
Abstract
Background:
Little is known about the sex differences in the association between body mass index (BMI) and dementia in late life.
Objective:
Therefore, this retrospective cohort study aimed to analyze associations between BMI and dementia in older women and men separately in general practices in Germany.
Methods:
This study included patients followed in one of 832 general practices in Germany between 2006 and 2019 (index date: first visit date). Study variables included dementia (dependent variable), BMI (independent variable), age, sex, and comorbidities (control variables). Kaplan-Meier curves and adjusted Cox regression analyses were conducted to analyze associations between BMI and the 10-year incidence of dementia in women and men, separately.
Results:
There were 296,767 patients included in this study (mean [standard deviation] age 70.2 [5.9] years; 54.3% women). The proportion of underweight, normal weight, overweight, and obesity was 0.9%, 25.5%, 41.5%, and 32.1%, respectively. The 10-year incidence of dementia significantly decreased with increasing BMI, from 11.5% in women with underweight to 9.1% in those with obesity (log-rank p < 0.001). Respective figures in men were 12.0% and 8.2% (log-rank p < 0.001). In women, only overweight (versus normal weight) was significantly associated with dementia (HR = 0.93, 95% CI = 0.88–0.97). In contrast, in men, the only BMI category significantly associated with the incidence of dementia was underweight (HR = 1.58, 95% CI = 1.11–2.25).
Conclusion:
In this study conducted in Germany, overweight was negatively associated with dementia in women, whereas there was a positive underweight-dementia relationship in men. More data are needed to confirm or refute these findings in other settings.
INTRODUCTION
Dementia refers to a syndrome of progressive nature characterized by the alteration of several higher cognitive functions (e.g., memory, comprehension, and judgment) severe enough to impair independent functioning and daily living [1]. The prevalence of dementia in the community is around 697 cases per 10,000 people aged≥50 years [2] and, because of aging of the population, the number of individuals with dementia is likely to increase in the following decades [3]. Dementia is associated with multiple deleterious health outcomes such as impaired mental health [4, 5], higher functional disability [6], and increased mortality [7]. Moreover, the efficacy of available dementia treatments is only modest [8], and the management of dementia imposes a substantial economic burden on patients and their families as well as healthcare systems [9]. Thus, it is of utmost importance to better characterize risk factors for and protective factors against dementia.∥A substantial body of literature has analyzed the potential association between late-life body mass index (BMI) and dementia [10–15]. For example, a study of 6,940 older adults from the United States showed that an increase in late-life BMI was associated with a decrease in the risk of mild cognitive impairment and dementia [10]. A systematic review and meta-analysis of 29 prospective studies further found a negative association between overweight/obesity and cognitive impairment/dementia, while there was a positive association with midlife underweight [15]. Several factors may explain the inverse relationship between BMI and dementia. First, weight loss may be one of the first symptoms of dementia, resulting from apathy [16], difficulty in eating [17], and disrupted olfaction [18]. Second, a higher BMI in late life may promote synaptic plasticity and better cognitive performance [12]. Given that there are some data suggesting that estrogen has neuroprotective effects [19], it is possible that the BMI-dementia relationship differs between women and men. However, to date, no research has yet investigated this hypothesis.∥Therefore, the aim of this retrospective cohort study was to investigate associations between BMI and dementia in older women and men separately in general practices in Germany.∥
MATERIALS AND METHODS
Database
This study used data from the Disease Analy-zer database (IQVIA). This database has already been extensively described in the literature [20]. To summarize, the Disease Analyzer database contains demographic, diagnosis and prescription data from patients followed in general and specialized practices in Germany. Practices to include in the database are selected based on multiple factors (i.e., physician’s age, specialty group, community size category, and German federal state), and the database is composed of around 3% of all practices in Germany. Diagnosis and prescription data are coded using the International Classification of Diseases, 10th revision (ICD-10), and the Anatomical Classification of Pharmaceutical Products of the European Pharmaceutical Marketing Research Association (EphMRA), respectively. Data are anonymously sent to IQVIA on a regular basis, and the quality of these data is assessed using several criteria such as completeness of documentation and linkage between diagnoses and prescriptions. Finally, previous research has shown that the Disease Analyzer database is representative of private practices in Germany [20].
Study population
This retrospective cohort study included patients followed in one of 832 general practices in Germany between January 2006 and December 2019. Index date corresponded to the first visit date between 2006 and 2019. Inclusion criteria were the following: available data on BMI for the period between one year prior to the index date and one year prior to the diagnosis of dementia or last follow-up; age≥65 years at the index date; and no diagnosis of dementia (ICD-10: F00-F03 and G30) prior to or at the index date. Selection of study patients is displayed in Fig. 1. Characteristics of patients included and those not included in the study are displayed in Supplementary Table 1.
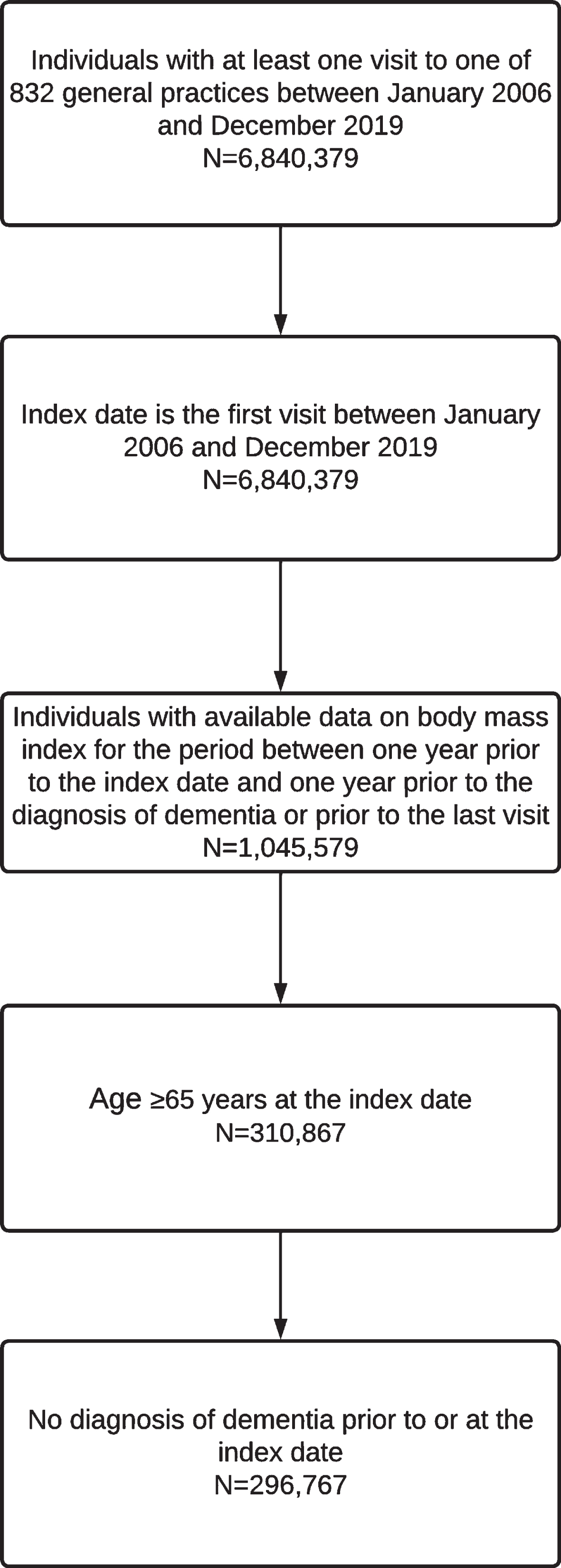
Selection of study patients.
Characteristics of study patients
SD, standard deviation. Data are proportion unless otherwise specified.
Study variables
Dementia (dependent variable) included Alzhei-mer’s disease (ICD-10: G30), vascular dementia (ICD-10: F01), and undefined dementia (ICD-10: F03). Using the definition of the World Health Organization [21], and using the mean BMI value between one year prior to the index date and one year prior to the diagnosis of dementia or last follow-up, BMI was included in this study as a four-category variable: underweight (i.e., BMI < 18.5 kg/m2), normal weight (i.e., BMI 18.5 – < 25 kg/m2), overweight (i.e., BMI 25 – < 30 kg/m2), and obesity (i.e., BMI≥30 kg/m2). Control variables included age, sex, and comorbidities documented in the five years prior to the diagnosis of dementia or the end of follow-up. These comorbidities were hypertension (ICD-10: I10), lipid metabolism disorders (ICD-10: E78), diabetes mellitus (ICD-10: E10–E14), ischemic heart diseases (ICD-10: I20–I25), depression (ICD-10: F32 and F33), stroke or transient ischemic attack (ICD-10: I63, I64 and G45), chronic obstructive bronchitis or lung disease (ICD-10: J42–J44), heart failure (ICD-10: I50), chronic kidney disease and renal failure (ICD-10: N18 and N19), liver diseases (ICD-10: B18 and K70–K77), neck of femur fracture (ICD-10: S72.0), epilepsy (ICD-10: G40 and G41), inflammatory bowel disease (ICD-10: K50 and K51), and mild cognitive impairment (ICD-10: F06.7).
Statistical analyses
Age at index date, sex, and comorbidities were compared between BMI categories (i.e., underweight, normal weight, overweight, and obesity) using the Kruskal-Wallis test for continuous age and chi-square tests for other variables. The 10-year incidence of dementia by BMI category was further studied in the whole sample, women and men using Kaplan-Meier curves and log-rank tests. Finally, associations between BMI and dementia in all patients and by sex were analyzed with Cox regression models adjusted for age, sex (except the sex-stratified analyses), and comorbidities. Interaction by sex was also assessed by including the interaction term continuous BMI * sex in the Cox regression models. The results of the Cox regression analyses are displayed as hazard ratios (HRs) and 95% confidence intervals (95% CI). p lower than 0.05 were considered statistically significant. Finally, analyses were conducted with SAS 9.4.
RESULTS
This study included 296,767 patients (mean [standard deviation] age 70.2 [5.9] years; 54.3% women; Table 1). The proportion of underweight, normal weight, overweight, and obesity was 0.9%, 25.5%, 41.5%, and 32.1%, respectively. Most frequent comorbidities were hypertension (76.9%), lipid metabolism disorders (52.3%) and diabetes mellitus (39.7%). The 10-year incidence of dementia significantly decreased from 11.6% in people with underweight to 8.7% in those with obesity (log-rank p < 0.001; Fig. 2). Similar results were obtained in the sex-stratified analyses. Dementia occurred in 11.5% of women with underweight and in 9.1% of those with obesity (log-rank p < 0.001; Fig. 3, higher panel). Respective figures in men were 12.0% and 8.2% (log-rank p < 0.001; Fig. 3, lower panel). The results of the adjusted Cox regression analyses are displayed in Table 2 and Supplementary Table 2. In the overall sample, compared with normal weight, underweight was significantly and positively associated with the incidence of dementia (HR = 1.21, 95% CI = 1.05–1.40), whereas there was a significant and negative association between overweight and dementia (HR = 0.94, 95% CI = 0.91–0.98). The interaction between continuous BMI and sex tended to be significant (p = 0.061). In women, only overweight was significantly and negatively associated with dementia (HR = 0.93, 95% CI = 0.88–0.97). In contrast, in men, the only BMI category significantly and positively associated with the incidence of dementia was underweight (HR = 1.58, 95% CI = 1.11–2.25). In terms of the specific types of dementia, obesity was significantly and negatively associated with Alzheimer’s disease (HR = 0.81, 95% CI = 0.70–0.93) and overweight negatively with undefined dementia in female patients (HR = 0.90, 95% CI = 0.85–0.96). In male patients, there was also a negative and significant association between obesity and Alzheimer’s disease (HR = 0.82, 95% CI = 0.69–0.98), while underweight was positively associated with undefined dementia (HR = 1.95, 95% CI = 1.30–2.93). The interaction between continuous BMI and sex was not significant for the three specific types of dementia (Alzheimer’s disease: p = 0.248; vascular dementia: p = 0.549; and undefined dementia: p = 0.147).
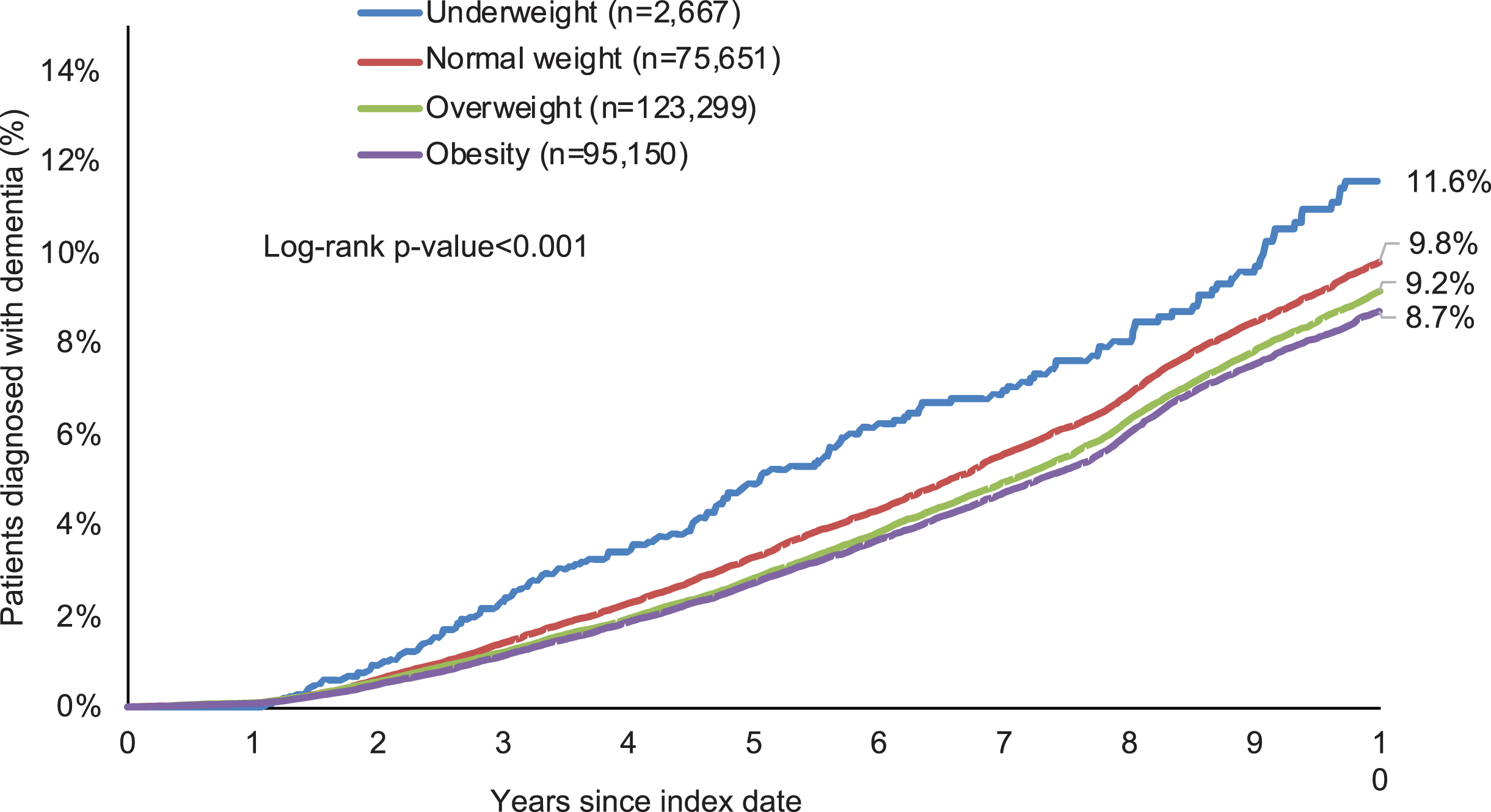
Incidence of dementia by body mass index category in older individuals followed in general practices in Germany.

Incidence of dementia by body mass index category in older women (upper panel) and men (lower panel) followed in general practices in Germany.
Association between body mass index categories and the incidence of dementia (adjusted Cox regression models)
HR, hazard ratio; CI, confidence interval. Bold is used for statistically significant associations. Cox regression models were adjusted for age, sex (except the sex-stratified analyses) and all comorbidities listed in Table 1.
DISCUSSION
Main findings
This study, including more than 296,000 patients followed in general practices in Germany, identified sex differences in the association between BMI and the incidence of dementia. Overweight was negatively associated with dementia in women (HR =0.93), whereas there was a positive and significant association between underweight and dementia in men (HR = 1.58). It was further revealed that, in female patients, obesity and overweight were associated with a significant decrease in Alzhei-mer’s disease (HR = 0.81) and undefined dementia (HR = 0.90), respectively. In contrast, in male patients, a negative association was found between obesity and Alzheimer’s disease (HR = 0.82), while there was a strong and positive relationship between underweight and undefined dementia (HR = 1.95). To the best of the authors’ knowledge, this is the first study to have investigated the sex-differential associations between BMI and the incidence of dementia.
Interpretation of findings
Corroborating previous literature, this study showed that underweight was positively and overweight negatively associated with dementia in older adults living in Germany. For example, it was observed, in one study of 1,349,857 participants without dementia from Asia, Europe, and the United States, that a five-kg/m2 increase in BMI led to a significant decrease in the risk of dementia (HR = 0.71) when BMI was assessed in the decade prior to the diagnosis of dementia [13]. The positive effects of high BMI in late life on dementia may be mediated by several hormones such as leptin and oxytocin. Indeed, there is a strong and positive correlation between BMI and high leptin levels [22, 23], and leptin plays a substantial role in enhancing cognition [24]. Moreover, some data suggest that high BMI is associated with higher levels of oxytocin [25], while higher levels of oxytocin might protect against the decrease in hippocampus and amygdala volumes in late life [26]. Finally, it should be mentioned that decreasing BMI in the years preceding the occurrence of dementia is associated with other cardiometabolic changes such as decreasing diastolic blood pressure and increasing blood glucose levels [27].
The present study adds to the literature by showing substantial sex differences in the association between BMI and dementia in older individuals. Of particular importance, underweight was significantly associated with an increase in the incidence of dementia in men but not in women, and this differential association was also observed for undefined dementia. These results are not in line with a recent cohort study of 3,696 individuals from Japan, as being underweight was identified as a significant risk factor for dementia in women but not in men [28]. It is possible that sex differences in the association between BMI and dementia vary between ethnicities. Besides, although the findings of the Japanese study are of particular interest, this study only included a few comorbidities (i.e., diabetes, hypertension, dyslipidemia, and stroke), and this may have biased the results. The differences observed in the present study are likely explained, at least partially, by the higher levels of estrogen in women than in their male counterparts. There is evidence suggesting that estrogen may stimulate the secretion of leptin [29, 30] and even mimic this hormone [31], potentially buffering the deleterious impact of low BMI on dementia in women. Similarly, some data indicate that estrogen also stimulates the release of oxytocin [32, 33]. Moreover, underweight may favor the occurrence of dementia via pathways specific to men. For example, underweight is a risk factor for vertebral fracture in men but not in women [34, 35], and vertebral fracture can in turn increases the risk of dementia [36]. In addition, studies have highlighted the fact that underweight favors the occurrence of asthma in older men and not in older women [37, 38], while asthma in middle and late life increases the risk of developing dementia [39]. Furthermore, preliminary research has shown that the negative effects of underweight on physical mobility limitation are more pronounced in middle-aged and older men than in their female counterparts [40], and midlife function limitations positively predict the occurrence of dementia [41]. Besides, being underweight increases medical and pharmacy costs at an older age [42], and financial difficulties are associated with memory decline in the male elderly population [43]. Finally, the differential association between BMI and the incidence of dementia in men and women may involve social factors [44]. As a matter of fact, there is some literature suggesting that marital status may impact BMI [45], while data suggest that being not married is a risk factor for incident dementia in men but not in women [46].
Clinical implications and directions for future research
Based on the results of this study, there are substantial sex differences in the association between BMI and dementia. It appears that there is a strong and positive relationship between underweight and dementia in older men. In this context, cognitive impairments should be regularly assessed in older male patients with BMI < 18.5 kg/m2. Furthermore, interventions aiming at weight gain should be implemented in this population, and these interventions may include nutritional supplements, high-energy snacks and community support services [47]. On the other hand, overweight may protect against dementia in older women, suggesting that a moderate weight excess in late life may be acceptable from a cognitive perspective. In terms of future research, more studies are needed to corroborate or invalidate these findings in other countries and settings. Moreover, further data are warranted to understand better the underlying reasons for these sex differences in associations between BMI in late life and dementia, and to characterize better the exact role played by female hormones.
Strengths and limitations
The two major strengths of this study are the large sample size and the use of longitudinal data obtained in general practices. However, the results of the study should be interpreted in the light of several limitations. First, data on BMI were unavailable for the majority of patients followed in general practices between January 2006 and December 2019, and this may have biased the study findings. Second, BMI may not be a reliable measure of underweight, overweight, and obesity [48], and the use of other parameters such as waist circumference may have allowed more accurate analyses. Third, dementia may have been diagnosed in specialized practices such as neuropsychiatric and geriatric practices, and therefore the incidence of dementia may have been underestimated. Fourth, there was no information in the database on physical activity and diet, although these two factors are associated with both BMI and dementia. Fifth, participants with underweight were significantly older than those in other BMI categories and, although age was included in the Cox regression analyses, this difference may have impacted the results of these analyses.
Conclusions
Overall, this study of 296,767 older adults from Germany identified major sex differences in associations between BMI and dementia. Underweight was positively associated with dementia in male patients, whereas there was a negative and significant association between overweight and dementia in women. More research is warranted to confirm or refute these findings in other countries and settings.