
Abstract
Background:
Although thyroid dysfunction has been considered as a cause of reversible cognitive impairment, association between subclinical hypothyroidism and cognitive impairment is controversial.
Objective:
We compared cognitive profiles of patients in an euthyroid or subclinical hypothyroid (sHypo) state, as well as their disease progression from mild cognitive impairment (MCI) to dementia within 3 years.
Methods:
We included 2,181 patients in a euthyroid and 284 in a sHypo state over 60 years of age who underwent an extensive cognitive assessment at Seoul National University Bundang Hospital but were not prescribed levothyroxine, methimazole, carbimazole, or propylthiouracil. After propensity score matching for age, sex, and education level, 1,118 patients in a euthyroid and 283 patients in a sHypo state were included. Attention, language, memory, visuocontructive, and executive functions were compared between the groups using Student’s t-test or the Mann-Whitney U test. To investigate the association between disease progression and subclinical hypothyroidism, a Cox regression analyses was performed in 379 patients with MCI. Patients with thyroid-stimulating hormone levels over 10 mlU/L was classified as the “sHypo10”, and hazard ratios for sHypo or sHypo10 were assessed.
Results:
There was no difference in attention, language, memory, visuoconstructive, and executive functions between the patient groups. Progression from MCI to dementia was not associated with sHypo or sHypo10.
Conclusion:
There was no difference in cognitive profile between euthyroid and sHypo patients, and no association between subclinical hypothyroidism and disease progression. This might suggest a clue of strategies regarding hormone therapy in subclinical hypothyroidism with cognitive impairment.
INTRODUCTION
Subclinical hypothyroidism is the state of elevated levels of serum thyroid-stimulating hormone (TSH) but normal levels of serum free thyroid hormones [1]. The prevalence of subclinical hypothyroidism ranges from 2 to 15% depending on age, sex, race, and region [1, 2]. Elderly populations tend to be more frequently diagnosed with subclinical hypothyroidism due to an increase in concentrations of TSH with age [3]. The treatment of subclinical hypothyroidism depends on several factors, such as TSH levels, comorbidities, and age [4]. TSH levels between 4.5 and 10 mlU/L are classified as subclinical hypothyroidism grade 1 and TSH levels over 10 mlU/L as grade 2; grade 2 is one of the criteria for hormone treatment and related to an increased risk of other diseases such as heart failure [4, 5].
The association between subclinical hypothyroidism and cognition is controversial. Although thyroid dysfunction has been considered as a cause of reversible cognitive impairment [6]. Numerous studies on the effect of subclinical hypothyroidism on cognition have shown inconsistent results. A recent meta-analysis reported that subclinical hypothyroidism is not associated with cognitive function or cognitive decline [7], which raises questions for clinicians concerning the treatment of subclinical hypothyroidism with cognitive impairment.
In this observational study, we used propensity score matching to minimize selection bias, and then compared the results of an extensive cognitive performance assessment between patients in a euthyroid and those in a subclinical hypothyroid (sHypo) state. We also compared their clinical progression from mild cognitive impairment (MCI) to dementia within 3 years. Additionally, clinical progression was evaluated in a subgroup with subclinical hypothyroidism with TSH levels over 10 mlU/L (subclinical hypothyroidism grade 2).
METHODS
Study population
This retrospective longitudinal observational study was conducted at Seoul National University Bundang Hospital from January 2013 to January 2021. We included patients who were over 60 years old and underwent an extensive baseline cognitive assessment and a baseline thyroid function test. Of all patients assessed during this time, those in a euthyroid or sHypo state were included. Subjects who were prescribed thyroid hormone-related medication including levothyroxine, methimazole, carbimazole, and propylthiouracil were excluded.
This study design was approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB number: B-2103-670-101).
Thyroid function
Thyroid function was assessed by measuring concentrations of free thyroxine (FT4) and TSH. A euthyroid state was defined as a serum TSH level of 0.45–4.5 mlU/L and a FT4 concentration of 0.8–1.8 ng/dL. A sHypo state was defined as a serum TSH level of 4.5–20 mlU/L or greater and a normal FT4 concentration of 0.8–1.8 ng/dL [8]. A TSH level of 10 mlU/L or higher was defined as a sHypo10 state [4].
Cognitive function
We assessed the global cognitive status with the Mini-Mental State Examination (MMSE) [9], dementia severity with the Clinical Dementia Rating Sum of Boxes (CDR SOB) [10], and depressive symptoms with the short form of the Geriatric Depression Scale (GDpS) [11]. Additionally, extensive neuropsychological assessments were performed to evaluate attention, language, verbal and visual memory, visuoconstructive, and frontal executive function. We used the Digit Span Test for attention [12], the Korean version of the Boston Naming Test for language [13], the Seoul Verbal Learning Test for verbal memory [14], the Rey Complex Figure Test (RCFT) for visuoconstructive function [15], the categorical and phonemic fluency test of the Controlled Oral Word Association Test and the Stroop color reading test for executive function [16, 17]. For the statistical analysis, MMSE, CDR, CDR SOB, and GDpS scores were used as raw scores. The scores for specified neuropsychological tests were converted to standardized scores (z-scores), which were adjusted for age, sex, and education level.
Statistical analysis
To minimize differences in baseline characteristics between the euthyroid and the sHypo group, a propensity score matching analysis was conducted. Propensity scores were calculated through logistic regression with covariates such as age, sex, and education level using the Matchit package in R. Patients were paired in a ratio of 1 (sHypo):4 (euthyroid) based on these propensity scores with a caliper size of 0.2.
Demographics between groups of unmatched and matched patients were compared with Student’s t-test, the Mann-Whitney U test, or a Chi-squared test as appropriate. Cognitive assessment results at baseline between groups of matched patients were compared using Student’s t-test or the Mann-Whitney U test.
A multivariate Cox regression analysis was performed to investigate the determinants of cognitive decline from MCI to dementia. MCI was defined as a CDR score of 0.5, and dementia was defined as a CDR score of 1 or more. Of the entire matched cohort, 1,127 patients were classified as having MCI, of which 748 were not available for follow-up cognitive assessments. Consequently, 379 patients with MCI were included in the Cox regression analysis. We assessed hazard ratios (HR) using two models: model 1, with sHypo, age, sex, baseline MMSE scores, education level, and APOE ɛ4 carrier status as covariates, and model 2, with sHypo10, age, sex, baseline MMSE scores, education level and APOE ɛ4 carrier status as covariates. Models 1 and 2 were also analyzed without APOE ɛ4 carrier status due to a substantial number of missing values. Follow-up time was used as a time variable, and the progression to dementia as a status variable.
All statistical analyses were performed using R (version 4.1.2). Statistical significance was set at < 0.05.
RESULTS
Demographics of the study population
The total cohort consisted of 63.5% men and had a mean age of 75 years. Before the propensity score matching, 2,181 patients were found to be in a euthyroid and 284 in a sHypo state. The sHypo group was older and had a higher education level than the euthyroid group. The propensity score-matched cohort comprised 1,118 patients in a euthyroid and 283 in a sHypo state, and the imbalance in the covariates including age and education level was alleviated, as expected. The covariate differences between the groups before and after matching are shown in Table 1.
Demographics and clinical characteristics of patients before and after propensity score matching
sHypo, subclinical hypothyroid; TFT, thyroid function test. Data are presented as the n (%) or median [interquartile range]. *APOE ɛ4 carrier information was unavailable for 611 patients in a euthyroid and 78 in a sHypo state in the unmatched cohort and 310 in a euthyroid and 78 in a sHypo state in the matched cohort.
Comparison of baseline cognitive profiles between the eythyroid and sHypo groups
Between the matched patient groups, there were no significant differences in general cognitive status, disease severity, depressive symptoms, attention, language, memory, and visuoconstructive and executive functions (Table 2).
Comparison of cognitive functions at baseline between the euthyroid and subclinical hypothyroid groups
CDR, Clinical Dementia Rating; CDR SOB, Clinical Dementia Rating sum of boxes; GDpS, short form of the Geriatric Depression Scale; MMSE, Mini-Mental State Examination; RCFT, Rey Complex Figure Test; sHypo, subclinical hypothyroid; SVLT, Seoul Verbal Learning Test. Data are presented as the mean±standard deviation or median [interquartile range]. Raw scores were used for the MMSE, CDR, CDR SOB, and Geriatric Depression Scale, and z-scores were used for the rest of the neuropsychological tests.
Clinical progression from MCI to dementia
Among 1,401 patients of the matched cohort, 1,127 patients had MCI with a baseline CDR score of 0.5, of which 379 patients had follow-up cognitive assessments. Among 379 patients with MCI, 109 patients progressed to dementia over 3 years. The median follow-up time was 712 days, with an interquartile range of 463 days.
In both models 1 (sHypo) and 2 (sHypo10), only baseline MMSE scores and education level showed a significant association with the disease progression (Table 3). Neither sHypo nor sHypo10 were related to the progression from MCI to dementia. The results were the same when analyzed without information about the APOE ɛ4 carrier. The progression of the disease in patients with euthyroid and sHypo states is shown as the Kaplan-Meier curve in Fig. 1.
Multivariate Cox regression analysis of disease progression from mild cognitive impairment to dementia
CI, confidence interval; HR, hazard ratio; MMSE, Mini-Mental State Examination; NI, not included; sHypo, subclinical hypothyroid; sHypo10, subclinical hypothyroid with THS over 10 mlU/L. *APOE ɛ4 carrier information was unavailable for 95 patients.
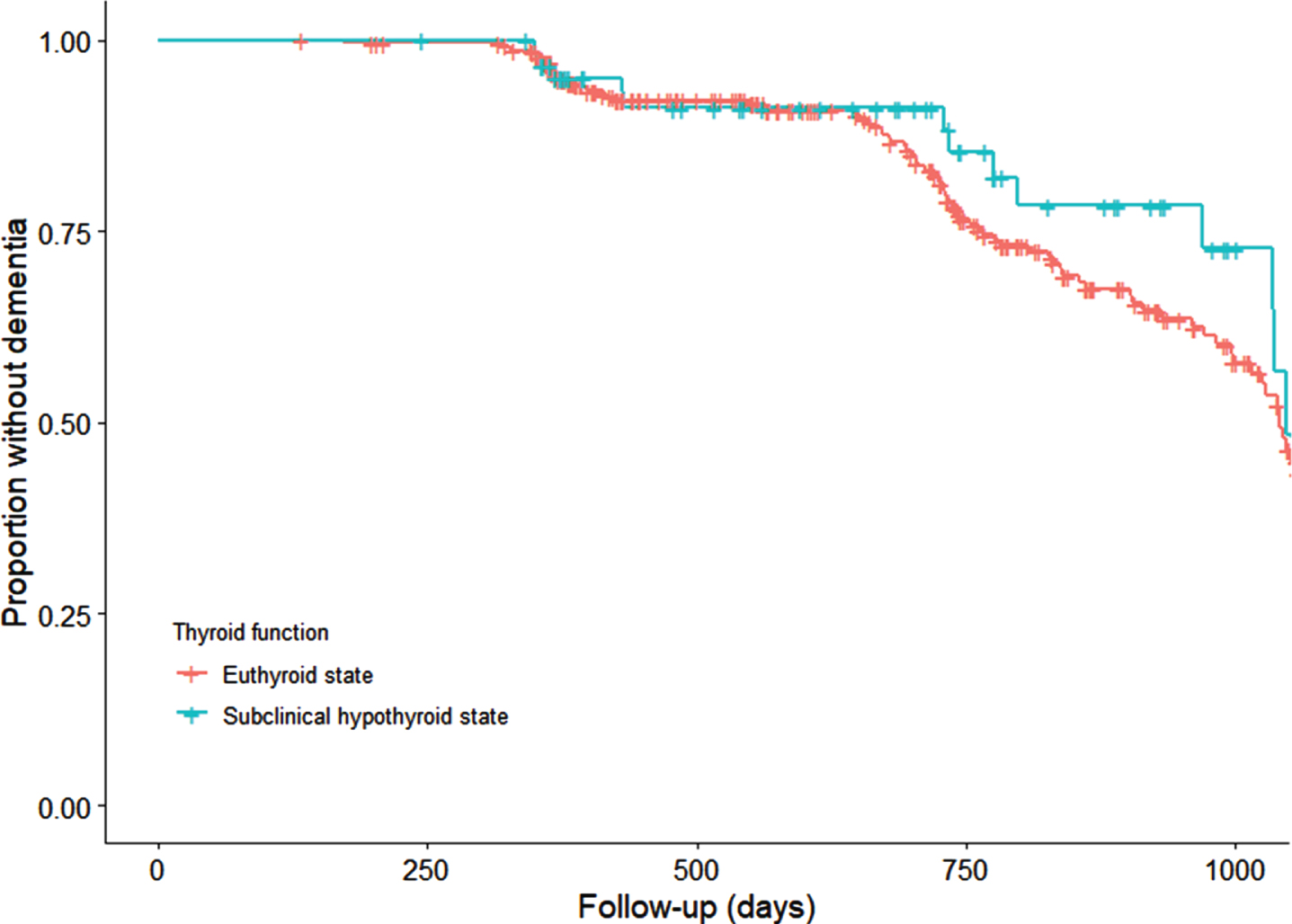
Kaplan-Meier survival plot comparing the progression from mild cognitive impairment to dementia between patients in euthyroid and subclinical hypothyroid states.
DISCUSSION
In this study in a propensity score-matched cohort, we found no difference in cognitive profiles between patients in a euthyroid and those in a sHypo state. Clinical progression from MCI to dementia was also not associated with sHypo or sHypo10.
Previous studies investigating the association between subclinical hypothyroidism and cognition have reported controversial results. Decreased immediate and delayed verbal memory on the MMSE was reported in a study in 15 patients in a sHypo state [18]. Another study found impaired memory function in 14 young patients (mean age 38.7 years) in a sHypo state [19]. On the other hand, numerous studies showed no association between subclinical hypothyroidism and cognitive impairment or decline in elderly people [8, 20–23]. A recent meta-analysis reported no association of subclinical hypothyroidism with cognitive performance and incident dementia [7]. However, cognitive performance was mainly measured on the MMSE scale, which evaluates global cognition without a sufficient assessment of the entire cognitive spectrum. Additionally, the relationship between subclinical hypothyroidism and incident dementia was assessed based on the 8 studies with only 136 cases. Considering the heterogeneity of these studies, a small number of cases in the meta-analysis may indicate the need for studies with large sample size. The results of our study could be strengthened by the large sample size in the form of single-center-data, extensive cognitive assessment, minimized bias in the case and control groups, stringent inclusion criteria with clear levels of TSH and free T4, and the exclusion of hormone users.
Another meta-analysis showed an increased risk of cognitive impairment and dementia in patients in the sHypo state, but only in those under 75 years of age. No correlation was found in the total population [24]. This difference may be related to potential misdiagnosis of subclinical hypothyroidism due to a lack of age-related reference ranges of TSH [24] or potential distinct pathomechanisms of thyroid dysfunction on cognitive abilities depending on age. Further studies are needed to explore these issues. Our study focused on subclinical hypothyroidism in elderly patients over 60 years of age, and the current findings may differ from the results for middle-aged or younger patients.
From the perspective of clinicians treating patients in a sHypo state with cognitive impairment, the question of whether that cause can be treated, are important concern. Several randomized controlled trials investigating the effect of levothyroxine therapy on cognition in subclinical hypothyroidism also presented inconsistent results, that is, improvement in cognitive functions as well as no improvement [25–28]. In our study, a subclinical hypothyroidism state of grade 2, which is more likely to be treated with thyroid hormones than grade 1 subclinical hypothyroidism [4], did not show an association with disease progression to dementia. This finding might provide a clue for the clinical decision making when it comes to different treatment options.
This study has several limitations. First, although demographic differences between groups were reduced by propensity score matching, the pathologies underlying cognitive impairment are heterogeneous. In the future, studying the effect of subclinical hypothyroidism in various disease entities with objective biomarkers might therefore be interesting. Second, this is a single-center study, and a multi-center study with a larger sample and a longer follow-up period is warranted to validate the current results.
Conclusion
This study found no differences in attention, language, memory, visuoconstructive, and executive functions between patients in a sHypo and those in a euthyroid state over 60 years of age. Progression from MCI to dementia was not associated with subclinical hypothyroidism, even at high TSH levels. These findings may be relevant for practitioners choosing a treatment strategy for hormone therapy in subclinical hypothyroidism with cognitive impairment.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0302r1).