
Abstract
Background:
Most previous studies focusing on the migraine headache-dementia relationship have failed to simultaneously adjust for several common comorbidities.
Objective:
The goal of this retrospective cohort study was to investigate the association between migraine headaches and dementia in general practices in the UK.
Methods:
The current study sample included patients who received a migraine diagnosis in one of 67 general practices in the UK between January 1997 and December 2016 (index date). Patients without migraine diagnoses were matched 1 : 1 to patients with migraine diagnoses based on propensity scores using a greedy algorithm and derived from the logistic regression using age, sex, index year, and co-diagnoses. The main outcome of the study was the association between migraine headaches and the incidence of dementia within 10 years of the index date.
Results:
This study included 7,454 individuals with or without migraine diagnoses. Mean age was 67.7 years (SD = 5.8 years), and 72.9% of patients were women. Within 10 years of the index date, 5.2% of participants with and 3.7% of those without migraine headaches were diagnosed with dementia (log-rank p < 0.001). The respective figures were 5.8% and 3.6% in women (log-rank p < 0.001) and 4.5% and 3.4% in men (log-rank p = 0.722). We observed a positive association between migraine diagnoses and all-cause dementia (hazard ratio [HR] = 1.43) as well as Alzheimer’s disease (HR = 1.87). Sensitivity analyses further revealed that these associations were only significant in women (all-cause dementia: HR = 1.65; Alzheimer’s disease: HR = 2.27).
Conclusion:
Migraine diagnoses were positively associated with all-cause dementia and Alzheimer’s disease in women.
INTRODUCTION
Around one billion individuals throughout the world suffered from migraine headaches in 2016 [1]. Migraine headaches were associated with a significant burden and caused approximately 45 million years lived with disability in that same year. Further research has found that migraine headaches are also associated with decreased workplace productivity [2] and increased health costs [3], which demonstrates the major impact of this neurological condition in modern society.
Several studies have recently focused on the association between migraine headaches and other headaches, respectively, and dementia [4–10]. For example, a 2018 meta-analysis of six cohort studies revealed that any headache led to a 1.24-fold increase in the risk of all-cause dementia but found no significant association between any type of headache and Alzheimer’s disease [9]. These findings were corroborated one year later in a nested case-control study that included more than 57,000 participants and found a positive migraine-dementia relationship in the overall sample (odd-ratio [OR] = 1.13) [10]. The association between migraine headaches and dementia may be mediated by several biological and clinical factors, such as white-matter hyperintensity, pain, depression, and stress [9]. Although these previous studies are interesting, most of them have failed to simultaneously adjust for several common comorbidities (e.g., hyperlipidemia [11, 12], depression [13, 14], diabetes [15, 16], stroke [17, 18]), thus potentially introducing bias into their findings. Furthermore, most of these analyses were conducted outside of Europe [4, 10], and extrapolating their findings to this region of the world is difficult.
Therefore, the goal of this retrospective cohort study was to investigate the association between migraine diagnoses and dementia in 7,454 patients followed in general practices in the UK. Since the number of people with dementia in this country is expected to exceed one million by 2030 [19], studying potential risk factors such as migraine headaches is a public health priority.
METHODS
Database
This study was based on data from the Disease Analyzer database (IQVIA), which compiles drug prescriptions, diagnoses, and basic medical and demographic data obtained directly and in anonymous format from computer systems used in the practices of general practitioners and specialists [20]. Diagnoses (International Classification of Diseases, 10th revision [ICD-10]), prescriptions (Anatomical Therapeutic Chemical [ATC] Classification system), and the quality of reported data are monitored by IQVIA based on a number of criteria (e.g., completeness of documentation, linkage between diagnoses and prescriptions).
In the UK, the sampling methods used to select physicians’ practices were appropriate for obtaining a representative database of people with migraine headaches [20]. The sampling method for the Disease Analyzer database is based on statistics from all doctors in the UK. These statistics are used to determine the panel composition according to the following strata: region, community size category, and physician age.
Finally, several studies using the UK Disease Analyzer database have already been published [21, 22].
Study population
The current study sample included patients who received a migraine diagnosis (ICD-10: G43) in one of 67 general practices in the UK between January 1997 and December 2016 (index date). Inclusion criteria were as follows: a follow-up time of at least 12 months prior to the index date; a follow-up time of at least 12 months after the index date; age between 60 and 80 years at the index date; and no diagnosis of dementia (ICD-10: F01, F03, G30) or mild cognitive impairment (F06.7) prior to or at the index date. After applying similar inclusion criteria, patients without migraine diagnoses were matched 1 : 1 to patients with migraine diagnoses based on propensity scores using a greedy algorithm and derived from the logistic regression using age, sex, index year, and co-diagnoses (i.e., diabetes mellitus, hyperlipidemia, coronary heart disease, stroke including transient ischemic attack, depression, intracranial injury, mental and behavioral disorders due to the use of alcohol, epilepsy, Parkinson’s disease, osteoporosis). The index date for participants without migraine diagnoses was a randomly selected visit between January 1997 and December 2016. The present study included 3,727 individuals with and 3,727 individuals without a migraine diagnosis (Fig. 1).
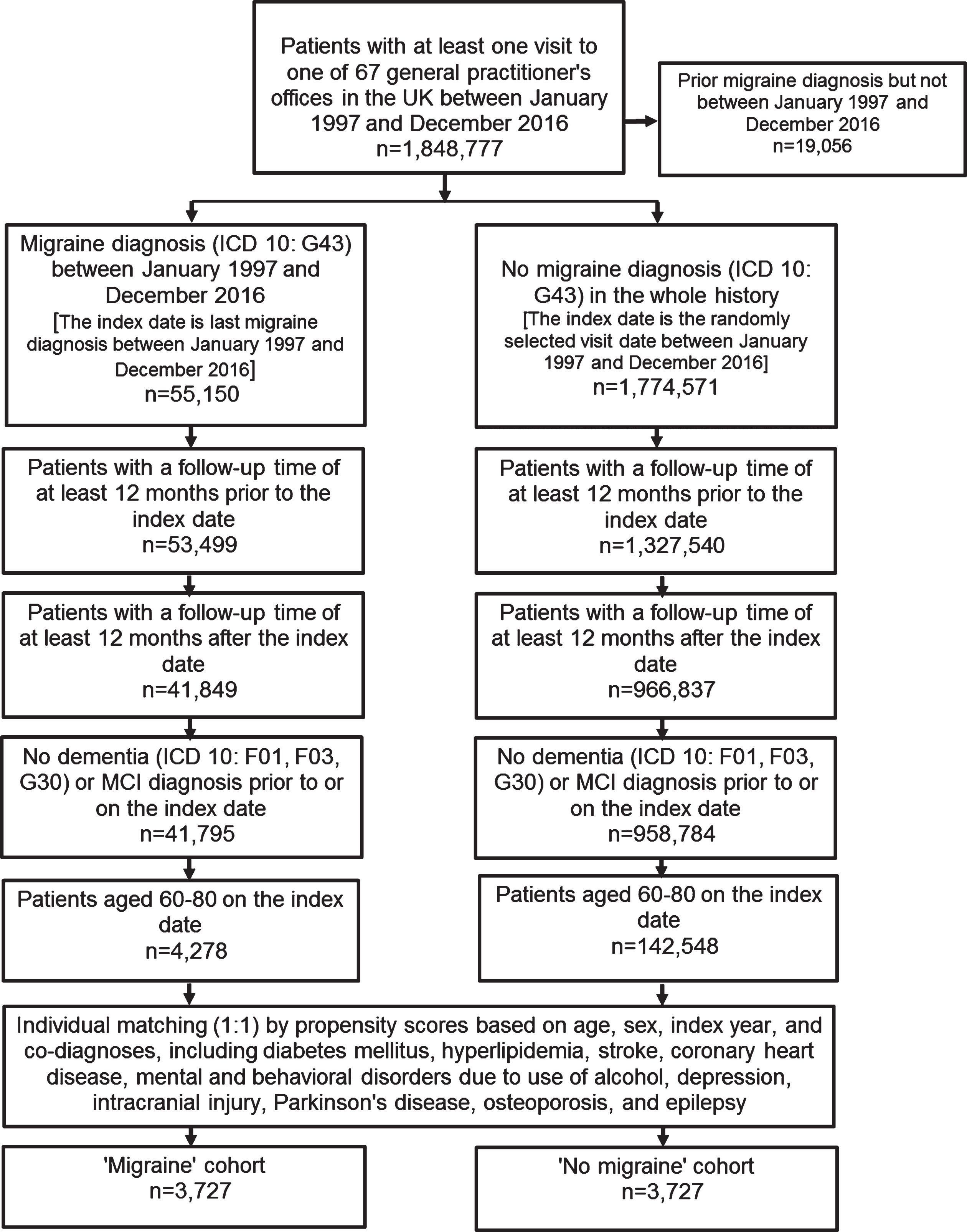
Selection of study patients.
Study variables
Variables included age, sex, index year, and 10 comorbidities documented prior to the index date or during the follow-up period (i.e., diabetes mellitus [ICD-10: E10-14] [15, 16], hyperlipidemia [E78] [11, 12], coronary heart disease [I24, I25] [23, 24], stroke including transient ischemic attack [I60-64, G45] [17, 18], depression [F32, F33] [13, 14], intracranial injury [S06] [25, 26], mental and behavioral disorders due to the use of alcohol [F10] [27, 28], epilepsy [G40, G41] [29, 30], Parkinson’s disease [G20, G21] [31, 32], and osteoporosis [M80, M81] [33, 34]).
Study outcome
The main outcome of the study was the incidence of dementia (ICD-10: F01, F03, G30) as a function of migraine diagnosis within 10 years of the index date. The analyses included three types of dementia: vascular dementia (F01), Alzheimer’s disease (G30), and unspecified dementia (F03).
Statistical analyses
Differences in the sample characteristics between those with and without migraine diagnoses were tested using chi-squared tests for categorical variables and Wilcoxon tests for continuous variables. We calculated the cumulative incidence of dementia in patients with and without migraine diagnoses for up to 10 years after the index date using Kaplan-Meier curves for men and women separately. As mortality data are not available in the Disease Analyzer database, dead participants were considered as loss to follow-up. We adopted univariate Cox regression models to study the association between migraine diagnoses and dementia (i.e., all-cause dementia, vascular dementia, Alzheimer’s disease, unspecified dementia) in the overall sample. Sensitivity analyses were conducted in men and women separately. A p-value of < 0.05 was considered statistically significant. Statistical analyses were performed using SAS 9.4.
RESULTS
This study included 7,454 individuals with and without migraine diagnoses (Fig. 1). Mean age was 67.7 years (SD = 5.8 years), and 72.9% of patients were women (Table 1). The three most frequent comorbidities were hyperlipidemia (62.0%), depression (29.4%), and diabetes mellitus (14.7%). A total of 17.4% of migraine patients received at least one triptan prescription during the follow-up period. Within 10 years of the index date, 5.2% of participants with and 3.7% of those without migraine diagnoses were diagnosed with dementia (log-rank p < 0.001; Fig. 2). The respective figures were 5.8% and 3.6% in women (log-rank p < 0.001; Fig. 3) and 4.5% and 3.4% in men (log-rank p = 0.722; Fig. 4). The results of the Cox regression models are shown in Table 2. We observed a positive association between migraine diagnoses and all-cause dementia (hazard-ratio [HR] = 1.43) and Alzheimer’s disease (HR = 1.87). Sensitivity analyses further revealed that these associations were only significant in women (all-cause dementia: HR = 1.65; Alzheimer’s disease: HR = 2.27). In contrast, migraine diagnoses did not have a significant relationship with either vascular or unspecified dementia.

Kaplan-Meier curves for time to diagnosis of all-cause dementia in patients with and without migraine headaches.

Kaplan-Meier curves for time to diagnosis of all-cause dementia in women with and without migraine headaches.
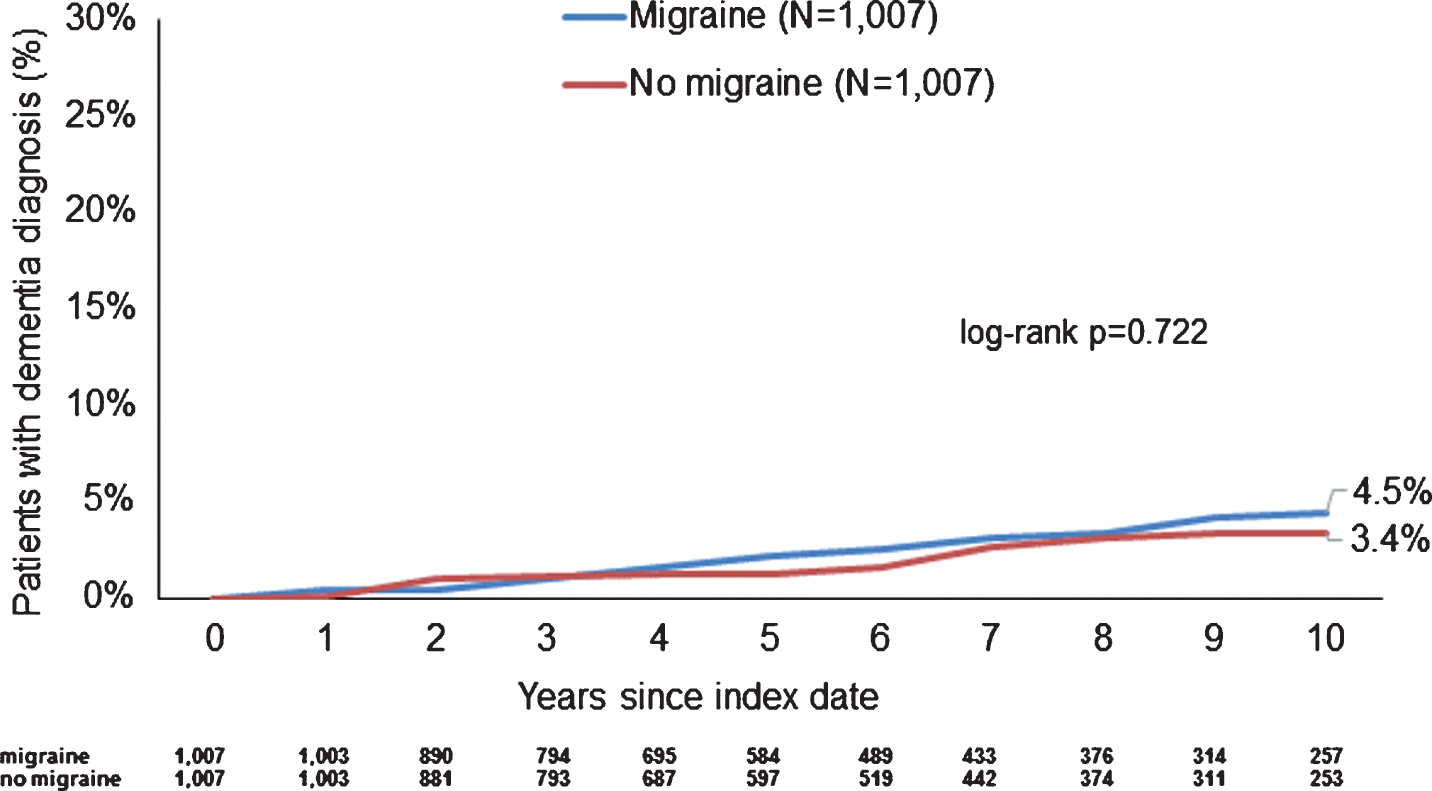
Kaplan-Meier curves for time to diagnosis of all-cause dementia in men with and without migraine headaches.
Baseline characteristics of study patients after 1 : 1 matching by age, sex, index year, and co-diagnoses using a propensity score method
Association between migraine headaches and the risk of dementia in individuals followed for up to 10 years in 67 general practices in the UK
DISCUSSION
Main findings
In this retrospective cohort study conducted in the UK, we observed that the cumulative incidence of all-cause dementia and Alzheimer’s disease was higher in individuals with migraine diagnoses than in those without them. Furthermore, we found a positive association between migraine diagnoses and both all-cause dementia and Alzheimer’s disease and, ultimately, these relationships were only significant in women.
Interpretation of the findings
In the past, few authors have investigated the impact of migraine headaches and other headaches on the likelihood of developing dementia [4–10]. For example, in 2013, Chuang and colleagues performed a nationwide retrospective cohort study including more than 167,000 participants from Taiwan and reported that the migraine headache group displayed a 1.33-fold increase in the incidence of dementia compared to the non-migraine headache group [5]. One year later, Hagen et al. showed in a prospective population-based study (n = 51,859) that any headache was positively associated with vascular dementia (HR = 2.3) and mixed dementia (HR = 2.0) but not with Alzheimer’s disease (HR = 1.0) [6]. The results of the present study are not in line with these findings, and such discrepancy may be explained by the fact that the regression models in this study were adjusted for numerous comorbidities. More recently, researchers from the Republic of Korea found, in a nested case-control study based on the data of 57,190 women, that those with dementia were more likely to have a history of migraine headaches than those without dementia (OR = 1.13) [10]. Taken together, these findings highlight the fact that migraine headaches may be a risk factor for dementia.
Another result of the present retrospective study that merits further attention is the fact that the positive association between migraine headaches and all-cause dementia and Alzheimer’s disease was significant in women but not in men. This outcome is in line with the Lee study [10], which found that men with migraine diagnoses were not at a significantly increased risk for dementia compared to the controls. Dementia exhibits major sex differences, which may play an important role in the differential relationship reported in our study [35]. Furthermore, a recent analysis that used data from a longitudinal survey of US adults with migraine headaches found that men were older at the onset of the disease, had fewer headache days per month, had less severe attacks, and were less frequently diagnosed with chronic migraine headaches than women [36]. Another study reported that migraine headaches were associated with greater disability in women than in men and that treatments for depression and anxiety were more frequently prescribed in female than in male participants [37]. Finally, a sample of 44 participants undergoing high-field magnetic resonance imaging (MRI) highlighted substantial differences in brain function and structure between men and women with migraine headaches [38]. All of these studies clearly show that there is a sex phenotype in migraine, which may play an important role in the sex differences in the migraine-dementia association observed in the present study.
Several biological and clinical hypotheses may explain the association between migraine headaches and dementia. First, a 2004 meta-analysis that included seven case-control studies identified migraine headaches as a risk factor for MRI white matter abnormalities [39], although a community-based cohort reported a lack of significant progression of most MRI-measured brain changes in both men and women throughout the course of the disease [40]. These abnormalities, particularly when located in the periventricular region, are positively associated with the likelihood of developing dementia in the elderly [41]. Second, migraine headaches and other headaches frequently involve chronic pain [42], which has recently been found to substantially impact the risk of memory decline and dementia [43]. Third, a 2013 prospective cohort study has revealed among more than 36,000 patients that nonmigraine headaches, migraine attacks without aura, and migraine attacks with aura increase the risk of incident depression [14]. On the other hand, an analysis of the Framingham Heart Study found a 1.72-fold increase in the odds of dementia and a 1.76-fold increase in the odds of Alzheimer’s disease in people diagnosed with depression compared to those without this psychiatric condition [13]. Fourth, people with migraine diagnoses often exhibit high levels of perceived stress [44], which is a well-known risk factor for cognitive decline [45], mild cognitive impairment [46], and dementia [47].
Our results indicate that elderly people with migraine headaches should be regularly screened for cognitive decline and dementia. Furthermore, offering adequate treatment and management to migraine patients is important, as it may help prevent the subsequent development of dementia. Randomized controlled trials and real-world studies are needed to substantiate these assumptions, while further research should focus on the potential mediators involved in the migraine-dementia relationship, as well as on the sex differences highlighted in this study.
Strengths and limitations
The two major strengths of this study are the number of patients available for analysis and the use of real-world data. That being said, this study also has several limitations that should be acknowledged at this point. First, although the prevalence of migraine headaches is the highest in young adults and tends to decrease with age [48], this study only included participants aged between 60 and 80 years, thus potentially introducing a bias into the statistical analyses. Second, headaches related to an underlying ischemic cerebral lesion are frequently misdiagnosed as migraine headaches in the elderly [49], which may have affected the results of the present study. Third, no information on how dementia was diagnosed in general practices was available, but there may be some important differences regarding diagnostic procedures compared to neuropsychiatric practices. Fourth, the diagnosis of migraine headaches relied solely on ICD-10 codes, and no data on the severity of migraine headaches, the frequency of recent migraine headaches, or the presence of an aura were available. Therefore, investigating their impact on the dementia was not possible. Fifth, since information on behavioral factors (e.g., alcohol use, smoking, sedentary lifestyle) was lacking, the roles played by these factors in the migraine-dementia relationship could not be studied. Sixth, the impact of anti-migraine medications like triptans was not investigated in this study.
Conclusion
Migraine diagnoses were positively associated with all-cause dementia and Alzheimer’s disease in the UK. The migraine-dementia relationship may differ substantially between men and women, and further studies are warranted to gain a better understanding of the underlying mechanisms.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-0581r1).