine [10, 28]. Briefly, we employed the automated lesion growth algorithm from LST on T1 anatomical and FLAIR images to quantify binary WMH lesion belief maps at 0.10 kappa threshold (κ-0.10). Finally, the total and global tissue volumes were computed using cat12 estimation routine. To compute the total and regional WMH volumes in MNI space, we created lobar brain masks for frontal, parietal, occipital, and temporal regions in MNI space and subsequently applied SPM routines to extract total and lobar WMH volumes.
MRI visual ratings
MRI markers of cerebrovascular disease including WMH subtypes (confluent versus non-confluent), lacunes and enlarged perivascular spaces (EPVS) were also visually rated to incorporate these measures in statistical analysis. The WMH ratings were based on the modified Fazekas scale [29], where periventricular WMH and deep subcortical WMH were separately rated on a 0–3-point scale for both hemispheres. Participants were then classified as having confluent WMH and non-confluent WMH based on the Staals criteria: Participants with Fazekas WMH rating of 3 in either periventricular and/or a rating of 2 or 3 in deep white matter regions on either hemisphere were assigned to the confluent WMH group and the rest to the non-confluent WMH group [30]. Similarly, lacunes were identified and counted based on STRIVE criteria [31], while EPVS were counted and scored based on criteria described in Doubal et al. [32]. The degree of medial temporal atrophy (MTA) based on Scheltens scale was also assessed [33]. All the visual ratings were performed independently by two trained raters prior to study hypothesis design and any differences in ratings that differed by a large margin (Fazekas total score difference of≥2) was resolved by rater consensus and ensuring that the appropriate image slices were used for rating. The inter-rater agreement between the raters was strong with kappa > 0.80.
Measurement of APOE genotyping
Blood was drawn from the study participants after cognitive assessments and getting informed consents. The details for A POE genotyping methodology are available in our previously published study [34]. Neither participants nor the study team members were aware of participants’ APOE4 status at the recruitment and study inclusion stage.
Statistical analysis
Data preparation
All variables were checked for normality using the Shapiro-Wilk test. WMH volumes were transformed using log-transformation with a 1 added prior to transformation to account for the zero WMH in the frontal, temporal, parietal and occipital regions in the moderation and regression analysis. The statistical assumptions for parametric tests were satisfied.
Group differences
To assess the statistical differences, independent sample T-test was carried out on age and education while chi-square test was carried out on sex in APOE4 carriers against non-carriers. For neuropsychiatric performance, CVD risk factors, and brain volume measures, we performed logistic-regression analysis on categorical variables and univariate analysis of covariance on continuous variables with age, education, GM, and TIV as covariates to control for group differences due to these confounding measures between APOE4 carriers against non-carriers.
Moderation and logistic regression analysis
A moderation analysis quantifies whether the relationship between a predictor variable (X) and an outcome (Y) is strengthened or weakened in the presence of a third variable (W). In our a priori moderation model (Fig. 1a), the predictor (X) was total and lobar WMH volumes, the outcome (Y) was domain-specific cognitive z-score, and the third moderating variable (W) was the presence of the APOE4 allele. An independent moderation analysis was run for total and each lobar WMH as the predictor and composite z-scores for each cognitive domain as the outcome.
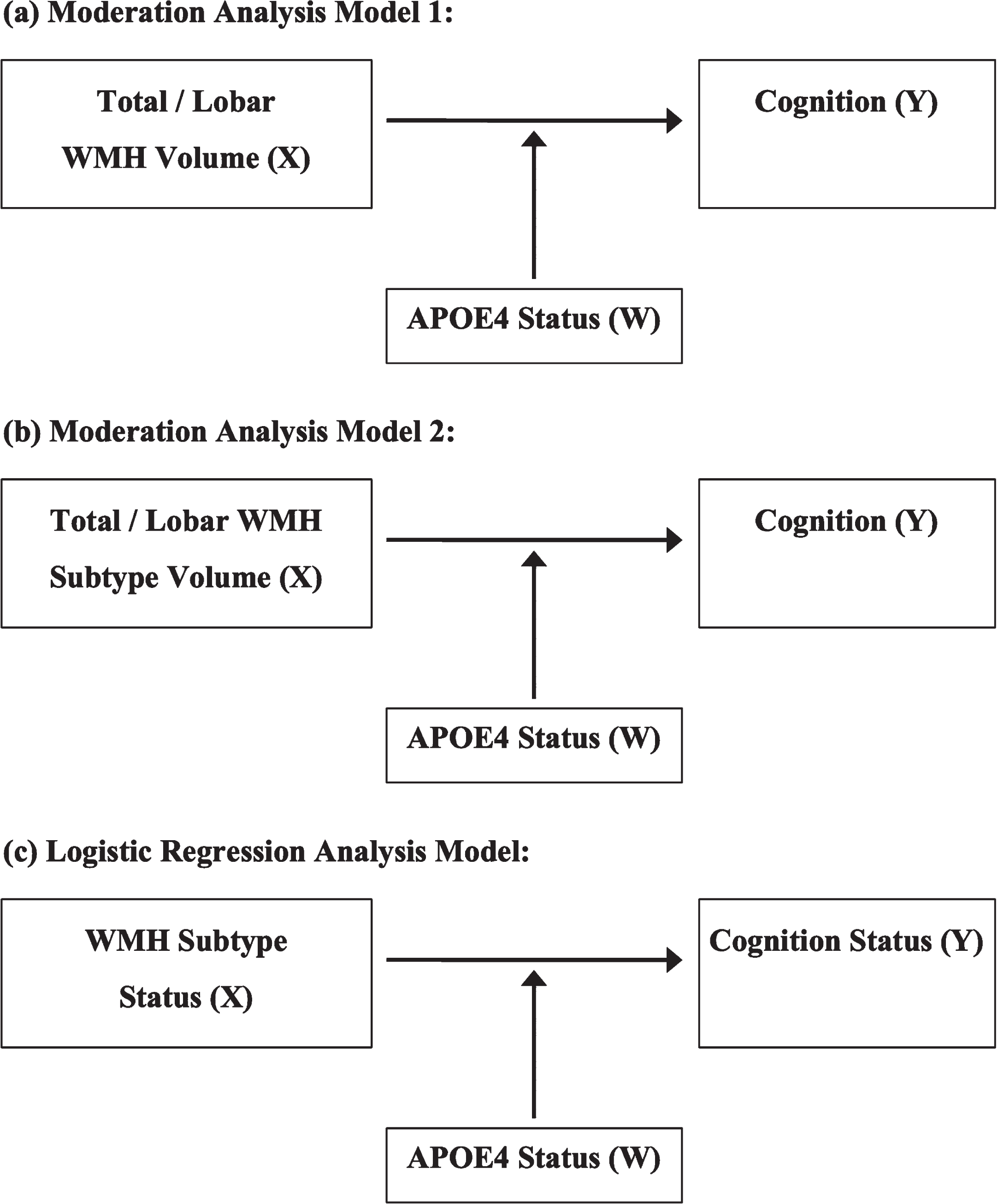
APOE4 moderation and regression analysis models. All the analyses models controlled for demographics (age, sex, education), diagnosis, CVD risk factors (history of hypertension), brain volume (total intracranial volume, grey matter), and cerebral small vessel disease markers (perivascular spaces and lacunes rating scores). a) Moderation model tested whether the association between the predictor WMH volumes (X) and the outcome, performance on cognitive tests (Y), was moderated by a third variable, the APOE4 allele (W) for total as well as lobar WMH volumes separately in the whole cohort. b) Moderation model tested whether the predictor WMH volumes (X) and cognition (Y) was moderated by APOE4 allele (W) for total as well as lobar WMH volumes in each confluent and non-confluent WMH subtype groups separately. c) Logistic regression model examining whether the WMH subtype status (X) and outcome variable, cognitive impairment status (Y), was moderated by APOE4 status (W) in the whole cohort.
Additionally, to identify whether the effect of WMH on cognition was driven by WMH severity, we split the cohort into confluent WMH (N = 119) and non-confluent WMH (N = 97) subgroups and reran the moderation analysis to examine how APOE4 status moderates their relationship in each subgroup separately (Fig. 1b). We also ran a t-test to identify any group differences between confluent and non-confluent WMH irrespective of their APOE4 status. We further sought to investigate the clinical relevance of any interaction findings by running a logistic regression to identify the probability of developing significant cognitive impairment in the presence of APOE4 and confluent WMH (Fig. 1c). The outcome for the logistic regression was domain-specific cognitive impairment, operationalized as a score of 1.5 SD below the group mean based on published guidelines and our previous work [35, 36]. Predictor variable (X) included confluent or non-confluent WMH status, moderator included APOE4 status, and outcome was cognition status. The moderation and logistic regression models controlled for age, sex, education, history of hypertension (as it was the only CVRF significantly different between APOE4 carriers and non-carriers), GM volume, TIV, EPVS, and lacunes. We further included the SCI and MCI diagnosis status as covariate since there have been prior reports to show that high prevalence of hypertension is linked to WMH pathology [37] and could have effects on cognition [1].
All moderation analyses were conducted using the PROCESS macro on SPSS [38]. All analyses corrected for multiple comparison using a simulated bootstrap procedure with 1000 resamples [39]. This bootstrapping procedure has been empirically validated to derive robust parameter estimates based on maximized power and limited type 1 error rates [39]. Effect size in tests of moderation was determined using f2 [40]. Cohen has suggested that f2 effect sizes of 0.02, 0.15, and 0.35 are termed small, medium, and large, respectively [41].
RESULTS
Baseline characteristics between APOE4 carriers and non-carriers
There were no significant differences between APOE4 carriers and non-carriers in terms of participants’ age, sex, and education level (p > 0.05, Table 1). The measures of CVRF were also not statistically different between the two groups except for the history of hypertension which was significantly lower in APOE4 carriers (26%) compared to non-carriers (40%) (p = 0.04). Among the cognitive measures, only performance on episodic memory domain tests, namely the ADAS immediate, ADAS delayed recall and immediate and delayed story recall, were significantly poorer in APOE4 carriers compared to non-carriers (Table 2) while global and other cognitive domains showed no statistical differences. Furthermore, the total as well as lobar WMH volumes in temporal and occipital regions were significantly higher in APOE4 carriers compared to non-carriers (Table 2). Other MRI markers including total GM volume, MTA score, EPVS, and lacunes count were also not statistically different between the two groups.
Participant characteristics and differences between APOE4 carriers and non-carriers
The values represent mean (standard deviation) or percentage unless otherwise indicated. aChi-square test was carried out. bTwo-sample T-test was carried out. cLogistic-regression test was carried out while controlling for age and education. dUnivariate analysis of covariance test was carried out, while controlling for age and education.
Differences in cognition and MRI biomarkers between APOE4 carriers and non-carriers
The values represent mean±standard deviation (range) unless otherwise indicated. The brain volumes are measured in ml. aUnivariate analysis of covariance test was carried out with age, education and history of hypertension as confounders. bChi-square test was carried out. cUnivariate analysis of covariance test was carried out with age, education, history of hypertension and total intracranial volume as confounders. Ψ The higher scores indicate poorer memory performance. WMH, white matter hyperintensity; MRI, magnetic resonance imaging; MTA, medial temporal atrophy.
Moderation trends in the whole cohort model
Direct relationships
X ⟶ Y: Global and lobar WMH (X) were not directly associated with any cognitive outcomes (Y), including global performance and performance with episodic memory, executive function, attention and language domains (p > 0.05) as shown in Table 3.
Direct relationships and interactions between WMH volumes and APOE4 on cognition
Moderation analysis was carried out with age, education, history of hypertension, grey matter volume, total intracranial volume, and diagnosis status as covariates. SE, standard error; BC, bias corrected; CI, confidence interval; WMH, white matter hyperintensities.
X⟶W: Global and lobar WMH (X) were not associated with the APOE4 status (p > 0.05).
W⟶Y: APOE4 was also not directly associated with cognitive outcome (Y) including global and domain specific cognitive measures (p > 0.05) in total and lobar WMH moderation models as shown in Table 3.
Interactions
XW⟶Y: Table 3 shows that APOE4 (W) significantly interacted with total as well as lobar WMH (X) to predict episodic memory (Y). In particular, APOE4 strengthened the relationship between higher total WMH burden and worse episodic memory performance (Table 3, Fig. 2a). Similarly, at the lobar WMH levels, APOE4 strengthened associations between frontal, temporal, parietal, and occipital WMH and episodic memory performance (Fig. 2b-e) with large sized effects (β) observed for total as well as lobar WMH. APOE4 did not interact with either total or lobar WMH to predict worse cognition in other cognitive domains— executive functions, attention, or language domains (p > 0.05).
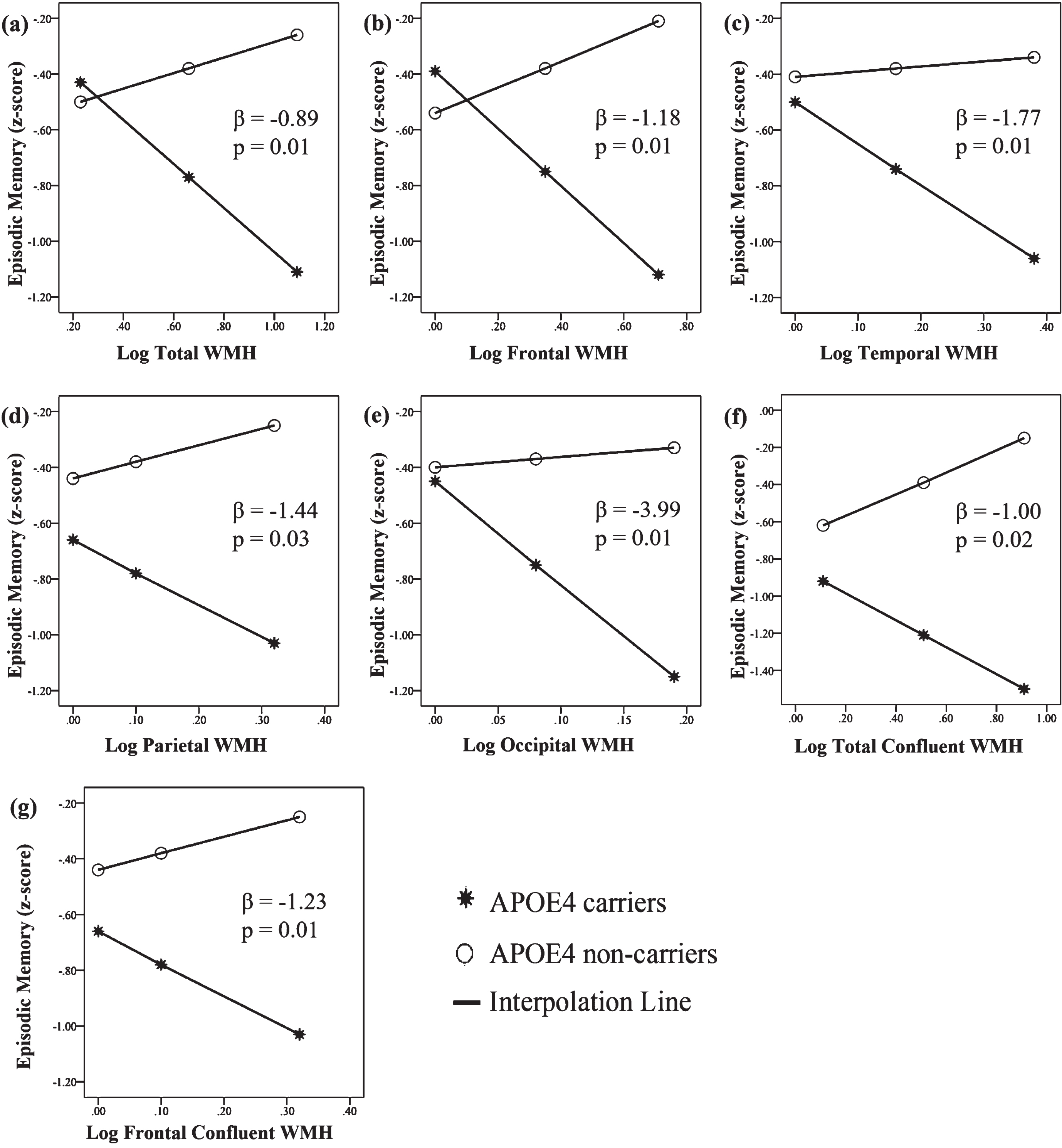
APOE 4 interaction moderated the relationship between WMH and episodic memory (composite z-score). a) With APOE4 interaction, higher WMH burden was associated with worse episodic memory with large effect size compared to APOE4 non-carriers. b-e) Similar APOE4 interaction trends were observed between episodic memory and frontal, temporal, parietal, and occipital WMH with varying but larger effect sized interactions. Likewise, for WMH subtype, panels f and g show that APOE4 interaction moderated the relationship between total as well as frontal WMH burden and episodic memory in the confluent WMH subgroup.
Group differences in confluent versus non-confluent WMH groups
Group-level differences for confluent and non-confluent WMH, irrespective of their APOE4 status, are shown in Supplementary Table 1. Overall, the participants with confluent WMH were older than non-confluent WMH and had significantly higher lacunes, EPVS, and WMH volumes in total and lobar regions.
Moderation trends in confluent and non-confluent WMH subgroup model
Direct relationships
X⟶Y: The frontal WMH showed direct relationship with episodic memory only in participants with confluent WMH subtype with large effect size (Table 4).
The relationships between WMH volumes, APOE4, and cognition in participants with confluent and non-confluent WMH
Moderation analysis was carried out with age, education, history of hypertension, grey matter volume, total intracranial volume and diagnosis status as covariates. SE, standard error; BC, bias corrected; CI, confidence interval; WMH, white matter hyperintensities.
W⟶Y: APOE4 showed no direct relationship with episodic memory in participants with confluent or non-confluent WMH for total as well as lobar WMH models (Table 4).
X⟶W: Global and lobar WMH (X) in WMH subtype groups showed no direct relationship with the APOE4 status (p > 0.05).
Interactions
XW⟶Y: The APOE4 strengthened the relationship between total as well as frontal WMH with episodic memory in the confluent WMH subgroup, which was a large effect size (Table 4, Fig. 2f, g). APOE4 also strengthened the relationship between parietal WMH with episodic memory in the non-confluent WMH subgroup, which was a large effect size (Table 4). However, this interaction effect for non-confluent WMH subtype was an incidental finding in opposite direction. The WMH log-transformation increased the parietal log-WMH volume when the WMH was actually absent in the majority of participants, resulting in this anomalous trend.
Logistic regression model trends
To determine the clinical relevance of above findings, we ran a logistic regression to identify the probability of developing significant cognitive impairment in the presence of APOE4 and confluent WMH. Looking at the interaction between APOE4 and WMH subtype status in the whole sample, we found that the memory impairment (defined as 1.5 SD below the mean) was 4.81 times more likely to develop in participants with APOE4 and confluent WMH compared to participants with no APOE4 allele and non-confluent WMH (Table 5). Within the APOE4 carriers, the odds of developing memory impairment were 7.85 times higher in those with confluent WMH compared to those with non-confluent WMH (p < 0.01) (Table 5). This trend was not observed in APOE4 non-carriers (p = 0.99) (Table 5).
The odds of developing memory impairment due to WHM subtype status from the logistic regression analysis
Logistic regression analysis was carried out with age, education, history of hypertension, grey matter volume and total intracranial volume and diagnosis status as covariates. OR, odds ratio; SE, standard error; BC, bias corrected; CI, confidence interval; WMH, white matter hyperintensities.
DISCUSSION
Our findings demonstrate that both global and regional WMH volumes have a strong negative effect on episodic memory performance among APOE4 carriers compared to non-carriers. In addition to total WMH volume, the presence of confluent type WMH was associated with greater impairment in episodic memory. Participants with confluent WMH and the APOE4 allele were 4.81 times more at risk of developing memory impairment compared to participants with non-confluent WMH and no APOE4 allele. Within the APOE4 carriers, the odds of developing memory impairment were 7.85 times higher in those with confluent WMH compared to those with non-confluent WMH. This difference was not observed in APOE4 non-carriers. These findings highlight that APOE4 and confluent WMH have a synergistic effect on cognitive impairment at the prodromal dementia stage.
In this paper, we report that the effect of WMH on cognitive domain impairment in the setting of APOE4 among prodromal dementia is not specific to the location of the WMH burden. Previous studies in participants with established dementia, have demonstrated association between WMH and cognition [13]. A recent study on effects of WMH lesion locations on cognitive domains in non-demented healthy elderly have linked frontal WMH with executive dysfunction and parieto-temporal WMH with memory dysfunction [16]. We demonstrate that at the prodromal dementia stage, WMH in the frontal, temporal, parietal, and occipital regions have a similar large sized APOE4 interaction effect with memory impairment. However, not all regions of WMH are equally sensitive to the APOE4 allele as the regional effect sizes differ.
The type of WMH lesion (confluent versus non-confluent) was also key in the synergistic relationship between WMH and APOE4 on cognition. We showed that APOE4 strengthened the relationship between total as well as frontal WMH and episodic memory in confluent WMH subgroup. The observed interaction effect of APEO4 in the confluent WMH subtype, especially in the frontal brain areas, indicate significant contribution of APOE4 in the episodic memory dysfunction at prodromal dementia stage. We further showed that APOE4 carriers exhibiting confluent WMH were 4.81 times more likely to develop memory impairment compared to APOE4 non-carriers exhibiting non-confluent WMH. This is consistent with previous research demonstrating that the higher the severity of the WMH (confluent versus non-confluent), the more rapidly the slope of cognitive decline in APOE4 carriers versus non-carriers [10, 11]. Importantly, recent data suggests that confluent WMH leads to widespread functional brain alterations in fronto-parietal, fronto-temporal, and temporo-parietal areas which may result in loss of inhibitory control among higher order brain networks and lead to cognitive worsening in participants with MCI [10]. This is consistent and in line with our observations suggesting confluent WMH to be a greater risk factor for cognitive decline in APOE4 carriers.
WMH have been widely linked with cognitive decline in studies examining direct relationship between WMH and cognition [3, 42]. However, in this study, we did not find a direct link between the total or lobar WMH and the cognitive measures in APOE4 carrier and non-carrier groups at the prodromal dementia stage. In a recent study on effects of APOE4 status on cognition in an AD cohort, APOE4 is reported to play a major role in influencing the relationship between WMH and cognition when comparing APOE4 carriers and non-carriers [13]. Importantly, memory impairment is believed to be one of the most consistent trends observed in APOE4 carriers among healthy elderly and MCI [43, 44]. In the prodromal dementia stage, APOE4 in known to influence the neurocircuitry in the frontal, temporal, parietal, and occipital regions linked with episodic memory [45, 46]. Our findings also indicate similar results with the decline in episodic memory performance. However, it was not observed as a direct relationship between WMH and cognitive performance. Our findings demonstrated a mechanism whereby APOE4 status influences the relationship between the episodic memory and WMH. The interaction of compromised white matter integrity due to higher WMH burden at prodromal dementia stage and the APOE4 genotype may induce episodic memory decline similar to previously observed trends [13, 42]. With further WMH progression, other cognitive functions such as processing speed and execute function may also deteriorate [15].
This study has some limitations as well. Limitations of this study include the relatively small sample group size, especially the APOE4 group, and the cross-sectional study design. Due to this small sample size, we were not able to look at the relationship between APOE4, WMH, and cognition within SCI and MCI participants independently. Additionally, due to the small sample size, participants with homozygotes and heterozygotes APOE4 gene expressions were grouped together for higher statistical power in the analysis. Another limitation of this study is unavailability of amyloid-β levels for the included participants which could have impacted the findings. Therefore, further longitudinal studies in cohorts with prodromal dementia having a larger proportion of APOE4 carriers and having AD biomarker profiles will need to becarried out.
Conclusion
We demonstrate that the risk of cognitive impairment was large in prodromal dementia individuals with confluent WMH and the APOE4 allele, as they were 4.81 times more likely to have memory impairment compared to individuals with non-confluent WMH and no APOE4 allele. Clinical implications include that APOE4 carriers with WMH in the frontal, temporal, parietal, and occipital regions, are most at risk of memory impairment and should be identified for early and intensive WMH management.
Footnotes
ACKNOWLEDGMENTS
This research is supported by the Ministry of Education, Singapore, under its MOE AcRF Tier 3 Award MOE2017-T3-1-002, National Medical Research Council (NMRC), Singapore, under its Clinician Scientist Award (MOH-CSAINV18nov-0007) and Clinician Scientist Individual Research Grant (NMRC/CIRG/14MAY025).