
Abstract
Background:
The relationship between diabetes mellitus and neurodegenerative disorders has been of great interest. Macrophage migration inhibitory factor (MIF) is a pro-inflammatory cytokine in which a variety of signaling cascades are activated through it. MIF has been involved in the pathogenesis of several diseases and can predict early pre-symptomatic stages of neurodegeneration in diabetic patients.
Objective:
To investigate whether serum MIF could predict brain neurodegeneration at the early pre-symptomatic stages in diabetic patients.
Methods:
We examined adults with type 2 diabetes mellitus and compared with normal control adults using a short form of the IQCODE and biochemical examination, including assessment of HA1C, fasting blood glucose, lipid profile, and MIF which was measured by ELISA technique. Correlations between parameters were studied. Computational PathLinker bioinformatic tool was used to search for potential pathway reconstructions for the insulin/amyloid-β/MIF signaling.
Results:
We demonstrated that MIF level was increased in the serum at the early pre-symptomatic stages of neurodegenerative disorder in diabetic patients. In addition, network analysis demonstrates that insulin receptor substrate 1 can ameliorate amyloid-β protein precursor through COP9 signalosome complex subunit 5 that enhances MIF elevation.
Conclusion:
Diagnosis processes could not be used as routine examinations for still pre-symptomatic neurodegenerative disorders. This may be due to the time constraints and the heavy dependence on the physician’s experience. Therefore, serum MIF level could predict brain neurodegeneration at the early pre-symptomatic stages in diabetic patients which may support its potential utility as a clinically useful biomarker.
Keywords
INTRODUCTION
Neurodegenerative disorders (ND) are associated with population aging. The numbers of patients with ND are predicted to escalate from 58 million in 2021 to 88 million in 2050 worldwide [1]. Many factors increase the risk of ND, besides aging, including impaired glucose processing which is a precursor to diabetes. Diabetes mellitus (DM) is a metabolic condition, and the estimated number of patients above 65 years with DM was 136 million in 2019 [2]. In cooperation, incidence of DM and ND increase with age and remain a remarkable universal problem. The relationship between DM and ND has been of great interest in which all-cause ND is more of vascular type rather than neurodegenerative type. Even between individuals without DM, greater glucose levels increased the hazard of cognitive deficiency [3]. Memory health centers are well-known for diagnosing dementia and cognitive follow-ups; however, post-diagnosis management has not been shown to improve the quality of life of patients. Otherwise, cognitive drop and glycemic control act together in patients with dementia in unidentified way [4].
Cognitive functions experienced with the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) involved short- and long-term memory, calculation, time and space coordination, learning, and organization. The summation of the scores was the average of the 16 items to produce a total score extending from 1 to 5, with higher scores demonstrating more impairment. In the present study, the diabetic informants represent predominantly clinical demonstration of memory loss, with a number of other alterations in brain function, including confused behavior and deficiencies in language, understanding, and visual-spatial abilities. Accordingly, IQCODE is one of the clinical assessment methods used for cognitive impairments. As the IQCODE is a consistent and certified informant-based instrument for assessing alterations in everyday cognitive dysfunction over a 10-year period, it has been widely accepted by clinical researchers across diverse languages and cultures [5–7]. In general, informant-based assessments do not depend on direct patient testing, consequently capturing ups and downs over time promising and making these assessments less susceptible to social-cultural biases [6, 8]. Also, a major advantage of the IQCODE is that it is not affected by the patient’s learning and/or intelligence. These properties are important for obtaining acceptable diagnostic accuracy, which is required for screening tools [9]. Moreover, from a clinician’s viewpoint, the assets of the IQCODE are that it is copyright allowed, obtainable in diverse languages, and quite easy to complete. There have been numerous studies supporting the rationality of the IQCODE for dementia screening, with a specificity extending from 68 to 100% and a sensitivity reaching from 79 to 100% [10–13]. On the other hand, no studies assessing the usefulness of IQCODE for evaluating the severity of cognitive deficiencies in patients with Alzheimer’s disease have been issued.
Traditional diagnostic tools for ND are established on clinical measures, and a complete diagnosis still relies on pathological estimation at autopsy. Furthermore, neurodegenerative processes begin several years before clinical symptoms. Pre-symptomatic stages of dementia could be more frequent at early onset of other diseases such as DM. It is now known that pre-symptomatic cognitive alterations occur as shortages in speaking episodic memory and deficiencies in giving out speed, decision-making function, and overall intelligence. There is increasing attention in discovery of neuropsychological measures that can prolong the interval over which pre-symptomatic cognitive drop is measurable; in particular, such measures would be very valuable to compliment biomarker changes. In spite of a series of biomarkers that are used from very early stages of the disease in plasma, cerebrospinal fluid, and neuroimaging such as PET, there is consequently a vital requirement for a consistent ND biomarker to help in the identification of preclinical symptoms, quick diagnosis, expectation of disease development, and response to treatment [14]. There is growing indication that inflammatory procedures show an essential role in the development of neuropathological variations in ND. Clinical and experimental confirmation supports the contribution of inflammatory changes in the early stages of ND, even earlier than the presence of amyloid deposits. Thus, biomarkers that reveal the inflammatory process in ND become assurance. Assessments dependent on these should if possible be reliable and costw effect, which will increase the motivation to use blood-based biomarkers [15].
Macrophage migration inhibitory factor (MIF) is a pleiotropic pro-inflammatory cytokine produced by several cells of the innate and adaptive immune system, as well as non-immune cells. Recent studies have shown that MIF is associated with brain aging and tau pathology, thus this molecule may be a valuable diagnostic marker and therapeutic target [16]. In turn, a variety of signaling cascades, for example the MAPK, PI3K/AKT, and NF-kB pathways are activated. By doing so, MIF activates pro-inflammatory events including the secretion of IL-6, TNF-α, and the activation of the inflammasome. For this reason, MIF has been implicated in the pathogenesis of several autoimmune diseases including type 1 diabetes, multiple sclerosis, autoimmune hepatitis, and rheumatoid arthritis [17].
On the other hand, signaling pathways are a keystone of systems biology. Numerous databases supply high-grade depictions of these pathways that are docile for automated analyses [18]. Computational techniques in molecular systems biology can help with understanding how cellular molecules, such as proteins, from different cellular processes can interact to contribute to a larger cellular response. PathLinker is an innovative computational method selected to reconstruct the interactions in a signaling pathway of interest. PathLinker powerfully computes multiple short paths from the receptors to transcriptional regulators (TRs) in a pathway within a background protein interaction network. PathLinker has higher precision and recall than several up-to-date algorithms, whereas also confirming that the resultant network links receptor proteins to TRs [19]. However, PathLinker has two main limitations: 1) producing many paths that have the same reconstruction weight, and 2) occasional incorporation of non-relevant interactions with respect to the process under investigation [20–22]. LocPL, post PathLinker processing technique, overcomes these limitations by utilizing protein localization information [21] to minimize the unrealistic interactions in terms of cellular compartment co-localization and to re-prioritize the tied paths resulting from PathLinker [20]. In this research we apply the PathLinker and LocPL techniques to reconstruct the insulin/amyloid-β/MIF signaling pathway, if existing computationally, to highlight the promising role of measuring the MIF level for the diagnosis of pre-sympatomatic ND diabetic patients.
The purpose of this study is to investigate whether serum MIF could predict early pre-symptomatic stages of neurodegeneration in diabetic patients.
MATERIALS AND METHODS
Patients
Forty community participants were included in this observational study, of whom 10 were non-diabetic cognitively healthy volunteers and 30 had type 2 DM (either non cognitive impairment symptoms (DMNAD, n = 10) or pre-symptomatic (DMPAD, n = 20) aged around 60 years old (Table 1). The participants with type 2 DM were recruited among patients attending the Mansoura University Hospital, Al Batinah specialized Hospital, and the international hospital, Mansoura, Egypt. Inclusion criteria also include those with duration of diabetes more than 5 years, hypertensive, and no specific criteria for educational level. Patients with severe diabetic complications or associated medical conditions such as: blindness, liver cirrhosis, congestive heart failure, neuropathy, retinopathy, unstable angina pectoris, and physiological conditions that hamper patient cooperation were excluded. Also, they had no major psychiatric or neurological disorders, substance abuse, or severe or unstable physical illness that may contribute to cognitive impairment. All subjects were informed of the study’s aims and methods, and informed consent was obtained. The control subjects had no history, symptoms, or signs of relevant psychiatric or neurologic diseases and no cognitive impairment. The study was accepted by the local Ethics Committee, Delta University for Science and Technology (FPDU 9/2021) and the study was completed in agreement with the ethical standards placed down in the 2010 Declaration of Helsinki and its advanced revisions with 1975.
Participants characteristics
N, normal control group; DMNAD, diabetes mellitus non symptomatic neurodegenerative disorder; DMPAD, diabetes mellitus pre-symptomatic neurodegenerative disorder. aSignificant versus control group, bSignificant versus DMNAD group, p < 0.05. Education level: 1. Nescience, 2. House education, 3. Adult literacy class or night school, 4. Drop out primary school, 5. Primary school, 6. Junior high school, 7. Senior high school, 8. Collage or above.
Informed consent was obtained from participants with the ability to consent. If they did not have the capability, a close family member was requested to give agreement for the person’s contribution and sign the agreement. All the informants were those who had been living with the patients for more than 10 years, communicated with them at least 4 times per week, or understood the patients’ situation well.
The diagnosis of pre-symptomatics was based on IQCODE and clinical evaluation and was made by a consensus conference of neuropsychologists, psychiatrists, and/or neurologists under supervision of the second author between December 2017 and October 2019. The protocol was carried out in accordance with Delta University for Science and Technology guidelines prior to inclusion into the study. The participants in this study completed IQCODE [5, 6] questionnaires. All tests and scales are validated and widely used in the field.
Assessment of cognitive functions by IQCODE
Cognitive functions that were tested with the short IQCODE included short- and long-term memory, space and time orientation, calculation, learning, and administration [7]. Each item was rated on a 5-point scale with representation of: 1 “much improved”, 2 “a bit improved”, 3 “not much change”, 4 “a bit worse”, and 5 “much worse”. The total of the scores of the 16 items was used to produce a total score extending from 1 to 5, with upper scores signifying greater impairment.
Brain imaging
All patients underwent brain imaging. Magnetic resonance imaging was chosen to compute tomography and achieved regularly. Imaging permitted us to eliminate a neurosurgical etiology of dementia (chronic subdural hematoma, normal pressure hydrocephalus, etc.) and to examine for vascular or degenerative lesions. It also permitted us to qualitatively evaluate corticosteroid-induced subcortical atrophy and hippocampal atrophy.
Samples collection
Blood was obtained by venous arm punctures from participants after overnight fasting. 5 mL of blood was added directly to plain tubes and centrifuged at 4000 rpm for 15 min (5804 centrifuge, Eppendorf Company, German) to separate the serum, at Mansoura university hospital’s laboratory. Serum was divided into two aliquots. The first portion was used for immediate analysis of lipid profile, HbA1c %, and fasting blood glucose (FBG) level. The second one was stored frozen at –70°C until analysis of MIF level.
Laboratory investigations
The separated serum samples were used for colorimetric determination of total cholesterol, LDL-cholesterol, and HDL-cholesterol by Cholesterol LiquiColor® Test kits (Stanbio Laboratory, Texas) [8], and triglycerides [9] using Triglyceride LiquiColor® Test kit (Stanbio Laboratory, Texas).
Enzyme linked immunoassay (ELISA) for quantitative determination of serum MIF
Serum MIF level was determined by enzyme-linked immunosorbent assay (ELISA) technique by a commercial kit obtained from NOVA (Bioneovan Co. Ltd., Beijing, China). Briefly, the Micro ELISA stripe plates were pre-coated with an antibody definite to MIF, and 50μL of horseradish peroxidase-conjugated antibody specific for MIF was further added to each well except the blank control well. The plate was closed and incubated for 30 min at room temperature. Free components were washed away. After that, 100μL of substrate solution was added to all wells, which were at that time protected from light, shaken mildly, and incubated at room temperature for 15 min. The reaction was ended by adding 50μL of stop solution to all wells. A color change in the well from blue to yellow was seen. The absorbance was measured using a microtiter plate reader (Tecan, Infinite 200 PRO, Switzerland) at 450 nm. Serum MIF concentration was calculated based on the standard curve and expressed in absolute terms (pg/mL). Limit of detection for MIF was 36–1800 pg/mL.
Network bioinformatics analysis
Signaling pathways were reconstructed using the PathLinker app (https://apps.cytoscape.org/apps/pathlinker) running within the Cytoscape software https://apps.cytoscape.org/help/getstarted_app_install. PathLinker [19] is used to computationally investigate the existence of potential relationships between insulin receptor 1 and amyloid-β (Aβ) passing to MIF. PathLinker takes three inputs: 1) an interactome G, 2) a set of cellular receptors R, and 3) a set of transcription regulators (TR) T. The interactome is a graph G = (V, E), where the graph nodes V are proteins and the graph edges E are the interactions between these proteins (PPIs). The graph edges are directed and each edge, e = (u, v) ∈ E, has a weight w uv ∈ [0, 1]. In this study, we used the PLNet2 interactome introduced in [11]. PLNet2 has 17,168 nodes and 612,516 directed edges. The considerations used in PathLinker were: 1) k: 50 (number of paths considered); 2) edge penalty: 1; and 3) edge weight: weight probabilities, whereby it reflects the edge weights as multiplicative, which result in the k highest probability paths (since weights here are probabilities and not penalties; but still they represent the k-shortest paths).The output of PathLinker is the k-shortest paths from any receptor in R to any TR in T. These k paths form the pathway reconstruction for a particular cellular process, and they are ranked by a reconstruction weight, where the shortest path has the highest reconstruction weight which reflects the degree of belief for that path to happen.
Molecular pathway reconstruction
To overcome the limitations of PathLinker in identifying the potential pathway reconstruction for a certain cellular process, we use LocPL. The cellular compartment-specific protein-protein interaction network was constructed by the ComPPI database (https://comppi.linkgroup.hu/) [21]. LocPL uses a dynamic programming approach to compute a signaling score, other than the reconstruction score, for each path in a group of tied paths. This signaling score is used to re-order paths to break their ties based on the compartment co-localization information and to push paths with unrealistic and irrelevant interactions down the paths list.
Statistical analysis
Data were collected, revised, verified, and then edited on a personal computer. The statistical analysis was performed using SPSS Statistics for Windows ver. 16.0. Association between categorical variables was tested using Fisher’s exact test or chi-square test. Data are represented as mean±SD. Unpaired data are compared using Student’s t test (for parametric data) and Mann-Whitney test (for nonparametric data). Significance of the obtained results was considered at a p value of ≤0.05. Pearson’s test was performed to detect correlation with each parameter.
RESULTS
Table 1 showed the characteristics of the included subjects. There were non-significant changes between age and educational level between DMNAD and DMPAD, while a significant elevation (p < 0.05) in diabetes treatment duration by nearly double time of years was seen. Additionally, DMPAD showed a significant elevation in blood pressure compared to non-diabetic patients. Data presented in Table 2 assessed the general items in 40 cases which revealed a comparison of single items (16 items) and total IQCODE score of different groups (p < 0.05). The DMPAD group showed a significant increase (p < 0.05) in both single and total IQCODE compared to both normal and DMNAD groups, in which score 1 represents the much improved and score 5 represents the much worse. However, the DMNAD group showed a significant increase in some single IQCODE items (p < 0.05), items 1, 2, 3, 11, 12, 13, and 14, compared to the normal group. Moreover, the DMNAD group showed a non-significant change in total IQCODE when compared with normal group. Data presented in Fig. 1 assessed the comparison of total IQCODE score of different groups (p < 0.05).
General Items in 40 cases: Comparison of single item and total IQCODE score of different groups
N, normal control group; DMNAD, diabetes mellitus non symptomatic neurodegenerative disorder; DMPAD, diabetes mellitus pre-symptomatic neurodegenerative disorder; aSignificant versus control group, bSignificant versus DMNAD group, p < 0.05.
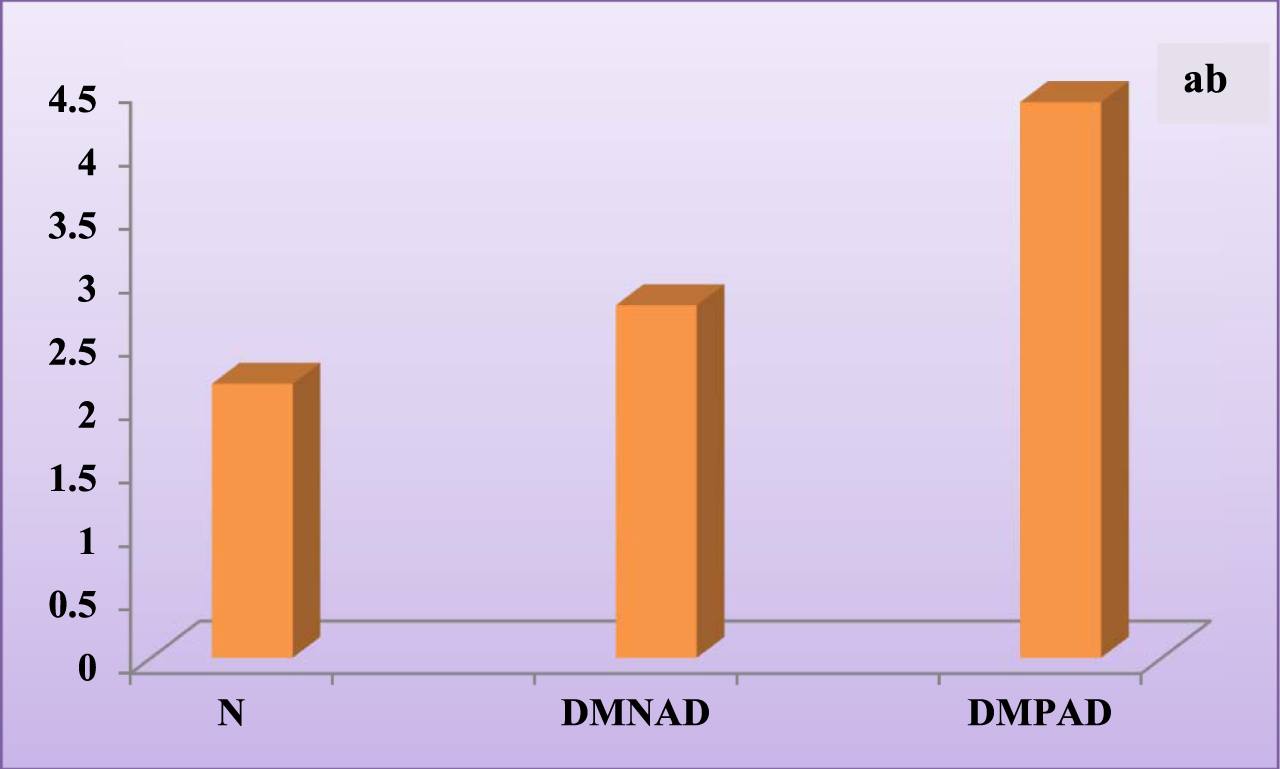
Total IQCODE score of different group. N, normal control group; DMNAD, diabetes mellitus non symptomatic neurodegenerative disorder; DMPAD, diabetes mellitus pre-symptomatic neurodegenerative disorder. aSignificant versus control group, bSignificant versus DMNAD group, p < 0.05.
On the other hand, Table 3 shows a non-significant change of serum lipid profile between the groups. Otherwise, HbA1C and FBG showed a significant elevation in both DMNAD and DMPAD groups when compared with normal group (Table 3). In the DMNAD group, HbA1C serum level and FBG were elevated significantly by nearly 28% (p < 0.05) and 99% (p < 0.05), respectively compared with non-diabetic group.
Lipid profile, HbA1C %, and FBG levels in different groups
Data presented as mean±SD, p < 0.05. T-C, total cholesterol; TG, triglycerides; LDL-C, low density lipoprotein-cholesterol; HDL-C, high density lipoprotein–cholesterol; FBG, fasting blood glucose; HbA1c, hemoglobin; N, normal control group; DMNAD, diabetes mellitus non symptomatic neurodegenerative disorder; DMPAD, diabetes mellitus pre-symptomatic neurodegenerative disorder. a significance compared to control group.
Figure 2 shows the MIF level in different groups. Diabetic patients with pre-symptoms of neurodegeneration showed a significant elevation in serum MIF level compared with non-diabetic ones (64.29%, p < 0.05) or compared with diabetics without symptoms with same ratio. Normal group is 0.87±0.78, DMNAD group is 0.92±0.41, and DMPAD group is 1.49±0.57.
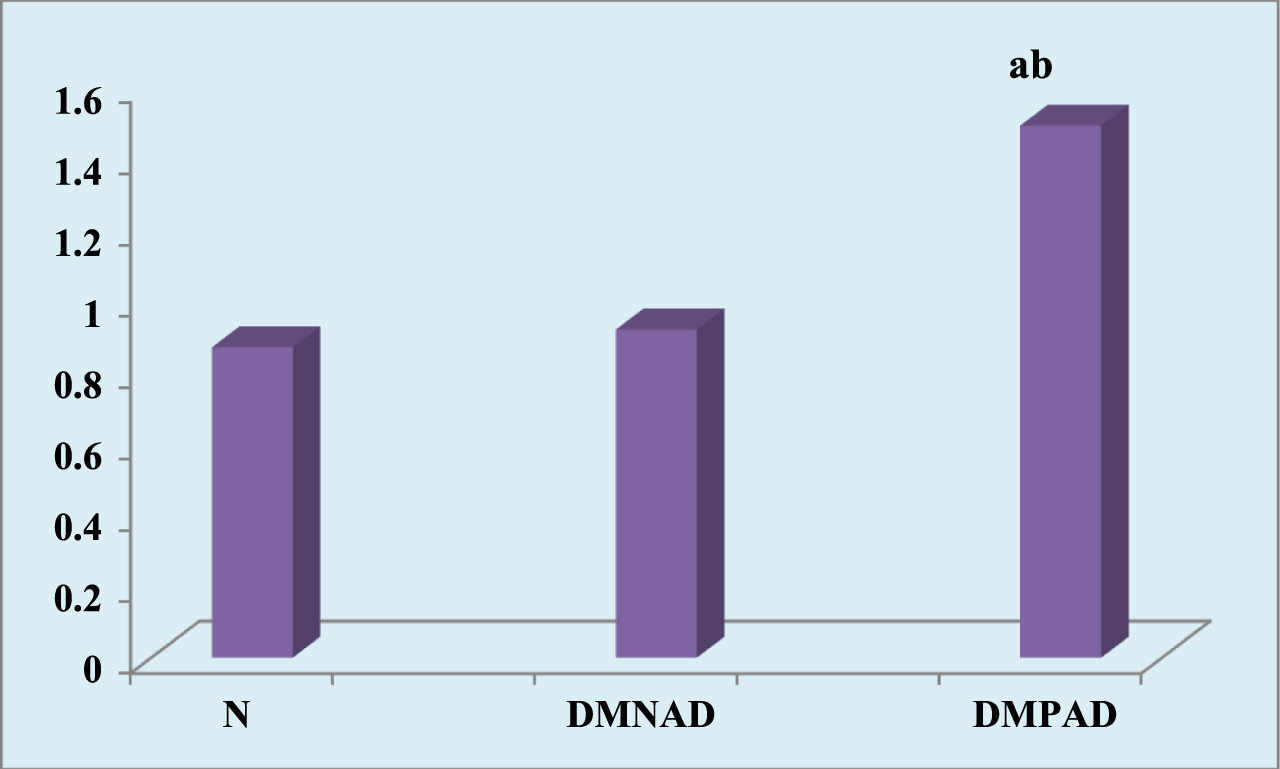
Macrophage inhibitory factor level in different groups. N, normal control group; DMNAD, diabetes mellitus non symptomatic neurodegenerative disorder; DMPAD, diabetes mellitus pre-symptomatic neurodegenerative disorder. aSignificant versus control group, bSignificant versus DMNAD group, Data presented as mean±SD, p < 0.05.
The correlations in DMNAD and DMPAD MIF values, IQCODE values, and other biochemical parameters are shown in Table 4. MIF exhibited no significant association with IQCODE and HbA1c%; however, MIF did demonstrate a significant negative association with FBG level in DMPAD and a non- significant negative association in DMNAD (r = –0.390, r = –0.351 p < 0.01) respectively.
Correlation between MIF serum concentrations and IQCODE, HA1C and FBG in different groups.
N, normal control group; DMNAD, diabetes mellitus non symptomatic neurodegenerative disorder; DMPAD, diabetes mellitus pre-symptomatic neurodegenerative disorder; IQCODE, Informant Questionnaire on Cognitive Decline in the Elderly; HbA1c, hemoglobin; FBG, fasting blood glucose; *Significant versus control group; p < 0.05, Pearson correlation.
PathLinker produced a pathway reconstruction of 29 paths, and they all are tied with the same reconstruction weight as shown in Table 5. LocPL re-prioritized these paths based on a signaling score, other than the reconstruction score, that is obtained from the cellular localization information as shown in Table 6 to guarantee that the paths residing at the top of the k-paths list are the most computationally and biologically sound paths. Figure 3 shows the reconstruction for the IRS1 and APP pathway. This reconstruction provides 29 potential paths for the interconnections, and hence relationships, between IRS1 and APP. The path with the highest probability of taking place is (IRS1, APP, COPS5, MIF). It links the insulin receptor substrate 1 (Gene Name: IRS1; UniProt ID: P35568) with the macrophage migration inhibitory factor (Gene Name: MIF; UniProt ID: P14174) through a series of interactions with the amyloid-β protein precursor (AβPP) (Gene Name: APP; UniProt ID: P05067) and the COP9 signalosome subunit 5 protein (Gene Name: COPS5; UniProt ID: Q92905).
PathLinker paths reconstruction
Path, uniport IDs; K, reconstruction path weight.
LocPL re-prioritized paths based on a signaling score
New_k, the new order of the path; Old_k, the original order of the path; Path_Score, the original score of the path based on the original PathLinker technique; Path, the path and its nodes (proteins/genes); Signaling_Score, the new score this obtained from the Localized PathLinker (LocPL) technique.

The LocPL pathway reconstruction for the top 5 paths of Table 6. Triangles represent receptors, rectangles represent transcription regulators, and ovals represent intermediate protein interactions. Protein uniprot IDs: P14174: MIF; P35568: IRS1_HUMAN Insulin receptor substrate 1IRS1; P05067: APP; Q92905 COP9 signalosome subunit 5 COPS5; O14965 aurora kinase A AURKA; P11142 heat shock protein family A (Hsp70) member 8HSPA8; P06748 nucleophosmin 1 NPM1; P04406 glyceraldehyde-3-phosphate dehydrogenase GAPDH; P00533 epidermal growth factor receptor EGFR.
DISCUSSION
Production of AβPP and build-up of neurotoxic Aβ peptide is essential to the pathogenesis of ND. Therefore, knowing the molecules that signify Aβ generation is vital for diagnostic approaches for pre-symptomatic ND. This study was designed to evaluate the role of MIF on prediction of brain neurodegeneration at the early pre-symptomatic stages in diabetic patients. PathLinker’s reconstruction of the insulin/Aβ/MIF signaling pathway is applied to predict the most probable signaling pathway that can establish the starring role of MIF in identification of pre-sympatomatic ND diabetic patients.
The initial purpose of this study was to inspect whether a sample of diabetic patients would perform in a different way on measures of cognitive functioning when compared to healthy ones. To our knowledge, this is the first feasibility trial from Egypt to report the performance of a diabetic people with mild cognitive impairment performing poorly on measures of cognitive activity compared to a healthy control group, agreeing to an Arabic version of IQCODE [23]. In previous studies, there has been a dispute on whether mild cognitive weakening is a prodromal phase of NDs [24]. This probability trial suggests that in a diabetic population, there is impairment of cognitive functioning between those who fulfilled the criteria of mild cognitive impairment, an assessment previously distinguished by others [25, 26].
The mechanisms concerning DM and ND are indistinct. In this study, we found that diabetic patients performed more poorly on cognitive testing and had IQCODE decline and risk of developing cognitive impairment compared to participants without diabetes. In addition, patients with elevated fasting glucose levels tended to have cognitive scores and rates of decline intermediate between diabetic and those with normal glucose measures. This finding supports the hypothesis that abnormal glucose metabolism is linked to cognition and increased risk of developing cognitive impairment and dementia in elderly patients. Our results are concomitant with several studies that have reported an inverse association between diabetes and cognitive performance in older adults [26–28]. Otherwise, the non-significant change in lipid profile for both DMNAD and DMPAD groups compared to the normal group indicates that the cerebrovascular risk factors such as dyslipidemia is not a conventional mechanism. The non-cerebrovascular mechanisms potentially linking DM and ND include FBG and HA1C levels and may accompany hyperinsulinemia [26, 27]. Insulin can cross the blood-brain barrier, and peripheral insulin infusion in the elderly raises Aβ levels in the cerebrospinal fluid, an indirect marker of ND risk. Diabetic human and animal tissues have upregulation of insulin receptor substrate 1 and increased progressive products of glycosylation, perceived in ND which is classically associated with peripheral insulin resistance in diabetes [28, 29].
MIF has been considered one among many moonlighting proteins which have diverse, unconnected capabilities. MIF functions are interrelated to its cell biology in regard to its existence within the nucleus, cytosol, and the extracellular space [30], but we need a whole consideration of the intermolecular and intramolecular mechanisms that manage its diverse and non-overlapping capabilities.
In the existing study, we have shown that MIF level was elevated within the plasma of diabetic pre-symptomatic ND subjects. Notably, the MIF level was not altered in patients without ND symptoms, suggesting that MIF probably was immediately upregulated at the early stage of ND pathology. MIF as a pro-inflammatory cytokine has been proven to be upregulated systematically in flow and regionally at lesion sites in lots of continual inflammatory illnesses and performs critical roles in complaint progression. Previous research has proven that MIF turned into upregulated in plasma and cerebrospinal fluid from ND sufferers [30–33]. This result is in accordance with those obtained in 14-month-old APP23 transgenic mice, which related to some Aβ deposits [34]. Remarkably, unaltered MIF level in diabetic non symptomatic subjects supports the hypothesis that the increase in MIF level in plasma is particularly occurring in the case of dementia sufferers because of ND. Therefore, it is believed that increases in MIF level might be a neuronal protection mechanism as reported in ND patients, which is suggestive that MIF level in plasma could reliably function as a biomarker.
While the PPIs can define the relationship between the involved cellular processes and can shed light on the underlying mechanisms [11], existing databases for manually curated and/or experimentally derived PPIs model the interaction information as a graph, an interactome, where proteins that are known to interact are connected by edges in the graph. This approach can help with understanding how signals flow between the interacting proteins [34, 35]. In general, the re-ordered paths are more likely to happen from the biology perspective. The first re-ordered path is the most probable path to happen considering the localization information of the proteins/genes. More importantly, we for the first time represent the shortest interplay among MIF and Aβ via the maximum promising pathway of insulin receptor substrate 1. Taken collectively, our bioinformatics network evaluation furnished first-hand notion of MIF pathway during Alzheimer’s disease development through insulin receptor substrate 1 which can enhance AβPP via the multi-protein complex photomorphogenesis 9 (COP9) (CSN) signalosome complicated subunit five (COPS5) that has multiple functions in the cell.
In a number of primary neuronal cultures and cell lines by forming multilateral protein complexes consequently leading to increased amyloid plaque burden in the brain, COPS5 robustly increased Aβ generation. Taken together, these results suggest that COPS5 is a MIF-binding protein that increases AβPP processing and Aβ generation by elevating MIF levels [36, 37]. Our study is in agreement with Turtzo et al. who identified the MIF as an intracellular interactor of COPS5 [38].
Other studies represent that by directly interacting with key inflammatory and apoptosis mediators such as MIF, p53, c-Jun, Smad4, or the β2 integrin LFA1, possibly in a COP9 complex-independent manner, subunit CSN5/JAB1 controls inflammatory, fibrogenic, and tumorigenic pathways [39–42]. Our study represents for the first time that the interaction between COPS5 and MIF also has been shown to functionally associate with insulin substrate receptor 1 thus raising the possibility that MIF may influence COPS5/Aβ interactions in DMPAD patients. Accordingly, MIF secretion, expression, and effect can be vital for prognosis of or even therapy for AD.
Finally, MIF has numerous other receptors and binding associates that can control its action on a cellular level. It is upregulated in NDs while its utility is far from clear. The purpose of the binding between MIF and such receptors is to prevent the proteolytic activity of enzymes, controlling the accessibility of molecules that can alter cell growth and differentiation. MIF is consequently the earliest endogenous inhibitor ever establish for protease receptors that is vital in development of CNS diseases [43].
The ultimate challenges and limitations of this study were the effort in enrolling the control group and the unpredictability of applicants withdrawing from the study, leading to a small sample size during the course of the study. We will need innovative strategies to help design ND prediction trials with feasible sample size requirements and durations of follow-up. On the other hand, there is a need for longitudinal studies with this population or use of other biomarkers to determine who is at risk of developing dementia and the results of the MIF in pre-clinical stages of the disease. A strong point of the present study was that it reflected DM as a causative disease with ND contributing to its etiology; this has often not been considered in previous research. This study aimed to fill the missing parts of this dilemma by studying the most important components involved in insulin receptor substrate 1 pathway through amelioration of AβPP that enhance MIF elevation. To our knowledge, this is the first time that these interactions have been investigated through network bioinformatics analysis.
Conclusion
Several methods are now available for diagnosis of diseases, but no method is applicable for routine examinations for pre-symptomatic patients. It is for the first time to overcome time-consuming and physician proficiencies to correlate a cytokine marker MIF level with brain neurodegeneration at the early pre-symptomatic stages in diabetic patients. Also, network computational analysis achieves effectiveness that may support MIF measurement as a potential clinically useful biomarker. A study group with MIF, AβPP, and COPS6 measurement correlated for the most promising pathway for prediction of NDs in diabetic patients is under consideration in upcoming work.