
Abstract
Background:
Traumatic brain injury (TBI) increases the risk of future dementia and Alzheimer’s disease (AD). However, it is unclear whether this is true for mild TBI (mTBI).
Objective:
To explore the association between mTBI and subsequent risk of developing AD.
Method:
We systematically searched four electronic databases from January 1954 to April 2020. We included studies reporting primary data and where mTBI preceded AD by≥5 years. We meta-analyzed included studies for both high quality studies and studies with a follow up of > 10 years.
Result:
We included 5 of the 10,435 results found. Meta-analysis found a history of mTBI increased risk of AD (pooled relative risk = 1.18, 95% CI 1.11–1.25, N = 3,149,740). The sensitivity analysis including only studies in which mTBI preceded AD by > 10 years, excluded two very large studies and resulted in wider confidence intervals (RR = 2.02, 95% CI 0.66–6.21, N = 2307).
Conclusion:
There is an increased risk of AD following mTBI. Our findings of increased risk even with mTBI means it cannot be assumed that mild head injuries from sports are harmless. The sensitivity analysis suggests that we cannot exclude reverse causation, and longer follow up times are needed. Implementation of policy to reduce mTBIs, including in children and sportsmen, are urgently needed. Further research is needed on the effect of frequency and age at injury of mTBIs.
INTRODUCTION
Traumatic brain injury (TBI) is one of twelve potentially modifiable risk factors for dementia which are estimated to account for 40% of dementia worldwide [1]. TBI is a disruption of normal brain function caused by contact to the head or a penetrating head injury [2]. Reduction in these risk factors, including TBI, may account for the 13% decline per decade seen over the last 25 years in dementia incidence in much of Europe and North America [3]. All severity TBI leads to an increased risk of dementia, and a recent systematic review and meta-analysis reported a relative risk for all cause dementia of 1.8 from midlife all severity traumatic brain injury [1, 5].
Mild TBI (mTBI) is an acute brain injury following an external force to the head, often resulting in confusion, loss of consciousness (for less than 30 min), post-traumatic amnesia, and other transient symptoms [6]. It occurs most commonly in contact sports, military activity, and as a result of domestic violence, as well as in falls and road traffic accidents [7]. It is the most common TBI, accounting for around 80% of the approximately 69 million individual all cause TBIs each year worldwide. mTBI also accounts for the majority of 1.4 million individuals seeking hospital treatment in England and Wales for TBI, although some individuals with mTBI probably do not seek treatment [8–10]. Differences in findings regarding the relationship of mTBI and dementia may be due to over 50 different mTBI definitions used prior to 2012 [11]. A recent review and meta-analysis of mTBIs and all cause dementia reported that individuals were almost twice as likely to receive a diagnosis of dementia following a mTBI but did not consider whether those people were cognitively impaired prior to the mTBI [12]. Two recent studies reported that mTBI was a risk factor for developing dementia [13, 14], but another showed that mTBIs are only associated with increased risk of dementia among older adults, suggesting that younger people may be more resilient to mTBI, or that people developing or with dementia may be more likely to have a mTBI [15]. TBI may be caused by existing cognitive impairment, as falls are at least twice as common in people with dementia as among older adults without dementia [16, 17]. Most studies of the link between mTBI and dementia include people whose falls or accidents are caused by dementia [18]. In order to address this issue of reverse causation, studies are required that assess the impact of mTBIs occurring sufficiently prior (e.g., > 5 years) to the onset of dementia.
There are contradictory findings about TBI and the risk of Alzheimer’s disease (AD) specifically, with one meta-analysis and a further, more recent study, reporting that individuals with any severity TBI had an increased risk of AD [19, 20]. In contrast, other studies have reported that risk was entirely associated with development of non-AD dementias [21, 22], or that TBI may reduce the time to onset of AD rather than increasing the general risk of AD [23, 24]. There are few studies specifically investigating the link of mTBI with AD, and a lack of clarity about whether mTBI increases the risk of AD [25]. Given the high prevalence of mTBI, even a slight increase in the risk of developing AD would have significant public health effects. In order to clarify risk from mTBI and to avoid the confound of those with mTBI in individuals with dementia at the time of injury, we conducted a systematic review and meta-analysis to quantitatively assess the nature of the relationship between mTBI and the subsequent risk of developing AD, excluding studies when mTBIs occurred less than five years before the onset of AD.
METHODS
We registered the review protocol at the PROSPERO website on May 4, 2020 (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CapRD42020177723).
Search strategy
We searched four electronic databases: Embase, Medline, PsycINFO, and Web of Science on the 2/4/2020, for papers from inception to 1954, using the following search terms with no limit on language:
AD OR Alzheimer* disease OR dementia OR major neurocognitive disorder OR memory disorder OR cognitive disorder OR neurocognitive impairment
AND
brain injury OR brain injur* OR concussion OR concus* OR TBI OR traumatic brain injury OR acquired brain injury OR head injur* OR craniocerebral trauma OR brain hemorrhage
We also screened reference lists of eligible studies to identify any other relevant studies.
Selection criteria
Studies were included if they fulfilled all the following criteria: Peer reviewed, primary research Participants met criteria for a mild traumatic brain injury (defined by the WHO) [6] included data on the time between mTBI and the presence of AD and the follow up time between mTBI and the onset of AD was≥5 years assessed Alzheimer’s disease either through clinical diagnosis or using diagnostic criteria (e.g., Diagnostic and Statistical Manual of Mental Disorders (DSM-IV, APA,1996; APA, 2013), or International Classification of Disorders (ICD-10 criteria)
Studies were excluded if they: assessed mTBI primarily in the context of significant comorbidities or confounding factors, e.g., drugs, alcohol, medication, other neurological or psychiatric illness included TBI caused by penetrating craniocerebral injury including skull fractures, or associated with oedema and brain hemorrhage were cross sectional, qualitative, or review studies focused on other forms of dementia, unless estimates of AD could be derived separately.
Data extraction
Following de-duplication, two reviewers (AG and LP) screened search results by title and abstract for relevance. They screened a random sample of 100 papers independently and calculated inter-rater reliability using Cohen’s Kappa with a predetermined satisfactory threshold of > 0.8 [26]. Full texts of relevant studies were then obtained and assessed for eligibility. If reviewers disagreed, consensus was reached through discussion or by consulting a third researcher (JH).
We extracted individual study data into tables including author, study region, study design, sample size, study participant’s baseline demographics (age, sex), the exposure (mTBI) ascertainment, outcome (AD) ascertainment, follow-up time between head injury and onset of AD, and the relative risk ratio of AD (relative risk ratios (RRs) with CIs, and factors adjusted for).
Two reviewers (AG and LP) independently assessed the overall quality of each study using the Newcastle-Ottawa Scale (NOS) designed to assess the quality of non-randomized studies for meta-analyses for cohort and case-control studies. We summarized the section ratings for each criterion into a global rating for the study. A score with a range of 0–9 was calculated for each study, and those with a score of 6 or more were considered to be high-quality studies, with those scoring below 6 considered moderate, and those scoring below 3 considered lower quality. Any discrepancies were resolved through discussion.
For cohort studies we assessed selection (representativeness of the exposed cohort, the selection of the non-exposed cohort), comparability (comparability of cohorts based on the design or analysis), and outcome (whether the follow-up was long enough for the outcomes to occur, and the adequacy of the follow up of cohorts and demonstration that the outcome of interest was not present at the start of the study). For case-control studies we considered selection (representation of cases), comparability of cases and controls (definition of controls), and exposure (quality of ascertainment of the exposure and the non-response rate).
Statistical analysis
As the type of effect estimate varies between studies, we used RRs as the common metric. Odds ratios [27] and hazard ratios [28] were converted to RRs using estimates for incidence rates from the published literature [29], as follows:
where RR is the relative risk, OR is the odds ratio, HR is the hazard ratio, and r is the incidence rate of AD at the mean age of follow up in the study.
We performed random effects meta-analyses using RevMan software version 5.3. [30] as included studies were heterogenous. We calculated pooled effect size by attributing a weight to the average effect size in each study given by the inverse of the variance of the effect estimate. Larger studies, which have smaller standard errors, therefore have more weight than smaller studies [31]. The z statistic was used to evaluate the pooled effect size. We then performed a sensitivity analysis using only the high-quality studies and a sensitivity analysis using only studies which specify a follow-up time of > 10 years.
We examined statistical heterogeneity with χ2 and I-squared (I2) tests of heterogeneity. Large I2 (> 50%) or p < 0.10 for Q-statistic suggests substantial heterogeneity among studies.
RESULTS
Study selection
Figure 1, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [32] diagram, shows the process of study selection. The initial search identified 10,435 studies after deduplication. We excluded 9,968 studies by title as they were irrelevant to the research question. Two reviewers screened 100 studies independently, with an inter-rater reliability κ=0.96. One reviewer (AG) screened the remainder of the abstracts (n = 467) and 111 full text studies, with five studies fulfilling inclusion criteria.
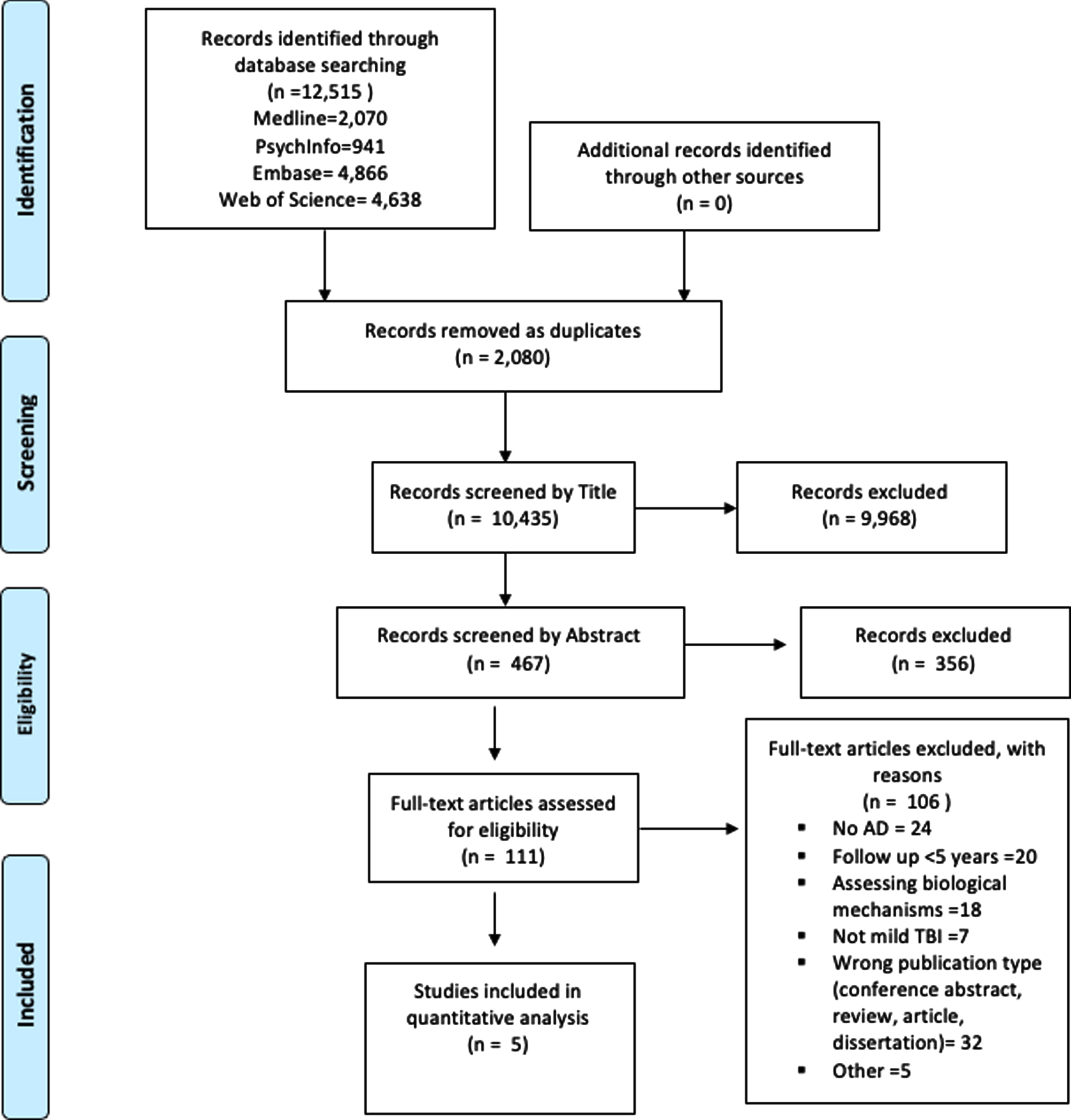
PRISMA diagram of the search strategy.
Table 1 shows study characteristics including baseline demographics, factors adjusted for, follow up duration, and relative risks. There were three cohort studies [33–35] and two case-control studies [36, 37]. Studies included data from a variety of settings, including two large sample size national register data [33, 37]. Follow up periods varied from 5 years to 53 years. The age of people at time of mTBI ranged from in their 20s to 70s, and at diagnosis mean age varied from 65 to 81. All studies included at least 260 participants. Relative risks in individual studies varied from 0.76 to 4.85.
Study characteristics, baseline demographics, factors adjusted for, follow up duration and relative risks
RR, relative risk; CI, confidence interval; AD, Alzheimer’s disease; NINCDS-ADRDA, National Institute of Neurological and Communicative Diseases and Stroke-Alzheimer Disease and Related Disorders Association; DSM-III-R, Diagnostic and Statistical Manual of Mental Disorders, third edition revised; ICD-9, International Classification of Diseases, Ninth Revision; NR, not reported. *Age refers to age at Alzheimer’s onset. **RR reported in original study or converted from published OR or HR.
Table 2 shows summary scores and ratings for risk of bias: three studies were rated as high quality and two were moderate quality.
Quality Assessment of studies
M, moderate; H, high. A score with a range of 0–9 was allocated to each study, and those with a score of 6 or more were considered to be high-quality studies.
Meta-analysis
Figure 2 shows the Forest plot with 3,149,740 participants included and a pooled RR of AD associated with mTBI = 1.18 (95% CI 1.11–1.25). I2 statistic for heterogeneity between studies was 50%, p value for the Q test = 0.09, suggesting moderate between-study heterogeneity.
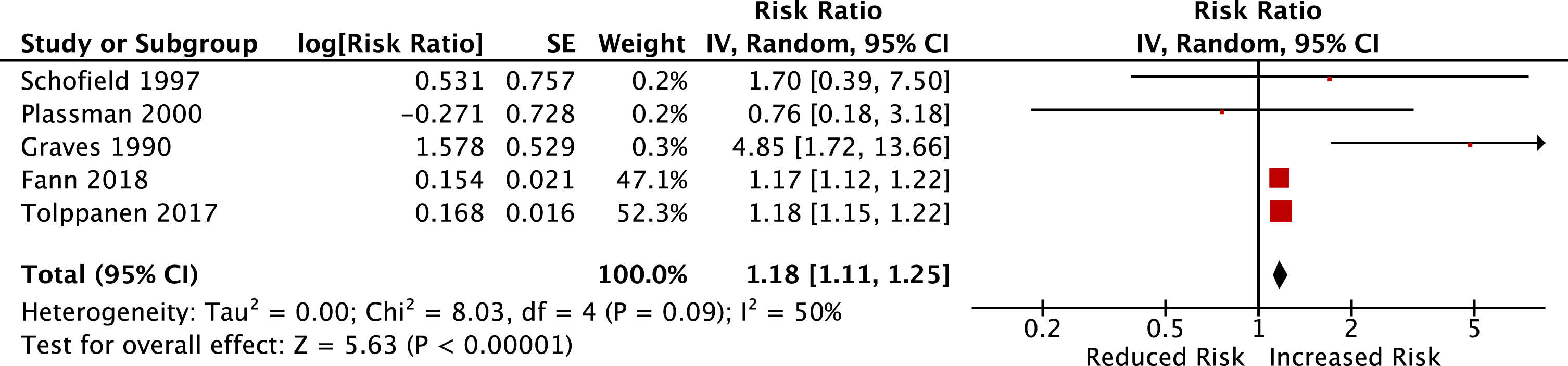
Pooled relative risk for Alzheimer’s disease, comparing individuals with mild head injury to those without head injury. Box sizes are in proportion to study weights. TBI, traumatic brain injury.
Figure 3 shows analysis using only the 3 high quality studies [33, 37] and the pooled relative risk ratio remained the same with narrower confidence intervals (1.18, 95% CI 1.15–1.21, N = 3,149,209). The I2 statistic for heterogeneity between studies was 0%, p value for the Q test < 0.001, suggesting no heterogeneity between studies.

Pooled relative risk for Alzheimer’s disease in studies rated as high quality only, comparing individuals with mild TBI to those without head injury. Box sizes are in proportion to study weights. TBI, traumatic brain injury.
Figure 4 shows analysis using only studies with follow-up times between recorded head injury and diagnosis of AD > 10 years [34–36]. This excluded the two very large studies, resulting in much smaller numbers (N = 2307). The pooled relative risk ratio is no longer statistically significant, with wider confidence intervals (RR = 2.02, 95% CI 0.66–6.21, p = 0.22, N = 2,307). The I2 statistic for heterogeneity between studies was 55%, p value for the Q test = 0.11, suggesting moderate heterogeneity between studies.

Pooled relative risk for Alzheimer’s disease in studies with a follow up time of > 10 years, comparing individuals with mild TBI to those without head injury.
DISCUSSION
To our knowledge this study is the first meta-analysis specifically examining the association between mTBI and AD. We found that mild traumatic brain injury is a risk factor for future AD, with a pooled analysis of five studies and data from more than 3 million individuals. The results demonstrate an overall 18% increase in the risk of AD, compared to people who experienced no TBIs. Previous meta-analytic reviews of case-control studies examining all severities of head injury have found an increased risk of AD, with ORs of 1.5 to 1.6 [20, 38] and that milder TBI results in less risk of future AD than more severe TBI [39]. Our study adds to the knowledge that all severities of TBI increase the risk of developing dementia [1] and clarifies that mTBI predisposes to AD, and not only to non-AD dementias. The sensitivity analysis, restricted to high quality studies, found the same relative risk as the main analysis but with narrower confidence intervals, as the overall results of the meta-analysis are driven by the findings from the larger, high-quality, homogenous studies. Further sensitivity analyses including only studies with a follow up time of > 10 years, found the same direction of relative risk, but with much wider confidence intervals, likely related to the reduced sample size.
Strengths and limitations
There are a number of strengths of the present study, the most notable of which is the effort to reduce any effects of reverse causation by excluding studies when TBIs are reported close in time to the AD diagnosis and are possibly a consequence of underlying AD rather than a contributory cause. However, one study with a mean follow-up time of 10 years and a minimum of 4 years may have had a few participants with less than 5 years follow-up [33].
Our study also included cohort studies where medical records were used to document head injuries. This means that recall bias (when informants and patients over-attribute previous head injury as they seek an explanation for developing AD [40]), and the difficulty of choosing well-matched controls with possible unknown confounding factors were removed. The primary aim in these cohorts was not to assess mTBI and AD, but we extracted specific data on both mTBI and specific AD diagnoses.
Only five studies were eligible for inclusion. Many studies were excluded due to short follow up times (< 5 years), and because of mTBIs not being separated from moderate and severe TBIs, meaning specific data could not be extracted. The results of the meta-analysis are dominated by two high quality studies due to their large sample sizes [33, 37]. Furthermore, both are of Nordic populations (Denmark and Finland respectively), and so may not be globally representative. Nonetheless, it is a strength that two very large studies, one a case-control study and one a cohort study, produce such similar results, therefore suggesting that this is a robust and replicable finding. The GRADE rating of certainty surrounding the results of the meta-analysis is moderate due to the large sample size of included studies, as well as the results withstanding the sensitivity analysis of high-quality studies. Publication bias has been limited by a number of the present studies presenting case-studies and observational data. The two large scale studies consist of analysis of national registry data. Narrow confidence intervals demonstrate the precision of the findings and boost certainty of the evidence.
The sensitivity analysis including studies with a follow up time of > 10 years produces statistically non-significant results with much wider confidence intervals. Reverse causation therefore cannot be definitively excluded from the primary analysis, which includes studies with a shorter follow up of > 5 years. It is possible that in the studies with shorter follow up durations undiagnosed early AD may have led to an increased risk of falls and mTBI, or that mTBI advances or accelerates early or pre-existing pathology. However, including studies with five or more years between injury and diagnosis of AD means it would be rare for someone in this analysis to have had dementia at the time of the mTBI. The increase in relative risk and widening of confidence intervals (RR = 2.02 (0.66–6.21)) in the sensitivity analysis is likely to be due to the removal of the two very large studies, and the remaining three studies having relatively low participant numbers, and wider confidence intervals. Of note, the Plassman paper is the only study to report a reduced relative risk, although non-significant, making it an outlier. This is perhaps due to its inclusion of military men with other physical health conditions, and the particularly long follow up time of 51–53 years [34]. This may suggest that the timing of the mTBI may be important, with mTBI during midlife or later leading to an increased risk of subsequent AD. Future research could begin to unpick whether the age at which mTBIs occur has an impact on the risk of AD. In addition, the sensitivity analysis highlights the importance of assessing longer follow-up times between TBI and diagnosis of AD to clarify whether mTBI can be considered a causal risk factor for AD.
Implications for policy and future research
An association between mTBI and AD has hugely important public health implications. For example, in informing regulations in areas in which mTBIs are common, including wearing cycling helmets and in the design of cars with air bags, seatbelts, and crumple zones. In many areas, including in Nordic countries which dominate the present study, restrictions regarding road safety are enforced by law and generally well adhered to [41]. However, three of the included studies are from the US where states have varying laws about seat belts and in which airbags became mandatory in 1998, after the time when many head injuries reported in the studies had occurred.
There is some evidence that previous professional rugby players have higher rates of mild cognitive disorders than other sporting professionals, more than 20 years after their retirement [42] and that AD can also occur in sports that involve lesser contact, like heading a ball, but in which concussion is rare [43, 44]. In one study neurodegenerative diseases, particularly AD, were almost three and a half times more common as a cause of death in former Scottish professional footballers than in controls [45]. Furthermore, mTBI has been linked to chronic traumatic encephalopathy (CTE; neurodegenerative tauopathy resulting from repeated head trauma) and dementia [46, 47]. However, there is no consensus on the clinical diagnostic criteria for CTE and it is difficult to compare with other neurodegenerative disorders [48].
The finding that mild TBIs increase the risk of AD may be explained by supposed biological causes. There are several reasons for the biological plausibility in the suggestion that TBIs may increase the risk of later AD and there have been a number of findings suggesting that head injuries may result in neurodegeneration with a similar pathogenesis to AD [49, 50]. Indeed, there is substantive evidence suggesting a number of plausible neuropathological mechanisms for this relationship such as frontotemporal lobar degeneration tau pathology, neuroinflammation, and increased Lewy bodies [51, 52]. However, as assessments of AD within the included studies were made on a clinical basis, but without an autopsy confirmation, a clinical diagnosis of AD may be reflective of alternative neuropathological changes including CTE. Similar tauopathy found in AD has been observed in postmortems following TBI and CTE, suggesting a similarity in the neuropathology [53].
Potential restrictions on sporting activities that may result in mTBIs (such as contact sports or riding a bicycle) might reduce head injuries; however. benefits of such activities are important. Physical inactivity is also a risk factor for dementia [54], and physical activities and sports serve to boost cardiovascular health [55]. A reduction in such activities may counteract these benefits and a careful weighing up of these factors is needed. Therefore, policy should consider reducing risk within these sports, for example by not allowing children to head balls and mandating helmet wearing, rather than a blanket ban on any contact sports. Our findings of increased risk even with mTBI means it cannot be assumed that lesser and frequent head injuries from sports are harmless. An increasing awareness of the chronic neurologic sequalae of repeated mild head injuries is evident, for example, in the decision by the Scottish Football Association to ban heading practice in football for children [56] and in the Industrial Injuries Advisory Council issuing a call for new evidence on neurodegenerative disease in professional sportspersons in 2014 [57]. In the US, management of concussion is taught in all schools and other countries should consider adopting this policy not just for sports, but for all concussion injuries [58].
The majority of research has addressed risk factors for dementia in high income countries; however, most dementia is in low- and middle-income countries (LMIC) [59]. The frequency of potentially modifiable risk is higher in those countries so addressing these factors in LMIC may lead to greater prevention of dementia [60]. This is of particular importance as there is a greater burden of TBI in South East Asia and the Western Pacific subregion [8]. Furthermore, the common mechanisms behind TBIs vary across countries. Therefore, in order to reduce mTBIs globally, there is a need to review regulations with regards to the specific country.
In addition, future research could begin to unpick whether the age at which mTBIs occur has an impact on the risk of AD. Interestingly, the study with some of the youngest participants and the longest follow up time of all included studies, was the only study to find no evidence that mTBIs increase the risk of AD [34]. The interaction between mTBI and other known risk factors is also important. For example, while people who play professional sports may drink less, approximately 65% of head injuries occur following the consumption of alcohol, also increasing the risk of AD [61]. Therefore, examining the interaction between mTBI and other risk factors for AD is an important area for future research.
The present study enables understanding and recognition of the importance of mTBIs but does not help understand the impact of the very mildest TBIs, that are not seen in hospitals. Further research to identify the risk of AD and other dementias following very mild TBI is difficult. Within the WHO definition of mTBI there also remains a significant range from mild transient confusion to loss of consciousness of up to 30 minutes. Furthermore, due to the lack of data on repeated mTBIs, the present study did not allow for an assessment of whether the frequency of mTBIs can further increase the risk of AD. There are challenges with identifying very mild TBIs and categorizing the exact number of mTBIs for research purposes; however, it would be useful to categorize individuals as those who have been subject to many mTBIs (e.g., through contact sports) from those individuals who have had a single mTBI or have never had a TBI, to identify if repeated mTBIs further increases risk of AD.
In summary, the present study importantly finds evidence of an association between mTBI and the risk of future AD with an 18% increase. Some of the head injuries and subsequent AD occurs at a relatively young age so people may lose many years of healthy life. As mTBI is common, reducing the number of mTBIs may be influential in reducing the risk of AD. Our findings of increased risk even with mTBI means it cannot be assumed that mild head injuries from sports are harmless. We agree with recent recognition of the importance of preventing mTBI in sport [57, 58], for example by wearing helmets and reducing heading of balls. More research, particularly in LMICs, is needed to specify the relationship between mTBI and AD in other countries, the frequency of mTBIs, and the interaction with other risk factors.
Footnotes
ACKNOWLEDGMENTS
This review did not receive any specific funding. JH is funded by a Wellcome Clinical Research Career Development Fellowship. This research was funded in whole, or in part, by the Wellcome Trust [Grant number 214547/Z/18/Z]. For the purpose of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission. GL is supported by University College London Hospitals’ National Institute for Health Research (NIHR) Biomedical Research Centre, North Thames NIHR Applied Research Collaboration, as an NIHR Senior Investigator.