
Abstract
Background:
Moderate- to vigorous-intensity physical activity (PA) may reduce the risk of dementia; however, few studies have examined the effects of PA intensity on dementia risk.
Objective:
To prospectively examine the dose-response relationship of PA intensity with the incidence of suspected dementia in community-dwelling older adults.
Methods:
We conducted a baseline mail survey with an 8-year follow-up of 3,722 older adults in Japan. We assessed PA levels using the International Physical Activity Questionnaire short form and calculated the amount of time per week spent performing moderate- and vigorous-intensity PA (VPA). Information regarding suspected dementia was obtained from the city database during the follow-up period. Cox proportional-hazard models with age as time scale, and delayed entry and restricted cubic spline regression as variables were used to estimate risk of developing suspected dementia, excluding cases occurring < 1 year after baseline evaluation.
Results:
The cumulative incidence of suspected dementia during the follow-up period was 12.7%. Compared with those who did not practice moderate-intensity PA (MPA), those who practiced≥300 min (hazard ratio, 0.73; 95% confidence interval 0.56–0.95) of MPA showed a lower risk of developing suspected dementia. Furthermore, when the dose-response relationship was examined, the hazard of developing suspected dementia decreased almost linearly with MPA. A significantly lower hazard was observed from 815 minutes/week. There was no significant association between VPA and suspected dementia.
Conclusion:
This study suggested that MPA is often practiced in older adults and this PA intensity has a sufficiently favorable effect on dementia prevention.
INTRODUCTION
Currently, there are 46.8 million people living with dementia worldwide, with this number estimated to increase to 131.5 million by 2050 [1]. Dementia severely affects the functioning and quality of life of patients [2] and imposes a heavy burden on caregivers [3]. In addition, the worldwide economic costs associated with dementia are enormous, estimated to be $818 billion in 2015 [4]. Since there are no established treatments for reversing dementia, it is important to prevent this disease by targeting modifiable factors that can suppress incident dementia [5].
Several meta-analyses have reported that physical activity (PA) can effectively reduce the risks of dementia and cognitive decline [6–8]. Additionally, the World Health Organization (WHO) recommends the performance of moderate-intensity PA (MPA) for at least 150 minutes per week or vigorous-intensity PA (VPA) for at least 75 minutes per week to reduce the risk of cognitive decline in adults aged 65 years and above, which corresponds to at least 600 metabolic equivalents (MET)-minutes/week [9]. However, more detailed knowledge is necessary regarding the appropriate level of PA to prevent incident dementia in older adults. Indeed, the lack of studies examining the effects of different PA intensities on incident dementia has been criticized [10, 11].
Exercise has been reported to increase the level of brain-derived neurotrophic factor, an important factor related to neuroplasticity [12]. This increase varies with exercise intensity and is more pronounced with moderate-intensity exercise than with vigorous-intensity exercise [13–15]. In addition, in observational studies focusing on PA intensity, most studies have reported that MPA is favorably associated with incident dementia [16, 17], while there are no consistent findings for VPA [16–18]. Therefore, it is necessary to examine the relationship between PA intensity and incident dementia.
Furthermore, the shape of the dose-response relationship between PA and incident dementia is unclear. A previous study found a dose-response relationship between leisure-time PA and the risk of developing all-cause dementia and Alzheimer’s disease (AD). However, the authors also reported that the AD risk curve tended to flatten at 1,000 kcal/week [19]. Dupré et al. [20] found an inverse, J-shaped association between household/transportation activity level and the risk of dementia. The shape of the dose-response relationship between MPA and VPA and the incidence of dementia remains unclear, and clarification of this shape is needed to effectively prevent dementia through PA. Therefore, the purpose of this study was to examine the dose-response relationship of PA intensity with the incidence of suspected dementia in community-dwelling older adults.
MATERIALS AND METHODS
Study design
The baseline survey was conducted in June 2013 as an inventory mail survey that targeted community-dwelling older residents (age≥65 years) of Kasama City, Ibaraki, Japan. We mailed all eligible older residents who had not received long-term care insurance [21]. This study complied with the guidelines of the Declaration of Helsinki. The survey’s purpose and data use for research were explained in a document, and informed consent was assumed with the voluntary return of the questionnaires. The Ethics Committee of the University of Tsukuba approved this study (Ref. No. Tai 26-31 and 020-142).
Supplementary Figure 1 shows the flow of participants in this study. Self-reported questionnaires were sent to 16,870 older adults and returned by 10,339 individuals (response rate, 61.3%). Of these respondents, 534 were excluded because they had dementia or stroke before the baseline survey. A further 6,017 respondents were excluded due to incomplete data. An additional 31 respondents who developed dementia less than 1 year after the baseline survey were also excluded. Finally, respondents lacking 1-year follow-up data due to death (n = 25) or moving to another city (n = 10) were also excluded. Ultimately, 3,722 participants were included in the analysis (response rate, 22.1%). These participants were followed up using the municipal database until they developed dementia, died, moved to another city, or until the end of the follow-up period (July 2021).
Ascertainment of dementia
The outcome of this study was the incidence of suspected dementia, which was determined using the dementia scale on the long-term care insurance certification, which is fair, efficient, and nationally standardized in Japan [22]. This dementia scale stratifies cognitive decline utilizing the ranks I, II, III, IV, and M. A higher rank (e.g., M) is associated with a lower level of independence and a stronger need for caregiver support. More detailed explanations can be found in other studies [21, 23]. This study was defined as rank II or higher and rank M was considered the incidence of suspected dementia [23, 24]. Rank II includes symptoms/behaviors, communication difficulties, or both that can hinder some daily activities, but independence is maintained with minimal assistance. In previous studies, this dementia scale was well correlated with Hasegawa’s dementia scale (Spearman’s rank correlation coefficient ρ= –0.73) and the Mini-Mental State Examination (ρ= –0.74) [25] and is in accordance with the clinical dementia rating scale [26].
Assessment of PA
We assessed the performed volume of PA at baseline, which was evaluated using the Japanese version of the International Physical Activity Questionnaire (IPAQ) short form [27]. Participants were asked to report the frequency and duration of three types of PA performed in bouts of≥10 minutes in a usual week, including walking corresponding to 3.3 MET, MPA (e.g., carrying light loads, swimming at a slow pace, or playing doubles tennis) corresponding to 4.0 MET, and VPA (e.g., carrying heavy loads, running, cycling up a hill, or playing single tennis) corresponding to 8.0 MET. Total moderate- to vigorous-intensity PA (MVPA) was calculated as the sum of these types of PA. In addition, MPA, including walking, was measured. Based on the PA duration recommended by the WHO, the durations of MPA (0, 10–149, 150–299, ≥300 minutes/week), VPA (0, 10–74, 75–149,≥150 minutes/week), and total MVPA (0, 33–599, 600–1,199,≥1,200 MET-minutes/week) were divided into four categories [9].
Covariates
Using baseline questionnaires, covariates were assessed, including age, sex, educational level (compulsory education, high school, or college/junior college), subjective economic status (very poor/poor, normal, or very good/good), living alone (yes or no), body mass index (BMI; underweight: ≤18.4 kg/m2, normal weight: 18.5–24.9 kg/m2, or overweight: ≥25.0 kg/m2), medical history (hypertension, dyslipidemia, diabetes, heart disease, and arthralgia/neuralgia), sleep duration (≤5.9, 6.0–8.9, ≥9.0 hours/day), television viewing (hours/day), depressive mood, and subjective memory complaints. BMI was calculated using self-reported height and weight.
In this study, the mood and cognitive function domains of the Kihon checklist were used to assess depressive mood [28] and subjective memory complaints [28, 29], respectively. The Kihon checklist consists of binary (yes or no) answers. Five items were summed to assess depressed mood, with higher values indicating worse depressive symptoms (range: 0–5 points). Depression, which is a well-known predictor of dementia [30, 31] and is also associated with PA [32, 33], was treated as a covariate in this study. The cognitive function domain of the Kihon checklist is composed of three items: “Do your family or friends point out your memory loss?”, “Do you make a call by looking up phone numbers?”, and “Do you find yourself not knowing today’s date?”. The three items were summed (range: 0–3 points), with a higher score indicating more significant memory complaints. Because this index can moderately predict incident dementia [29], it may be useful for adjusting for the baseline cognitive status of participants. For analysis, participants were divided into three categories by their subjective memory complaints score (0, 1, 2–3 points).
Statistical analysis
To compare the baseline characteristics by total MVPA levels, we performed chi-squared tests for categorical variables, Kruskal–Wallis tests for PA variables, and analyses of variance for other variables. We generated Kaplan–Meier curves for each type of PA and incidence of suspected dementia and performed the log-rank test. In this analysis, the dependent variable was the incidence of suspected dementia over a period of 8.16 years, excluding cases of suspected dementia occurring < 1 year after the start of the follow-up period, as mentioned previously. The independent variables included each PA category. Additionally, to examine the independent relationship between level of PA and the risk of developing suspected dementia, multivariable-adjusted Cox proportional-hazards regression analysis was performed with age as the time scale with delayed entry [34] to address the differences in dementia cases according to the status of covariates and PA by age. The hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated by two multivariable-adjusted models. The covariates of Model 1 included sex, educational level, subjective economic status, living alone, BMI, hypertension, dyslipidemia, diabetes, heart disease, arthralgia/neuralgia, sleep duration, television viewing, depressive mood, and subjective memory complaints. In Model 2, MPA and VPA were entered simultaneously into Model 1 to adjust for their effects as covariates on each other. Restricted cubic spline curves were generated to examine the adjusted dose-response relationships between each type of PA and the incidence of suspected dementia. For each type of PA, the reference value was set to 0. Different knots (3–5) were tested based on Harrell’s recommendations [35], and the Akaike information criterion (AIC) and Bayesian information criterion (BIC) were used for selecting the number of knots. The number of knots was set to three based on the best balance of AIC and BIC, and knots were placed at the 10th, 50th, and 90th percentiles in each PA type except VPA; the spline curve of VPA could not be analyzed due to its low practice rate.
As supplementary information, characteristic differences between the included and excluded cases were examined. In addition, because some studies treated walking of older adults as light intensity (2.5 MET) [27, 36], dose-response relationships of suspected dementia with walking, with MPA without walking, and with total MVPA without walking were also investigated using a previously described method.
Statistical analyses were performed using Stata 17 software (STATA Corp., College Station, TX, USA). The level of statistical significance was set at a p-value of < 0.05.
RESULTS
Supplementary Table 1 presents the comparisons of characteristics between the included and excluded cases due to incomplete data. Excluded individuals were more likely to have older age, lower education, higher depressive mood, and lower total MVPA than included participants.
Supplementary Figure 2 shows the distribution of follow-up period durations among the participants. The 3,722 participants in this study contributed a total of 27,475 person-years. The mean follow-up duration was 7.38±1.70 years and the median follow-up duration was 8.16 years. The total sample included 471 (12.7%) individuals with suspected dementia, with incidence of 17.1 people per 1,000 person-years. Table 1 shows the baseline characteristics of participants by total MVPA levels. At baseline, the mean age was 73.0±6.0 years, and 53.6% of them were male. Among the participants, 423 (11.4%), 439 (11.8%), 497 (13.4%), and 2,363 (63.5%) individuals performed 0, 33–599, 600–1,199, or≥1,200 MET-minutes/week of total MVPA, respectively. Significant group differences were found in terms of age, sex, educational level, subjective economic status, BMI, hypertension, dyslipidemia, arthralgia/neuralgia, sleep duration, television viewing, depressive mood, subjective memory complaints, walking, MPA, VPA, and total MVPA.
Baseline characteristics of participants by physical activity levels
Values are numbers (percentages) unless stated otherwise. p-values for differences between groups were calculated using chi-squared tests for categorical variables, Kruskal–Wallis tests for physical activity variables, and analyses of variance for other variables. aSince the International Physical Activity Questionnaire only evaluates≥10 minutes of consecutive physical activity, the minimum value is 33 MET-min/week when the participants only performed the minimum time of walking (intensity: 3.3 MET). IQR, interquartile range; M, mean; Mdn, median; MET, metabolic equivalents; MVPA, moderate- to vigorous-intensity physical activity; SD, standard deviation.
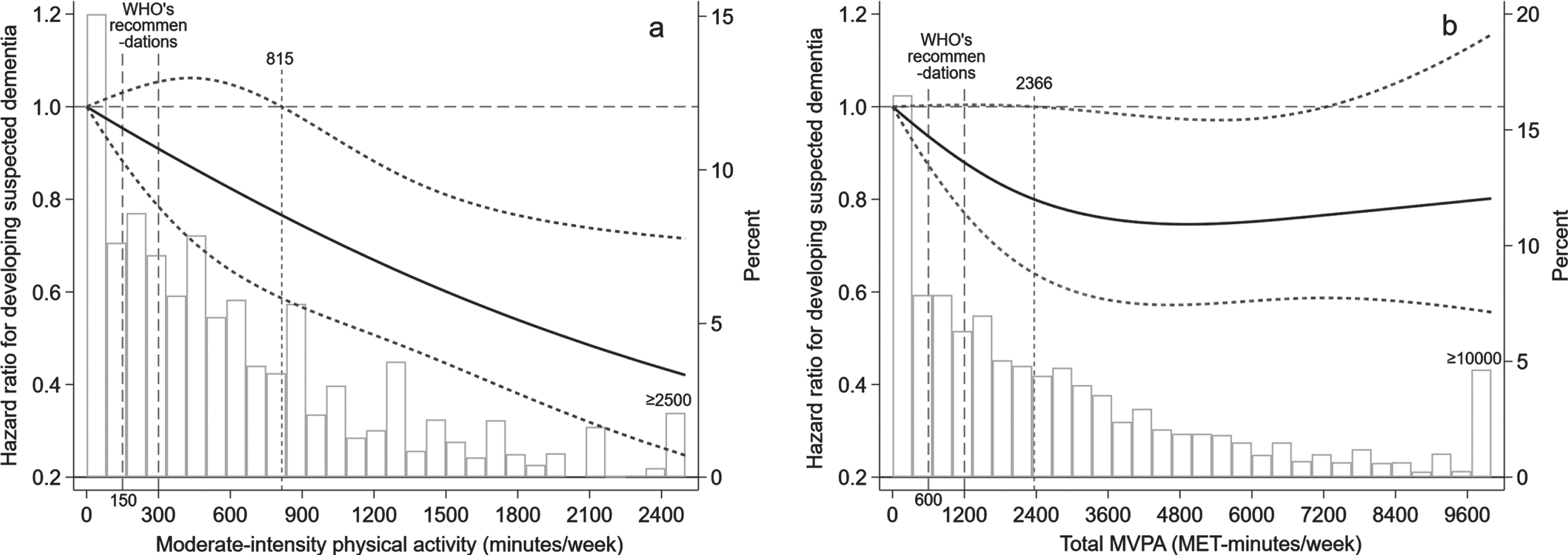
Cubic spline regressions for developing suspected dementia by (a) moderate-intensity physical activity and (b) total MVPA levels. Age was treated as the time scale with delayed entry. Each model was adjusted for sex, educational level, subjective economic status, living alone, body mass index, hypertension, dyslipidemia, diabetes, heart disease, arthralgia/neuralgia, sleep duration, television viewing, depressive mood, and subjective memory complaints. For (a) moderate-intensity physical activity, vigorous-intensity physical activity was also adjusted. The solid lines represent hazard ratios, and the dashed lines represent 95% confidence intervals. The activity time distribution is represented by histograms in the background. MET, metabolic equivalents; MVPA, moderate- to vigorous-intensity physical activity; WHO, World Health Organization.
Figure 1 shows the Kaplan–Meier curves for developing suspected dementia based on PA levels in the crude model. The log-rank test showed a significant difference between MPA and total MVPA (p < 0.001). The results of Cox proportional-hazards regression analysis for relationships between the PA levels and developing suspected dementia are shown in Table 2. Compared with those who did not practice MPA, performing≥300 minutes/week (HR: 0.73; 95% CI: 0.56–0.95) had a significantly lower risk of developing suspected dementia in model 2. However, VPA was not significantly associated with developing suspected dementia. For total MVPA, participants who practiced≥1,200 MET-minutes/week (HR: 0.75; 95% CI: 0.58–0.97) had a significantly lower risk of developing suspected dementia than those who did not practice total MVPA.
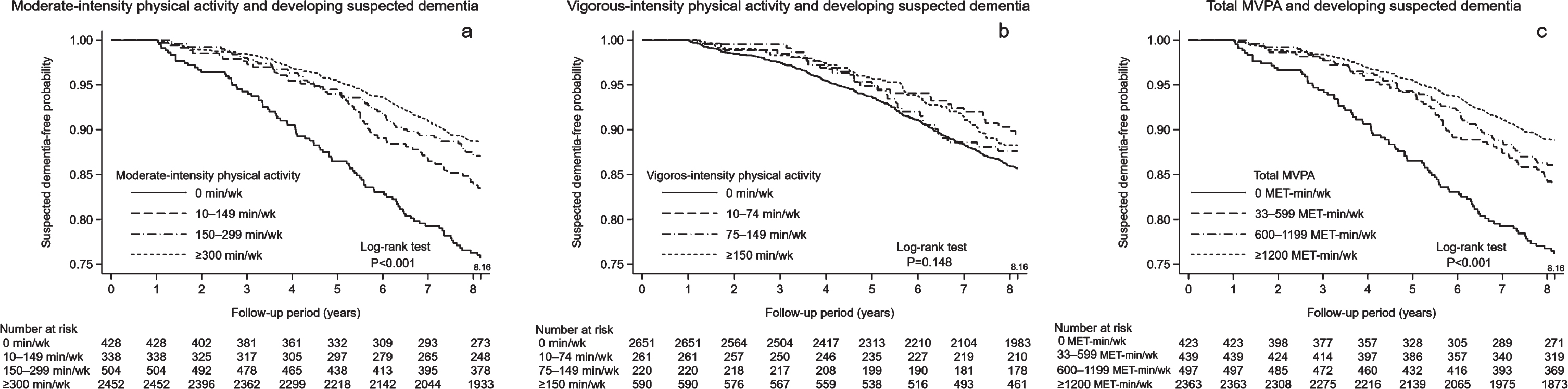
Kaplan–Meier curves for developing suspected dementia by (a) moderate-intensity physical activity, (b) vigorous-intensity physical activity, and (c) total MVPA levels. The survival probability values were obtained from the Kasama Study, with a mean follow-up period of 7.38 years (they excluded those who developed suspected dementia < 1 year after follow-up initiation). p-values are for log-rank tests examining whether the four different Kaplan–Meier curves significantly differed. MET, metabolic equivalents; MVPA, moderate- to vigorous-intensity physical activity.
Hazard ratios of developing suspected dementia by physical activity levels
aAge was treated as the time scale with delayed entry in each Cox proportional-hazards model. bIncluding walking. cAdjusted for sex, educational level, subjective economic status, living alone, body mass index, hypertension, dyslipidemia, diabetes, heart disease, arthralgia/neuralgia, sleep duration, television viewing, depressive mood, and subjective memory complaints. dAdditional adjustment of Model 1 for the other intensity type (moderate/vigorous) of physical activity. Boldface indicates statistical significance (p < 0.05). MET, metabolic equivalents; MVPA, moderate- to vigorous-intensity physical activity, PA, physical activity.
We also assessed the dose-response relationship between each PA level and the risk of developing suspected dementia by drawing restricted cubic spline graphs (Fig. 2). MPA showed an almost linear dose-response relationship with dementia, and MPA volumes of≥815 minutes/week were associated with a significantly lower hazard of developing suspected dementia. Total MVPA showed a decreasing hazard until approximately 3,600 MET-minutes/week, which subsequently plateaued. Furthermore, a significantly lower hazard of developing suspected dementia was observed from a volume of 2,366 MET-minutes/week.
Supplementary Figure 3 presents cubic spline curves for walking, for MPA without walking, and for total MVPA without walking. Although a relationship with a decreasing hazard of developing suspected dementia was likely to be present for each increased walking, increased MPA without walking, and increased total MVPA without walking, the 95% CIs for walking and total MVPA without walking were consistently over 1.0. For MPA without walking, there was a significantly lower hazard of developing suspected dementia from 450 minutes/week.
DISCUSSION
In this cohort study, we examined the relationship of MPA and VPA with developing suspected dementia in community-dwelling older Japanese adults. We found a significant negative relationship between MPA and developing suspected dementia, with cubic spline regression indicating a significant dose-response relationship between these two. Although the hazard of developing suspected dementia decreased almost linearly with MPA, no significant association was found between VPA and developing suspected dementia. The findings from this study could enhance our knowledge about the prevention of dementia by PA.
In this study, we confirmed a negative dose-response relationship between MPA and the risk of developing suspected dementia. Our results support those of previous studies showing that MPA is associated with a lower risk of developing vascular dementia [16] and AD [17]. Although WHO recommends that performing MPA for at least 150 minutes/week could help reduce cognitive decline in older adults [9], the same volume in the cubic spline analysis did not indicate a significant association. However, ≥815 minutes/week of MPA had a significant preventive effect on dementia. Similarly, total MVPA indicated a significantly lower hazard of developing suspected dementia from 2,366 MET-minutes/week. A meta-analysis of studies using the Global Physical Activity Questionnaire reported that MVPA improves health until 3,600 MET-minutes/week and that MVPA needs to be several times higher than the WHO’s minimum level of recommendation (i.e., 600 MET-minutes/week) in order to further reduce the risk of developing several diseases, including diabetes, ischemic heart disease, and ischemic stroke [37]. Our study supports this meta-analysis and suggests that a higher volume of PA than the WHO’s recommendation level is needed to prevent dementia in older adults effectively.
As supplementary information, walking, MPA except walking, and total MVPA except walking examined them in association with developing suspected dementia. In this analysis, a significant dose-response relationship was confirmed for MPA without walking. In a previous study that examined the type of exercise and cognitive decline, the practice of walking was not found to prevent cognitive decline, but the practice of calisthenics suppressed cognitive decline [38]. Netz suggests that physical training (e.g., walking) and motor training (e.g., tai chi), which is a type of coordinated exercise, have different pathways of influence on cognitive function [39]. Furthermore, a meta-analysis that examined the effects of exercise interventions on cognitive function reported that coordinated exercise was more effective for preserving cognitive function than endurance or resistance exercise [40]. Since this study could not investigate the specific content of MPA, it will be necessary to focus on the type of PA in future studies.
Although there were different associations between developing suspected dementia and MPA with or without walking, as mentioned above, the important finding is that MPA, including walking, was strongly associated with a lower risk of developing suspected dementia among the PA variables. This is useful information for achieving feasible PA changes in older adults because MPA including walking is easier to practice than VPA. Of the participants, 20.6% did not perform≥150 minutes of MPA per week, including walking, and 11.5% were non-practicing. In Japan, “+10,” which signifies “an additional 10 minutes of PA per day,” is recommended [41], and further dissemination of this message is expected to reduce the incidence of dementia.
This study did not detect a significant association between VPA and the risk of developing suspected dementia, whereas a cubic spline analysis for VPA was not conducted because of its lower practices. In this study, only 21.8% of the participants practiced VPA for≥75 minutes/week and the median of VPA was 0 minutes/week even in the highest total MVPA group. The low practice rate could make valid analysis difficult for VPA. Similar to this study, previous studies, which focused on the effect of PA intensity on dementia, have also reported a lower practice rate of VPA in older adults and did not detect a significant association between VPA and dementia [16, 42]. Although one study confirmed the significant preventive effect of VPA on dementia, this study has a limitation of VPA assessment that was evaluated as a single assessment of PA and was not evaluated separately from other PA intensities [18]. This study used the short form of the IPAQ for assessing PA and evaluated absolute PA intensity even in older adults. However, a guideline for PA suggested that relative intensity is a better guide for older adults than absolute intensity because older adults generally present a decreased aerobic capacity compared with younger adults [43]. As this guideline suggested, evaluating the relative intensity of VPA corresponding to individuals’ aerobic capacity may be needed to clear the effect of VPA on dementia in older adults.
Several potential mechanisms have been proposed to explain the role of PA in incident dementia. First, PA has been reported to affect other risk factors for dementia, including hypertension [44], type 2 diabetes [45], and depression [46]. Second, it has been reported that exercise increases the production of new neurons and neurotrophic factors in the hippocampus [47]. Third, it has been reported that improving mood through exercise may increase cerebral blood flow and enhance cognitive function [48, 49]. Fourth, animal studies have shown that PA reduces the accumulation of amyloid-β and tau proteins in the brain, which are pathological features of AD [50].
The strength of this study was the high follow-up rate over 8 years in a large sample size, which allowed us to determine the dose-response relationship between PA variables and dementia using cubic spline curves. However, this study also had several limitations. First, over the relatively short follow-up period (8 years), a lower level of PA may have been an early symptom of dementia rather than a premorbid risk factor [51]. To consider this potential inverse causal problem, we adjusted for subjective memory complaints at baseline and excluded those prospective participants who developed dementia less than 1 year after the baseline evaluation. However, our results may partially reflect the early behavioral changes associated with dementia. Second, the dementia assessment used in this study was not a clinical diagnosis and did not consider the causes of dementia. Dementia determination by the long-term care insurance system has the advantage of securing a large sample; however, the causes of dementia cannot be determined, and some misclassification may have occurred in the dementia assessment in this study. Previous studies reported that the effects of PA on the incidence of dementia depend on the cause of dementia [8, 19]. Therefore, future studies should use clinical diagnosis to determine dementia. Third, PA was assessed using the short form of the IPAQ. Although self-reported PA is susceptible to recall bias and social desirability bias, it is considered a reasonable method for collecting data related to PA for epidemiologic studies [52]. Additionally, the IPAQ short form does not assess low-intensity PA (LPA) (≤2.9 MET). Because a previous study reported that accelerometer-measured LPA was positively associated with total brain volume [53], including LPA data is necessary to enhance validity and expand knowledge. To resolve the limitation of assessing PA, assessing by more accurate measurement such as accelerometry (which can assess variety of intensity of human movement) is required. Fourth, the type of PA could not be evaluated in this study. Rovio et al. reported that work-related PA was not sufficient to protect against dementia [54]. In addition, Dupré et al. reported that the 5-year risk of dementia was significantly and negatively associated with the level of household/transport activity but not with leisure or sports activities in individuals aged≥72 years [20]. Therefore, it is necessary to consider not only the intensity of PA but also the type of activity in the future. Finally, a selection bias may have affected the results because the excluded individuals had older ages and a poorer health status than included participants. Therefore, our findings could be reflected in a healthy population, and the generalizability of our findings for other populations is uncertain.
In conclusion, we found that community-dwelling older adults who performed more bouts of MPA had a lower risk of developing suspected dementia, even after adjusting for covariates. In restricted cubic spline regression, MPA showed an almost linear inverse dose-response relationship with developing suspected dementia, and a significantly lower hazard was observed from 815 minutes/week. For VPA, a significant association was not detected in this study and cubic spline analysis could not be conducted because of its lower practices. Further research should focus on the relative intensity of VPA corresponding to individuals’ aerobic capacity to clear the effect of VPA on dementia in older adults, rather than assessing absolute PA intensity as in the younger population. Although this study has several limitations, our findings suggested that MPA is often practiced by older adults and this level of PA intensity has a sufficiently favorable effect on dementia prevention. This study’s findings have utility for creating feasible clinical recommendations to reduce dementia risk in this population.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the study participants and Kasama city officials for their cooperation. This study was supported by a Grant-in-Aid for Young Scientists (B) (26750348) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan and a grant from the Meiji Yasuda Life Foundation of Health and Welfare. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.