
Abstract
Background:
Although numerous studies have reported a decrease in dementia risk in the last two decades, it is unclear whether dementia-free cognitive function is also changing across generations.
Objective:
The objective was to systematically evaluate the published data on generational differences in cognitive function in the older population.
Methods:
Searches were performed on PubMed, Embase, and PsychInfo for articles published in English before 28 June 2021. Included studies were from population-based samples that reported generational differences in cognition in individuals without dementia, aged ≥60 years.
Results:
28,101 studies were identified and 15 selected covering the period from 1971 to 2015: including studies from China, Europe, and the USA. The results show generally consistent findings of improvements or stability in dementia free cognitive function in later versus earlier born generations, but not for all cognitive domains. Prevalence of mild cognitive impairment and cognitive impairment no dementia has remained stable in the USA, UK, and China over the last two decades.
Results:
Prevalence of vascular related mild cognitive impairment has increased in China. Improvements in cognition may only partially be explained by increased educational attainment across generations.
Conclusion:
This review provides evidence for generational effects in dementia-free cognitive function, predominately stability or improvements in performance, in later compared to earlier born individuals across different world regions. There is an urgent need to determine the factors driving such changes and whether they are being experienced in all world regions, particularly low- and middle-income countries where the burden of cognitive impairment is greatest and rising.
INTRODUCTION
Recent evidence suggests dementia risk is declining or remaining stable in some high-income Western countries including for example, the USA (e.g., declines of 22%, 38%, and 44% in dementia incidence from 1986–1991, 1992–1998, and 2004–2008 versus 1977–1983, respectively [1]) and UK (e.g., 22% decline in incidence 2008–2011 versus 1989–1994 [2]) [3, 4]. This has important healthcare, economic, and social implications and supports findings that dementia risk is modifiable [5]. These changes are hypothesized to be linked to increased cognitive reserve associated with higher education and improved health and living conditions in later born generations. However, it is not clear whether cognitive performance is improving across the whole cognitive spectrum from normal cognitive function to mild cognitive impairment (MCI), in parallel to changes in dementia risk in later born generations.
There is substantial evidence of improvements in cognitive function in later versus earlier born generations in multiple domains including for example, intelligence (fluid and crystalized), memory, and verbal fluency [6]. However, most studies focus on narrow age ranges (e.g., children or young adults), with few restricted to older adults (e.g., ≥60 years), free of dementia. In older populations, studies investigating generational effects in cognitive performance have reported mixed findings depending on sample demographics (e.g., age and sex distributions), how cognition is assessed (including the test battery used, cognitive domain, and cut-off scores for impairment), and sample selection (e.g., non-institutionalized versus population representative and geographical location). Therefore, we performed a systematic review with the aim to determine whether cognitive function in the older population, aged ≥60 years, and dementia free has changed across generations. There were three research questions: 1) Similar to trends seen in dementia [3], has cognition function improved or remained stable over time in older aged generations; 2) Are there differences in time trends depending on the cognitive domain tested or how cognitive test scores are categorized; and 3) What factors could explain observed generational effects? Indeed, if generational effects of improved cognitive function persist across the lifespan into older age, this could potentially explain reductions in dementia risk and highlight new opportunities for enhancing healthy cognitive ageing in future generations.
METHODS
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [7]. The protocol was registered on PROSPERO (CRD42020173933).
PubMed, Embase, and PsychInfo were searched for all original articles published in English before 28 June 2021. Full details of the search strategy are in the Supplementary Methods. Backward citation tracing was used to identify missed articles. Articles were included if 1) they were population-based studies with cognitive function tested in at least two similar populations using uniform procedures and separated by time, i.e., this review included studies investigating period or birth cohort effects; and 2) the sample were aged ≥60 years without dementia at baseline. Studies were excluded if 1) they did not present cognitive data from two or more unique groups sampled at different time periods; 2) the sampling strategy differed across samples/time points; and 3) it was unclear if people with dementia were excluded at baseline. Where people with dementia had not been explicitly excluded but cognition categorized using cut-off scores indicative of being dementia free (e.g., Mini-Mental State Examination (MMSE) scores ≥18) these studies were included. When needed, additional information was obtained by contacting the authors (n = 1 study [8]).
Three reviewers (BCMS, ET, MS) independently screened titles and abstracts, followed by the full text of the selected articles. Data were extracted independently by two reviewers (AG, BB) and checked by a third (EP). Risk of bias assessment used the tool developed by Hoy et al. [9] which includes 10 items to assess internal and external validity scored as 1 (no risk present) and 0 (risk present). This was completed independently by two reviewers (AB, AM). Any disagreements in study selection, data extraction or bias assessment were resolved by consensus. Data extracted included information on study location, sample representativeness, assessment dates/times, demographics (age, sex, education), cognitive test(s) administered (and cut-off scores where applicable), and key results.
Due to large heterogeneity in the methodology across studies a narrative synthesis was conducted for the cognitive test score and cognitive grouping (e.g., MCI) findings. However, there was consistency across some studies in the reporting of generational differences in global cognitive function assessed using the MMSE. Linear and non-linear regression (quadratic, cubic) models were used to identify the line of best fit to the prevalence estimates of different MMSE groups, stratified by location (China, Europe) and cognitive status (no or mild cognitive impairment). The average of the prevalence estimates from each study and for each specific year were calculated and included in the analysis. The graphs were built using Excel for Windows 10 (Microsoft Inc., Seattle, USA) and model goodness of fit was assessed by calculating the coefficient of determination (R2) and the Akaike Information Criterion (AIC) [10] using Statistica 10 for Windows (StatSoft Inc., USA).
RESULTS
The electronic search identified 28,101 articles after excluding 733 duplicates. Following title/abstract sifting, 88 articles were identified for full-text review and 13 selected for inclusion. Three additional articles [11–13] were identified from backward citation tracing and one [14] from a conference abstract; this making a total of 17 papers. On final inspection, five studies [12, 15–18] used data from the Chinese Longitudinal Healthy Longevity Survey; three [15, 18] were retained as they contained non-overlapping results and two [12, 16] excluded. Therefore, 15 articles were included covering generational differences in cognitive function in dementia free individuals aged ≥60 years from 1971 to 2015 (see Supplementary Figure 1: PRISMA flow diagram).
Study characteristics
Across studies, sample size ranged from 97 [19] (Sweden, time analyzed: 2001–2004, 2006–2012 versus 2012-current, in participants aged ≥60) to 13,873 [15] (China, time analyzed: 2002–2008 versus 2008–2014, in participants aged ≥65). Most studies were from China (n = 4 studies [11, 18]), and the USA (n = 4 studies [14, 20–22]) followed by Sweden (n = 3 studies [8, 23]), and one study each from Denmark [24], France [25], Switzerland [26], and the UK [13] (Table 1). Eight studies [8, 24] were nationally representative and three studies [14, 26] were regionally representative. Seven studies [8, 23–25] focused on the very-old (e.g., age ≥70 years) with the remaining studies capturing people aged ≥60 years. Across studies, most participants were female. In seven studies [19–21, 23–26], educational attainment significantly increased over time and in only one study [11] did educational attainment significantly decrease (in China, between 2010 and 2015).
Risk of bias
Total risk of bias scores (range 0 to 10) were categorized into 8–10 “low risk of bias”, 5–7 “moderate risk of bias” and 0–4 “high risk” of bias. As shown in Table 1, no study had a high risk of bias, eight studies had moderate risk of bias, and seven studies had a low risk of bias. Bias was mainly associated with non-response and a short time interval (i.e., < 10 years) for determining generational effects (see Supplementary Table 1 for full bias ratings). Therefore, all 15 studies were included in the evidence synthesis.
Description of each included study and risk of bias score
CIND, cognitive impairment no dementia; MCI, mild cognitive impairment; ns, not significant; UK, United Kingdom; USA, United States of America; y, years.
Generational effects in cognitive function
Supplementary Table 2 shows the key results reported in each study. These are described in separate sections below.
Cognitive test scores
Two studies from Sweden (2001–2004, 2006–2012 versus 2012-current, in participants aged 60 and 81 years [19]; and, 1971/1972 versus 2000/2001, in participants aged 70 years [23]) and one study each from China (2002 versus 2008, in participants aged ≥65 years [17]), France (1991/1992 versus 2001/2002, in participants aged 77–88 years [25]), Switzerland (2005, 2010 versus 2015, in participants aged 65+ years [26]), and the USA (1992 versus 1999, in participants aged ≥65 years [21]) investigated generational effects in cognitive test scores. Numerous tests were administered across the different studies including measures of global cognitive function (e.g., MMSE [17, 26] and the Clock Drawing Test [26]); attention, executive function and speed (e.g., Digit Symbol Substitution Test [25], Digit Cancellation [19], Pattern Comparison [19], Trail Making Test [19, 26], and Identical Forms [23]); fluency (e.g., Isaacs Set Test [25], letter fluency [19], animal naming [19], and fruit and vegetable naming [26]); verbal ability (e.g., Synonyms [23]); spatial ability (e.g., Block Design [23]); inductive reasoning (e.g., Figure Classification [23]); language (e.g., Repetition and Comprehension subtests of the Boston Diagnostic Aphasia Evaluation [21], Wechsler Adult Intelligence Scale-Revised Similarities subtest [21], Boston Naming Test [21], and Letter and Category Fluency test [21]); spatial ability (e.g., Benton Visual Retention Test [21], Rosen Drawing Test [21], and the Identities and Oddities subtest form the Mattis Dementia Rating Scale [21]); metacognition (e.g., Confidence in Test Performance [19]) and memory (Vocabulary (SRB) test [19], general knowledge [19], Benton Visual Renton Test [25], Free word recognition and recall [19], Digit Span Forwards [19, 23], Digit Span Backwards [19, 23], and the Selective Reminding Test [21]). Note, two studies [19, 21] created composite measures (e.g., for language, memory, inductive reasoning, etc.) from the individual test scores.
Results were generally consistent indicating gains or stability in performance in most studies when comparing later to earlier generations depending on the cognitive domain tested and control of confounding factors. Only one study [26] reported declines in test performance (Sweden; 1992 versus 2002, in participants aged 66–71 years) with cognition assessed using the MMSE, verbal fluency, and Clock Drawing Test (in both males and females). As shown in Fig. 1, later born generations performed better on tests of memory (visual working and episodic), processing speed, vocabulary, attention and executive function, spatial ability, and inductive reasoning. However, increased educational attainment over time appeared to drive generational differences in processing speed and episodic memory. Performance on measures of general knowledge, meta-cognition and short-term memory was stable. Performance on the Clock Drawing Test and a composite Trail Making Test score (i.e., Part B-Part A) declined. In contrast, results were mixed for verbal fluency, working memory and global function assessed using the MMSE— either improving, declining, or remaining stable across generations. In addition, controlling for educational attainment attenuated generational differences in verbal fluency and performance on the MMSE.
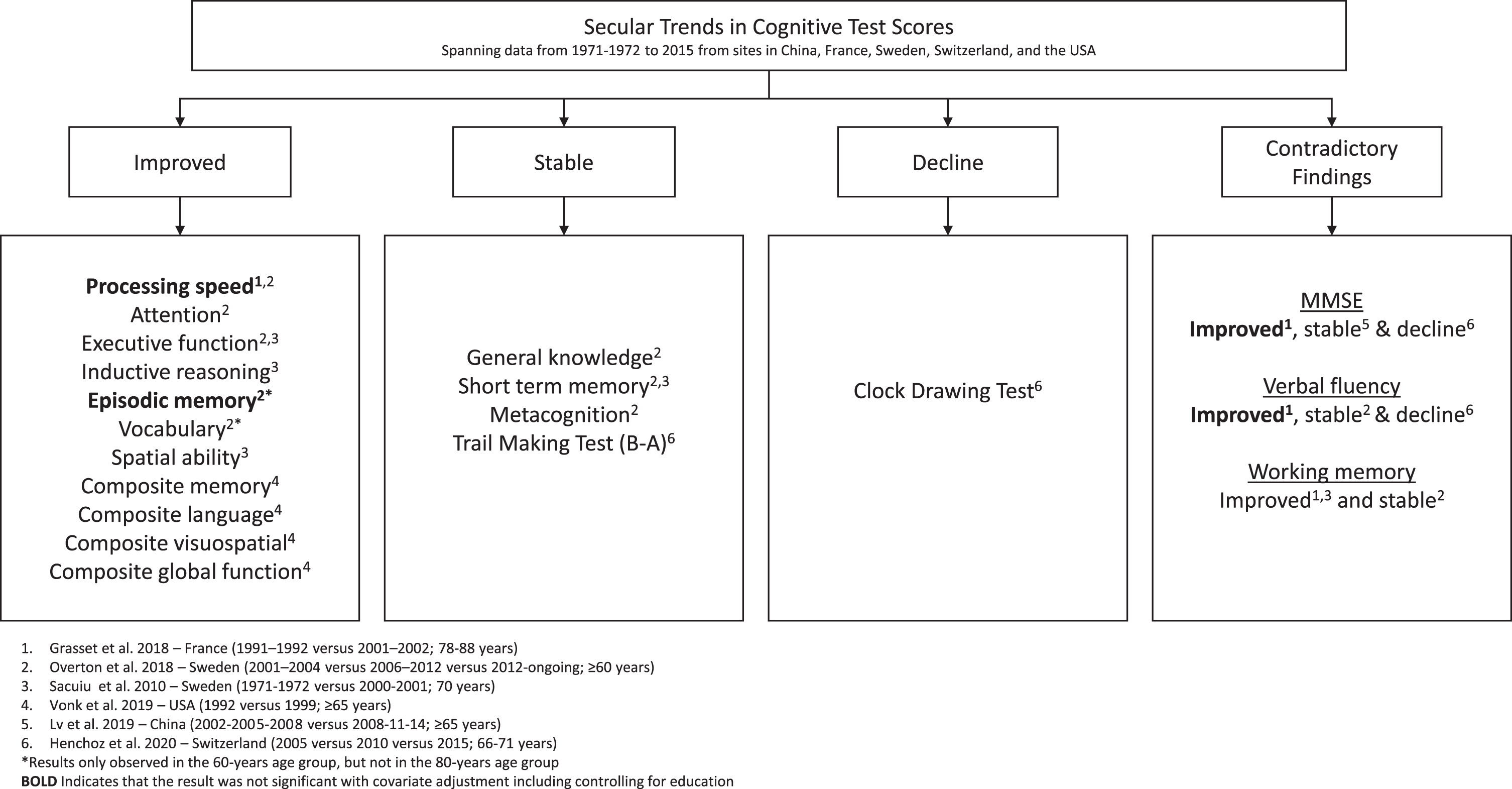
Secular trends in cognitive test scores spanning data from 1971-1972 to 2015 from sites in China, France, Sweden, Switzerland, and the USA.
Rates of change
Where rate of change over time was assessed, later born generations showed slower rates of decline in visuospatial (composite score, USA; 1992 versus 1999, in participants aged ≥65 years [21]), language (composite score, USA; 1992 versus 1999, in participants aged ≥65 years [21]), verbal fluency (Isaacs Set Test, France; 1991/1992 versus 2001/2002, in participants aged 78–88 years [25]), memory (composite score, USA; 1992 versus 1999 [21] in participants aged ≥65 years; and, visual working memory assessed using the Benton Visual Retention Test, France; 1991/1992 versus 2001/2002, in participants aged 78–88 years [25]) and global cognitive function (using a composite score [21], but not the MMSE [17, 25]). No generational effects were observed in executive function and processing speed assessed using the Digit Symbol Substitution Test (France; 1991/1992 versus 2001/2002, in participants aged 78–88 years) [25]. Where cognitive change was classified using MMSE scores (China; 2002 versus 2008, in participants aged ≥65 years) the results suggest an slight increase across generations in participants classified as improving (33.2 versus 37.4%), with no differences in those classified as stable (16.5 versus 15.5%), slow decliners (24.6 versus 23.4%) or rapid decliners (25.7 versus 23.7%) [17].
Cognitive states
Two studies classified cognitive function into groups using Mayo Clinic Criteria for amnestic MCI (aMCI; USA [14] and China [11]), one study [13] used international consensus criteria (UK), one study [20] used criteria for Cognitive Impairment no Dementia (CIND; USA) and one study [22] defined MCI as persons without dementia, but impaired in at least one cognitive domain (MCI-Any, USA). Lu et al. [11] further subtyped MCI into MCI with cerebrovascular disease (executive dysfunction: MCI-VD) and MCI-other (impairments not attributed to AD or cerebrovascular disease: MCI-O).
MCI
In the USA, prevalence of MCI-Any was stable from 1993–1996 (29.3%; 95% CI: 28.2–30.4%) to 2009–2012 (29.0%; 95% CI: 27.9–30.1%) in people aged ≥65 years from the Chicago Health and Aging Project [22]. Similar findings of stability in MCI prevalence were reported in the UK from 1991 (17.6%; 95% CI: 12.5–22.9%) to 2011 (15.2%; 95% CI: 13.5–16.6%), with MCI defined using consensus criteria [13]. Incidence of aMCI was found to be stable from 1993 to 2016, in individuals aged ≥70 years [14] from the Einstein Aging Study (New York); relative rates were not significantly different from one. There was also no effect of sex or race (Black versus White) on the aMCI incidence results [14]. Similarly, in rural areas of Northern China, aMCI prevalence was found to be stable between 2010 (19.0%) and 2015 (18.4%) in individuals aged ≥60 years. In contrast, prevalence of MCI-VD (2.3 and 6.8%, respectively) and MCI-O (1.6 and 2.7%, respectively) significantly increased over time (2010–2015) [11]. Risk of MCI-VD was associated with being female, single (i.e., no spouse) and a history of heart disease.
CIND
In individuals aged ≥65 years in the USA, in unadjusted analyses of the whole sample, there was a significant increase in the prevalence of good cognitive function (67.0 versus 70.9%) and a significant decrease in CIND (21.2 versus 19.7%) when comparing samples in 2000 and 2010 [20]; although the differences in prevalence across years were small. However, when stratified by age, sex, and education most changes were not significant, suggesting overall stability in trends across time for all cognitive groups. In contrast, in the UK, between 1991 and 2011, prevalence of no cognitive impairment increased (14.3% [95% CI: 9.3–19.4% ] versus 22.9% [95% CI: 21.3–24.5% ]) and the prevalence of Other Cognitive Impairment no Dementia (OCIND) was stable (36.8% [95% CI: 30.3–43.6%] versus 40.4% [95% CI: 38.5–42.3% ]) [13].
MMSE scores
Five studies investigated generational effects in cognitive groups defined exclusively using MMSE cut-off scores including two from China [15, 18] and three from Europe: Denmark [24], Sweden [8], and Switzerland [26]. The results were mixed.
China
In individuals aged ≥65 years, when comparing data from 2002–2008 and 2008–2014, the prevalence of the no (i.e., MMSE ≥24; men: 51.6% versus 52.7% and women: 48.4% versus 47.3%, respectively) and mild (i.e., MMSE 18–23; men: 33.5% versus 36.0% and women: 66.5% versus 64.1%) impairment groups was generally stable in both sexes; although there was some suggestion of a decrease in the prevalence of mild impairment in females over time [15]. Using the same data resource, when the population was restricted to those aged ≥80 years, from 1998 to 2014, while there were some fluctuations in prevalence over time, there was no obvious pattern suggesting stability in prevalence of the no (i.e., MMSE ≥24; 53.0%, 57.5%, 47.1%, 49.4%, 43.9%, 48.4%, and 51.2% across seven waves including 1998, 2000, 2002, 2005, 2008, 2011, and 2014, respectively) and mild impairment (i.e., MMSE 18–23; 18.0%, 16.0%, 18.3%, 15.6%, 16.4%, 17.1%, and 17.4% across seven waves including 1998, 2000, 2002, 2005, 2008, 2011, and 2014, respectively) cognitive groups [18]. As shown in Fig. 2a, a cubic curve best approximated the prevalence trends over time in the two Chinese studies and better fit was found in the mild cognition group indicated by the lower AIC score. The results highlight overall stability in the prevalence of the different MMSE groups: no and mild impairment.
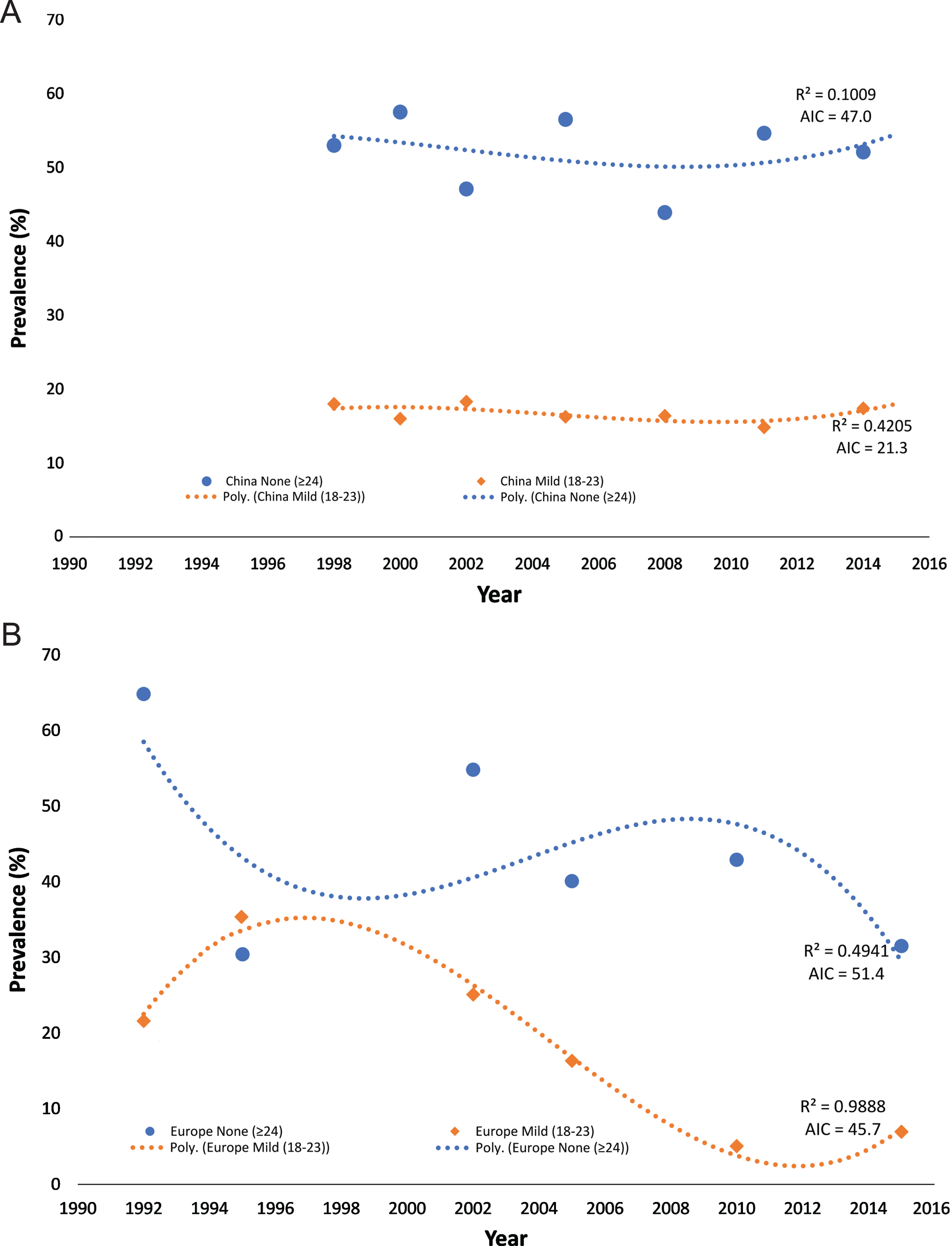
Trends in dementia prevalence in China (A) and in three European countries (B: Denmark, Sweden, and Switzerland). AIC, Akaike Information Criterion; Poly., Polynomial regression; R2, coefficient of determination.
Europe
Similar to the findings from China, a study of centenarians from Denmark found no systematic differences in prevalence over time (1995–1996 versus 2005) for the no (i.e., MMSE ≥24; 28.9% versus 31.8%) or the mild (i.e., MMSE 18–23; 33.3% versus 29.0%) impairment groups [24]. However, there was some suggestion that males living at home had better cognitive performance in the later (versus earlier) born generation and that there was more cognitive impairment in institutionalized participants, namely females, in the later (versus earlier) generation. This possibly due to differences in the availability of home health care services across generations meaning that more people can stay at home in later versus earlier born generations with those in care the people with the most significant cognitive decline. In contrast, in younger participants (aged 66–71 years) in Switzerland, from 2005–2015 the prevalence of mild/serve impairment (i.e., MMSE < 24) was found to remain stable in females (5.6%, 5.0%, and 6.0% in 2005, 2010, and 2015, respectively) and males (5.0%, 5.1%, and 7.9% in 2005, 2010, and 2015, respectively); while the prevalence of unimpaired performance (i.e., MMSE > 28) declined significantly in both males (36.7%, 38.7%, and 28.7% in 2005, 2010, and 2015, respectively) and females (42.3%, 47.1%, and 34.3% in 2005, 2010, and 2015, respectively) over time [26]. Similarly, in individuals aged ≥77 years in Sweden over 10-years (1992 versus 2002), using a short 11-item version of the MMSE, there was a significant decrease in the prevalence of no impairment (10% decrease) and stable prevalence of mild impairment (3.5% increase) [8]. Like the results from China, a cubic model best approximated the prevalence trends in Europe (Fig. 2b). However, the data indicated an overall decline in the no impairment and mild impairment groups with the mild group showing the best fit (i.e., lower AIC score).
DISCUSSION
The main finding of this review is that in the older population who are free of dementia there is evidence of changes in cognitive function across generations for some, but not all cognitive domains/groups. This is consistent with findings of a decrease or stability in dementia risk over time particularly in high-income countries and extends them to dementia free cognitive functioning [3, 4]. While improved cognitive function is often explained by increased educational attainment in later compared to earlier born generations this was not always the case. This suggesting that there is a complex interplay between diverse factors— including for example socio-cultural, healthcare, nutrition, and lifestyle— driving generational changes in brain health and cognitive function.
Overall, later born generations generally show evidence of better performance on tests of memory, executive function, spatial ability, processing speed, vocabulary and attention, and no change on measures of general knowledge, short-term memory, and metacognition. Only one study reported a decline, mainly affecting higher levels of performance on three measures including the MMSE, verbal fluency test and Clock Drawing Test over 10-years (2005, 2010, and 2015) [26]. However, the changes were not considered clinically meaningful, and the authors speculated that the results could possibly be linked to decreasing motivation to engage in cognitive activities in later born generations. Where improvements in cognitive test performance have occurred, they are likely to have multiple casual pathways. Over time, changes in educational attainment (and increased cognitive reserve), physical functioning and improvements in healthcare, health status (e.g., reductions in stroke and cardio-metabolic disease), lifestyle factors (e.g., physical activity and smoking levels), and digitalization/stimulation (e.g., access to internet, use of smart technology, gaming), are likely driving these trends [26, 27]. However, the exact factors contributing to changes in scores across the different cognitive tests remain to be ascertained. This knowledge will be important for informing public health campaigns focused on maintaining good cognitive health at older age.
While numerous studies have shown a decline in the age-specific risk of dementia over the last two to three decades [3], the same pattern was not always observed for prodromal cognitive states. Indeed, rates of aMCI (China [11] and USA [14]), MCI any domain (USA [22] and UK [13]) and CIND (USA [20] and UK [13]) were found to be stable even in the context of declining dementia. There are several possible explanations for differing trends across cognitive groups. First, in later generations there could be a slowing in progression from MCI/CIND to dementia leading to stable MCI/CIND rates but declines in dementia. However, whether rates of progression from prodromal states to dementia have changed over time is unknown. Second, it could depend on how MCI is diagnosed, e.g., the cognitive test battery used and whether cognitive difficulties are considered along with health-related co-morbidity. Indeed, when investigating changes in the prevalence of vascular related MCI, MCI-VD was found to increase in China between 2005 and 2015 consistent with changes in trends of cardio-metabolic health. However, no other study has tested for generational effects in different sub-types of MCI and further work is needed to confirm these results.
MMSE scores when analyzed continuously showed improvement [25] (1991–92 versus 2001–2002, France, 78–88 years), stability [17] (2002–2008 versus 2008–2014, China, ≥65 years) and decline [26] (2005 versus 2010 versus 2015, Switzerland, 66–71 years) across different world regions and age groups. Trends were also heterogeneous when MMSE scores were categorized into groups, including no or mild impairment, despite some overlap in cut-off scores. Cross-cultural differences in interpretation of MMSE test items [28], as well as variability in sampling (e.g., age, sex, educational, and socio-cultural factors) and cut-off scores, across studies may have contributed to the lack of consistency in results. Further research into generational differences in global cognition assessed using the MMSE and other measures is needed to confirm the results.
Strengths and limitations
The study has several strengths. We used broad search terms to minimize the risk of missing relevant articles. Further, most (i.e., n = 11; 73%) studies were undertaken in samples representative of local or national populations enhancing generalizability of the results. However, there are limitations. First, most findings were from a single study and where multiple studies assessed the same cognitive domain the results were often mixed. Indeed, differences in sample characteristics and methodology (e.g., date of testing, temporal distances between generations, age, selection criteria) made it difficult to compare results and may explain some of the contradictory findings. Second, studies could have been missed due to the language restriction (e.g., English) and this could have also led to bias in the analysis comparing China versus other countries. However, we did undertake backward citation searching to minimize missed articles. Third, those studies [17, 25] that reported rates of change in cognitive function over time may be bias by practice effects. Therefore, future studies using alternative test forms will be important for validating these results. Last, apart from China, there were no data representing low- and middle-income countries (LMIC). Even across high-income countries, data are limited to the USA, UK, France, Denmark, Sweden, and Switzerland. Given the differences in the burden of disease associated with cognitive impairment and dementia across world regions, there is an urgent need to determine whether the trends are consistent across different locations globally. This is particularly relevant to LMICs which are experiencing rapid population aging in the context of limited (and often non-existent) older age health policy.
Conclusions
Despite large differences in study design and methodology, there is some consistency that later generations have similar and sometimes better cognitive function to earlier generations. Determining what is driving the changes in trends across the different cognitive domains and cognitive states (including normal functioning, MCI, CIND, and dementia) is an important priority for future research to generate actionable recommendations to ensure that gains in cognitive function continue to be observed in future generations.
Footnotes
ACKNOWLEDGMENTS
This research was funded by the National Institute for Health Research (NIHR) (16/137/62) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care. The authors acknowledge the support of NIHR DePEC (Dementia Prevention and Enhanced Care) team members in this study. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.