
Abstract
Background:
Available evidence on the association of physical activity (PA) or sedentary behavior with cognitive decline is inconclusive.
Objective:
To assess the association between an active lifestyle score and leisure-time physical activity (LTPA) and changes in cognitive function in the Seguimiento Universidad de Navarra (SUN) prospective cohort.
Methods:
Cognitive function was evaluated in a subsample of 806 participants of the SUN cohort study using the validated Telephone Interview for Cognitive Status-modified (STICS-m) questionnaire at baseline and after 6 years. LTPA was evaluated with a previously validated 17-item self-administered questionnaire and with information on sedentary lifestyles. We also calculated a multidimensional 8-item PA score. Multivariable linear regression analysis evaluated the association between PA and changes in cognitive function and its interaction by APOE genotype.
Results:
Mean age of participants was 66 (SD 5.3) years and 69.7% were male. When stratifying by APOE variants, no significant associations between the active lifestyle score or LTPA and changes in cognitive performance over time were found among APOE ɛ4 carriers. However, we observed that a higher adherence to an active lifestyle (high versus low PA score β= 0.76 95% CI 0.15,1.36; p trend = 0.011) and a high LTPA (Q4 versus Q1 β= 0.63; 95% CI –0.01,1.26; p trend = 0.030) were associated with more favorable changes in cognitive function over time among APOE ɛ4 non-carriers with statistically significant interactions in both cases (p for interaction = 0.042 for PA score, and p = 0.039 for LTPA).
Conclusion:
The results of the present study suggest that an active lifestyle is associated with a better status of cognitive function over time only among APOE ɛ4 non-carriers.
INTRODUCTION
Globally, around 44 million persons were living with dementia in 2016 [1]. According to the World Health Organization, this number is projected to increase to 75.6 million people by 2030 and to 135.5 million people by 2050 [1].
Alzheimer’s disease (AD) is the most common cause of dementia, accounting for 60% to 80% of all dementia cases [1]. The pathophysiological process of AD is thought to begin many years before the diagnosis of AD dementia. This long “preclinical” phase of AD would provide a critical opportunity for therapeutic intervention [2]. Although no disease-modifying treatment for any dementia is available, a delay in the onset of dementia would benefit even the oldest adults [3]. With age being the single biggest non-modifiable risk factor for dementia and given the lack of effective pharmacological treatment, several modifiable lifestyle factors have been identified and shown their potential beneficial effects in slowing cognitive decline [4]. Non-modifiable risk factors for AD also include the apolipoprotein E gene allele ɛ4 (APOE ɛ4), the major genetic risk factor for late-onset AD [5]. In the Spanish population, the APOE ɛ4 estimated frequency is 0.104, lower than those reported for Northern European populations, but similar to other South-European populations [6].
The Lancet Commission on dementia prevention, intervention, and care suggests that around 40% of dementia is attributable to a combination of the following twelve risk factors: education to a maximum of age 11–12 years, midlife hypertension, midlife obesity, hearing loss, late life depression, diabetes, physical inactivity, smoking, social isolation, excessive alcohol consumption, head injury and air pollution [7]. The Committee on Preventing Dementia and Cognitive Impairment of the National Academy of Sciences [8] also underlined the potential beneficial effects of lifestyle factors in preventing or delaying dementia.
Physical inactivity is associated with numerous diseases, including type 2 diabetes, cardiovascular di-sease (CVD), and breast and colon cancers, being the fourth leading risk factor for global mortality [9]. In general, accumulating research evidence from epidemiological, cross-sectional, and neuroimaging studies shows that physical activity (PA) is associated with benefits for cognitive health; however, evidence from randomized controlled trials (RCTs) is less consistent [10]. Otherwise, information about the relationship between sedentary behaviors and cognition is limited [11]. While preliminary evidence suggests that sedentary behaviors are associated with lower cognitive performance, the reported magnitude of this association is inconsistent [11]. For example, it is unclear whether reducing sedentary behavior is more beneficial for long-term cognitive health than increasing PA. Only a few longitudinal studies addressed the effects of both PA and sedentary behavior on cognition [11].
The aim of this study was to assess the association between a score of adherence to an active lifestyle and leisure-time physical activity (LTPA) and changes in cognitive function over a 6-year follow-up period in a prospective cohort of university graduates, the Seguimiento Universidad de Navarra (SUN) Project, according to the APOE ɛ4 haplotype.
MATERIALS AND METHODS
Study population
The SUN Project is a prospective, dynamic, cohort study, which started in December 1999 and currently includes more than 22,000 Spanish university graduates. Its aim is to assess the association between PA, diet, and other lifestyles with chronic diseases and mortality. The study design, methods and cohort profile have been previously reported in detail elsewhere [12].
Until May 2008, a total of 19,919 participants had completed the baseline questionnaire. Out of these, 1,921 participants over 55 years old were invited to participate in a sub-study designed to evaluate the effect of PA, dietary, and environmental factors in the development of cognitive impairment. A subsample of 1,069 agreed to participate.
For the present analysis, we excluded 145 participants without follow-up visit after 6 years, 1 participant due to implausible Spanish version of the modified Telephone Interview of Cognitive Status (STICS-m) (the change in score was greater than 4 standard de-viations), 103 participants who did not provide the saliva sample to determine the APOE gene or were not correctly genotyped, and 14 participants who re-ported values of energy intake outside of predefined values (1st–99th percentiles). The resulting final sample size was 806 participants (Fig. 1).
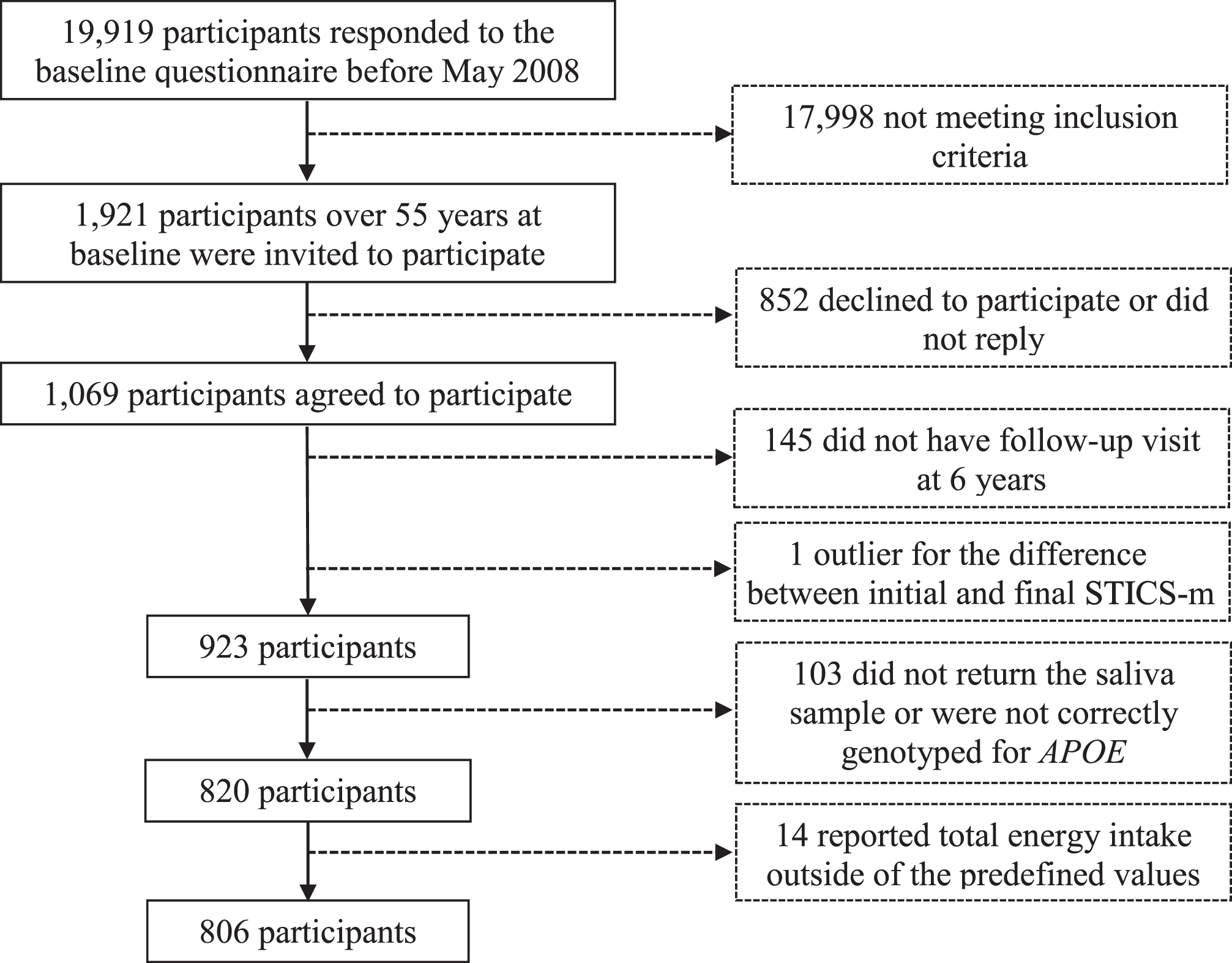
Flow-chart of participants in the Seguimiento Universidad de Navarra.
Cognitive function assessment
Cognitive function was assessed with the validated STICS-m [13]. The questionnaire was administered over the phone at baseline, and at 6 years of follow-up. The STICS-m is composed by 11 items with a maximum score of 41. It assesses four cognitive domains: orientation, memory, attention/calculation, and language.
A total of 14 subjects at baseline and 1 subject at the 6-year follow-up showed missing data for some of the items in the STICS-m (n = 13 with 1 item missing, n = 1 with 2 items missing, n = 1 with 3 items missing). These missing values were imputed based on the participants’ sex and age, the attained scores in the other items in the questionnaire, and the attained scores for the item in the 2 years and 6 years follow-up questionnaires for subjects with missing data in the baseline questionnaire, and in the baseline and 2 years follow-up questionnaires for those with missing data in the 6 years questionnaire [14].
Physical activity assessment
PA was evaluated with a previously validated 17-item self-administered questionnaire [15]. This questionnaire collects information about 17 different activities (walking, jogging, athletics, cycling, stationary cycling, swimming, tennis, soccer, basketball, dancing, hiking, gymnastics, gardening, skiing, martial arts, sailing, and other activities) and the time spent on each activity. Metabolic equivalents (METs) corresponding to each activity were obtained from the Compendium of Physical Activities [16]. Afterwards, the number of METs for each activity was multiplied by the hours dedicated to it per week, obtaining the total METs-h/week for each activity. Total energy expenditure during LTPA was quantified by summing the total METs-h/week of all the activities performed by each participant.
Based on the information on PA and sedentary lifestyles collected in the SUN cohort, we also calculated the total PA score (Table 1) according to a 0-to-8-point scale previously assessed in other evaluations of participants in the SUN cohort [17]. This PA score has shown a moderate correlation (r = 0.55) with PA parameters (METs-h/week). Thus, we scored with 1 point each of 6 items capturing the pattern of PA: 1) doing exercise; 2) expending at least 16.1 METs-h/week; 3) practicing sports with vigorous intensity (≥6 points); 4) adopting usually a brisk/very brisk walking pace; 5) walking for ≥30 min/d; and 6) climbing upstairs ≥3 floors/d. In addition, we scored with 1 point the following items which capture reduced sedentary activities: 7) watching television for <1.5 h/d; and 8) spending <5 h/d sitting down. The sum of these 8 items was subsequently categorized into 4 groups (low [≤2 points], medium-low [3 points], medium-high [4 points], and high [≥5 points]).
Scoring criteria for physical activity score in the SUN Project
aExercise intensity ranged from 0 (minimum intensity) to 10 (maximum intensity). bIncluding working and leisure time.
Covariates assessment
The baseline questionnaire collected information about participants’ sociodemographic characteristics (sex, age, years of university education), medical history (hypertension, hypercholesterolemia, low HDL-c, diabetes, and CVD), lifestyles (smoking habit), and anthropometric measurements (weight, height). Dietary habits were assessed with a validated 136-item semi-quantitative food-frequency questionnaire (FFQ) [18, 19] with 9 possible consumption frequencies (never or seldom; 1–3 times/month; once weekly; 2–4 times/week; 5-6 times/week; once daily; 2-3 times/day; 4–6 times/day; 6 or more times/day). To calculate the nutrient composition of the diet we used the Spanish food composition tables once the daily food consumption was calculated for each food item multiplying the consumption frequency by typical portion sizes [20, 21]. Adherence to the Mediterranean Diet (MedDiet) was assessed with the MedDiet Score developed by Trichopoulou et al. [22], with scores ranging from 0 (lowest adherence) to 9 (highest adherence).
Statistical analysis
To analyze the association between the score of an active lifestyle (combining PA intensity and avoidance of sedentary activities) and changes in cognitive function, we conducted multiple linear regression models. The dependent variable was the change in STICS-m from baseline to 6 years follow-up. Crude and multivariate models adjusted for several potential confounders were conducted as follows: Model 1 was adjusted for age, sex, years of university education, and APOE genotype; Model 2 was additionally adjusted for baseline body mass index (BMI, tertiles), follow-up time between baseline and cognitive evaluation, smoking status (current, former, never smoker), package-years among ever smokers, energy intake (quartiles), prevalent hypertension, prevalent hypercholesterolemia, low HDL cholesterol (HDL-c), prevalent diabetes, prevalent CVD, adherence to the MedDiet (tertiles) and use of aspirin, other painkillers and dietary supplements. To address the p for trend across the different categories of the active lifestyle score, we assigned the median value to each category and treated the resulting variable as continuous.
Participants were grouped into quartiles according to their total energy expenditure during LTPA. The first quartile was considered as the reference category. To investigate linear trends across the different LTPA categories, we assigned the median value to each category and treated the resulting variable as continuous. We calculated crude and multivariate adjusted models: Model 1 was adjusted for age, sex, years of university education, and APOE geno-type, Model 2 was additionally adjusted for BMI (tertiles), follow-up time between baseline and cognitive evaluation, smoking status (current, former, ne-ver smoker), package-years among ever smokers, energy intake (quartiles), total energy intake (kcal/ day), prevalent hypertension, prevalent hypercholesterolemia, low HDL-c, prevalent diabetes, prevalent CVD, adherence to the MedDiet (tertiles), time spent watching TV (h/d) and use of aspirin, other painkillers and dietary supplements.
We tested the interaction between the score of an active lifestyle and the APOE genotype (dominant model) on cognitive decline with the likelihood ratio test. For the interaction we considered the score of an active lifestyle as a qualitative variable (4 categories). Thus, the interactions had 3 degrees of freedom. We also tested the interaction between the score of an active lifestyle and sex in the same way.
Additional exploratory analyses were performed using as the dependent variable the change in each of the four domains of the STICS-m (orientation, immediate memory, attention/calculation, and language).
Statistical analyses were performed with STATA version 12 (STATA Corp., TX, USA). All p values were two tailed and a p value≤0.05 was considered as statistically significant.
RESULTS
Baseline characteristics of participants according to the score of PA are shown in Table 2. Of the 806 individuals, 69.7% were male and 30.3% female. The mean age of participants at recruitment was 61 (SD 6) years and at the time of the cognitive evaluation it was 66 (SD 5) years. The mean follow-up time in the cohort until first cognitive evaluation was 5.6 (SD 2.6) years. Compared to subjects with a low score (≤2 points) of adherence to an active lifestyle, those with a high score (≥5 points) were more likely to refrain from smoking, present a lower BMI, and have a higher adherence to the MedDiet. Supplementary Table 1 shows the baseline characteristics of participants of the SUN cohort according to quartiles of LTPA. Compared to subjects in the lowest LTPA quartile, those in the highest LTPA quartile were more likely to refrain from smoking, to suffer diabetes, to have a lower BMI and a higher adherence to the MedDiet.
Baseline characteristics of the participants of the SUN cohort according to score of physical activity
aIncludes stroke, myocardial infarction, coronary heart disease, coronary artery surgery, or angioplasty. bScore proposed by Trichopoulou et al. [22]. cPresence of at least one APOE ɛ4 allele.
Overall, we found no significant association be-tween adherence to an active lifestyle score and global cognitive function changes after 6 years of fol-low-up (Table 3). However, we found a statistic-ally significant interaction between adherence to the active lifestyle score and APOE genotype in their association with changes in cognitive function over time (p for interaction = 0.042). We observed that a higher adherence to an active lifestyle was associated with a better global cognitive function over time only among APOE ɛ4 non-carriers (high versus low adherence to the active lifestyle score β 0.76 95% CI 0.15;1.36; p for trend = 0.011) (Table 3). APOE ɛ4 carriers did not show any significant association between adherence to an active lifestyle score and changes in cognitive function over time (high versus low adherence to the active lifestyle score β –0.99 95% CI –2.30;0.31; p for trend = 0.149). Similar results were observed when analyzing the association between the score of PA as a continuous variable and changes in global cognitive function after a 6-year follow-up period (Table 3).
Global cognitive function changes after 6 years according to score of physical activity in the overall sample and stratified by APOE ɛ4 genotype
Note: Results for acategories of score of PA and for ban increase in 2 points in the score of PA (continuous). Boldface indicates statistical significance (p≤0.05). Model 1: Adjusted for age, sex, years of university education, and APOE genotype. Model 2: Model 1 + baseline BMI (tertiles), follow-up time between baseline and cognitive evaluation, smoking status (current, former, never smoker), package-years among ever smokers, energy intake (quartiles), prevalent hypertension, prevalent hypercholesterolemia, low HDL-c, prevalent diabetes, prevalent CVD, adherence to the MedDiet (tertiles), and use of aspirin, other painkillers and vitamin supplements.
Similarly, when we assessed the association bet-ween total energy expenditure during LTPA (Table 4), we found no significant associations in the overall sample but a significant interaction according to APOE genotype was found (p for interaction =0.039). As such, among APOE ɛ4 non-carriers higher LTPA (METs-h/week) was associated with more favorable changes in cognitive function over time (Q4 versus Q1 β 0.63; 95% CI –0.01;1.26; p for trend = 0.030), whereas in APOE ɛ4 carriers we did not observe a significant association between LTPA and changes in cognitive function over time for the comparison across extreme quartiles and the p for trend was not statistically significant (Q4 versus Q1 β –0.82; 95% CI –2.26;0.61; p for trend = 0.289).
Global cognitive function changes after 6 years according to the total energy expenditure during leisure-time physical activity (METs-h/week) in the overall sample and stratified by APOE ɛ4 genotype
Note: Boldface indicates statistical significance (p≤0.05). Model 1: Adjusted for age, sex, years of university education, and APOE genotype. Model 2: Model 1 + baseline BMI (tertiles), follow-up time between baseline and cognitive evaluation, smoking status (current, former, never smoker), package-years among ever smokers, energy intake (quartiles), prevalent hypertension, prevalent hypercholesterolemia, low HDL-c, prevalent diabetes, prevalent CVD, adherence to the MedDiet (tertiles), time spent on TV watching, and use of aspirin, other painkillers and vitamin supplements.
Additionally, we found no significant associations between adherence to the score of PA and cognitive domains. LTPA was associated with more favorable changes in the language domain in the overall sample (Q4 versus Q1 β 0.18; 95% CI 0.03; 0.33; p for trend = 0.038) but no further significant associations were observed for the other domains. When we explored the interaction between the score of PA or LTPA and APOE genotype in their association with changes in individual domains, we found a statistically significant interaction only for the orientation domain (p < 0.05 for both interactions). A higher adherence to the PA score was associated with more favorable changes in the orientation domain score among APOE ɛ4 non-carriers (Q4 versus Q1 β 0.25; 95% CI 0.02;0.47; p for trend = 0.035) but not among APOE ɛ4 carriers (Q4 versus Q1 β –0.58; 95% CI –1.06;–0.11; p for trend = 0.021). Similar results were observed for LTPA (data not shown).
We found no significant interaction between the score of PA or total LTPA and sex on cognitive function changes (p values for interaction > 0.05).
DISCUSSION
The results of the present prospective cohort study suggest that, among carriers of the APOE ɛ4 allele, an active lifestyle is not associated with beneficial changes in cognitive function over a 6-year period. However, measures of an active lifestyle did show a favorable association with changes in cognitive function among APOE ɛ4 non-carriers.
Mouse models of AD indicate that exercise (e.g., treadmill, wheel running, walking) improves cognition [23 –33]. Animals exposed to exercise showed several beneficial effects, including reduced reactive oxygen species and mitochondrial dysfunction, reduced levels of amyloid-beta 1–40 and 1–42 and phosphorylated tau, decreased inflammatory respo-nses and increased synaptic proteins, and improved cognitive behavior [23 –33].
Several observational and interventional studies have indicated that PA could potentially decrease the risk for dementia in elderly individuals [10 , 34–36]. A recent meta-analyses of prospective studies [37] showed that PA is associated with a reduced risk of developing AD among adults aged 65 years and older, and other recent systematic review demonstrated that a sedentary lifestyle is associated with poorer cardiovascular and cognitive health and faster decline of cognitive performance [11]. Nevertheless, a large prospective cohort study with a mean follow-up of 27 years found no evidence of a neuroprotective effect of PA, suggesting that previous findings showing a lower risk of dementia in physically active people may be attributable to reverse causation due to a decline in PA levels in the preclinical phase of dementia [38]. Despite the large sample size and the long follow-up period, this study did not ascertain important non-modifying risk factors, such as APOE genotype of participants, and the diagnosis of dementia was based on linkage to electronic health records. On the other hand, the evidence from clinical trials of PA and cognitive function in healthy individuals is equivocal. A Cochrane meta-analyses, including 12 RCTs, concluded that aerobic exercise or increased fitness did not improve cognitive function in healthy older people [39]. The null findings from clinical trials may be in part due to the short duration of the interventions, the age at which interventions were implemented or possibly a suboptimal level of PA studied.
There is less evidence regarding to sedentary be-havior and cognition. Some cohort and case-control studies suggest that sedentary behavior is associated with reduced cognitive function over the lifespan [40 –44]. However, there is a great heterogeneity in the methods used to quantify sedentary behavior and cognitive function in these studies, which is a major barrier to determine the precise magnitude of this association. To date, there are few studies on cognition that use an objective measure of sedentary behavior but none of them have a longitudinal design [45, 46].
The exact biological mechanism by which PA could preserve cognitive function in older adults is not well established. Participation in physical activities has been linked to improvements in muscular function, blood pressure, blood lipid levels, and lower risk of coronary heart disease [36], and it may also be beneficial for cognition [47 –49]. Some evidence attributes PA with an increased blood flow to the brain, while alternative evidence suggests that regular exercise is associated with increases in molecular growth factors, such as brain derived neurotrophic factor (BDNF) and insulin-like growth factor (IGF-1), which play a crucial role in neuroprotection [37]. In addition, cholinergic enhancement due to PA may increase cerebral blood flow, enhance neural activation, and possibly relieve amyloid burden [50]. In humans, recent evidence suggests that PA may have similar neurogenic effects in the hippoc-ampi of healthy younger [51] and older adults [52]. Recently, a systematic review including all controlled trials that examined the effect of aerobic exercise on the hippocampal volumes in humans found that aerobic exercise had significant positive effects on left hippocampal volume in comparison to control con-ditions [53]. However, it is not known if the neurotrophic effects of PA are comparable among APOE ɛ4 carriers and non-carriers.
Otherwise, a plausible mechanism by which sedentary behavior is associated with cognitive decline is emerging. Recent data suggest that prolonged sedentary time impairs glucose and lipid metabolism [54], which are well-recognized risk factors for cognitive decline and all-cause dementia. There is also evidence supporting that sedentary behavior is associated with many chronic diseases [55], which are also associated with cognitive impairment and dementia risk [56].
The APOE ɛ4, an APOE gene polymorphism, is the major genetic risk factor for late-onset AD and is involved in the increased production of amyloid-beta [5, 57]. There is evidence that the APOE genotype interacts with modifiable risk factors, but variability in reported findings still precludes firm conclusions [43, 58]. It remains unclear whether ɛ4 carriers are more likely to benefit from preventive interventions or whether the ɛ4 allele counteracts potential intervention benefits.
Interestingly, in our study, we found a significant interaction between PA and APOE genotype and the positive association between PA and upward 6-years cognitive function changes was restricted to APOE ɛ4 non-carriers. One of the main concerns regarding dementia prevention strategies is whether genetically susceptible individuals can still benefit from preventive lifestyle interventions. Some benefits for APOE ɛ4 carriers and non-carriers were observed in a trial of MedDiet–based interventions [59]. Otherwise, better effects among APOE ɛ4 non-carriers were found in a short PA RCT [60], similar to the findings of our study. In the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) trial [61], a multimodal lifestyle intervention RCT, overall improvement in global cognition and memory was less pronounced among ɛ4 carriers (362 over 1,109 subjects) compared with non-carriers (767 over 1,109 participants) (intervention and control groups together). It should be mention that the frequency of APOE ɛ4 carriers (32.6%) in the FINGER trial was higher than in our Spanish cohort study (20.0%), in line with previous studies that reported lower APOE ɛ4 frequencies for the Spanish population than in Northern European populations [6]. In a small observational study, Smith et al. [62] found that individuals with the APOE ɛ4 allele, and therefore at high genetic risk for AD, who reported regular levels of PA showed less hippocampal atrophy during an 18-month follow-up period than those with low PA. Therefore, whether benefits of PA on cognition are more pronounced in APOE ɛ4 non-carriers compared with APOE ɛ4 carriers is not well established. It is known that ApoE plays key roles in lipid transport and metabolism, both systemically and in the brain, and inheriting an APOE ɛ4 allele results in the disruption of lipid homeostasis [63, 64]. The effects of PA on brain lipid metabolism in human ɛ4 carriers are not yet known [65], nor if responses to exercise training differ based on APOE genotype [66].
Regarding LTPA, a large community-based pro-spective cohort study found that, compared with no LTPA, high LTPA in midlife was associated with lower incidence of dementia and lower declining in general cognitive performance [67]. In that study, not participating in LTPA in midlife was associated with a faster 14-year rate of decline in general cognitive performance relative to participants with high levels of LTPA in midlife.
The main strengths of this study are the large sample size, its longitudinal design with long follow-up, the simultaneous evaluation of PA and sedentary lifestyle, and the use of objective measures of cognitive performance during follow-up. However, we acknowledge that the present work has some limitations that should be mentioned. First, we used self-reported data for the active lifestyle score information rather than an objective measurement of cardiorespiratory fitness (i.e., maximal rate of oxygen consumption) or sedentary behavior (i.e., accelerometer), which might have led to some misclassification bias. Self-report LTPA may overestimate more vigorous PA and underestimate sedentary time. Second, although the STICS-m has been widely used in other epidemiological studies and has been previously validated in the Spanish population [14], it has been designed as a screening tool. A comprehensive battery of neuropsychological tests could be more appropriate to assess cognitive performance over time, but difficult to implement in large epidemiological studies. Third, the participants of the SUN project are university graduates and therefore the generalizability of the results may be limited. Nevertheless, it is plausible that the observed association would also apply to subjects with lower educational level. Fourth, the homogeneity of the population might have reduced the between-subject variability in PA exposures and therefore the sensitivity to detect significant differences on cognitive function across PA score or LTPA categories. However, this fact can also be considered as an advantage. This restriction could also reduce the potential confounding by socioeconomic and education level. In any case, we adjusted our results for a wide array of potential confounders in the multivariable analyses, which enhances the internal validity of our results. Fifth, since education is considered a protective factor against cognitive decline and AD [68], this could also further explain some non-statistically significant results. Sixth, despite the relatively large cohort of our study, the proportion of APOE ɛ4 carriers is smaller than the APOE ɛ4 non-carriers. The limited number of APOE ɛ4 carriers could reduce the statistical power to find significant differences within this group, which may be overcome with a bigger sample size. Otherwise, due to the observational design of our study, residual confounding by unmeasured potential confounders cannot be completely ruled out. Nevertheless, our analyses were adjusted for a wide range of confounders. Finally, our work is focused on analyzing the impact of PA on aging-related changes in cognition but not on dementia risk per se. This may be addressed in a future study on the same cohort after a longer follow-up period.
Reducing the high burden of cognitive impairment and its sequelae in our rapidly aging population is a high priority that may be attainable by intervening in modifiable behaviors such as PA. Our findings support the presumed neuroprotective effects of an active lifestyle on cognitive function among non-genetically predisposed individuals. Nevertheless, further studies are needed to confirm whether or not an active lifestyle or higher total energy expenditure during LTPA improves cognition and prevents dementia.
Footnotes
ACKNOWLEDGMENTS
We thank all the SUN participants for their continued cooperation and participantion. We also thank the other SUN Project investigators (Alonso A, Álvarez-Álvarez I, Balaguer A, Barbagallo M, Barrio-López MT, Basterra-Gortari FJ, Battezzati A, Bazal P, Bertoli S, Beulen Y, Beunza JJ, Buil-Cosiales P, Carlos S, Carmona L, Cervantes S, Cristobo C, de Irala J, de la Fuente-Arrillaga C, de la O V, de la Rosa PA, Delgado-Rodríguez M, Díaz-Gutiérrez J, Díez Espino J, Domínguez L, Donat-Vargas C, Donazar M, Eguaras S, Fernandez-Montero F, Fresán U, Galbete C, García-Arellano A, García López M, Gardeazábal I, Gea A, Gutiérrez-Bedmar M, Gomes-Domingos AL, Gómez-Donoso C, Gómez-Gracia E, Goñi E, Guillén F, Henríquez P, Hernández-Hernández A, Hershey MS, Hidalgo-Santamaría M, Hu E, Leone A, Llorca J, López del Burgo C, Marí A, Marques I, Martí A, Martín Calvo N, Martín-Moreno JM, Martínez JA, Martínez-Lapiscina EH, Mendonça R, Menéndez C, Molendijk M, Murphy K, Muñoz M, Núñez-Córdoba JM, Pajares R, Papadaki A, Parletta N, Pérez de Ciriza P, Pérez-Cornago A, Pérez de Rojas J, Pimenta AM, Pons J, Ramallal R, Rico-Campá A, Romanos-Nanclares A, Ruano C, Ruiz-Canela M, Ruiz-Estigarribia L, Ruiz Zambrana A, Salgado E, San Julián B, Sánchez D, Sánchez-Bayona R, Sanchez-Villegas A, Santiago S, Sayón-Orea C, Schlatter J, Serrano-Martinez M, Toledo J, Tortosa A, Valencia F, Vázquez Z, Zarnowiecki D, Zazpe I).
The SUN Project has received funding from the Instituto de Salud Carlos III, and the European Reg-ional Development Fund (FEDER) [grant number RD 06/0045], CIBER-OBN [grant number PI10/02658, PI10/02293, PI13/00615, PI14/01668, PI14/01798, PI14/01764, and G03/140], the Navarra Regional Government [grant number 45/2011, 122/2014], and the University of Navarra.