
Abstract
Background:
Older age is associated with an increase in altruistic behaviors such as charitable giving. However, few studies have investigated the cognitive correlates of financial altruism in older adults.
Objective:
This study investigated the cognitive correlates of financial altruism measured using an altruistic choice paradigm in a community-based sample of older adults.
Methods:
In the present study, a sample of older adults (N = 67; M age = 69.21, SD = 11.23; M education years = 15.97, SD = 2.51; 58.2% female; 71.6% Non-Hispanic White) completed a comprehensive neuropsychological assessment and an altruistic choice paradigm in which they made decisions about allocating money between themselves and an anonymous person.
Results:
In multiple linear regression analyses that controlled for age, education, and sex, financial altruism was negatively associated with performance on cognitive measures typically sensitive to early Alzheimer’s disease (including word list learning and recall, delayed story recall, and animal fluency).
Conclusion:
Findings of this study point to a negative relationship between financial altruism and cognitive functioning in older adults on measures known to be sensitive to Alzheimer’s disease. Findings also point to a potential link between financial exploitation risk and Alzheimer’s disease in older age.
INTRODUCTION
As individuals reach older adulthood, they are faced with important financial decisions regarding investment of retirement savings, allocation of assets, and transfers of wealth, among many other decisions. Unfortunately, poorer financial decision making has been reported in some older adults compared to younger or middle-aged adults [1–4]. Further, many older adults are the victims of financial abuse and exploitation (e.g., [5, 6]). Thus, understanding factors that promote strong financial decision making in older adults is imperative for optimizing financial well-being, health, and quality of life of this age group [7–11].
Economic preferences, or how one ranks choices based on their relative utility, are known to impact how older adults make financial decisions [12]. One such economic preference is altruism, defined as the motivation to help others even when doing so is costly [13]. Research has found that older age is associated with increased altruistic behaviors such as charitable giving, helping a stranger, etc. [14–16]. Indeed, a recent meta-analysis which reviewed 16 studies of altruism assessed using various methodologies (e.g., self-report, hypothetical choice outcomes) found a robust increase in altruistic behaviors with increasing age [17].
A body of research has investigated factors that may contribute to an increase in altruistic behaviors with increasing age. Age-related changes in cognitive functioning is one such factor that may be relevant in this context (see [16] for review). For example, studies investigating prosocial behaviors like altruism, volunteerism, and other behaviors intended to help others [18], suggest that altruism may be an instinctive and automatic human trait that is inhibited by cognitive control processes [16, 20]. In support of this, experimental paradigms have shown that increasing cognitive load via experimental manipulations increases prosocial behaviors [19]. Such findings suggest that cognitive decline associated with increasing age may weaken deliberative processes that inhibit the more automatic and intuitive prosocial behaviors inherent in individuals (for review, see [16]). However, inferences drawn from studies utilizing timed approaches to measuring altruistic decisions may be misleading given that decisions made quickly under time constraints may reflect mistakes rather than intuitive preferences [21], and there is considerable debate regarding whether altruism is in fact an instinctive trait or represents a more deliberative process (e.g., see [16, 21]).
Findings of increased altruism as a result of experimental manipulations of cognitive load [19] may be interpreted to suggest that more altruistic behaviors will be associated with poorer cognitive functioning. However, studies that have directly examined the relationship between altruism and cognitive functioning have shown positive relationships between the two constructs, and primarily test these relationships in adult samples [22, 23]. To our knowledge, few studies have investigated such relationships in older adults. In a study by Corrêa et al. [24], older adults who were considered more altruistic based on a self-report measure of altruistic behavior had better cognitive performance (also see [25]). In a study by James [26], self-reported charitable giving was associated with better cognitive functioning. While such findings are informative on their own, actual altruistic behaviors versus self-report measures may reveal differences in their associations with cognition, as each may reflect different underlying motivations (e.g., pure altruism vs. norm-guided motivations; see [27]).
The present study aimed to examine the neuropsychological correlates of altruism in a community-based sample of 67 older adults who completed a series of behavioral economics choice paradigms with real monetary outcomes, one of which included an altruistic choice paradigm. Participants also completed a comprehensive neuropsychological assessment as part of their participation. Given conflicting findings from the literature regarding the possible relationships between cognitive functioning and altruism, and the paucity of empirical evidence in older adults, we did not make specific predictions regarding results of our analyses.
METHODS
Participants
Seventy-one adults aged 50 or older were initially recruited to participate in a study of finances, cognition, and health. Participants from the greater Los Angeles area were recruited from senior centers, elder abuse awareness events, and community outreach programs. All participants were screened via telephone for eligibility prior to study enrollment. Exclusion criteria included known signs of cognitive impairment or a diagnosis of dementia, a neurological or psychiatric illness, or current problems with drugs or alcohol. Participants were further screened for significant cognitive impairment on the day of their study visit using the Montreal Cognitive Assessment (MoCA) [28] screening instrument. Per study protocol [29], participants who scored 23 or below on the MoCA [30] were excused from further participation in the study and thanked for their time.
Procedure and measures
On the day of their evaluation, participants completed a series of behavioral and self-report measures including a comprehensive neuropsychological assessment and an altruism choice paradigm. All study procedures were approved by the University of Southern California institutional review board (IRB approval number: HS-16-00902). Consent to participate in the study was provided by all study participants.
Altruism choice paradigm
During this portion of the study, participants were informed that they were matched with another person, Person B, who was participating in this part of the study anonymously online. They were informed that Person B would never know who they are, and they would never know who Person B is. In order to avoid deceiving participants, anonymous online participants were recruited through MTurk to serve as Person B. There was no direct interaction between the anonymous online participants and study participants. Participants were then told the following: “You have the opportunity to send a portion of your $10 to Person B. You can send any amount between $0 and $10. Any amount you keep will be added to your earnings at the end of the study today. Any amount you send will be added to Person B’s earnings at the end of the study today.” Participants were then asked to select one of 10 options in $1 increments ranging from sending $0 to Person B up to all $10 to Person B. Thus, those who selected to send $0 to Person B can be considered least altruistic while those who chose to send all $10 can be considered most altruistic. Participants also completed four additional economic choice paradigms during their study participation that assessed other economic preferences including time, risk, and trust. Following completion of all the paradigms, a lottery system was used to select which one of the five economic choice paradigms would add to their study earnings. As such, only the specific decisions the participant made for the particular paradigm selected in the lottery would be those that contributed to their final study earnings. For the present study, only the altruism choice paradigm was examined.
Neuropsychological assessment
Participants completed the California Verbal Learning Test, second edition (CVLT-II) [31], and measures within the Uniform Dataset 3 (UDS 3) neuropsychological battery [32]. These included the Montreal Cognitive Assessment (MoCA), Craft Story 21 immediate and delayed recall (total scores), Benson complex figure copy and recall (total scores), number span forward and backward (total correct trials, and longest span), total score on the Multilingual Naming Test (MINT), verbal fluency phonemic test (combined total of F-words and L-words), category fluency (animals total score; vegetables total score), trail making test part A, and trail making test part B. The CVLT-II involves reading a 16-item word list to participants who are then asked to freely recall as many words as they can from the list. These initial learning trials were repeated five times. The sum of these five immediate recall trials were considered in the present study (CVLT-II List A Total). Following the five learning trials, a distractor word list (List B), was read to participants who were then asked to recall words from the distractor list (CVLT-II List B Total). Following this, participants were asked to freely recall words from List A (Short Delay Free Recall), and then provided with category cues (Short Delay Cued Recall). After a twenty-minute delay in which participants completed other cognitive assessments, the free and cued recall trials were repeated (Long Delay Free Recall; Long Delay Cued Recall).
Demographic variables
Sex (1 for male; 0 for female), age and education (in years) were assessed. Income was assessed on a 16-point scale. Participants were asked to select the category that most represents the total combined income of all family members living in the household during the past 12-months, “including money from jobs, net income from business, farm or rent, pensions, dividends, interest, Social Security payments, and any other monetary income received by members of the family who are 15 years of age or older.” Response options ranged from 1 (“less than $5,000”) to 16 (“$150,000 or more”). As a point of reference, a response of 8 indicated “$25,000 to $29,000.”
Statistical analyses
Bivariate associations between altruism and demographic and neuropsychological variables were assessed using Spearman correlations or one-way ANOVAs. Multiple linear regression models regressed altruism on those cognitive tests that were significantly related to altruism in bivariate analyses. In these models, age, education, and sex were included as covariates.
In a set of additional analyses, altruism was considered as a categorical variable in order to examine whether significant correlations between altruism and cognitive tests were driven by a particular response set on the altruism game. Participants were divided into one of three groups based on their response to the altruism choice paradigm. Specifically, those who selected to give more money to Person B than to themselves were included in the “Gave More” group (GM). Those who selected to give less to Person B than to themselves were included in the “Gave Less” group (GL). Finally, those who selected to give an equal amount to themselves and to Person B were included in the “Gave Equally” group (GE). We then ran one-way ANOVAs and post-hoc Tukey HSD tests to examine differences between groups on each cognitive test that yielded significant correlations with the continuous altruism score.
RESULTS
Participant demographics
Of the 71 participants enrolled in the study, four were excluded from analyses due to not participating in the altruism choice paradigm. This left a total of 67 participants available for data analysis (M age = 69.21, SD = 11.23; M education years = 15.97, SD = 2.51; 58.2% female). Participant demographics and scores on each of the neuropsychological tests are reported in Table 1. With regard to race breakdown, 48 participants (71.6%) self-reported Non-Hispanic White race. Four participants reported Non-Hispanic Black race (6.0%), nine reported being of Asian descent (13.4%), one reported ‘other’ (1.5%), and one reported ‘unknown’ (1.5%). Four participants reported being of Hispanic descent (6.1%). Distribution of altruism scores are presented in Fig. 1.
Sample demographics, scores on neuropsychological tests, and bivariate associations with the financial altruism score
aResults of one-way ANOVA comparing males to females on the altruism score and White to non-White participants on the altruism score. M, mean; SD, standard deviation; s, seconds; MoCA, Montreal Cognitive Assessment; MINT, multilingual naming test.
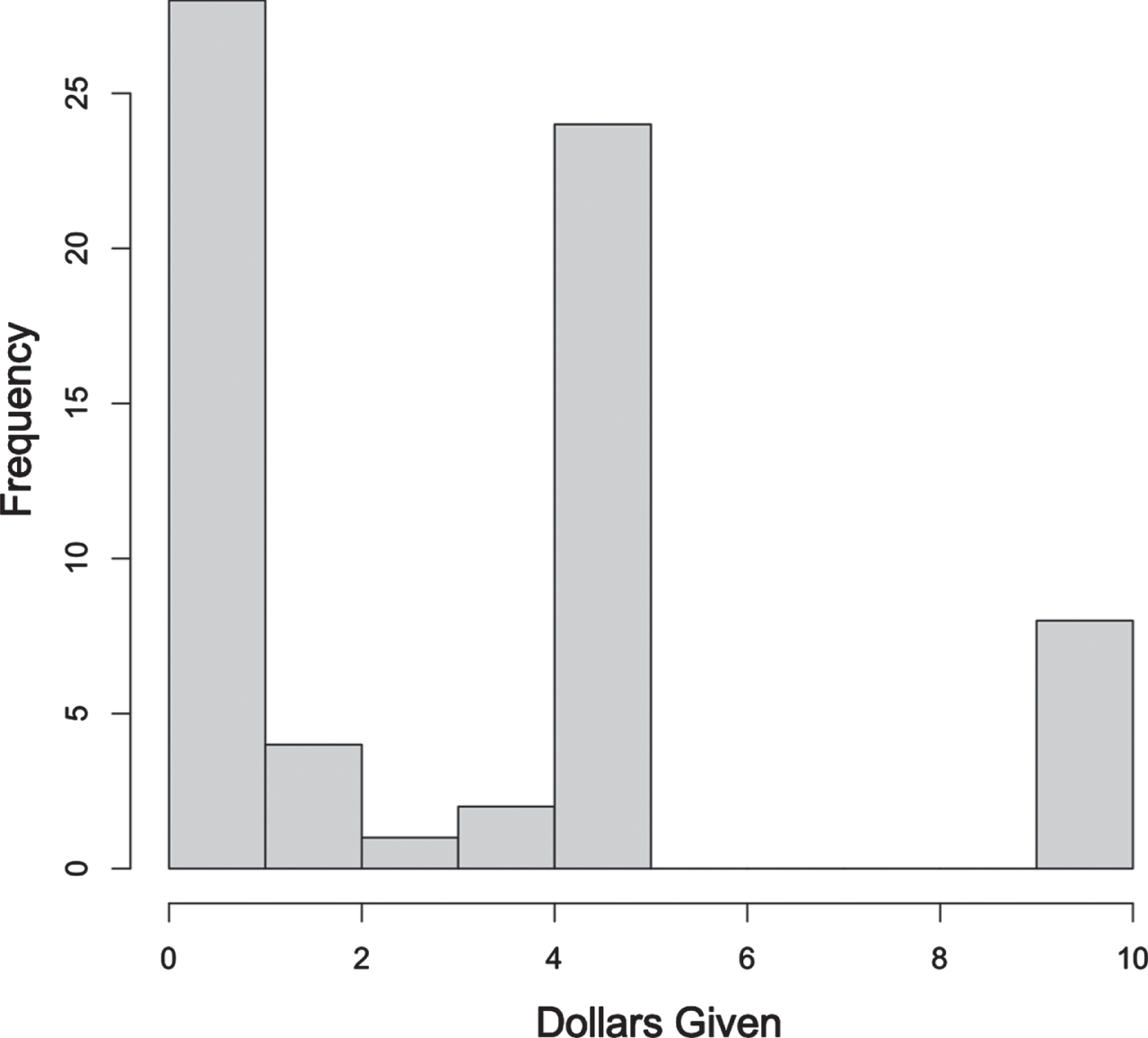
Histogram displaying frequency of altruism scores for the 67 participants in the study sample. Scores range from $0 given to $10 given.
Bivariate associations
Results of the bivariate associations with altruism are also reported in Table 1. In bivariate Spearman correlations, the financial altruism score was not associated with age, education, income level, or total score on the MoCA. One-way ANOVA analyses revealed that altruism scores did not differ significantly between males and females in the study sample, or between non-Hispanic White and non-White participants.
With regard to cognitive outcomes, the altruism score was significantly negatively associated with total words immediately recalled on CVLT-II List A, short delay free recall, and long delay cued recall. The altruism score was marginally negatively associated with long delay free recall on the CVLT-II. The altruism score was also negatively associated with the delay recall trial of Craft Story 21 and total score on the MINT. The altruism score was marginally negatively associated with animal list generation.
Multiple linear regression analyses
We ran multiple linear regression analyses for those cognitive outcomes which were marginally or significantly associated with financial altruism in bivariate analyses. Model statistics and coefficients for main effects are reported in Table 2. After controlling for age, education, and sex, financial altruism remained significantly negatively associated with total words immediately recalled on the CVLT-II List A, CVLT-II short delay free recall, and CVLT-II long delay cued recall. Specifically, a one standard deviation increase in the altruism score resulted in a 0.29 standard deviation decrease in the CVLT-II List A Total score, a 0.26 standard deviation decrease in the CVLT-II Short Delay Free Recall Score, and a 0.25 standard deviation decrease in the CVLT Long Delay Recall Score. The financial altruism score was also significantly negatively associated with delayed recall of Craft Story 21 and animal fluency, such that a one standard deviation increase in the altruism score was associated with a 0.32 standard deviation decrease in Craft Story 21 delayed recall, and a 0.27 standard deviation decrease in animal fluency. The main effect of financial altruism on the MINT total score was marginal.
Results of the multiple linear regression analyses between financial altruism scores and cognitive outcomes, adjusting for demographic covariates
B, standardized beta coefficients; CVLT-II, California Verbal Learning Test, second edition; MINT, multilingual naming test.
Analyses with altruism as a categorical variable
Altruism was also considered as a categorical variable to examine whether findings were driven by a specific response option in the economic paradigm involving altruistic choices. There were 35 participants who gave less than $5 to Person B and were thus included in the Gave Less (GL) group. Twenty-four participants gave $5 and kept $5 and were included in the Gave Equally (GE) group. Eight participants gave all $10 to Person B and were included in the Gave More (GM) group. There were no participants who gave between $6 and $9 to Person B, thus the GM group represented only participants who gave all $10 to Person B. Means and standard deviations of demographic variables and neuropsychological test scores are presented in Table 3.
Participant demographics and neuropsychological test scores by financial altruism group
Gave More, participants who gave $6 or more; Gave Equally, participants who kept $5 and gave $5; Gave Less, participants who gave $4 or less. MoCA, Montreal Cognitive Assessment; CVLT-II, California Verbal Learning Test, second edition; s, seconds; MINT, multilingual naming test.
Results of the one-way ANOVA models, and the post-hoc Tukey tests are presented in Table 4 and displayed in Fig. 2. Groups did not differ with regard to age, education, sex breakdown, race breakdown, income, and total scores on the MoCA (all ps ≥ 0.28). With regard to group differences on neuropsychological tests, groups significantly differed on total words immediately recalled on CVLT-II List A, short and long delay free recall, and long delay cued recall (all ps ≤ 0.05). Groups also differed on the delayed recall trial of Craft Story 21 (p = 0.033). There were no differences between groups on the immediate recall trial of Craft Story 21, animal list generation, or total score on the MINT. Post-hoc Tukey tests were conducted for those tests in which the one-way ANOVAs were significant (see Table 4). Significant group differences appear to be mostly driven by the GL versus GM pairwise comparisons, such that the GL group demonstrated higher performances than the GM group. This was the case for the immediate recall trial of CVLT-II List A, CVLT-II long delay free recall, CVLT-II long delay cued recall, and the delayed recall trial of Craft Story 21. Post-hoc analyses for the CVLT-II short delay free recall trial revealed that the GL group achieved marginally higher scores than the GE group on this portion of the CVLT-II. The same pattern of differences was observed for GL versus GM on this test, although this pairwise comparison did not approach significance.
Results of one-way ANOVAs comparing altruism groups
1Chi-square test of independence. GE, Gave Equally; GM, Gave More; GL, Gave Less; MoCA, Montreal Cognitive Assessment; CVLT-II, California Verbal Learning Test, second edition; MINT, Multilingual Naming Test.
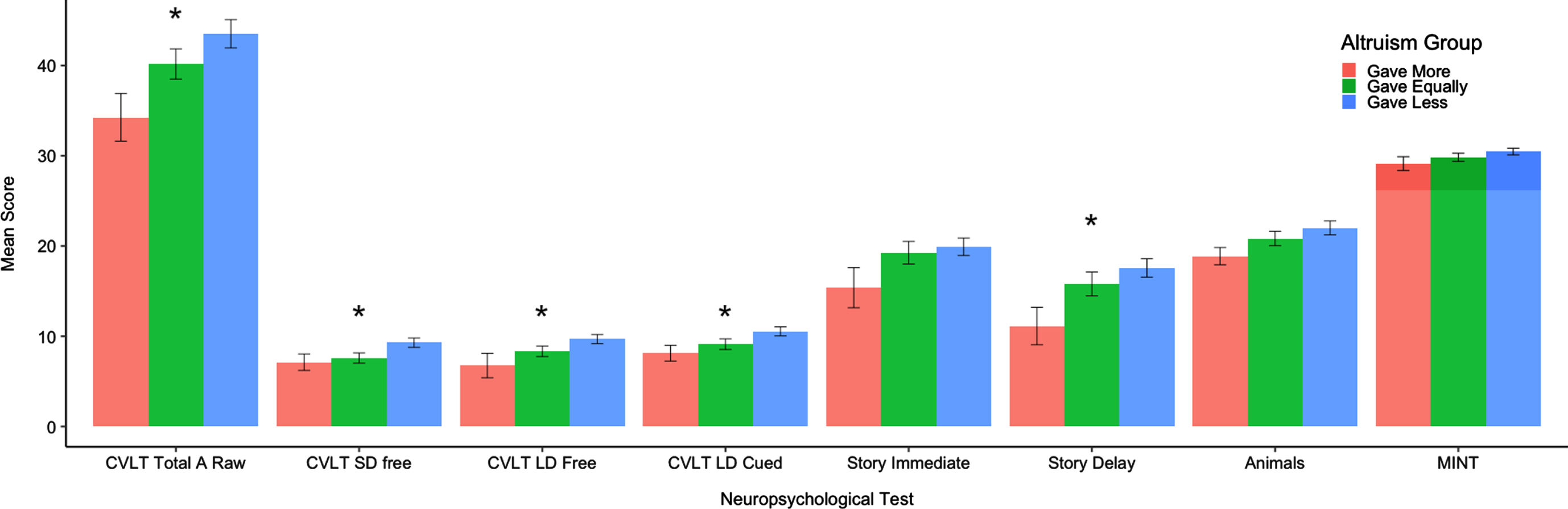
Bar plot of average scores across the neuropsychological tests for each of the three altruism groups. The three groups represent those who gave more to an anonymous person than they kept for themselves, those who gave equally (gave $5 and kept $5), and those who gave less to an anonymous person than they kept for themselves. Significant group differences (p < 0.05) are labeled with an asterisk. CVLT, California Verbal Learning Test; SD, short delay; LD, long delay.
DISCUSSION
This study investigated the neuropsychological correlates of altruism measured during a behavioral altruism choice paradigm involving real monetary outcomes in a community-recruited sample of older adults. We found greater altruism to be associated with poorer performance on several neuropsychological tests involving list learning and recall, delayed story recall, picture naming, and animal fluency. With the exception of picture naming on the MINT, relationships remained significant after adjusting for demographic covariates including age, sex, and education. In this study, altruism was not related to measures of visual memory, attention and working memory, phonemic fluency, and executive functioning. Findings were similar when we considered altruism as a categorical variable and examined group differences in performance on neuropsychological tests, such that the GM group demonstrated the lowest performance on neuropsychological tests and the GL group demonstrated the highest performance.
Findings in this study are in contrast to previous studies that have examined the neuropsychological correlates of altruism in older adults and reported positive associations between altruism and neuropsychological functioning [24–26]. For example, Corrêa et al. [25] found increased altruism to be associated with higher scores on the Mini-Mental State Examination, animal fluency, and CERAD Word List recall. It is possible that differences between studies are due to differences in how altruism was measured. Findings of the Corrêa et al. [25] study are based on a self-report measure of altruism in which participants were asked to report their engagement in altruistic behaviors, some of which do not involve money (e.g., “I have given directions to a stranger”). In contrast, our study utilized outcomes of a behavioral economics paradigm with real monetary outcomes. Differences in methodologies may explain differences between the studies. For example, one’s impressions of his or her degree of altruism may differ from their actual behaviors involving monetary consequences (e.g., see [27]), and as such, neuropsychological correlates may also differ between these two measures of altruism. In our particular study, the decision to give all $10 (no one gave between $6 and $9) may reflect poor ability to make a rational choice rather than an unselfish motivation. To clarify the impact of different methodologies on cognitive findings, future studies may consider including both behavioral and self-report measures of altruism.
Greater altruism was related to poorer performance on measures of episodic and semantic memory, functions commonly vulnerable to early Alzheimer’s disease (AD) pathology [33–36]. This is a novel finding that to our knowledge has not been reported before, and thus requires further research. The neuroimaging literature may provide some insight into the nature of this finding. In one study by Rilling et al. [37] using a sample of University students, the authors found that unreciprocated cooperation (i.e., cooperating with a partner who does not cooperate in return) was associated with greater activity in the bilateral anterior insula, left hippocampus, and left lingual gyrus compared to reciprocated cooperation. The authors suggest that such regions are particularly responsive to non-reciprocation of cooperation and may be activated specifically when a person believes a partner is uncooperative [37]. These brain regions are also known to be vulnerable to age-related neural changes and AD pathology and are important for episodic and semantic memory functioning [38–40]. Thus, changes to the integrity of these regions may play a role in the age-related increases in altruistic behaviors observed in the literature (for review, see [17]), although this is speculative and requires investigation. For example, if a person has encoded many past experiences of unreciprocated cooperation, he or she may be less likely to engage in future altruistic behaviors. Conversely, if such encodings become less available due to age-related changes to the integrity of brain regions underlying these associations, a person may still engage in altruistic behaviors despite past negative experiences. Future studies may consider investigating such a possibility.
Altruism is an economic preference that plays an important role in financial decision making [4]. Recent studies suggest that poor decision making may be a very early sign of impending AD [41, 42]. Additionally, work from our group and others that have examined neural correlates of financial vulnerability and exploitation of older adults have reported associations with regions vulnerable to age-related neuropathological changes (e.g., susceptibility to scams [43, 44]; financial exploitation experiences [45, 46]). For example, a study by our group utilizing a subset of the present sample found altered hippocampal connectivity in older adults who reported a perceived financial exploitation experience compared to those who did not [46]. Given the present findings of associations between altruism and cognitive functions commonly implicated in early AD (e.g., [33]), it is possible, though at this point very speculative, that an increase in altruistic behavior may also signal early changes associated with AD. Further research is needed to support such a speculation.
Another possible explanation for the observed findings is that episodic and semantic memory may be involved in the process of deciding to be less altruistic. This relationship may be task and/or study specific. For example, it is possible that participants in our study who decided to give less or give equally were able to more accurately recall the rules of the economic choice paradigms used in this study (i.e., that their decision will directly affect the amount of monetary reward they receive at the end of the study). It is also possible that these cognitive functions play a role in altruistic behaviors more generally. One way in which they may do so may be explained via the dual systems hypothesis (e.g., [19, 20]). According to the dual systems hypothesis of prosocial behavior, the expression of altruism is determined by two interactive systems. The first system is automatic and reflexive, while the second is dominated by deliberation and cognitive control. According to this approach, people are intuitively prosocial, and only through deliberation and engagement of control mechanisms can the innate altruistic tendency be suppressed [20]. Thus, older adults experiencing even subtle levels of cognitive decline may be less able to suppress innate prosocial tendencies [16]. In line with this hypothesis, we would have expected to see neuropsychological tests involving executive control functions to be particularly associated with increased altruism, and this was not the case. However, episodic and semantic memory may also be part of the cognitive processes that underlie altruistic decisions (e.g., see [47] for a discussion of the role of memory systems in dual process models), although more research is needed to investigate such a possibility.
Importantly, in examining altruism categorically, we found that the group that gave more (GM) was comprised of only individuals who gave all $10. In other words, no participants in our sample gave between $6 and $9. It is possible that negative associations between altruism and cognition are driven solely by individuals who are willing to give all their earnings to an anonymous individual. Generally, those who gave equally (GE; gave $5 and kept $5) did not show significant differences with those who gave less (GL; gave $4 or less) on the cognitive measures examined. Thus, it is possible that altruism at the complete expense of one’s own benefit (rather than choosing an equal option for both parties) may be particularly relevant when considering negative associations with cognitive functioning.
The findings of this study are not without limitations. First, this is a highly educated and predominantly Non-Hispanic White sample. As such, generalizability of findings may be limited. Second, although we measured altruism objectively by using an economics choice paradigm, the paradigm was administered by a research assistant, and the presence of a person in the room may have affected participant responses. We took steps to minimize this potential response bias by providing participants with the response form and placing the research assistant directly across from the participant such that the specific response chosen by the participant would not be monitored by the research assistant. However, this does not completely eliminate the possibility that participants chose certain options due to being observed. Additionally, results of this study are cross-sectional and thus the temporal nature of associations between financial altruism and cognition cannot be concluded. Longitudinal studies are needed to clarify the temporal nature of these associations in older adults (e.g., see [24]). An additional limitation relates to our cognitive battery, which does not include measures that directly map onto financial decision making. Development of a neuropsychological test that captures financial decision-making ability will not only provide more information regarding cognitive correlates of altruism and other economic preferences, it is also imperative given recent studies suggesting that poor decision making may be a very early sign of future AD [41, 42]. Future studies may also consider examining social and emotional correlates of altruism, given that altruism is not a purely cognition-dependent construct. Additionally, while research has shown that altruistic behaviors increase with aging [14–16], it is likely that there are individual differences in baseline altruistic tendencies in younger adulthood which may impact the degree of change in altruism observed as one ages. Future research may consider examining how cognition maps on to degree of change in altruistic behaviors. It is possible that the findings observed in this study are specific to individuals who do exhibit a change in altruistic behaviors (rather than those who have always been altruistic).
This is one of the first studies to our knowledge that has investigated the relationship between financial altruism and cognitive functioning in a community-based sample of older adults. Findings of this study point to a negative relationship between altruism and cognitive functioning in older adults. Future studies are needed to understand possible mechanisms behind this relationship. The findings of this study provide insights into how some adults may become vulnerable to financial exploitation in older age and add to an increasing body of literature suggesting that declines in financial decision making in older adulthood may be an early sign of adverse cognitive outcomes associated with AD.
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants from the NIH (RF1AG068166) and the Elder Justice Foundation awarded to SDH, NIA (T32AG000037) to ACL, as well as the Department of Family Medicine of the University of Southern California. Some participants from the present study were recruited with the help of the Alzheimer’s Prevention Registry. The Alzheimer’s Prevention Registry is supported by a grant from the National Institute on Aging (R01 AG063954). The Alzheimer’s Prevention Registry has been supported by the Alzheimer’s Association, Banner Alzheimer’s Foundation, Flinn Foundation, Geoffrey Beene Gives Back Alzheimer’s Initiative, GHR Foundation, and the state of Arizona (Arizona Alzheimer’s Consortium). The content is solely the responsibility of the authors and does not necessarily represent the official views of the named funders. The authors acknowledge Caroline Nguyen for her help with management of the study and data collection.