
Abstract
Background:
Subjective cognitive decline (SCD) is related to personality functioning and risk of subsequent objective cognitive impairment.
Objective:
The aim of this study was to examine whether lower neuroticism and higher conscientiousness—resilient personality traits—protect against conversion from SCD to objective cognitive impairment in two longitudinal community-based cohorts.
Methods:
Data from the Health and Retirement Study (N = 1,741, Mean age = 68.64 years, Follow-up mean = 7.34 years) and the National Health and Aging Trends Survey (N = 258, Mean age = 79.34 years, Follow-up mean = 4.31 years) were analyzed using Cox regression analysis, controlling for sociodemographic covariates, symptoms of anxiety and depression, and apolipoprotein ɛ4.
Results:
The pooled results showed that lower neuroticism and higher conscientiousness were associated with decreased risk of conversion from SCD to objective cognitive impairment.
Conclusion:
Among individuals with SCD, those with a resilient personality may have more cognitive and psychological reserve to maintain cognitive functioning and delay conversion to objective cognitive impairment. The findings further contribute to a better understanding of personality along the cognitive continuum: The observed effect sizes were smaller than those reported in cognitively normal individuals but larger than in individuals with mild cognitive impairment. Personality could provide useful information to identify individuals with SCD who may develop objective cognitive impairment—namely those who hold a vulnerable personality (higher neuroticism, lower conscientiousness).
Keywords
INTRODUCTION
It is estimated that 55 million people have dementia worldwide, and nearly 10 million new cases occur each year [1]. Given that there is no cure for dementia to date, characterization of early risk stages and detection of the disease are crucial for targeted prevention [2]. Subjective cognitive decline (SCD) is potentially the earliest risk stage of dementia [3, 4]. SCD refers to perceived decline in memory and other cognitive abilities compared to previous abilities in the absence of objective cognitive dysfunction [5]. In the updated Alzheimer’s disease (AD) research framework of the National Institute on Aging and Alzheimer’s Association, SCD is recognized within the cognitively unimpaired stage on the cognitive continuum, a stage that precedes the first objective cognitive symptoms [6]. A recent study combined data from 15 countries across five continents and concluded that prevalence of SCD is about 25% in cognitively unimpaired individuals aged 60+ years [7]. About 25% of individuals with SCD go on to develop mild cognitive impairment (MCI) and about 11% develop dementia over the following five years [8].
In the last few years, SCD has received increasing attention due to interest in characterizing the preclinical stages of AD [9, 10]. Research has identified a broad range of factors associated with increased risk of conversion from SCD to objective cognitive impairment, such as worry about cognition [11], apolipoprotein ɛ4 (APOE) allele [12], and low education [13]. Among the factors associated with SCD, personality has been recognized as a relevant factor [14]. Of the Five-Factor Model (FFM) personality traits, particularly higher neuroticism and lower conscientiousness are associated with SCD [15–18]. Neuroticism and conscientiousness have also been associated with transitions in cognitive status: Among individuals with intact cognition, for example, higher neuroticism and lower conscientiousness are well-established risk factors for the development of MCI and dementia over time [19–23]. Less is known, however, about the predictive power of personality during further transitions, such as from MCI to dementia. In a previous HRS analysis, lower conscientiousness (but not higher neuroticism) was associated with increased risk of conversion from cognitive impairment no dementia (CIND) to dementia over the up to 12-year follow-up [24]. Another study found that high scores in rigidity (a construct related to conscientiousness) were associated with a lower risk of conversion from MCI to dementia over the up to 10-year follow-up [25]. A recent study, however, did not find any effects of neuroticism nor conscientiousness on the transition between MCI and dementia over up to 23 years [23]. Further, biomarker studies suggest that personality confers resilience against cognitive dysfunction even in the presence of neuropathology [26–28]. For example, a recent study reported that individuals with lower neuroticism performed better on cognitive tasks relative to their level of pathology, while individuals with higher conscientiousness experienced less cognitive decline relative to their level of pathology [26].
Nevertheless, it is currently unclear whether personality is associated with risk of conversion from SCD to objective cognitive impairment. In particular, the extent to which individuals with SCD who hold a vulnerable personality (higher neuroticism, lower conscientiousness) are at heightened risk of progression to objective cognitive dysfunction remains unassessed. In personality research, the most common approach is to examine neuroticism and conscientiousness separately, but it is also possible to investigate combinations or interactions of these traits. Specifically, someone who scores both high on neuroticism and low on conscientiousness may have a vulnerable personality (while reversely, someone who scores low on neuroticism and high on conscientiousness can be considered as having a resilient personality), and someone who scores both high on neuroticism and high on conscientiousness may be a healthy neurotic. There is a separate line of research on healthy neuroticism [29–31], which has been motivated by the observation that neuroticism can lead to poor health (via anxiety-provoked maladaptive behaviors) as well as better health (due to anxiety-provoked vigilance) [32, 33]. For example, healthy neuroticism has been found to be protective against smoking and physical inactivity [29], but its association with cognitive health remains to be investigated. The present study will examine combinations of neuroticism and conscientiousness in addition to their singular effects during the transition from SCD to objective cognitive impairment.
Such knowledge is critical for two reasons. First, it will inform interventions to maintain cognitive and psychological health in individuals with SCD [34]. These individuals are a target population of particular interest because they perceive cognitive decline prior to detection of objective impairment. And, even if they do not progress to cognitive impairment (i.e., the etiology of SCD is non-AD related), SCD can lead to anger, increased stress, and fear of dementia—and thus should be treated to maintain psychological well-being [35] and quality of life [36]. Second, a better understanding of personality across the cognitive continuum is needed. The cognitive continuum ranges from a cognitively unimpaired stage (with or without SCD) to CIND/MCI and dementia (with dementia further subdivided into mild, moderate, and severe stages) [6]. To date, it is unclear whether the effect of personality on onset of the next stage changes in magnitude along the cognitive continuum. For example, if the effect of neuroticism on onset of further impairment strengthened from SCD to MCI (i.e., the effect size is greater in individuals with MCI than in individuals with SCD), the reverse causation hypothesis could be supported. In the reverse causation model, personality is a prodrome or other subclinical manifestation of AD rather than a risk factor. The hypothesis suggests that personality is changed by the underlying neuropathology in the prodromal phase of dementia (but see [37]). If that were the case, the association between neuroticism and onset of impairment would be stronger in individuals with MCI, because neuroticism would be expected to increase towards the onset of dementia. In our previous work, however, the association between personality and dementia risk was substantially weaker in individuals with CIND than in cognitively normal individuals [24], contradicting the reverse causation hypothesis.
To our knowledge, there is only one study that examined the association of personality and risk of cognitive impairment in individuals with SCD: Bessi and colleagues [38] examined memory clinic visitors who reported persistent decline in cognitive capacities but performed normal on standardized cognitive tests, and found that those with lower neuroticism were at higher risk of progression to MCI over the up to 7-year follow-up. It should be noted, however, that the sample size was relatively small (N = 36) and that the results contrast with the broader personality-dementia literature. The present study aims to extend the current literature by examining the association between personality and conversion from SCD to objective cognitive impairment in two United States (U.S.) community-based cohorts of older adults followed for up to 7–12 years. We focus on neuroticism and conscientiousness, which are the strongest and most consistent predictors of dementia risk among the FFM personality traits [19–23]. We hypothesize that lower neuroticism and higher conscientiousness will be associated with decreased risk of conversion from SCD to objective cognitive impairment, controlling for sociodemographic, mood, and genetic covariates. In addition, we examine two combinations of neuroticism and conscientiousness: 1) low neuroticism and high conscientiousness (a resilient profile) and 2) high neuroticism and high conscientiousness (healthy neuroticism). We expect the resilient profile to be associated with decreased risk of progression to cognitive impairment. We do not state a hypothesis for healthy neuroticism due to the mostly null or mixed findings across different health outcomes [30]. We do not have hypotheses for openness, agreeableness, or extraversion, but we report the results to provide a comprehensive assessment of the role of personality in the conversion from SCD to objective cognitive impairment.
MATERIALS AND METHODS
Transparency and openness
The present research is based on deidentified data from two studies that are publicly available for registered users. We report how we determined our sample sizes and describe all measures. The hypotheses and statistical analyses of this project were preregistered. Links to data and preregistration can be found in the Acknowledgments.
Selected studies
This project used existing publicly available data from two cohort studies, the Health and Retirement Study (HRS) and the National Health and Aging Trends Survey (NHATS). The two cohorts were selected as they met the following criteria: 1) longitudinal study design, 2) assessment of personality, cognitive status (i.e., cognitive impairment), and subjective memory rating (compared to the past: i.e., SCD), 3) assessment of personality and SCD at the same wave, and 4) longitudinal data on cognitive impairment. Participants with complete data on neuroticism, conscientiousness, cognitive status, past memory rating, and sociodemographic covariates (i.e., age, gender, race, ethnicity, and education) were considered for eligibility. Since this study focuses on SCD, only participants who perceived memory decline but showed no cognitive impairment at baseline were included in the analyses. Figure 1 shows a flow chart about how eligible participants were identified.
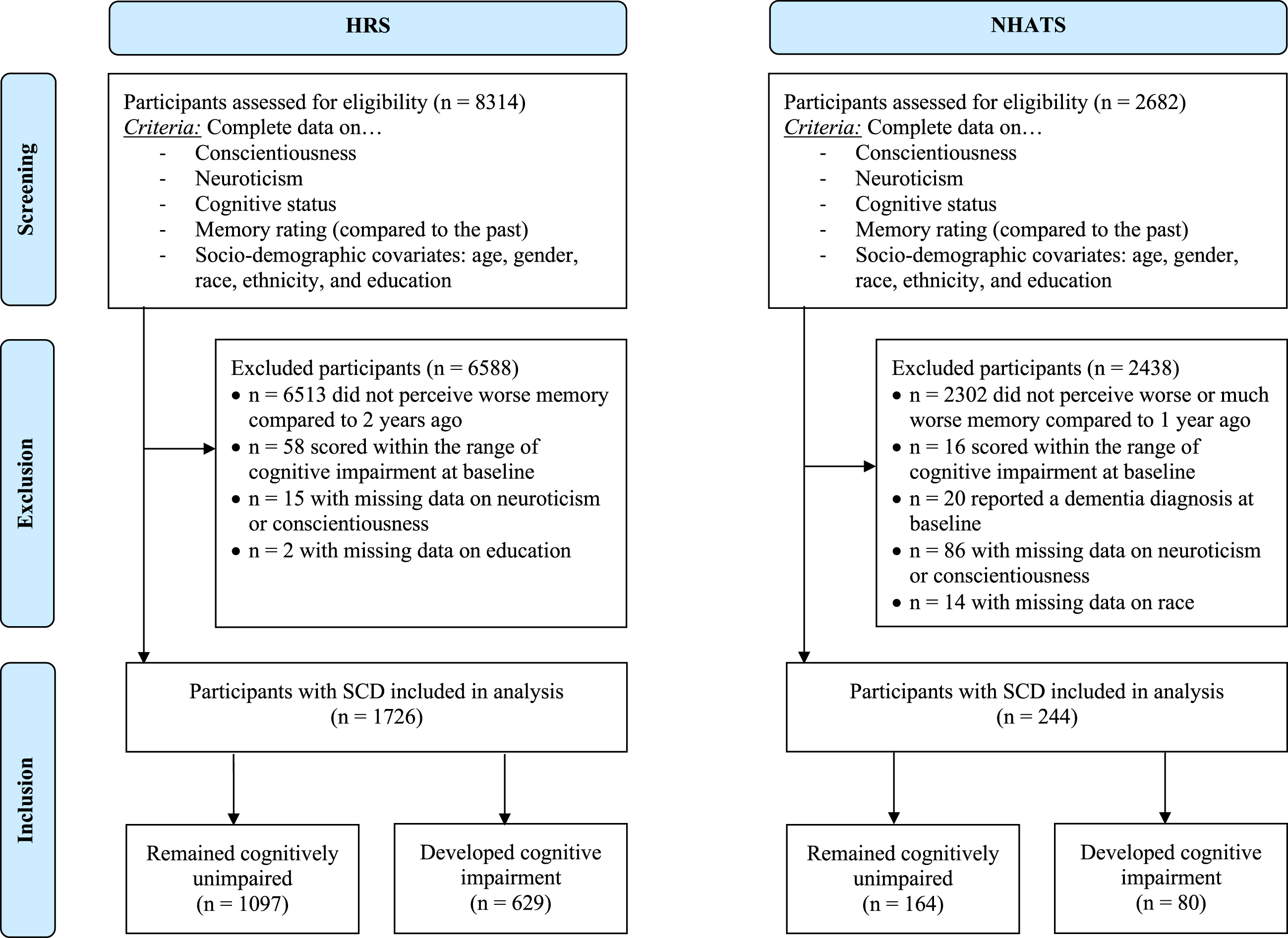
Flow diagram for identifying eligible participants with Subjective Cognitive Decline (SCD) in the Health and Retirement Study (HRS) and the National Health and Aging Trends Survey (NHATS).
HRS
The HRS is a longitudinal panel that tracks adults aged ≥50 years and their spouses (regardless of age) in the U.S. HRS uses a national area probability sample of U.S. households with supplemental oversamples of African Americans, Hispanics, and residents of the state of Florida. A detailed description of the multi-stage area probability sample design can be found elsewhere [39]. Data collection began in 1992 with biennial testing occasions. For the present analyses, we used data from 2006/2008 waves as baseline, as this is the first assessment that included both personality and SCD. For personality, HRS employed a half-sample strategy—half of the sample completed the questionnaire in 2006 and the other half completed it in 2008. We used the combined 2006/2008 personality data for the analyses. Data from 2008 (for those who completed the personality questionnaire in 2006), 2010, 2012, 2014, 2016, and 2018 were used to assess cognitive status.
NHATS
The NHATS is a prospective cohort study of Medicare enrollees aged ≥65 years in the U.S. Participants were first interviewed in 2011 and are re-interviewed annually. In 2011, participants were sampled in three stages: First, 95 counties (or groups of counties) were sampled from the U.S., then 655 ZIP codes were sampled within selected counties, and finally, 12,411 beneficiaries aged 65+ (enrolled as of September 2010) were sampled within selected ZIP codes and released to the field. For the last step, individuals at older ages and African Americans were oversampled. More information on the sampling methods is described elsewhere [40]. For the present analyses, data from 2013/2014 were used as baseline, as this is the first assessment that included both personality and SCD assessments. Of note, personality was assessed in 2013 for one third of the sample, and in 2014 for a second third of the sample. We used the combined 2013/2014 personality data for the analyses. Data from annual cognitive assessments from 2014 (for those who completed the personality questionnaire in 2013) up to 2020 were used to assess cognitive status.
Measures
Subjective cognitive decline
In HRS, participants were asked to compare their memory at the time of the interview to their memory at the previous assessment (2 years earlier), with response options on a 3-point scale: 1 = better, 2 = same, 3 = worse. In NHATS, participants were asked a similar question to compare their memory at the time of the interview to their memory at the previous assessment (1 year earlier), with response options on a 5-point-scale: 1 = much better, 2 = better, 3 = about the same, 4 = worse, 5 = much worse. Participants who rated their memory as “worse” (HRS) and “worse” or “much worse” (NHATS) but showed no objective cognitive impairment at baseline (see Cognitive Status) were classified as SCD and included in the present study.
Personality
In HRS, personality traits were assessed using the Midlife Development Inventory (MIDI) [41]. Participants were asked how well 26 adjectives described them on a Likert-type scale ranging from 1 (not at all) to 4 (a lot). The MIDI includes 4 items for neuroticism (e.g., moody; Cronbach’s α= 0.75), 5 for extraversion (e.g., outgoing; α= 0.78), 7 for openness (e.g., imaginative; α= 0.84), 5 for agreeableness (e.g., helpful; α= 0.82), and 5 for conscientiousness (e.g., organized; α= 0.72). A shorter 10-item version of the MIDI was used in NHATS, with each trait assessed with two adjectives on the same 4-point scale. Due to the brevity of the measure and because it has been developed by prioritizing content breadth over internal consistency, no Cronbach alpha was calculated [42].
The items were reverse-coded if needed and the mean was computed, so that higher scores represent higher levels of each trait. In addition, we created two binary variables, one for a resilient personality (low neuroticism, high conscientiousness) and one for healthy neuroticism (high neuroticism, high conscientiousness). Low and high scores were determined calculating the mean scores within each sample. Participants who scored below the sample mean on neuroticism and above the sample mean on conscientiousness were identified as having a resilient personality profile. Participants who scored above the sample mean on both neuroticism and conscientiousness were identified as having a healthy neuroticism personality profile. Personality profiles were coded as 1 (having a resilient or healthy neurotic personality, respectively) and 0 (not having a resilient or healthy neurotic personality, respectively).
Cognitive status
Cognitive status was used to identify objective cognitive impairment. Cognitive impairment was defined based on a combined approach of cognitive performance and self-/or informant-reported dementia. In HRS, three cognitive tasks were used to assess cognitive status: immediate and delayed word list recall task, serial 7 subtraction, and backward counting. These three tasks are part of the modified Telephone Interview for Cognitive Status (TICSm) [43]. The total TICSm score is the sum of immediate and delayed recall of 10 words (0–20 points), serial 7 subtraction (0–5 points), and backward counting (0–2 points) [44]. A total score of 27 points is possible. Based on published criteria [45, 46], participants can be classified into “normal cognition” (12–27 points), “cognitively impaired not dementia (CIND)” (7–11 points) and “dementia” (≤6 points). Individuals with ≤11 points were identified as cases of cognitive impairment for the present analyses.
In NHATS, cognitive impairment was classified as follows [47, 48]: Participants completed a memory recall task (immediate and delayed recall of 10 common words), an orientation task (date, month, year, day of the week, President and Vice President), and a broad cognitive screening task (clock drawing). Participants who performed 1.5 standard deviations (SD) below the age-graded mean on at least two out of these three domains were identified as a case of cognitive impairment. Likewise, if participants or their proxy respondents reported that a doctor had diagnosed the participant with dementia or AD, they were also identified as case of cognitive impairment.
Covariates
Age (in years), gender, race, ethnicity, and education were included as sociodemographic covariates (Model 1). We dummy coded gender (0 = men, 1 = women), race (two dummy variables, one for African American coded as 1 = African American and 0 = White and Other; and one for otherwise identified race coded as 0 = African American and White, 1 = Other), and ethnicity (0 = non-Hispanic, 1 = Hispanic). Education was included in years in HRS and on a scale (from 1 = no schooling completed to 9 = Master’s, professional or doctoral degree) in NHATS. In both studies, covariates were self-reported.
In an additional model (Model 2), we further included symptoms of anxiety and depression. In HRS, anxiety symptoms were assessed using five items (fear of the worst happening; nervous; hands trembling; fear of dying; felt faint) from the Beck Anxiety Inventory [49]. Participants rated the frequency of these symptoms during the past week on a scale from 1 (never) to 4 (most of the time). Cronbach alpha was 0.81. Depressive symptoms were measured with the 8-item Center for Epidemiological Studies Depression Scale (CES-D) [50]. Participants reported whether they experienced depressive symptoms (feeling depressed; activities are efforts; having restless sleep; feeling happy; feeling lonely; enjoying life; feeling sad; feeling unmotivated) during last week (yes/no). Cronbach alpha was 0.79. In NHATS, symptoms of anxiety and depression were assessed using the 4-item Patient Health Questionnaire [51]. Participants reported on their anxiety symptoms (two items: feeling nervous, anxious or on edge; not being able to stop or control worrying) and depressive symptoms (two items: had little interest or pleasure in doing things; felt down, depressed, or hopeless) over the last month on a scale from 1 (not at all) to 4 (nearly every day). No reliability was calculated due to the brevity of the measure. In both studies, items were reverse-coded if needed. Following recommendations to apply cut-offs on mood scales in SCD research [14], we used binary variables of anxiety symptoms and depressive symptoms. Participants with scores ≥12 (HRS) and ≥3 (NHATS) on the anxiety scales were classified as having anxiety symptoms [51–53]. In both samples, participants with scores ≥3 on the depression scales were classified as having depressive symptoms [51, 55].
Finally, in HRS, APOE status was included (Model 3; note that NHATS does not have APOE data). Genetic information was consensually collected from participants in the HRS data set during the years of 2006–2012, including information on the presence of the APOE allele type. The procedure is described elsewhere [56]. We categorized participants with at least one ɛ4 allele as APOE4 carriers (coded as 1) versus non-carriers (coded as 0).
Statistical analyses
We used Cox proportional hazards (PH) survival models to test whether personality was associated with progression to objective cognitive impairment. Time-to-detection (survival time) was coded in years from baseline to the year in which participants scored in the range of objective cognitive impairment. Participants who did not score in the range of objective cognitive impairment were censored at the time of their last cognitive assessment. Cox PH models were run separately for each personality trait and each personality profile controlling for covariates: Model 1 controlled for age, gender, race, ethnicity, and education. Note that because only n = 14 NHATS participants identified as Hispanic, we dropped ethnicity from the statistical analyses in NHATS. Model 2 additionally included symptoms of anxiety and depression. In HRS, Model 3 controlled for APOE ɛ4 status in addition to the variables entered in Model 2. Continuous variables were z-standardized for ease of interpretation, such that associations with these variables (personality traits, age, and education) reflect differences of one standard deviation.
The analyses were run with R software [57]. Cox PH models were calculated using the “survival” package [58]. The estimates were pooled to provide a meta-analytic effect across samples using the “metafor” package [59]. Interpretation is based on the pooled estimates rather than individual study results. Using the function “test.ph”, we tested for the PH assumption with the global goodness-of-fit test based on the scaled Schoenfeld residuals. Assessment of Schoenfeld residuals for agreeableness (HRS) as well as age, gender, and African American (NHATS) revealed a potential violation of the assumption of proportionality. In accordance with the interaction method when a potential violation of the assumption occurs [60], we included interaction terms for these variables with time-to-event as covariates. Using the “rms” package [61], we calculated a Variance Inflation Factor (VIF) for each predictor variable to detect potential multicollinearity in the Cox PH models. Across all models in both samples, the VIF was <1.5 for each predictor, suggesting that multicollinearity was not a problem.
The sample sizes were determined using existing publicly available data sets. Power calculations were conducted using the R package “FDRsampsize“ [62]. Based on recent meta-analytic estimates [19], we used a hazard ratio (HR) = 1.24 for neuroticism and HR = 0.77 for conscientiousness as possible scenarios for the effect size, because SCD is recognized within the cognitively unimpaired stage on the cognitive continuum. HRS provides power of 99% for both neuroticism and conscientiousness, while NHATS provides power of 85% for neuroticism and 86% for conscientiousness to estimate these hazard ratios at the 5% significance level. We acknowledge that with alpha <0.05, the risk of type 1 errors is increased, especially in HRS, but the validity of any associations is more accurately tested by evidence of replication across studies [63]. A stricter alpha level would increase risk of false negative [64], especially in NHATS, and impede discovering potentially interesting findings in the first place [65].
RESULTS
The descriptive statistics are displayed in Table 1 for the full samples and separately for participants with SCD who progressed to objective cognitive impairment and those who did not. In HRS, compared to participants who remained cognitively intact (n = 1,097), participants who developed objective cognitive impairment (n = 629) were older (Cohen’s d = 0.49, p < 0.001), had fewer years of education (d = 0.43, p < 0.001), were more likely to identify as Hispanic (χ2 = 8.88, p < 0.01), African American (χ2 = 6.56, p < 0.01), or another race than White (χ2 = 14.93, p < 0.001), reported more symptoms of anxiety (χ2 = 4.13, p < 0.05) and depression (χ2 = 3.97, p < 0.05), and were more likely to have at least one APOE ɛ4 allele (χ2 = 12.10, p < 0.001). They further scored higher on neuroticism (d = 0.12, p < 0.05), lower on openness (d = 0.11, p < 0.05) and conscientiousness (d = 0.19, p < 0.001), and were less likely to have a resilient personality profile (χ2 = 14.93, p < 0.001). Those with a resilient personality profile had a longer follow-up (M = 7.96 years, SD = 3.33) than those without a resilient profile (M = 7.13 years, SD = 3.50; d = 0.24, p < 0.001). In NHATS, compared to participants who remained cognitively intact (n = 164), participants who developed objective cognitive impairment (n = 80) had fewer years of education (d = 0.29, p < 0.05) and were more likely to be female (χ2 = 4.90, p < 0.05). Follow-up time did not differ between individuals with (M = 4.41 years, SD = 2.07) and without (M = 4.28 years, SD = 2.11) a resilient personality profile (d = 0.06, p = 0.657). Table 2 summarizes the main findings for HRS and NHATS. The full results (including all model parameters) are reported in Table 3 (HRS) and Table 4 (NHATS).
Descriptive statistics for individuals with SCD
SCD, subjective cognitive decline; HRS, Health and Retirement Study; NHATS, National Health and Aging Trends Survey; M, mean; SD, standard deviation. Impairment refers to the group of participants with SCD who progressed to objective cognitive impairment, while no impairment refers to the group who did not. Group difference refers to Cohen’s d or χ2, respectively.
Personality and progression to cognitive impairment among individuals with SCD
SCD, subjective cognitive decline; HRS, Health and Retirement Study; NHATS, National Health and Aging Trends Survey; HR, hazard ratio; CI, confidence intervals; p, p-value. Model 1 controlled for age, education, gender, race, and ethnicity (in HRS). Model 2 included Model 1 covariates and symptoms of anxiety and depression. Model 3 (HRS only) included Model 2 covariates and APOE ɛ4 status.
Personality and progression to cognitive impairment among individuals with SCD in HRS
SCD, subjective cognitive decline; HRS, Health and Retirement Study; APOE, apolipoprotein; HR, hazard ratio; CI, confidence intervals; p, p-value. Sample size varied from n = 1,726 (Model 1) to n = 1,695 (Model 2) and n = 1,544 (Model 3).
Personality and progression to cognitive impairment among individuals with SCD in NHATS
N = 244. SCD, subjective cognitive decline; NHATS, National Health and Aging Trends Survey; HR, hazard ratio; CI, confidence intervals; p, p-value.
Personality and progression to cognitive impairment in SCD
In HRS, the Cox regression analysis indicated that for every standard deviation increase in neuroticism, there was a 16% increase in risk of progression to objective cognitive impairment for individuals with SCD over the up to 12-year follow-up (Table 2, Model 1). The effect size remained similar when controlling for mood covariates (Model 2) and APOE ɛ4 status (Model 3). Higher scores on conscientiousness were associated with reduced risk of progression to objective cognitive impairment, even in the fully adjusted model (HRModel3 = 0.88, 95% CI [0.80, 0.96], p < 0.01). In line with these results, having a resilient personality profile (low neuroticism, high conscientiousness) was associated with decreased risk of progression to objective cognitive impairment (HRModel3 = 0.74, 95% CI [0.60, 0.96], p < 0.01). In NHATS, the hazard ratios were in the same direction but not statistically significant (Table 2). Healthy neuroticism, extraversion, openness, and agreeableness were not associated with risk of progression to objective cognitive impairment in either sample.
The pooled estimates of the two studies were significant and supported our hypotheses: Low neuroticism and high conscientiousness were protective against conversion to cognitive dysfunction. Individuals with SCD who hold a resilient personality (combination of low neuroticism and high conscientiousness) were at decreased risk of progression to objective cognitive impairment. The other three traits and the combination of high neuroticism and high conscientiousness (healthy neuroticism) were not significant predictors.
DISCUSSION
This study examined the association between personality and risk of progression to objective cognitive impairment among individuals with SCD in two community-based cohorts. The findings suggest that having a resilient personality protects against conversion from SCD to objective cognitive impairment, even in the presence of genetic vulnerability.
SCD: Does a resilient personality prevent progression to impairment?
Individuals with SCD are a vulnerable group for developing dementia [5]. There is considerable variation in the timing to conversion, and not all individuals with SCD develop cognitive impairment, nor do not all individuals with cognitive impairment develop dementia [66, 67]. In line with our hypotheses, we found that among those with SCD, lower neuroticism and higher conscientiousness were protective factors against progression to objective cognitive impairment. Both effects were significant in HRS and in the meta-analysis, but not in NHATS (although the hazard ratios went into the expected direction). In HRS, the strength of the associations was nearly the same when taking mood and genetic covariates into account. These findings align with the broader personality-dementia literature [19, 25], but contrast with results from a previous SCD study, in which lower neuroticism was associated with increased risk of conversion from SCD to MCI [38]. Bessi and colleagues [38] suggest that among those with SCD and higher neuroticism, self-reported cognitive problems may represent a subjective complaint rather than a manifestation of an underlying neurodegenerative disease. This explanation refers to the “complaint hypothesis” [68] and implies that the etiology of SCD in individuals with higher neuroticism is non-AD related. We cannot exclude the possibility that this was the case for those 36 participants in Bessi and colleagues’ study; however, chance findings in small studies are not uncommon. Our findings suggest that high stress levels induced by neuroticism may provide high sensitivity to intra-individual change [14] such that individuals with higher neuroticism may be more hyper-aware of actual, subtle cognitive decline [69], and actual cognitive performance could be even worse than perceived [47]. Importantly, it could be that our findings differ from Bessi and colleagues’ study because we examined perceived memory decline, while they examined perceived cognitive decline. As such, our SCD measure was narrower (focusing on memory only), while their measure was broader (focusing on decline in any cognitive capacity). Another difference was that our study is based on two non-clinical samples, while they examined a clinical sample. Individuals who seek medical help for their cognitive problems differ from individuals with reported cognitive problems who do not seek medical help [70–72]. For example, help-seekers express more negative memory related beliefs compared to non-help-seekers [73], are more likely to express worry about dementia [74], and believe that their memory is worse than that of others [72].
More than simply complaints, a growing literature indicates that a vulnerable personality is associated with poor cognitive performance, SCD, AD neuropathology, and risk of MCI as well as dementia. For example, higher neuroticism and lower conscientiousness have been associated with worse cognitive performance, steeper cognitive decline, fewer years with healthy cognitive functioning (i.e., cognitive health span), and increased risk of both MCI and dementia [23, 75–81]. Further, cognitive complaints have been associated with AD neuropathology in those participants who scored high on neuroticism [82]. More broadly, neuroticism and conscientiousness have been associated with amyloid and tau neuropathology [28, 84]. It could be that personality modulates resistance to pathology [28], such that lower neuroticism and higher conscientiousness help to avoid the development of pathology. It is also possible that personality may increase resilience to pathology [26], such that lower neuroticism and higher conscientiousness facilitate coping with pathology. Among individuals with SCD, those with lower neuroticism and higher conscientiousness may have more cognitive and psychological reserve—accumulated over the lifespan—to maintain cognitive functioning despite neuropathological burden and thereby prevent or delay progression to objective impairment. For example, lower neuroticism and higher conscientiousness have been associated with engagement in cognitive activities [85], which help to build up cognitive reserve [86]. Likewise, individuals who score high on conscientiousness tend to be responsible and follow through with obligations, which may foster strong interpersonal connections that could promote additional cognitive stimulation and again contribute to cognitive reserve [87]. Lower neuroticism and higher conscientiousness have further been associated with healthier behavior in multiple domains, including physical activity, diet, and smoking [88–90] that are relevant for cognitive functioning [91]. It thus could be that, when perceiving cognitive decline, individuals with a resilient personality are eager to engage in even more health behaviors and stimulating activities that allow them to defy or slow the progression to objective impairment. In addition, these individuals may have more beneficial coping strategies to deal with perceived cognitive problems and stress in general. While neuroticism is associated with problematic strategies such as wishful thinking, withdrawal, and emotion-focused coping, conscientiousness is associated with problem-solving and cognitive restructuring [92]. In the long-term, problem-solving and cognitive restructuring may be better suited to reduce chronic stress and thereby slacken cognitive decline [93]. Moreover, specific aspects of emotional stability (low neuroticism) and conscientiousness might provide some psychological reserve to maintain functional independence despite incipient cognitive decline. For instance, people who are well-organized and self-disciplined (high in conscientiousness) tend to have structured daily lives [94]. A stable daily routine may help to keep individuals functional for longer because they know how to effectively move through their days even as cognitive functioning starts to decline [87].
The current findings do not support the idea that healthy neuroticism protects against progression to objective cognitive impairment. Specifically, the current study provides no evidence that high levels of neuroticism may be protective for individuals with SCD who also have high levels of conscientiousness, nor does it find that the negative effects of neuroticism on cognitive health are buffered by high levels of conscientiousness. Although healthy neuroticism may be beneficial for certain health behaviors (i.e., smoking, physical activity [29]), this effect may not be substantial enough to impact broader health outcomes such as chronic conditions [30], longevity [31] or cognitive health as examined in this study. For instance, conscientiousness may curb the behavioral tendencies of individuals high in neuroticism but do little to reduce the attenuated emotional stress reactivity of neuroticism. As such, the effects on health behaviors may not be large enough to translate into actual differences in progression to objective cognitive impairment. It is also possible that only certain facets of neuroticism or conscientiousness drive healthy neuroticism. For instance, high levels of depression (a facet of neuroticism) may not support cognitive health in any circumstance, but higher levels of anxiety (another facet of neuroticism) may be protective, such that individuals higher on this facet may be more afraid of dementia and thus more likely to seek help for their cognitive problems. Similarly, certain facets of conscientiousness, such as being systematic and self-disciplined, may be more health-beneficial than others (e.g., productiveness).
We did not make formal hypotheses regarding extraversion, openness, and agreeableness, and none of these traits was associated with progression to objective cognitive impairment. To our knowledge, the one previous SCD study [38] examined the effect of neuroticism—but none of the other traits—on risk of conversion from SCD to MCI; thus, the present study seems to be the first examining all FFM personality traits in conversion from SCD to objective impairment. Although there is some evidence that extraversion, openness, and agreeableness are protective against risk of cognitive dysfunction, these associations tend to be less robust and less consistent than for neuroticism and conscientiousness [19, 95]. It is unclear why neuroticism and conscientiousness seem to have a stronger impact on cognitive aging processes than the other traits, but it was noted that neuroticism has a strong emotional component [96] and conscientiousness has a strong behavioral component [94, 97], which may be most powerful in affecting underlying neurological degeneration. Further research is needed to better understand the role of extraversion, openness, and agreeableness among transitions of cognitive status.
Does the effect of personality weaken across the cognitive continuum?
Among individuals with SCD, those with higher neuroticism and lower conscientiousness were at ∼15% increased risk of progression to objective cognitive impairment. These findings may not be surprising, considering that cognitively normal individuals with higher neuroticism and lower conscientiousness are at increased dementia risk, and SCD is recognized within the cognitively unimpaired stage—that is, the same stage as cognitively normal individuals. For example, in our previous HRS analysis [24], we found that higher neuroticism and lower conscientiousness were associated with about 20% increased risk of dementia in cognitively normal individuals. Interestingly, the effect of personality seems to weaken during further transitions. In the transition from CIND to dementia, only lower conscientiousness (but not higher neuroticism) was a significant predictor in the previous HRS analysis [24]. The effect size was substantially smaller than the effect in the transition from normal cognition to dementia. Putting the findings from our previous and present HRS work together, the decrease of effect sizes along the cognitive continuum can be further observed: For every SD increase in neuroticism, the risk of dementia increased by 18% (HR = 1.18, 95% CI [1.07, 1.30]) in cognitively normal participants [24], by 16% (HR = 1.16, 95% CI [1.08, 1.26]) in participants with SCD (this study), and by 7% (HR = 1.07, 95% CI [0.99, 1.17]) in participants with CIND [24]. The protective effect of conscientiousness likewise extenuated along the cognitive continuum in HRS participants, with effect sizes changing from HR = 0.80 (95% CI [0.73, 0.88]; normal cognition) to HR = 0.86 (95% CI [0.80, 0.93]; SCD) to HR = 0.92 (95% CI [0.86, 0.99]; CIND). A similar pattern can be found in the study of Yoneda and colleagues [23]: Higher neuroticism and lower conscientiousness were related to increased risk of transitioning from normal cognition to MCI, with effect sizes of HR = 1.12 (95% CI [1.04, 1.21]) for neuroticism and HR = 0.78 (95% CI [0.72, 0.85]) for conscientiousness—but then, during the transition from MCI to clinically diagnosed dementia, these effects were reduced to non-significance, with sizes of HR = 1.12 (95% CI [1.00, 1.26]) for neuroticism and HR = 0.96 (95% CI [0.85, 1.09]) for conscientiousness. These patterns of findings indicate that the effect of personality on transitions in cognitive status weakens along the cognitive continuum. In other words, conscientiousness and neuroticism may be associated with cognitive functioning most substantially in the early transitions from normal cognition to cognitive impairment. Once an individual progresses to MCI, the characteristic of a resilient personality may have less power to protect against underlying neurological degeneration [23]. Such a pattern also contrasts with expectations from the reverse causality hypothesis: If personality was changed in the prodromal phase of dementia (as suggested by the reverse causality hypothesis), the association between personality and risk of cognitive impairment would be stronger among individuals with SCD and CIND (because neuroticism/conscientiousness would be expected to increase/decrease in those progressing toward the onset of dementia), but the opposite pattern has emerged. Other studies also contrast the reverse causation model by showing that (a) changes in personality were not significantly different between individuals who developed dementia versus individuals who remained cognitively intact over time [37] and (b) high school personality in adolescence—when individuals presumably are free of AD neuropathology—predicted dementia risk five decades later [95].
Future research is needed to study the causal pathways of personality along the cognitive continuum and its interactions with other factors (e.g., biomarkers). Understanding these complex interactions may increase the knowledge about the development of dementia. It may also be important to consider how the timing between measures affect these associations. Finally, future SCD studies should follow recommendations of the SCD-I working group on how to operationalize and implement SCD criteria that will help foster comparability and harmonization of criteria for future clinical trial enrollment [3, 14].
Strengths and limitations
This study has several strengths, including the use of two samples from well-characterized national panel studies of older adults, the longitudinal study design, a multi-analytical approach of resilient personality, the inclusion of mood covariates in both studies, and the inclusion of APOE status in HRS. There are some limitations to be considered. We examined two non-clinical samples, and findings may be different in clinical samples. More research in memory clinic visitors with SCD is needed to examine whether a resilient personality protects against progression to objective cognitive impairment.
Although we used established cognitive cut-offs to identify cognitive impairment, the operationalization and assessment interval (every 2 years in HRS versus annually in NHATS) was different across both samples. Furthermore, in both samples, the cognitive assessment was brief and mostly focused on episodic memory. Likewise, the SCD measure focused on memory only. Although memory decline is a prominent manifestation in SCD, complaints beyond memory are also reported [5, 98]. Memory concerns are highly prevalent in older adults (∼53% in a large population-based sample [99]) and may thus be highly sensitive but not specific for the detection of preclinical AD. Complaints in other domains may be more characteristic of non-normative decline at the early stages of AD [98]. Our SCD did not include worry associated with SCD; a SCD-plus feature [5] that is important to assess, and, in general, there is still no standard measurement for SCD available in the field [98]. In addition, our SCD measure was a single-item and differed slightly across samples regarding the time frame (2 years in HRS versus 1 year in NHATS) and answer scale (“worse” in HRS versus “worse” and “much worse” in NHATS). These inconsistencies may limit comparability across studies and the generalizability of findings. Future studies should use a more comprehensive SCD measure that considers complaints in various cognitive domains (e.g., language, visuospatial, executive function) and SCD-plus features.
Moreover, both studies had brief measures of personality, particularly NHATS with only two items per trait. Such limited measures may not comprehensively assess each trait, and do not allow to assess facet-level personality. Facets could provide a more fine-grained picture about resilient personality and healthy neuroticism, and a better understanding of the personality-SCD association in general.
Finally, due to limited representation of participants who identified as Hispanic, we had to drop ethnicity from the analyses in NHATS. Additional work is needed to examine the generalizability of our findings in more diverse samples. This is important because the reporting of SCD may be influenced by cultural practices and social determinants of health. For example, in a sample of Hispanics, SCD was found to be associated with depressive symptoms rather than concurrent cognitive performance [100], and another study found that African Americans were less likely to report SCD despite greater evidence of objective cognitive decline than Whites [101]. Further, Hispanics and African Americans are more likely to experience limited access to health care, lower level of education, less income, and lack of social support [102], which all are well known risk factors of dementia [103].
Conclusion
In sum, the present findings suggest a heightened risk of conversion from SCD to impairment in individuals with higher neuroticism and lower conscientiousness. Personality could provide useful information to identify individuals with SCD who may develop objective cognitive impairment. Using web-based questionnaires, it could be possible to inexpensively screen people in both communal and clinical settings to identify those with scores high on neuroticism and low on conscientiousness [96, 104]. Individuals with a vulnerable personality may benefit most from inclusion into SCD interventions to maintain cognitive health, psychological well-being, and quality of life—or, once established, into personality interventions [105] that aim to decrease neuroticism and increase conscientiousness. Translational research is needed to determine the feasibility of a systematic application of personality surveys in memory clinics, to develop personality-tailored interventions, and to test whether individuals with a vulnerable personality respond well to such interventions.
Footnotes
ACKNOWLEDGMENTS
This work has been supported by the National Institute on Aging of the National Institutes of Health under Award Numbers R01AG068093 (PI: Antonio Terracciano) and R01AG053297 (PI: Angelina R. Sutin). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The authors gratefully acknowledge the parent studies whose public data made this work possible: The Health and Retirement Study (HRS) is sponsored by the National Institute on Aging (NIA-U01AG009740) and conducted by the University of Michigan. The National Health and Aging Trends Study (NHATS) is being conducted by the Johns Hopkins University Bloomberg School of Public Health, with data collection by Westat, and support from the National Institute on Aging.
HRS was approved by the Institutional Review Board of the University of Michigan, NHATS was approved by the John Hopkins Bloomberg School of Public Health Institutional Review Board.
The present research is based on deidentified data that are publicly available for registered users. Data and research materials are available at https://hrs.isr.umich.edu/about
(HRS) and https://www.nhats.org/ (NHATS). The hypotheses and statistical analyses of this project were preregistered at ![]() .
.