
Abstract
Background:
There is currently a lack of a comprehensive review identifying the broad scope of factors that impact quality of life (QoL) of informal carers of people with dementia in order to validate existing measures and inform the provision of support services for carers of people with dementia that impact QoL domains important to them.
Objective:
To explore and identify QoL impacts on informal carers from providing care to people with dementia.
Methods:
A systematic review was conducted across four databases: EMBASE, CINAHL, PsychINFO, and Medline. Eligible studies consisted of published, peer-reviewed, qualitative studies focusing on lived experiences of informal carers of people with dementia. Non-English studies and quantitative studies were excluded. Screening of included studies was conducted independently by three reviewers. A “best-fit” framework synthesis was used to combine the qualitative data, applying deductive and inductive analysis techniques. Quality assessment was conducted using the Critical Appraisal Skills Programme.
Results:
Of the 4,251 articles identified, 59 articles were included. Five main themes pertaining to QoL aspects were identified that included coping (emotion-coping and problem-coping), relationship with the person with dementia (sense of loss and change in relationship), support (formal support and informal support), interference with life (control over caring situation, and freedom and independence), and health (physical health, emotional and mental health, and social health).
Conclusion:
This study identified domains of QoL that are impacted by providing informal care to people living with dementia, offering a conceptual framework for instrument validation and development as well as guidance for service provision.
INTRODUCTION
It is estimated that more than 55 million people have been diagnosed with dementia globally [1]. Dementia is a complex illness characterized by various levels of cognitive impairment, including forgetfulness, loss of speech, and physical impairment [1]. Several countries in Europe, Australasia, and North America have developed, or are in the process of developing, government policies addressing dementia-related care [2]. The total annual costs of dementia are estimated to be up to $70,911 per patient, with informal care costs identified as the main component, followed by residential care and the cost of medications [3]. Further, the total estimated cost of informal caring of people with dementia in high-income countries is 38 times more than the cost in low-income countries likely due to the increased use of direct medical cost and more people utilizing social care services [2].
People living with dementia are commonly supported by informal carers [1, 2]. People who often assume the role of informal carers are partners, family, and friends of people with dementia [1, 4]. Additionally, neighbors, community members, and other volunteers may contribute to an integrated caring system in the form of a supplementary informal caring role but may not have as much involvement as the primary caregiver [2]. Informal carers commonly assist with daily activities for people with dementia. Although caring for a person with dementia can be enriching and fulfilling and some carers have a positive experience [5], carers more often experience negative psychological, social, economic, and health impacts associated with the caring role [1, 6]. The challenges experienced by informal carers supporting a person living with dementia can have a significant impact on carers’ quality of life (QoL). QoL is defined as a multi-faceted construct aimed at studying different aspects of a person’s wellbeing and functioning from a physical, emotional, and social perspective [7].
In recent years, there has been an increase in studies evaluating the effectiveness of support services and interventions for carers of people with dementia to help maintain and improve their QoL [8]. Formal support interventions evaluated have included educational and training programs, support groups and psychological counselling. Such interventions have been implemented in-person, telephone-based, and online support [9, 10]. Outcomes of these interventions show only low to moderate benefit in improving carers’ QoL, perhaps due to the differing needs and challenges experienced by carers [9, 10]. Factors shown to impact carers’ needs include carers’ age, gender, stage of dementia of the care recipient, management of multiple roles and responsibilities, and access to and quality of informal support and formal support [9, 11]. Other formal support services for people with dementia include use of respite care, day care, and residential care.
Recognizing that QoL has become a key outcome measure in health services research and government policies that aim to improve carers’ QoL [12], the evaluation of formal support services requires comprehensive QoL instruments to capture important aspects of caring and reflect changes in carers’ QoL following health services or policy changes or comparisons of these. This requires the use of standardized measures to enable these changes or comparisons across support services and interventions. Current QoL measurement tools include generic measures that focus on health-related aspects of QoL, such as the EQ-5D instruments [13], or generic instruments that focus on carer-specific QoL, such as the Adult Social Care Outcomes Toolkit for Carers (ASCOT-Carer), Care-Related Quality of Life (CarerQol), or Carer Experience Scale (CES) [14]. Further, recognizing that providing informal care to a person living with dementia may involve unique experiences of caring, specific measures for dementia carers have been developed [15], such as the carer quality of life (CGQoL) [16].
Many instruments have been developed de-novo, involving qualitative and quantitative approaches. However, the identification of domains of QoL to inform the content of existing measures was study-specific, involving often small samples. Currently, there is no systematic review and synthesis of qualitative data investigating QoL domains most relevant to carers of people with dementia. A previous review exploring the factors associated with the QoL of family carers of people with dementia included predominantly quantitative studies [17]. Synthesis of qualitative studies to date have mainly focused on carers’ perception of negative and positive aspects of caring or the psychosocial impact of caring [11, 18]. What is currently missing is a synthesis of qualitative studies, identifying domains of QoL important to carers of people living with dementia. Such synthesis is important to validate existing measures and inform the need for new measures, as well as to inform and guide the provision of support services for carers of people with dementia that impact QoL domains important to them [19]. Therefore, this paper aims to explore and identify the QoL impacts of providing informal care to persons living with dementia via the use of systematic review techniques.
MATERIALS AND METHODS
The systematic review protocol was developed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement (PRISMA) and registered in the International Prospective Register of Systematic Reviews, PROSPERO (CRD42021284376) [20]. This review adheres to the dementia language guidelines published by Dementia Australia and will use the following terms interchangeably when referring to persons with dementia: person with dementia, people with dementia, and care-recipient [21]. We use the term ‘informal carers’ describing the unpaid care provided by family members, friends, community members or neighbors.
Search strategy and selection criteria
Four bibliographic databases were searched: EMBASE, CINAHL, PsycINFO, and Medline. The initial search was conducted from inception to 4 June 2019, followed by an updated search on 26 March 2021 to capture more recent qualitative studies. A combination of the following terms, their synonyms, and MeSH terms were used: ‘dementia’ and ‘carer’ and ‘experience’ or ‘quality of life’ or ‘wellbeing’ and ‘qualitative research’ or ‘focus group’. The full search strategy is included in the Supplementary Material (see Supplementary Table 1).
The eligibility criteria are outlined in Table 1. Included studies consisted of qualitative studies and mixed methods studies with a qualitative aspect to investigate lived experiences of informal carers supporting a person with dementia and the associated impact on carers’ QoL. Studies were limited to developed countries to address the QoL impact on informal carers of countries with higher level of access to formal support services and utilization of social care services [1, 2]. Developed and developing countries were classified according to the World Economic Situation and Prospects (WESP) to represent the economic conditions of individual countries [22].
Eligibility criteria for inclusion or exclusion of studies
Stages of screening
Prior to the screening process, references were imported into a reference manager tool, EndNote X9 [23], and duplicates were removed. A free web and mobile app used for conducting systematic reviews, Rayyan [24], was used to independently screen titles and abstracts of search results by three reviewers (SA, LE, and JB) against the eligibility criteria. In the next step, full-text articles were retrieved and assessed according to the eligibility criteria by the same three reviewers. Full-text articles that met the eligibility criteria were included and any disagreements were resolved through discussion between two reviewers (SM and LE or JB and LE) until consensus was reached.
Quality assessment
The Critical Appraisal Skills Programme (CASP) tool for qualitative studies was used to assess the quality of eligible studies. The CASP tool consists of ten questions, covering a broad range of methodological aspects of a study [25]. Instead of excluding studies based on their quality, we used the CASP tool to identify potential strengths and limitations of each study applying one of three responses: ‘Yes’ when a criterion was fulfilled; ‘Can’t tell’ when unsure about whether a criterion was fulfilled; and ‘No’ when a criterion was not fulfilled. When a study had inadequate information for one or more criterion, a ‘Can’t tell’ response was applied.
Data extraction and analysis
Data extraction included the following study characteristics: author, year of publication, country, research questions/study aims, carer characteristics and sample size, qualitative methodology used, type of analysis applied, and research probing questions used in the study.
Data analysis and synthesis was conducted using a “best-fit” framework synthesis approach informed by an a priori framework [26]. The a priori framework was drawn from a previous study conducted by the authors, which explored the constructs of three carer-related preference-based measures (ASCOT-Carer, CES, and CarerQol) [14]. The domains used to inform our a priori framework included: relational problems, control over caring, fulfilment from caring, self-care, physical health problems, mental health problems, financial problems, personal safety, social participation, occupation, space and time to be yourself, support from family and friends, and assistance from organizations and the government [14].
Direct quotes, themes, and authors’ interpretations were extracted from the results section of included studies and collated. A deductive approach was used, whereby informal carers’ experiences were coded against the a priori framework by two reviewers (SE and LE). At the same time, both reviewers applied an inductive, interpretive approach using thematic analysis to identify additional themes and refine the a priori coding framework [26]. Final themes were developed based on the a priori framework and new themes derived from the thematic analysis during an iterative process, which involved constant comparisons and discussions between the two reviewers.
RESULTS
In total, 59 articles were included in the review. The results of the literature search and selection process are summarized in Fig. 1. A detailed summary of study key characteristics is provided in Supplementary Table 2. Studies were published between 1989 to 2021 across Europe (n = 31), North America (n = 21), and Oceania (n = 7). The United States of America (n = 18) had the highest number of studies, followed by the United Kingdom (n = 11) and Australia (n = 6). Sample sizes ranged between 3 to 280 participants, aged from 8 to 90 years of age. The primary focus of the studies on caring experience were from the perspective of: partner carers (n = 20) [27–46]; adult children carers (n = 4) [47–50]; young carers (n = 3) [51–53]; rural and urban family carers (n = 1) [54]; siblings (n = 1) [49]; women (n = 3 wives, n = 1 daughters, and n = 1 wives and daughters combined) [27, 56]; and men (n = 2 sons, and n = 4 husbands) [30, 50].
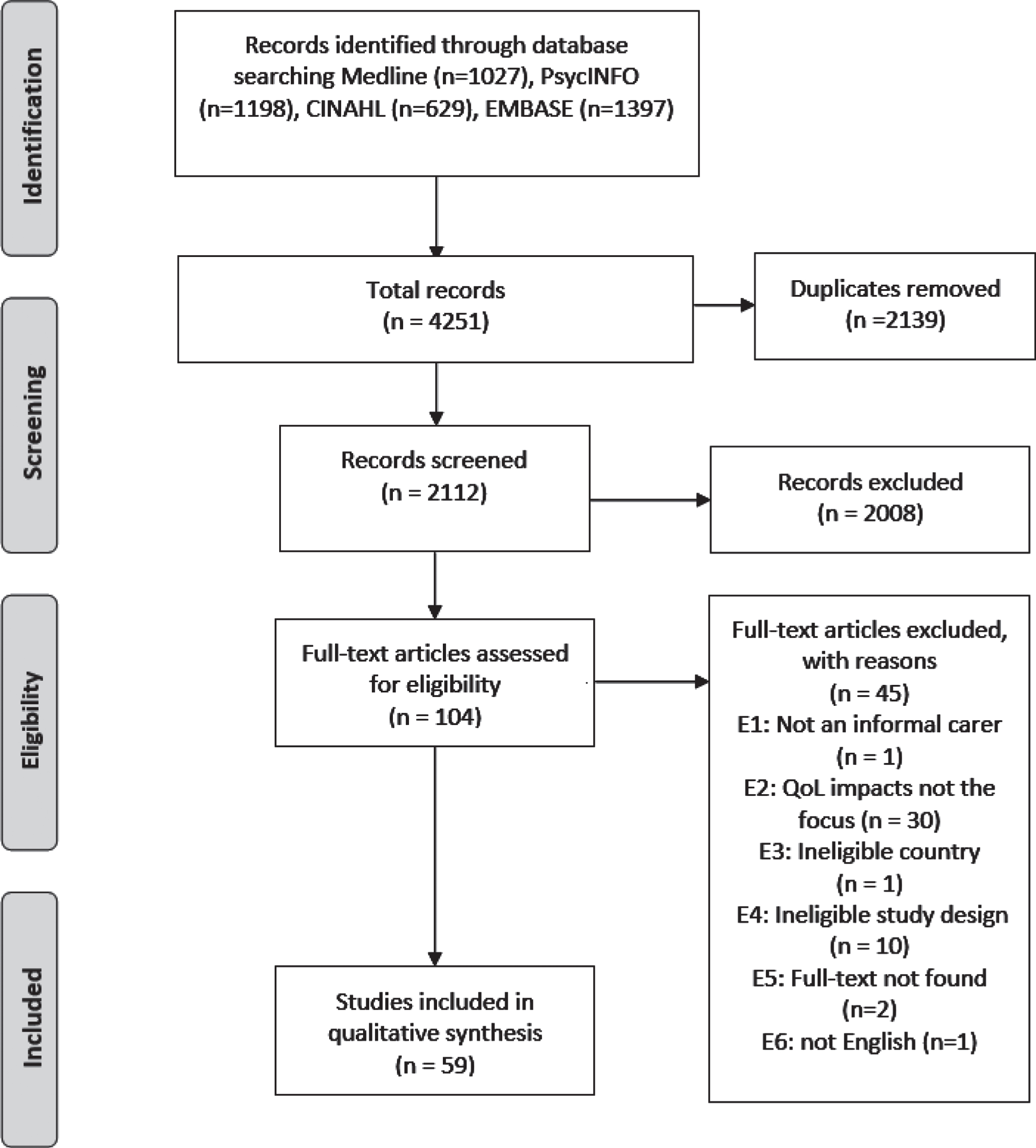
PRISMA flow diagram.
Results of CASP quality assessment are detailed in Supplementary Table 3. Approximately 22% of studies fulfilled all criteria and about 75% of studies fulfilled most criteria. Question 6 of the CASP checklist “Has the relationship between researcher and participants been adequately considered?” was the most poorly reported criterion (32% of studies), followed by Question 7 “Have ethical issues been taken into consideration?” (61% of studies).
Themes of QOL impacts on informal carers
Based on the a priori framework and the secondary thematic analysis, the final synthesis revealed five major themes: coping (emotional coping and problem coping), relationship with the person with dementia (sense of loss and change in relationship), interference with life (control over caring situation, and freedom and independence), support (formal support and informal support), and health (physical health, emotional and mental health, and social health). Figure 2 depicts the conceptual model of the five themes. Reference was made to the conceptual model, where appropriate, to highlight relationships between themes and conceptual overlap. Table 2 provides an overview of the QoL domains of informal carers impacted by their caring role.
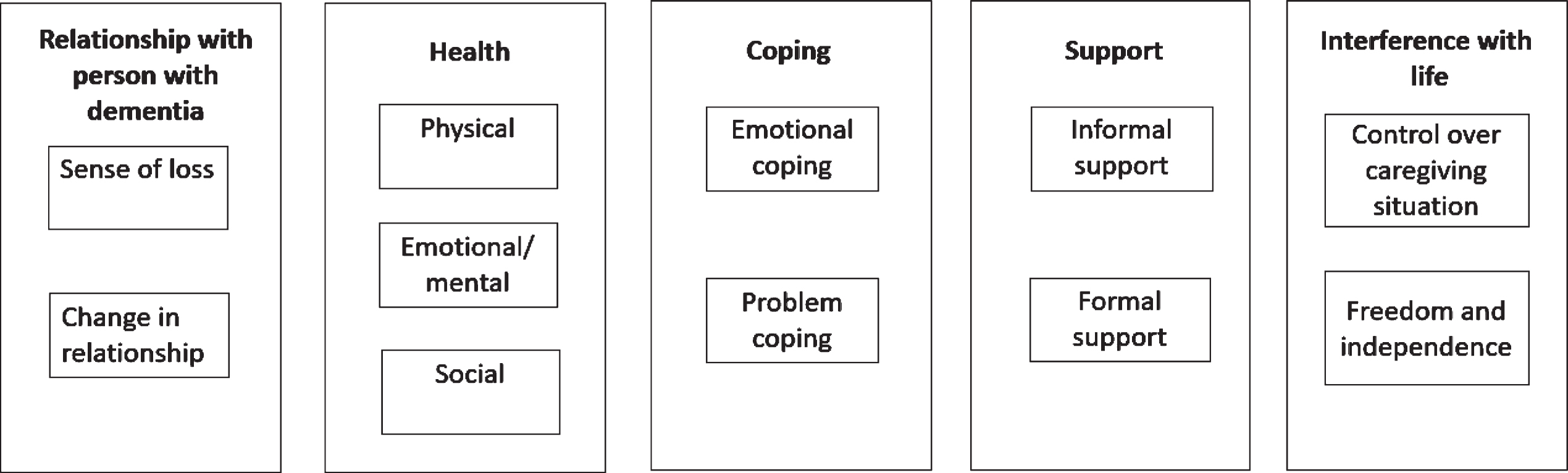
Conceptual model of factors that impact QoL of informal carers of people with dementia.
QoL domains of informal carers impacted by their caring role
Coping
This theme is based on the Coping Circumplex Model, which identifies how coping impacts people’s health and performance [86]. Two descriptive themes were identified in this study: emotion coping and problem coping. Emotion coping is described as positive and negative emotion coping, and problem coping is described as problem solving and problem avoidance approaches [86]. In line with the association between emotional coping and problem coping illustrated in Fig. 2, positive emotional coping mechanisms can overlap with problem-solving approaches, as emotional regulation and positive reappraisal of a situation can be seen as a form of problem-solving.
Emotion coping
Emotion coping describes the capacity and approaches utilized by informal carers to regulate positive and negative emotional responses to potentially stressful situations in caring [86]. Positive emotional coping refers to approaches taken by informal carers to enable positive reappraisal of their situation, regulation of emotions and acceptance of their situation [86]. Positive emotion coping was positively associated with improved QoL. Several papers reported that participants utilized positive emotional coping strategies such as self-compassion, humor, hobbies, reliance on faith and preserving normalcy to regulate their emotions, reframe situations positively, and facilitate resilience in situations that can cause informal carers’ distress [30, 73]. Informal carers mentioned that having a sense of humor has been a helpful approach in maintaining positive emotional health and wellbeing when confronted with stressful situations and adjusting to changes in the person with dementia [30, 52]. Faith has been expressed as a source of inner strength and to a lesser extent, a method to give carers perspective of realities in caring and the practice of gratitude for their situation not being worse [62, 73].
Positive reappraisal refers to viewing positive aspects of caring such as providing carers with a sense of purpose, an identity, and their achievements from their caring role and demonstrating their capability in supporting a person with dementia [40, 70]. For example, one study reported a carer who felt responsible to serve as a role model to their children after taking on the role of a carer for a person with dementia [50]. A few factors that facilitated carer resilience included accepting current caring situation and changes in the person with dementia and their lifestyle and directing their focus on fulfilling daily caring duties instead of ruminating on the past and future concerns [34, 57]. Carers’ acceptance of their role was associated with carers feeling a sense of responsibility towards their care recipient, finding meaning in supporting a person with dementia and associating their caring role with their own identity [55, 64]. A few studies reported that adult child carers who define caring as a means of “giving back” to their parent with dementia for their previous care and felt a sense of “satisfaction” from “giving back” [55, 61]. From a family perspective, maintaining shared family values and memories of helping each other evoke a sense of togetherness and normalcy, which can be interpreted as a form of positive emotion coping for both carer and the person with dementia [54]. Emphasis on positive thoughts about caring in recognizing joyful and positive experiences in caring was associated with building strength [55]. In terms of coping for the future, some carers expressed a sense of hopefulness that Alzheimer’s disease medication can delay or prevent disease progression [73]. Self-compassion was mentioned in only one study, where a carer felt like their mistakes should be met with self-forgiveness [45]. The practice of emotion coping such as feeling fulfilled through caring and ascribing meaning to caring role is positively associated with the subtheme ‘control over caring situation’, which refers to carers’ capacity to manage their situation (ref Fig. 2).
Negative emotional coping describes a person’s focus on negative aspects of a situation, negative emotional responses (e.g. anger, resentment) and venting of emotions and denial of caring situation, existence of dementia and limited caring capacities [86]. Denial of stressful situation or predicament can negatively affect emotional and mental wellbeing of carer [86]. Negative emotion coping is associated with poorer QoL, poorer emotional and mental health, and problem avoidance.
Problem-coping
Problem coping is an approach that employs either a problem-solving approach or a problem-avoidance approach. Problem-solving involves finding the capacity to manage a stressful situation and strategically plan solutions to resolve the issue and action their plans [86]. Problem avoidance refers to carers using denial as a coping mechanism to disengage from the reality of their situation and presentations of dementia in person with dementia [86].
From the perspective of problem avoidance, carers in denial of their limited capacity to manage their caring situation could potentially contribute to poorer QoL [32, 58]. A few papers described carers in denial of visible signs of dementia in people with dementia and deterioration in their cognitive function, which may reflect lack of resilience in carers [45, 65]. One study reported self-medication with alcohol as a coping mechanism to manage carer stress [43]. Problem avoidance can be deemed as a form of disengagement from reality as demonstrated by carers in denial or self-medicating. This denial of emotional stress in problem coping is also reflective of negative emotional coping (ref Fig. 2).
From the perspective of problem coping, adaptability to changes in the caring situation and care-recipient’s behavior served as a measure to cope with life changes [44, 60]. Carers also used critical thinking, strategic planning, and knowledge application to meet care-recipients’ needs. Examples of employing problem-solving skills among carers to strengthen patience included seeking to understand dementia and issues related to caring, recognizing carer’s own capacities and need for additional support [48, 75]. Problem-solving approaches for carers overlap with ‘positive emotion coping’ and ‘social health’ (ref Fig. 2). This overlap is seen in the context of carers utilizing hobbies and socializing as a distraction that can assist a carer in reducing the likelihood of being depressed or lonely and help reduce carer stress [43, 80].
Relationship with person with dementia
The analytical theme relationship with person with dementia describes the negative and positive impacts of caring on carer’s relationship with the care-recipient and its impact on carers’ QoL. Two descriptive themes were identified: (a) sense of loss, and (b) change in relationship. Sense of loss in a relationship with the care-recipient has been conceptualized as loss of communication, connection or reciprocity of affections, intimacy (for partners) and loss of goals for the future with disease progression in people with dementia [57, 77]. The descriptive theme ‘change in relationship’ describes how positive and negative changes in relationship dynamics between carer and care-recipient can impact carers’ QoL.
Sense of loss
Sense of loss from the perspectives of partner carers and adult child carers posed a significant negative impact on carers’ QoL [55, 57]. Carers’ feelings of sense of loss in communication, loss or drastic change of care-recipient’s personality, and sacrifices made by the carer (e.g., retiring from work) was conceived as a sign of grief [53, 79]. A common re-occurring concept with loss was the feeling of an “absent-presence” relationship with care-recipients and the disappearance of a loved one with the progression of dementia [28, 77]. Across studies, many carers felt a sense of isolation, loneliness, sadness, abandonment, unfairness, and anger with the loss of their previous relationship with their care-recipient [44, 78]. For adult children, loss of previous relationship with a care-recipient was described as the loss of a parental figure [55]. Sense of loss was also seen in the loss of joint activities between a couple as the carer was not able to enjoy the care-recipient’s company due to loss of the care-recipient’s ability to communicate [58].
Among partner carers, sense of loss was described as a loss of intimacy and connection, referring to the loss of physical touch or desire for physical touch [34, 39]. A few studies reported carers feeling distant from the person with dementia, which was largely associated with discomfort or desensitization towards the person with dementia in a sexual manner or loss of connectedness with progression of disease and burden of carers’ duties [34, 39]. One study reported that partner carers with low sexual desire for the care-recipient was due to the fatigue of performing caring duties [39]. In comparison, other studies mentioned lack of initiation or interest in sex from the care-recipient contributed to loss of intimacy, feelings of insecurity and rejection [39, 77]. Another study mentioned that despite a carer longing for sexual intimacy with their partner, they managed to retain value in other aspects of their relationship [77].
Change in relationship
Change in relationship mainly describes the impact of changes in person with dementia on relationship dynamics and perception of informal carers towards their care-recipient [59, 66]. A small number of studies reported positive aspects of caring on relationship with people with dementia such as improved communication, emotional closeness, companionship, and even deepened feelings of love for the person with dementia contributing to improved QoL [35, 65]. Studies also reported patience and acceptance of changes in relationship and reframing caring as a source of personal development and inner strength as qualities that fostered carer resilience [52, 61]. This overlap in acceptance of situation and approaching caring situation with patience is also seen in ‘positive emotional coping’ and ‘control over caring situation’ (ref Fig. 2). An example of fostering carer resilience was seen among adult child carers who made sense of their caring situation by accepting role reversal and positively framed role reversal as a tool to manage the person with dementia and viewed caring as a strength [33, 78]. In comparison, other studies on adult child carers reported role reversal as challenging and “emotionally traumatic” due to feelings of a sense of loss of their parent-child relationship [66, 78].
Most carers regarded care-recipient’s increased dependency and behavioral changes as difficult to accept and manage. Changes in relationship due to progression of dementia, loss in cognitive function and communication skills and behavioral changes in care-recipient were likely to negatively impact emotional health and QoL by invoking a ‘sense of loss’ and ‘emotional pain’ from the loss (ref Fig. 2) [59, 66]. One study reported that progression of dementia created distance between adult child carers and care-recipients as they could not recognize each other as parent and child [78]. Some studies reported poorer QoL among carers due to overwhelming demands, such as managing care-recipient’s aggression, irritation, and sometimes physical abuse [36, 76]. Care-recipient’s irritability created tensions in the carer-care-recipient relationship and led one carer to feel hatred towards the care-recipient [59].
Interference with life
Interference with life describes QoL impacts under two descriptive themes: (a) control over caring situation and (b) freedom and independence.
Control over caring situation
This subtheme describes the decision-making processes of carers for person with dementia, carers’ daily roles and responsibilities and the impact of these responsibilities on carers’ QoL. Carers reported that they assumed a more authoritative role in decision-making, advocating for the person with dementia and taking over the responsibilities of meeting care-recipient’s needs [27, 66]. As a consequence of assuming decision-making roles for care-recipients, studies reported some carers felt traumatized and overwhelmed from the experience [34, 83]. Carers recognized increasing dependency of care-recipients in terms of daily tasks such as bathing, grooming, dressing, cooking, providing medication, and cleaning [41, 66].
Poorer QoL was associated with experiences of hardships in managing daily uncertainty and struggles in adjusting to their carer roles and responsibilities [78, 80]. In assuming caring responsibilities, a carer expressed experiencing undesirable changes in their sense of self including forced aging [34]. Another study reported a carer harboring resentment towards their caring role [41]. The level of difficulty experienced in fulfilling daily caring is dependent not only on the carer’s capability, but also the care-recipient’s willingness to be supported. One study reported that carers struggled with daily caring, where a carer accidentally bruised the care-recipient when bathing as they were not being cooperative causing the carer to feel a sense of shame [43]. Studies reported that carer’s struggle in accepting their new caring role stemmed from difficulty in accepting changes in the person with dementia and/or from the time-consuming tasks involved in daily caring [52, 80]. External challenges that contribute to carer strain include managing multiple responsibilities such as work and childcare, in addition to caring [49, 55]. Financial hardship was also recognized as a contributing factor to carer struggle and was linked to care-recipient’s uninhibited spending, change in flow of their finances, where carers were now solo financial managers, and lacked access to government financial support [36, 83]. Carers with limited knowledge and awareness of information and resources were less prepared for their caring role, with lesser understanding of dementia, and less support for coping with their caring situation [72, 81]. One study described the impact of carers’ lack of preparedness for care-recipients’ arrangements for dying and death causing some carers to feel regret about delaying discussing this aspect with the person with dementia while they were still cognizant [78].
Carers with a sense of preparedness, dedication to honing their caring skillset, and building their knowledge were seen as central components to accepting the caring role, which contributed to carer’s confidence, resilience, and improved QoL [38, 52]. Components that facilitate resilience are reflective of ‘positive emotion coping’ and ‘problem solving’. Maintaining normality within carer and care-recipient relationship was also seen as being positively associated with ‘having control over caring situation’ (ref Fig. 2). For example, to retain care-recipient’s agency, one carer would include the care-recipient’s opinion in decision-making like choosing clothing [57]. Carers also mentioned their previous work experience in the healthcare sector, which gave them a sense of preparedness in managing practical challenges, such as administration of medication or flexibility when posed with unexpected situations in caring [68, 81]. Other facilitators of control over caring included positive framing of their situation, having a scheduled daily routine, continual switching of responses (dependent on the care-recipient’s mood and behavior) and having the financial means to maintain lifestyle [42, 80]. Some carers utilized positive reappraisal as seen in positive emotion coping, where they associated caring with a sense of achievement, fulfilment or as a form of personal development from caring [50, 70].
Freedom and independence
This subtheme explores the impact of caring on carers’ freedom and independence. Studies reported that carers stressed that freedom and independence, such as having a sense of identity beyond caring, time for self-care, work and time for social engagement was associated with improved QoL, while loss of freedom and independence was negatively associated with those aspects [56, 78]. Engaging in self-care was associated with maintaining physical and mental wellbeing and to fulfill the caring role [33, 83]. Self-care is closely linked to positive impact in all aspects of health (Fig. 2).
Most studies reported that carers experienced a loss of freedom and independence due to caring responsibilities and reported feeling trapped, loss of personal time, and experience of self-neglect [56, 64]. Carer sacrifices include giving up their paid employment, education, and missing social events due to caring [38, 84]. Studies also reported that carers were unable to do things without planning ahead (i.e., lack of spontaneity) but in certain instances, even planning ahead did not have the expected outcome [56, 64]. Lack of freedom and independence to participate in social gatherings resulted in relationship strain with family members and negative impact on emotional well-being stemming from social isolation and exhaustion from caring [56, 79]. Loss of self-identity was associated with carer’s self-identity being subsumed by their caring role and inability to switch off from their role due to care-recipient’s need for constant supervision [30, 55]. Loss of freedom and independence was associated with frustration, exhaustion and isolation associated with emotional and mental health, and social health (Fig. 2) [38, 49].
Support
The analytical theme, support, explored the impact of met and unmet needs of carers under two descriptive themes: (a) formal support and (b) informal support. Formal support services discussed in studies include respite care, home care, legal support, financial support, support groups for informal carers, healthcare, and other resources [48, 83]. Informal support refers to support for informal carers usually provided by partners, family, friends, neighbors, or members of religious congregations [65, 66]. Informal support was typically in the form of practical support like contributions to caring duties and advice, social support, or emotional support for carers [42, 83]. Support received by carers can hinder or facilitate freedom and independence and control over caring situation (ref Fig. 2). Adequate support can enable carers’ time for oneself to rest, socialize and engage in leisurely activities, in turn improve their QoL and make their caring responsibilities manageable. Inadequate support, both formal and informal, can contribute to carer burden and stress, negatively affecting carer’s QoL. Uptake of formal and informal support, perception of support and level of satisfaction with support were largely dependent on carers’ perceived needs, care-recipient’s perceived needs and experiences with formal and informal support [42, 79].
Formal support
A few studies reported informal carers experienced improved QoL after seeking formal support, but most informal carers reported having unmet needs.
At the healthcare level, healthcare professionals who exhibited poor knowledge and awareness of dementia and carer’s needs—learning resources or support groups for informal carers—contributed to carers’ isolation, feelings of disappointment, and poorer QoL [27, 83]. Similarly, some studies reported carers’ experiences of feeling unseen or unheard by healthcare professionals who did not acknowledge carers’ potential health needs and only focused on the care-recipient’s condition or disrespected carer’s opinions [27, 81]. Carer stress was exacerbated by inconsistent information delivered by healthcare professional [48].
At the professional support services level, a few studies reported carers’ reluctance in using respite care due to their commitment to care-recipient, or respecting care-recipient’s wants [79]. A few carers developed mistrust and lack of confidence in quality of residential care and respite care services due to their personal experiences of poor treatment by staff and tardiness [61, 65]. In terms of family dynamics, disapproval or stigma from family members of carers seeking additional support from professional support services served as an obstacle for the carer to overcome [31, 72]. Lack of flexibility and continuity with formal support was associated with negative perception of care and emotions like anger and lack of freedom and independence to participate in social activities [57]. Positive perception towards professional support was associated with the informal carer feeling heard by formal carers or flexibility to changing needs and schedules and a sense of “continuity” when establishing or having established a relationship between formal carer, informal carer and care-recipient [29, 57].
At the level of support groups, carers had an unmet need for targeted support that address specific groups like young carers [29, 52]. Some studies reported support groups as a helpful form of social support for carers to relieve stress and as a medium to foster inner strength [34, 74]. On the other hand, one study reported that carers felt that time spent attending support groups was not useful [74]. For some carers, a support group was a source for learning about caring and dementia [66, 72]. Knowledge-seeking behavior in understanding dementia was a contributing factor in facilitating carer’s resilience [59].
Navigating unfamiliar areas like legal support or financial support has been a struggle for informal carers, in addition to time-consuming nature of caring [64, 74]. Additionally, the complexity of administrative processes in formal support services and long processing times contributed to carer frustration [29].
Informal support
This subtheme explores the perception of informal support, types of informal support, and impact of informal support and its absence. Most informal carers reacted positively to informal support from family, partners, friends, and, to a lesser extent, neighbors, community members, and religious groups. Informal support enabled informal carers time for self and work, and a source to enable caring [66, 67]. The concept of time for oneself and work ties into ‘freedom and independence’ (ref Fig. 2). A few studies found carers who rejected informal support did so due to personal wishes to maintain their and the care-recipient’s privacy [63, 77]. However, this can result in isolation for some carers [77]. Other studies found carers felt like they did not want to impede on their family member’s lives so they did not seek informal support [73, 77].
Most informal carers who received little to no informal support expressed need for further support in the form of practical support, like assisting with caring duties and emotional support [64, 78]. One study identified gender constructs as justification for women to fulfill caring roles but this standard was not expected for male family members [67]. Lack of emotional support was described as lack of appreciation from others for caring [78]. Other carers expressed a sense of isolation due to other people’s lack of familiarity with dementia and carers being unable to separate themselves from their caring role and making comparisons of their situation with the situation of others [27]. One study identified lack of visitation from local religious groups with lack of informal support and feeling dispirited [83]. Social stigmatization towards dementia served as a barrier to seeking informal support [52]. A few studies mentioned that the caring role created family tensions due to the time-consuming nature of caring and dissatisfaction with sharing caring duties [30, 81].
Informal carers who lacked support were more likely to experience negative emotions like disappointment, resentment towards family members, and frustration [64, 70]. Experience of negative emotions greatly impacted carers’ emotional and mental health, and social isolation contributes to poorer social health (ref Fig. 2).
Health
Under the analytical theme ’health’, three descriptive themes have been identified: (a) Physical health; (b) Social health; and (c) Emotional/mental health.
Physical health
In terms of valuing physical health, several studies reported carers acknowledging the physical burden of caring on health, with only a few carers having the capacity to maintain their health to manage their caring duties [sub theme – control over caring situation] (see Fig. 2) [68, 79]. Lack of time for rest or self-care due to caring and caring stress has led to health deterioration, poorer ageing, tiredness, physical drain, weight loss, lack of sleep, and even slow recovery from illness [27, 64]. Carers with pre-existing chronic illness reported that their condition had worsened after becoming a carer [56, 83].
Social health
This theme describes the shortfall of social connections due to caring and the impact of caring on carers’ social health and QoL. Social aspects described in this study include carers’ ability to sustain and develop social connections, as well as impact of care-recipient’s condition and caring on carers’ relationships with friends, family members, members of organized religion, and neighbors [36, 56].
Carers positively associated improved wellbeing through having time separate from caring and socializing with friends, family, members of organized religion, and online communities [44, 84]. A few studies highlighted the importance of planning and scheduling social activities with friends and family outside of caring to enable carer time to de-stress [44, 80]. Another study emphasized a feeling of anticipation with carer receiving regular social engagement outside of caring [40].
Factors associated with poorer QoL in informal carers include carers’ feeling a sense of loneliness and isolation due to lack of companionship, lack of capacity to socialize, people distancing themselves from carer, people’s unfamiliarity with caring and dementia, or feeling misplaced in social activities due to a struggle in separating themselves from their caring role [30, 80]. Feelings of loneliness and isolation can be linked to not only poorer social health but also poorer emotional and mental health and wellbeing (ref Fig. 2). Lack of familiarity or understanding of full scope of dementia and its presentation has been a contributing factor to carer stress. In terms of partner relationships, some adult child carers have attributed relationship tensions and failed relationships to carers prioritizing the care-recipient over their own partner [84]. A few carers highlighted the difficulty in fostering new partner relationships due to ambiguity of relationship with care-recipient or consuming nature of caring [69, 77]. Some studies reported that carers experienced tensions in family relationships when discussing care of the person with dementia, which contributed to carer stress [47]. Another study outlined family tensions were due to carers prioritizing care-recipient over another family member [47].
Emotional and mental health
This subtheme describes the key emotions that influence carers’ QoL. Several studies identified the negative impact of caring on their emotional wellbeing and exacerbation of pre-existing mental health conditions in some carers [56, 68]. Receiving adequate practical, social and emotional support, freedom and time for oneself, and utilization of positive emotion coping strategies was associated with positive emotions. Positive emotions are reported as feeling glad from engaging in self-care and finding happiness from providing support to care-recipient [38, 85].
A diverse range of negative emotions were identified, with the most common emotions being anger, frustration, guilt, worry, anxiety, depression and lesser common emotions of sadness, sense of hopelessness, distress, emotional drain, and ambivalence [50, 78]. Carers’ guilt stemmed from their own perception of failing to fulfill care-recipients’ needs, not being able to regulate their negative emotions and lashing out at care-recipient, having separation from their role as carer to work or engage in other activities, and in an adult child carer, sharing their caring obligations with a partner [34, 78]. One study reported a carer who associated time away from caring with guilt due to feeling like they were not fulfilling their caring responsibilities [57]. Anger, frustration, and deterioration was associated with the stress of caring and lack of recognition by other people for their caring efforts [57, 83]. Studies reported that carers permitted themselves to get angry with their care-recipient since they would “forget” due to the deterioration of their memory [50]. Some studies reported carers resorted to physical and verbal abuse out of anger, tiredness, and stress [82]. Self-criticism is seen as a by-product of negative emotion coping from ruminating over past mistakes and negative emotions like guilt [34].
The time-consuming nature of caring and lack of time to seek professional mental health support led to emotional drain [79]. One study reported that carers experienced a sense of hopelessness from struggling to accept alterations to their lives [46]. Ambivalence was expressed across a few studies. Carers found themselves oscillating between different emotions and responses towards the person with dementia and caring complexities [76, 81]. Examples of ambivalence have been described as carers feeling anger towards person with dementia and feeling a sense of closeness to them or feeling anger to indifference towards caring [76, 81]. Carers’ projections about the future—carers’ and care-recipient’s health and wellbeing and ability to manage caring responsibilities with the progression of dementia—were often associated with worry and anxiety [49, 57]. Some carers reported that their caring experiences led to suicidal ideation and homicidal thoughts of care-recipient as a means to end their caring role [37, 82]. Carers who ruminated over homicidal thoughts towards care-recipient expressed either relief or framed death of care-recipient through euthanasia as an act of sympathy towards person with dementia due to their perceived poorer QoL [82].
An interrelationship between emotional/mental health and emotional coping, in the form of positive or negative emotions, was found during our analysis, which in turn is linked to greater control over the caring situation (ref Fig. 2).
DISCUSSION
Our review details the experiences of informal carers and provides a better understanding of factors that can impact carer QoL that include: coping mechanisms (emotion coping and problem coping), relationship with person with dementia (sense of loss, and change in relationship), support (formal support and informal support), health (physical health, emotional and mental health, and social health), and interference with life (control over caring situation, and freedom and independence). Most studies discussed emotional and mental health impacts, control over caring situation, and freedom and independence. Physical health and problem coping were mentioned in less than a quarter of the included studies. There were also very few studies that mentioned the impact of caring on finances and changes in financial flows on carers’ QoL [36, 83]. This may be due to lack of prompting participants during interviews or focus group discussions on topics pertaining to physical health, finances, and problem coping. Otherwise, these findings indicate that there is heterogeneity in carer experiences and aspects of informal carers’ QoL across different studies and within studies.
Our findings detail how experiences of informal carers can impact carer wellbeing and QoL. This conceptual model can be used to identify unique aspects that can contribute to improved or poorer QoL among informal carers of people with dementia. The demands of caring and extent of caring burden can have negative consequences on different QoL domains. Our conceptual model can be seen as an extension of two previous systematic reviews on informal caring [11, 17]. Farina and colleagues identified key aspects that impact carer QoL (“carer health”, “carer independence”, “support received”, and “self-efficacy”) reflected in our conceptual model [17]. However, they only identified three qualitive studies out of 51 studies, missing the broader scope of influential factors on carer QoL [17]. Similar to our review, Lindeza and colleagues identified positive and negative aspects of the caring role in their systematic review but did not highlight the interrelationships of contributing factors to carer QoL [11]. Our coding framework is consistent with carer-QoL instruments (ASCOT-Carer, CES and CarerQol) and one dementia-specific measure (CGQoL) [14, 17]. Using an inductive analysis, we identified additional QoL domains such as sense of loss, coping, and emotional and mental health. Only the CarerQol currently includes one domain around mental health, yet the theme ‘emotional and mental health’ in our review is much broader and includes also positive emotions in providing informal care. Sense of loss in a relationship with person with dementia expands the “relational problems” domain in CarerQol and “getting on with the care recipient” domain in CES by addressing carer’s sense of connection and intimacy towards person with dementia [14]. Coping contributed to the “control over caring” domain in CES, “control over daily life” domain in ASCOT-Carer and “problems with daily activities” in CarerQoL by highlighting positive and negative coping mechanisms [14]. In contrast to our review, CGQoL focused on family support, spirituality and faith, while we conceptualized faith under coping mechanisms and family interactions as informal support that extends to friends, partners, neighbors and religious communities [16]. Thus, our conceptual model can potentially be used to evaluate the suitability of QoL domains in dementia-specific instruments in the future. Our conceptual model also highlights the gaps in QoL domains of carer-QoL instruments and demonstrates the importance of utilizing qualitative data collection methods when developing new measures.
A diverse range of positive and negative coping mechanisms were identified as contributing factors of carer QoL. Denial of limited caring capability are seen in problem avoidance and focus on negative aspects of caring seen in negative emotion coping mechanisms tended to lead to poorer emotional and mental health [86]. Positive emotion coping mechanisms and problem-solving skills fostered caring resilience. Knowledge, experience, and skills in caring used for problem-solving and regulation of emotions in positive emotion coping enabled control over caring situation, carer resilience and improved QoL [38, 73]. Carers who utilized previous work experience to resolve issues in caring, recognized the need for additional support and focused on positive aspects of caring. The use of skills and experience of caring over time enabled carer resilience, acceptance of caring situation and control over caring situation, ultimately improving carer QoL [50, 86].
High caring demands and stress often pose a risk of poorer physical, emotional, mental, and social health [27, 56]. Impact of carer QoL can differ depending on presence of pre-existing health conditions but negative impact of caring on health is largely due to physical demands of caring, time dedicated to caring, limiting opportunity to participate in social activities that lead to social isolation and time for self-care [56]. Carers often experienced poorer emotional and mental health from sense of loss and changes in relationship with person with dementia. Negative emotions ranged from anger, loneliness, and sadness to more extreme emotions related to suicide and homicidal thoughts towards person with dementia [68, 82]. These findings are supported by the “Dementia Grief Model” detailing grief as a process of carers adapting to life changes and fostering carer resilience through understanding and accepting caring situation and difficult emotions when faced with a sense of loss [87]. Few studies identified carers who focused on positive aspects of caring such as improved relationship dynamic in a carer-care-recipient relationship influencing carer resilience [35, 38].
Many studies reported caring as sacrificing personal time with constant supervision of care-recipient and difficulty in separating from the caring role. Freedom and independence were seen as self-care, having time for personal activities and work, and were associated with improved QoL [44]. Meaning of carer’s self-identity varied between having identity synonymous with carer role to having freedom, independence and having time apart from caring role to maintain sense of self-identity [55]. Informal support (e.g., family friends, religious groups, and neighbors) was reported as an enabling factor for freedom and independence when support met carer’s and care-recipient’s needs, and reduced carer burden. Informal support was often deemed as unsatisfactory for reducing carer burden and was often limited [27, 29]. Carers who did not receive the desired level of support experienced poorer emotional and mental health expressed as negative emotions such as anger and disappointment [35, 64].
Poor quality of healthcare delivery and lack of social and emotional support from informal networks often led to carer isolation and stress [27, 29]. Some studies reported healthcare staff being unaware of resources for dementia or delayed diagnosis of dementia, causing carers to feel alone [27, 82]. Access to quality formal support (e.g., healthcare and support groups) enabled access to learning resources and a sense of unity among informal carers in a support group [66, 72]. Carers also reported lack of social and emotional support from informal support networks (e.g., friends, family, neighbors, and religious groups) as contributing factors to carer isolation and negatively affected carer’s emotional and mental health [27]. However, sense of loneliness among carers varied, with a few carers feeling content with lack of socialization [77]. Some studies reported that some friends and family distancing themselves from the carer and the person with dementia after diagnosis. Need for improved formal support for informal carers is recognized in Lindeza and colleagues’ review [11].
Informal caring remains a largely negative experience with limited support addressing carers’ needs. With increasing prevalence of dementia, this reflects an increasing need to address both carer and care-recipient’s needs to enable caring [11]. Overall, findings from this review present as a basis for identifying carer QoL domains in future studies related to experiences of carers of people with dementia and can potentially inform strategies related to informal carers.
Strengths and limitations
While we have identified new domains in the conceptual model, we acknowledge that the conceptual model may be incomplete, as our review may not have captured all studies on informal carers’ lived experiences due to the limitation on number of searched databases, exclusion of developing countries and other exclusion criteria applied. Reinterpretation of participants’ experiences and original author’s interpretation of participants’ experiences can pose another limitation. However, the conceptual model can serve as a basis for comparing different domains that impact QoL of informal carers and identify gaps in generic instruments for informal carers’ QoL. Variation in dementia-related policies at a state-, territorial-, regional-, and federal-level can have different implications on carers’ QoL. Thus, our findings may not be generalizable to all developed countries. Generalizability of our findings is further compromised by characteristics of study participants included in the studies, which may underrepresent the hard-to-reach group of informal carers. In this context, future studies should consider alternative approaches for data collection, such as participatory health research [88] and further qualitative research is required. There was also insufficient evidence to compare culture, age, and length of time in caring as potential underlying factors given that only a few studies explicitly highlighted any differences. We were also unable to compare carer experience by dementia subtypes, time of disease and severity stage due to insufficient details in the studies reviewed. In addition, restriction of this review to developed countries may not capture the full scope of carers’ experiences and factors that impact carer QoL outside of the developed country context.
Nevertheless, our review has numerous strengths, with respect to previous systematic reviews [11, 17]. This review is a comprehensive and up-to-date review of the literature, which includes recent studies focusing on the experiences of carers of people with dementia and QoL impacts on carers of people with dementia. We have also developed an innovative conceptual model, introducing new themes, expanding initial QoL domains based on three carer-related preference-based measures (ASCOT-Carer, CES, and CarerQol) used to base our a priori framework.
Conclusions
This review has identified key aspects that impact the QoL of informal carers’ of people with dementia: coping (emotion-coping and problem-coping), relationship with the person with dementia (sense of loss and change in relationship), support (formal support and informal support), and interference with life (control over caring situation and freedom and independence) and health (physical health, emotional and mental health, and social health). Our conceptual framework can be used to guide service provision, addressing areas of QoL most important to informal carers of people with dementia. It can also be used to validate and develop QoL instruments, with findings indicating a need for a more comprehensive QoL instrument which identifies QoL domains pertaining to informal carers of people with dementia.
Footnotes
ACKNOWLEDGMENTS
The authors would like to extend their gratitude towards Dementia Australia Research Foundation for funding this project. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the findings; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.