
Abstract
In people with dementia, provision of mobility aids is standard treatment for those with impaired gait. However, mobility aid use is independently associated with increased falls risk. In this short communication, gait velocity and stride time variability were recorded in eleven adults with Alzheimer’s disease dementia. Three conditions were tested: single-task (no aid), walking with a walker, and dual-task (walker use and counting backwards) under both a straight path and Figure-of-8 walking configuration. Gait velocity increased when using a walker compared to no aid in the Figure-of-8 walking configuration. Walker use improved gait in simple walking, but benefits diminished upon dual-task.
INTRODUCTION
Balance and gait problems are common in people with Alzheimer’s disease (AD) dementia [1]. These mobility deficits are progressive [1] and prominent factors for an increased risk for falls [2]. Compared to cognitively healthy older adults, people with dementia have twice the annual risk for falls and are more susceptible to serious injuries [3]. Providing a mobility aid is standard treatment used to compensate for balance and gait problems [4]. Paradoxically, mobility aids are independently associated with a three-fold increase in the odds of falling [5].
Mobility aids enlarge the base-of-support and provide haptic feedback [6]. While there are benefits to stability, using mobility aids is cognitively demanding and a complex motor task [4]. Proper use requires planning, specific motor sequencing, and insight into the environment (e.g., maneuvering around obstacles) [4, 6]. For people with dementia, the planning and completion of complex motor tasks is difficult [7]. Moreover, the increased cognitive demands with mobility aid use are associated with deteriorated gait and instability [8–10].
In older adults without cognitive impairment dependent on a mobility aid for ambulation, 4-wheeled walkers result in increased gait velocity, stride length, and better stability relative to when no aid is used [11]. It is unknown if these changes to gait would also be seen in people with dementia. What is currently known in people with dementia is that walking using a walker through increasing path complexity and under situations of divided attention (i.e., dual-task testing) results in decreased gait velocity and increased stride time variability [10], an established marker for gait instability associated with falls [12]. The effectiveness of mobility aids for those with impaired mobility and cognitive function has not been evaluated in-depth but could inform prescription and training.
The study objective was to evaluate the effect of using a 4-wheeled walker on gait across different tasks and walking paths compared to walking without an aid in people with dementia. It was hypothesized that using a walker would improve gait in simple situations, but benefits would deteriorate in complex situations.
METHODS
Participants
Participants were recruited from a day program for adults with dementia in London, Canada (December 2019-March 2020). Program admission required a diagnosis of probable AD dementia [13]. The study inclusion criteria were: ≥50 years of age, mild-moderate AD dementia, able to follow instructions, currently using a 4-wheeled walker and able to walk 60-m without support. Mild-moderate dementia severity was confirmed using the Mini-Mental State Examination (MMSE) [14, 15]. Exclusion criteria were any medical condition limiting movement. Informed written consent was obtained either from the participant or substitute decision maker. Participants also provided verbal assent prior to collection if consent was initially obtained from a substitute decision maker. This study was approved by the Health Sciences Ethics Review Board of The University of Western Ontario.
Outcome measures
Sociodemographic and medical information included age, gender, height and weight, years of education, comorbidities, prescription medications, 12-month falls history as per Lamb et al. [16], basic and instrumental activities of daily living using the Lawton-Brody scales [17], and information about mobility aid prescription and use. Global cognitive status was evaluated using the MMSE [14], while the Falls Efficacy Scale International assessed for falls efficacy [18]. The participants’ physical function and proper 4-wheeled walker use was evaluated with the Safe Use of Mobility Aids Checklist (SUMAC) [19]. The SUMAC includes nine functional tasks, each scored for physical function (range: 0–40) and interaction with the equipment (range: 0–63). A higher SUMAC score is indicative of better performance using a walker [19].
Gait assessment
Two tri-axial accelerometers (LEGSystrademark, BioSensics, Cambridge, MA, USA) affixed below the tibial tuberosity of each lower limb in a frontal plane orientation were used to record spatiotemporal gait. The gait variables of interest were velocity and stride time variability (coefficient of variation) as these are the most common parameters for the domains of pace and variability [20]. Reduced gait pace and increased variability are associated with aging and cognitive impairment [20]. Gait variability is a reflection of motor task automaticity [12] and a proxy for instability due to the link that exists to the risk for falls [21,22, 21,22].
Gait testing was performed at a usual walking pace under three task conditions: single-task (ST)- walking without a 4-wheeled walker, walking with a 4-wheeled walker (4WW), and dual-task (4WW-DT)- walking with a 4-wheeled walker while counting backwards by ones beginning from a random number between 100–150 out loud. All responses were recorded for accuracy and no instructions were given to prioritize any one task.
Each walking task was completed over two configurations: a 6-meter straight path and the Figure-of-8 Walk Test [23]. Only steady state walking was recorded for the straight path configuration, while for the Figure-of-8 Walk Test participants walked over a floor template to standardize the path used. A practice trial followed two trials that were averaged. Walking without a walker was completed first, followed by 4WW and then 4WW-DT for the straight path and Figure-of-8 Walk Test. A seated rest was provided between tests or when requested.
Data analysis
Continuous variables were summarized using medians and interquartile ranges [25th, 75th percentile] and categorical variables were summarized as frequencies and percentages.
Gait velocity and stride time variability differences across tasks and walking paths were evaluated using Friedman’s ANOVAs. If statistically significant, pairwise comparisons were performed using Wilcoxon Signed-Rank Tests. Cohen’s r, a non-parametric effect size, was calculated for each comparison [24]. The software SPSS (version 25.0, IBM Corp., Armonk, NY, USA) was used to run all statistical analyses using a 0.05 experiment-wise alpha alongside Holm-Bonferroni adjustments for multiple comparisons.
To examine the effect that using a 4-wheeled walker had on gait, the relative change in an individual’s performance between walking without a walker and walking with a walker was also calculated using the following formula:
Relative changes in performance are reported as a percentage with positive values indicating better gait performance upon using a walker, while negative values indicate deteriorated performance.
RESULTS
Eleven people participated (median age: 91.0 years [84.0, 92.0], female: 64%, MMSE: 19.0 [16.0, 20.0]) (Table 1). Participants indicated having used a walker for 3.0 years [1.5, 4.0], and scored 27.0 [25.0, 32.0] and 45.0 [43.0, 47.0] on the SUMAC for physical function and interaction with equipment, respectively.
Most participants had been prescribed their walker by a healthcare professional (82%), which was set-up and fit (82%) and participants had also been taught how to use it (73%) (Table 1). Everyone expressed feeling steady when using their walker.
Sociodemographic and clinical characteristics in sample of people with Alzheimer’s disease dementia who use 4-wheeled walkers for ambulation (n = 11)
IQR: 25th, 75th Interquartile range.
Straight path configuration
A statistically significant difference in gait velocity (p < 0.001) across tasks was observed (Fig. 1a). Gait velocity was lowest for 4WW-DT (0.44 m/s [0.35, 0.55]), and was significantly different to ST (0.67 m/s [0.54, 0.96]; adj. p = 0.01, r = 0.89) and 4WW (0.62 m/s [0.59, 0.98]; adj. p = 0.01, r = 0.88). Gait velocity was not different between the ST and 4WW task (adj. p = 0.66).
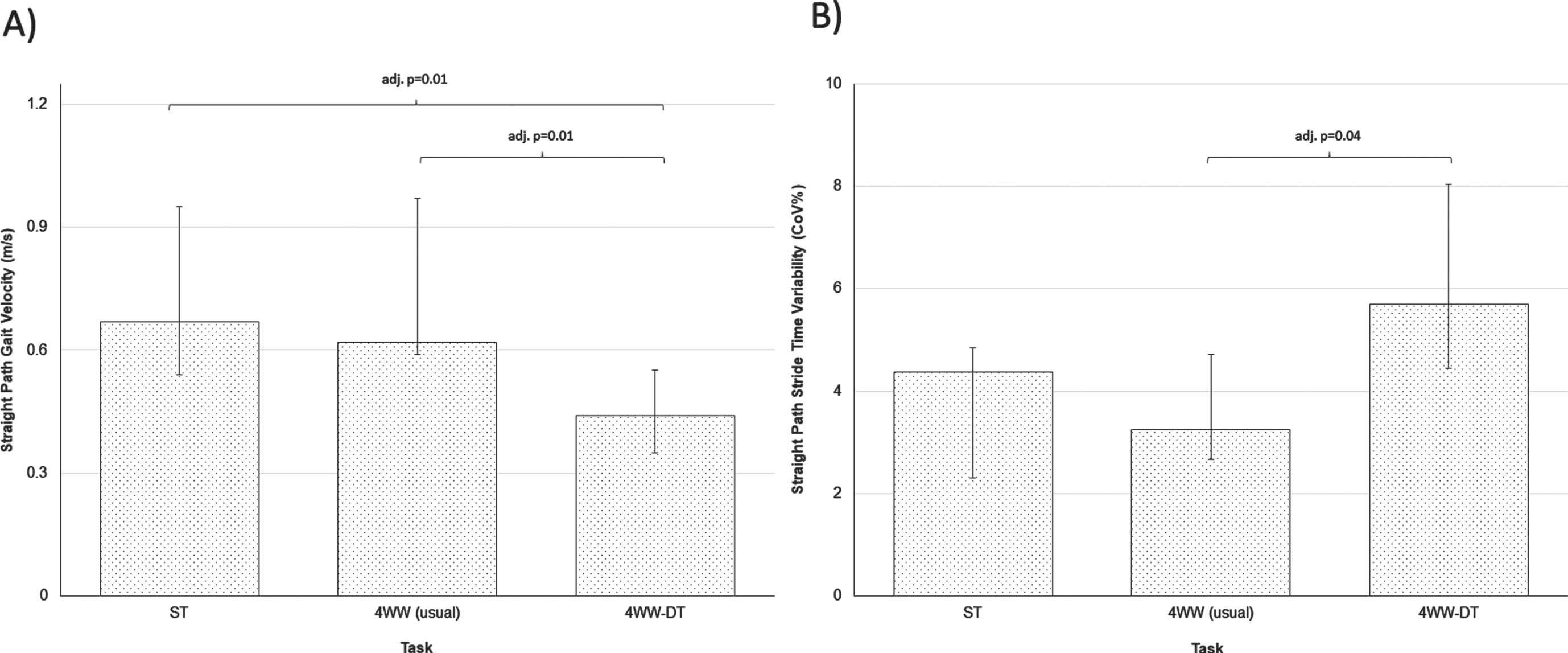
Evaluation of A) gait velocity and B) stride time variability for people with dementia walking without a 4-wheeled walker, walking with a 4-wheeled walker (usual) and walking with a 4-wheeled walker while completing serial subtractions over a straight walking path. 4WW, walking with a 4-wheeled walker (usual); Adj., Holm-Bonferroni adjusted p-values; 4WW-DT, dual-task (walking with a 4-wheeled walker while completing a secondary cognitive task); ST, single-task (walking without a 4-wheeled walker). Statistical significance was p < 0.05 for pairwise comparisons using Wilcoxon Signed-Rank Tests. Medians [25th, 75th Interquartile range] displayed.
For stride time variability, a statistically significantly difference (p = 0.02) across tasks was also observed (Fig. 1b). Stride time variability was highest for 4WW-DT (5.69% [4.45, 8.04]), followed by ST (4.38% [2.31, 4.85]) and 4WW (3.25% [2.66, 4.71]). However, a significant difference was only observed between 4WW and 4WW-DT (adj. p = 0.04, r = 0.79).
Figure-of-8 Walk Test
One participant was unable to complete ST trials, thus testing was based on a smaller sample (n = 10). A statistically significant difference in gait velocity (p < 0.001) across tasks was observed (Fig. 2a). Gait velocity was highest for 4WW (0.38 m/s [0.25, 0.54]) and was significantly different to ST (0.29 m/s [0.17, 0.48]; adj. p = 0.01, r = 0.89) and 4WW-DT (0.27 m/s [0.20, 0.37]; adj. p = 0.01, r = 0.89), but not between ST and 4WW-DT (adj. p = 0.84).
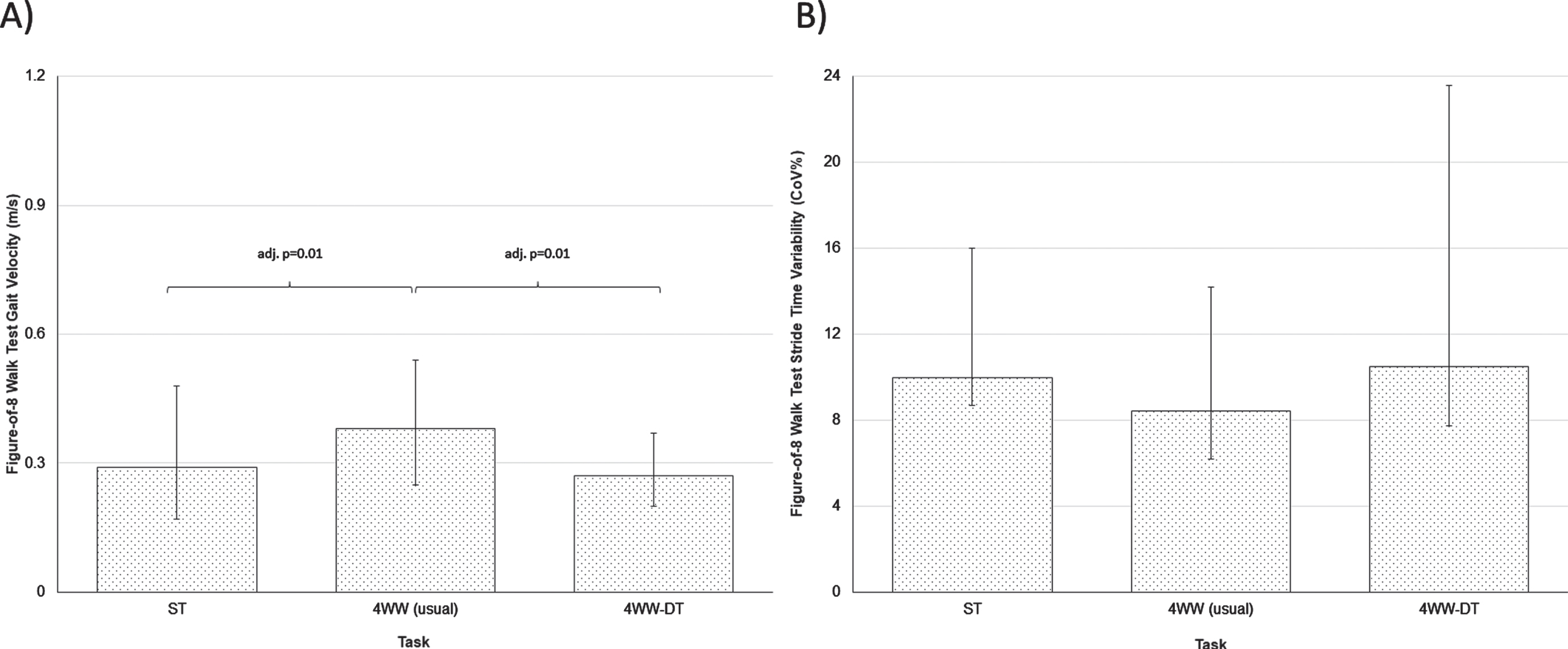
Evaluation of A) gait velocity and B) stride time variability for people with dementia walking without a 4-wheeled walker, walking with a 4-wheeled walker (usual) and walking with a 4-wheeled walker while completing serial subtractions during the Figure-of-8 Walk Test. 4WW, walking with a 4-wheeled walker (usual); Adj., Holm-Bonferroni adjusted p-values; 4WW-DT, dual-task (walking with a 4-wheeled walker while completing a secondary cognitive task); ST, single-task (walking without a 4-wheeled walker). Statistical significance was p < 0.05 for pairwise comparisons using Wilcoxon Signed-Rank Tests. Medians [25th, 75th Interquartile range] displayed.
For stride time variability, the highest values were observed in 4WW-DT (10.49% [7.76, 23.59]), followed by ST (9.97% [8.69, 15.99]) and 4WW (8.45% [6.2, 14.18]) (Fig. 2b). However, no significant differences were observed (p = 0.24).
Relative changes in gait performance
The ST to 4WW relative change in performance for gait velocity was 4.5% [–6.3, 14.8] in the straight path and 27.5% [15.2, 42.0] for the Figure-of-8 Walk Test. For stride time variability, these values were 16.9% [–35.7, 38.9] and 32.4% [7.2, 41.0], respectively.
DISCUSSION
Walking with a 4-wheeled walker resulted in a significant gait velocity increase compared walking with no aid in the complex walking path configuration. Descriptive analysis of the magnitude of change between task conditions also suggests that stride time variability decreased for trials of walking with a walker aid relative to walking with no aid. Interestingly, gait velocity and stride time variability when walking with no aid was similar in performance to complex situations involving dual-task testing while walking with a walker for people with AD dementia prescribed this type of device for everyday use.
This is the first study in people with AD dementia to examine both benefits and adverse changes to gait associated with the use of walkers relative to trials without an aid. The current findings are consistent with Härdi et al. [11] who indicated that the use of 4-wheeled walkers significantly increased gait velocity and stride length, decreased double support time, and also resulted in lesser stride time variability although not statistically significant in community-dwelling older adults. The sample recruited in our study exhibited considerably lower gait velocities and higher stride time variabilities when walking without a walker compared to what was reported by Härdi et al. [11]. Thus, relative gait changes with the use of a walker our study reports arguably represents a larger and more meaningful effect knowing the limited physical abilities of the participants we recruited.
Also demonstrated was that dual-task testing while using a walker resulted in adverse gait performance which was of similar magnitude to when participants walked without an aid. A higher gait variability is reflective of stride-to-stride inconsistencies (i.e., gait instability) [12] which increases the risk for falls [21, 22]. Even though walkers provide physical support, dual-task gait testing led to cognitive-motor interference as the cognitive demands exceeded participants’ cognitive capacity. It appears there is agreement with the line of research suggesting that the higher odds of falling with mobility aid use in people with dementia [5] may be explained by the added cognitive load and subsequent changes to gait observed with the use of these devices.
Training for the safe use of a mobility aid may need evaluation in this patient group to minimize the resultant increase in cognitive load. No consensus guidelines exist for healthcare professionals to learn how to incorporate mobility aid training. Research related to mobility aid training in people with dementia is scarce [25]. People with dementia can acquire new motor skills; however, a tailored protocol is required [7]. Successful motor learning in this population includes using implicit learning strategies; high repetitions; guidance consistency; a training environment mimicking the living environment, and to accommodate for barriers (e.g., vision, language, etc.) [7]. Also absent is the relationship between mobility aid training, or mobility aid induced gait changes, and important clinical outcomes, such as falls. Future research should establish if the gait pattern seen with the use of walkers are also observed with other gait aids (e.g., canes) which are more prevalent [26], and more challenging to use due to their upper body and timingrequirements [6].
There are several considerations for interpretation. Results need to be confirmed using a larger sample and an expanded assessment that includes both lower and upper body mechanics. Findings cannot be generalized to all people with dementia as only community-dwelling individuals with mild-moderate AD dementia were included. Several strengths exist. Our data analysis included the quantification of the magnitude of changes in gait which allowed for a more detailed assessment of deviations. Moreover, our protocol included various tasks and walking paths that required increased cognitive demands and that are considered reflective of real-life situations.
Conclusions
Using a 4-wheeled walker resulted in increased gait velocity in the complex walking path compared to walking with no aid in people with AD dementia. Descriptive findings also depict decreased stride time variability with the use of a walker relative to performance without an aid. Comparable gait parameters were observed between trials of walking with no aid and dual-task testing while walking with a walker. Future research should establish mobility aid training protocols specific to this population and aimed at improving gait to minimize the risk for falls.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the Director of McCormick Dementia Services, Karen Johnson; the CEO of the McCormick Care Group, Steve Crawford; the Research Associate of McCormick Dementia Research, Catherine Blake; and the many staff and clients who assisted and participated in this project. This work was supported by The Ontario Neurotrauma Foundation (2019-PREV-FALL-1070) which had no involvement in the conduct of the study.