
Abstract
Background:
Older adults presenting with dual-decline in cognition and walking speed face a 6-fold higher risk for dementia compared with those showing no decline. We hypothesized that the metabolomics profile of dual-decliners would be unique even before they show signs of decline in cognition and gait speed.
Objective:
The objective of this study was to determine if plasma metabolomics signatures can discriminate dual-decliners from no decliners, purely cognitive decliners, and purely motor decliners prior to decline.
Methods:
A retrospective cross-sectional study using baseline plasma for untargeted metabolomics analyses to investigate early signals of later dual-decline status in study participants (n = 76) with convenient sampling. Dual-decline was operationalized as decline in gait speed (>10 cm/s) and cognition (>2 points decline in Montreal Cognitive Assessment score) on at least two consecutive 6-monthly assessments. The participants’ decliner status was evaluated 3 years after the blood sample was collected. Pair-wise comparison of detected compounds was completed using principal components and hierarchical clustering analyses.
Results:
Analyses did not detect any cluster separation in untargeted metabolomes across baseline groups. However, follow-up analyses of specific molecules detected 4 compounds (17-Hydroxy-12-(hydroxymethyl)-10-oxo-8 oxapentacyclomethyl hexopyranoside, Fleroxacin, Oleic acid, and 5xi-11,12-Dihydroxyabieta-8(14),9(11),12-trien-20-oic acid) were at significantly higher concentration among the dual-decliners compared to non-decliners. The pure cognitive decliner group had significantly lower concentration of six compounds (1,3-nonanediol acetate, 4-(2-carboxyethyl)-2-methoxyphenyl beta-D-glucopyranosiduronic acid, oleic acid, 2E-3-[4-(sulfo-oxy)phenyl] acrylic acid, palmitelaidic acid, and myristoleic acid) compared to the non-decliner group.
Conclusions:
The unique metabolomics profile of dual-decliners warrants follow-up metabolomics analysis. Results may point to modifiable pathways.
INTRODUCTION
Alzheimer’s disease and related dementias (ADRD) affect 1 in 10 older adults and are responsible for discomfort, disability, and health care utilization projected to become even more prevalent in the coming years. Currently, there is no cure for dementia suggesting a multifactorial therapeutic and preventive approach [1]. Mechanisms such as amyloid-β protein precursor metabolism, phosphorylation of tau protein, mitochondrial function, inflammatory reaction, regulation of membrane lipids, and neurotransmitter pathways can contribute to ADRD pathology [2–6]. Epidemiological evidence suggests that older adults with metabolic comorbidities such as hypertension, diabetes mellitus, and dyslipidemia are 4-times more likely to develop dementia [7]. Therefore, novel mechanistic insights from systems biology and the discovery of metabolic states associated with cognitive and motor decline and dementia may help in early detection of ADRD risk and explain how lifestyle interventions work to delay the onset of the condition.
We have previously shown that older adults who exhibit a dual-decline in cognition and gait speed (a novel phenotype) are 3-fold more likely to develop dementia [8], later replicated in a worldwide multi-cohort meta-analysis (N = 8,699) that showed the novel phenotype (dual-decliners) were at 6 times higher risk of dementia than non-decliners [HR = 6.28; 95% CI, 4.56–8.64]) [9].
We further reported that this novel phenotype enrolled in our ongoing Gait and Brain (G&B) study (N = 144) (https://clinicaltrials.gov/ct2/show/NCT03020381) had a higher prevalence of hypertension, diabetes, and dyslipidemia [8]. A recent clinical trial identified eight metabolites (hexoses, sphingomyelin (SM) 16:1, SM 18:0, SM 18:1, phosphatidylcholine aa 32:3, lysophosphatidylcholine (LPC) 17:0, LPC 18:1, and LPC 18:2) significantly associated with slowing of gait speed independent of age and sex [10]. Interestingly, the same metabolites concentrations decrease when people get older (>60 years) (sphingomyelins and phosphatidylcholines) [11], gain weight (body mass index >30 kg/m2) (sphingomyelins and phosphatidylcholines), develop type 2 diabetes (lysophosphatidylcholine) [12], AD and mild cognitive impairment (MCI) (phosphatidylcholines) [13, 14]. There is an opportunity to improve our understanding of dementia pathophysiology by describing the metabolomics profile of older adults with a known high-risk phenotype such as dual-decline [15]. Moreover, plasma metabolomic signature is a stable indicator that is not affected by diet or therapeutic drugs and deserves study.
We hypothesized that the novel phenotype of older adults will have a unique metabolomics profile before they show signs of decline in cognition and gait speed. The purpose of this analysis was to determine if plasma metabolomics signatures can discriminate dual-decliners from the other three phenotypic groups prior to decline.
MATERIALS AND METHODS
This is a secondary analysis of our ongoing G&B cohort study. The G&B cohort included older adults aged 60 to 80 years independent of sex, gender, ethnicity, religion, and socio-economic status. Participants have been followed up bi-annually for 20 years to collect data on their cognitive status and walking speed. Dementia status is being ascertained during the bi-annual visits by the Principal Investigator clinician (MMO), blinded to gait and cognitive assessments, following Diagnostic Manual of Mental Disorders, 5th ed [16] criteria with a re-assessment diagnosis after six months for confirmation [17, 18].
The G&B study protocol allow one time blood sample collection at the baseline visit and continuous monitoring of cognition and gait speed every 6 months (https://clinicaltrials.gov/ct2/show/NCT03020381). Blood via venipuncture was collected at the baseline (when participants enrolled in the G&B study) and stored in a –80°C double-locked fridge. At the time the blood samples were collected, none of the participants had a decline in cognition and gait speed. Metabolomics analyses were performed by the Metabolomics Innovation Centre (TMIC), Montreal, Quebec. Dual-decline was operationalized 3 years after the blood samples were collected as gait speed (>10 cm/s slowing of gait velocity [19]) and cognitive decline (>2 points decline in Montreal Cognitive Assessment (MoCA) [20] score on at least two consecutive 6-monthly assessments [21]). The participants’ gait and cognition were measured at least 6 times (once every 6 months) before we identified their decliner status. To ensure that phenotype classification was stable during follow up prior to progression to dementia, we first selected gait and cognitive dual-decliners with blood samples available and with at least 3 years of follow-up (n = 19) as our exposure group of primary interest. The total sample was of 76 participants (mean age 72.5 years, 56% women). Using the G&B Cohort we nested 19 participants from each group (pure-cognitive-decline, pure-motor-decline, dual-decline, and no-decline). Their baseline blood samples were sent to TMIC to detect existing metabolomes across the unobserved groups using Liquid Chromatography Mass Spectrometry (LCMS) with good validity and reproducibility using stored human plasma [22].
The plasma samples from the participants (n = 76) were mixed with an organic solvent (acetylnitrile) that precipitates the majority of the protein compounds. We then centrifuged the sample so that we could collect the supernatant containing all low molecular weight chemical compounds (commonly known as metabolites). Then we injected the supernatant into LCMS that separates all the compounds based on chemical features. The LCMS detects the mass peak of the compounds based on their retention time alignment [23]. The peak area gives an indication of the concentration of the particular compound in the plasma sample that can act as a proxy to the concentration of the compound in the plasma [23]. In targeted metabolomics, the concentration of the compound can be calculated precisely as the process uses a standard chemical with known molecular weight [24]. We performed an untargeted metabolomics to detect if there were any differences between the groups (i.e., non-decliners, dual-decliners, cognitive-decliners, and gait or motor-decliners) in terms of plasma metabolome concentration. Therefore, we had to rely on a proxy for the concentration of the compound in untargeted metabolomics [24]. We performed LCMS analysis for each sample using reversed phase and hydrophilic interaction chromatography in both positive and negative MS detection modes. We identified compounds with Compound Discoverer version: 3.2.0.421 using mzCloud (ddMS2) and ChemSpider (formula or exact mass). We performed pair-wise comparison of detected compounds with descriptive statistics.
100 microliter (μl) aliquots of plasma samples were added to 400μl acetonitrile (MeCN). The samples were vortexed and centrifuged (21000× g) for 1 min at room temperature (23°C). Supernatants were transferred to the Eppendorf tubes and stored at –80°C until subsequent analysis. Pooled samples for each group were made by combining 10μl of each sample of the same group. For the analysis, samples were thawed at room temperature for 30 min and 100μl aliquots were transferred to the sample vials. LCMS analyses were performed using Vanquish Ultra-high-Performance Liquid Chromatography with 0–100% 10-min gradient (0.1% formic acid (FA) - 0.1% FA/MeCN) at 200μl/min flow rate on Phenomenex Luna Omega 3μm Polar C18 100A 50×2.1 mm (Reverse Phase [RP]-LCMS) or 100-0% 10 min gradient (MeCN - 10 mM ammonium acetate, 10 mM ammonium hydroxide) on Phenomenex Luna 3 um NH2 100A 100×2 mm (Hydrophilic Interaction [HILIC]-LCMS). Columns were thermostated at 30°C. 10μl injection volumes were used for each run. Mass spectra were acquired using Thermo Orbitrap QE+ spectrometer in positive and negative modes in separate runs. Data for each LC/acquisition type were analyzed using Compound Discoverer (Thermo).
Statistical analysis
A pair-wise comparison among the groups to detect metabolomes with Compound Discoverer, version: 3.2.0.421 (https://assets.thermofisher.com/TFS-Assets/CMD/manuals/man-xcali-98277-compound-discoverer-gc-studies-manxcali98277-en.pdf) was conducted. Compound Discoverer was programmed to compare the groups based on the ratios of abundancies of the detected compounds (Fig. 1), principal component analysis and hierarchical cluster analyses. A descriptive statistical analysis was performed using the results from the Compound Discoverer to analyze the detected compounds to understand the metabolomics profile of the 4 groups.

Volcano plot comparing dual decliners and no-decliners, the colored box area indicates statistically significant differences in concentrations of compounds. The X-axis indicates 2-fold log ratio of a compound concentration (or a proxy to 2-fold higher/lower concentration where positive scale indicates higher and the negative scale indicates lower concentration). The Y-axis indicates statistical significance of concentrations for compounds.
RESULTS
Table 1 shows the baseline characteristics of the participants. For better illustration, we presented their data classifying into 4 phenotypic groups.
Baseline characteristics of participants stratified by phenotypic groups
Table 2 shows the unobserved participants who progressed to subjective cognitive impairment, MCI, and dementia (mutually exclusive) during the three years of follow-up.
Progression to cognitive decline in 3 years stratified by phenotypic groups
Among these four phenotypic groups, an untargeted plasma metabolomics analyses identified 12,660 compounds. However, most of them did not have information with complete chemical formula (Supplementary Material 1). We putatively assumed 4,724 compounds as accurate based on their complete chemical formula. The compounds were detected using four types of analysis: RP-LCMS (+), RP-LCMS (–), HILIC-LCMS (+), and HILIC-LCMS (–) (Supplementary Material 1).
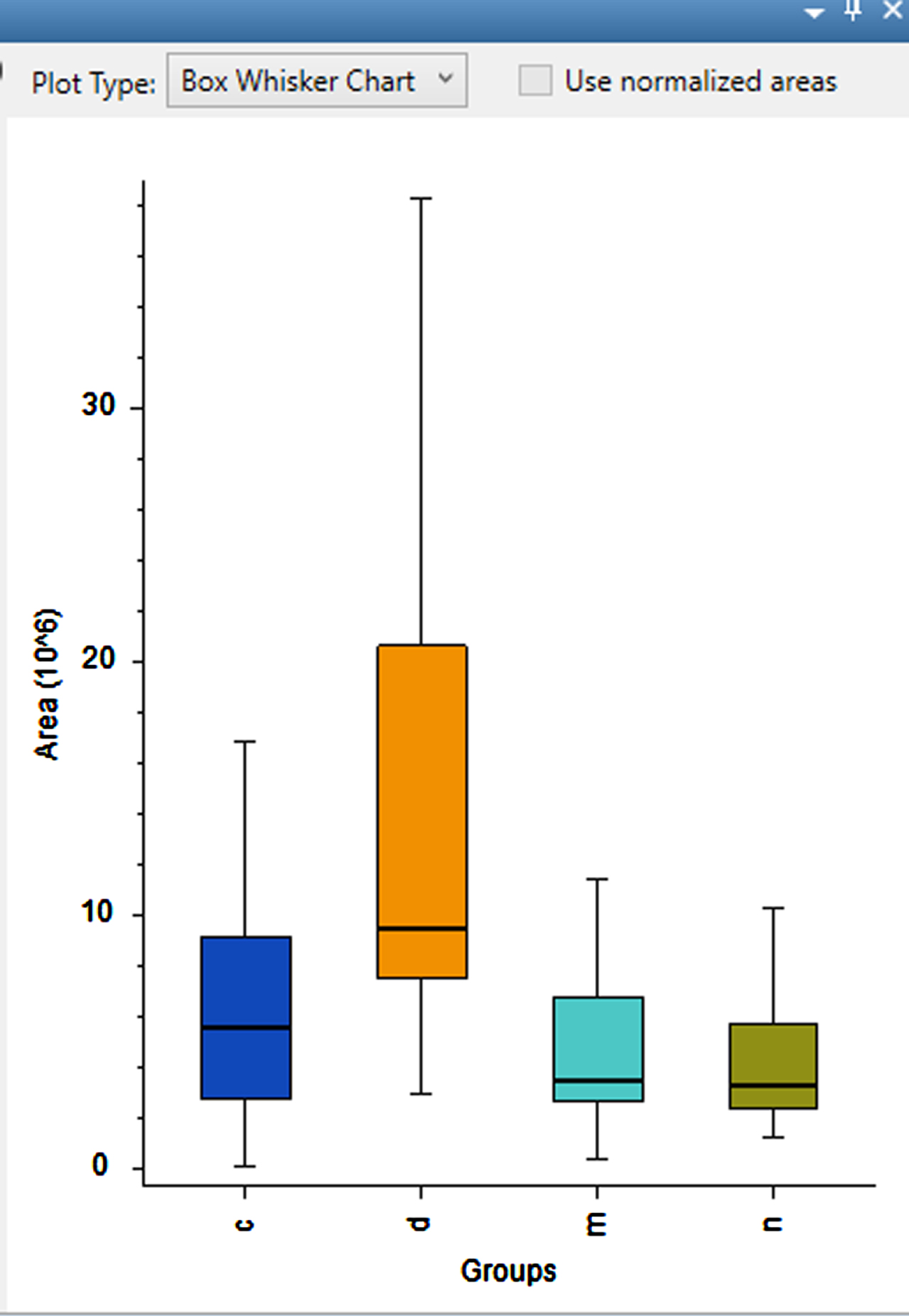
We compared the groups based on the ratios of abundancies of the identified compounds and differential analyses. Principal components analysis and hierarchical clustering analysis did not detect any cluster separation in metabolomes across groups. However, four compounds (17-Hydroxy-12-(hydroxymethyl)-10-oxo-8 oxapentacyclomethyl hexopyranoside, Fleroxacin, Oleic acid, and 5xi-11,12-Dihydroxyabieta-8(14),9(11),12-trien-20-oic acid) were present in significantly higher concentration among dual-decliners compared with non-decliners (p < 0.05) (Figs. 1–5, Table 3).

Serum concentration of a compound of interest (17-Hydroxy-12-(hydroxymethyl)-10-oxo-8 oxapentacyclomethyl hexopyranoside) in different groups (c, cognitive decliners; d, dual decliners; m, motor decliners; n, non-decliners).
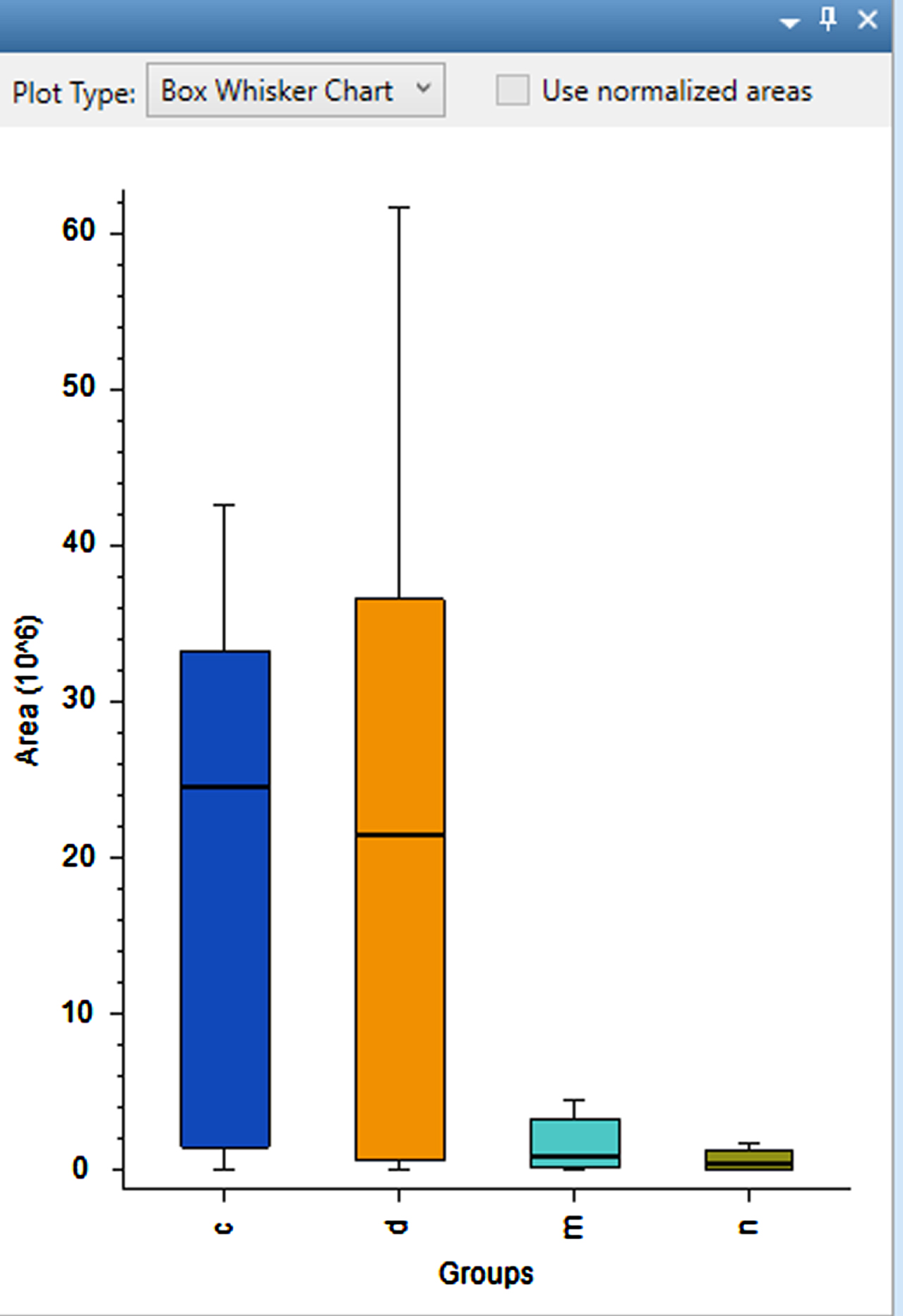
Serum concentration of a compound of interest (Fleroxacin) in different groups (c, cognitive decliners; d, dual decliners; m, motor decliners; n, non-decliners).
Serum concentration of the compound of interest (5xi)-11,12-Dihydroxyabieta-8(14),9(11),12-trien-20-oic acid) in different groups (c, cognitive decliners; d, dual decliners; m, motor decliners; n, non-decliners).
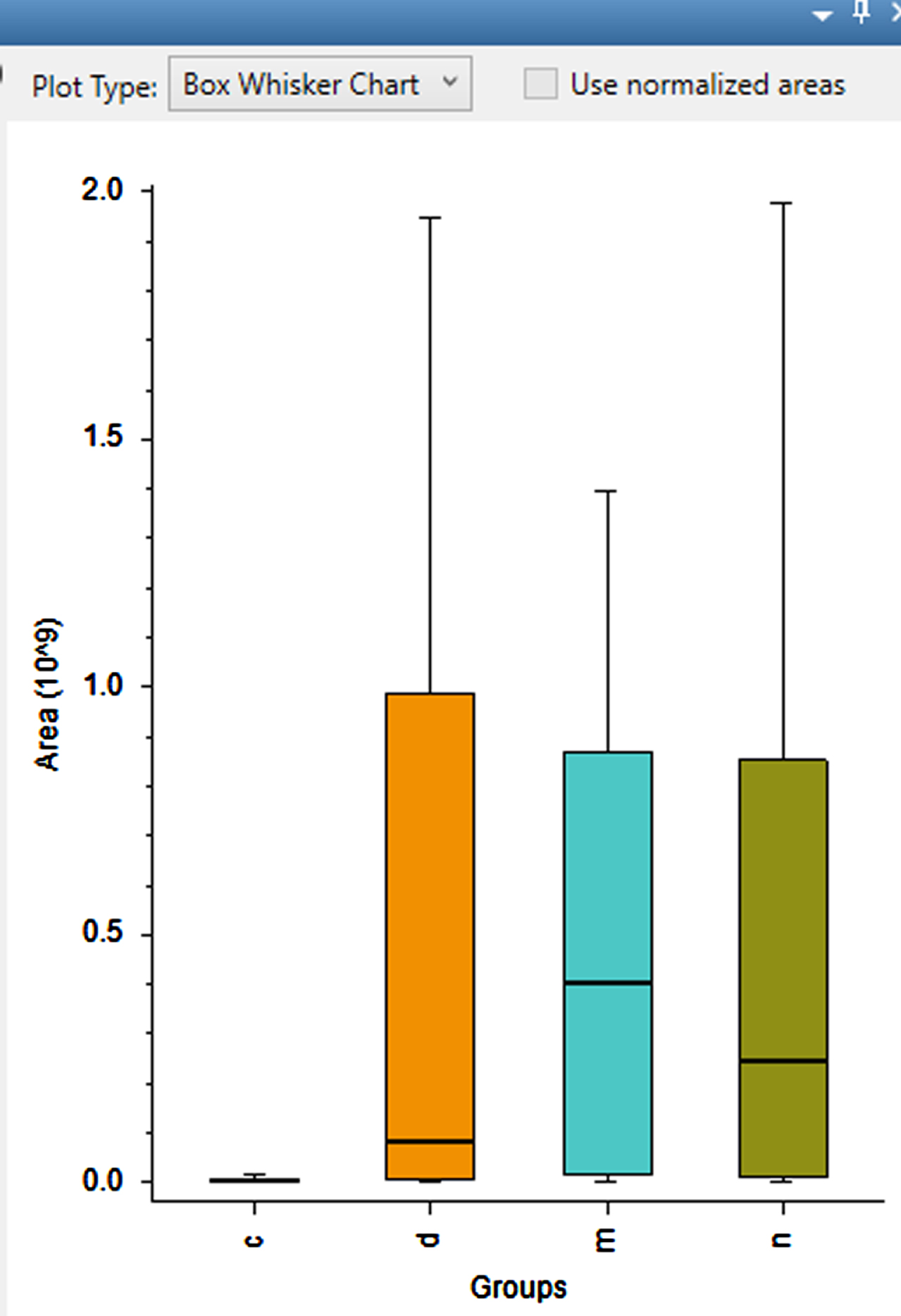
Serum concentration of a compound of interest (Oleic acid) in different groups (c, cognitive decliners; d, dual decliners; m, motor decliners; n, non-decliners).
Ratio of compounds in higher concentration among the different cohorts
CD, Cognitively Declined participants; DD, Dual Declined participants; MD, Motor Declined participants; ND, No Decline participants.
The pure cognitive decliner group had significantly lower concentration (p < 0.05) of six compounds (1,3-nonanediol acetate, 4-(2-carboxyethyl)-2-methoxyphenyl beta-D-glucopyranosiduronic acid, oleic acid, 2E-3-[4-(sulfo-oxy) phenyl] acrylic acid, palmitelaidic acid, and myristoleic acid) compared to the non-decliner group (Table 4). No published source exists on presence of the identified metabolites in people exhibiting cognitive decline.
Ratio of compounds in lower concentration among the different cohorts
CD, Cognitively Declined participants; DD, Dual Declined participants; MD, Motor Declined participants; ND, No Decline participants.
DISCUSSION
Although no cluster separation in metabolomes across baseline groups were detected, a descriptive statistical analysis of the detected compounds to understand the metabolomics profile of the cohort after stratifying them in 4 phenotypic groups based on their cognitive and motor function status 3 years later, revealed 4 compounds in significantly higher concentration among dual-decliners compared with non-decliners. Among these 4 compounds, Fleroxacin is an ingredient used in many bactericidal drugs [25] and 5xi-11, 12-Dihydroxyabieta-8(14),9(11),12-trien-20-oic acid is often used in deodorants and cosmetics [26]. This may be because dual decliners were on antibiotics or using cosmetics on their skin at the time their blood was collected. However, further research into the association between those compounds and cognitive and motor decline can better answer if that assumption is valid or not. Interestingly, Fleroxacin was also found significantly higher in concentration among the cognitive-decliner group compared to non-decliner and motor-decliners. The same compound was in significantly higher concentration among the motor-decliners compared to non-decliners. Fleroxacin is a broad-spectrum fluoroquinolone antibacterial agent used against most Gram-negative species (particularly Enterobacteriaceae) and a number of Gram-positive organisms, including methicillin-sensitive staphylococci to treat uncomplicated urinary tract infections, gonorrhea, chancroid, nonpneumococcal lower respiratory tract and skin and soft tissue infections and typhoid fever, bacterial enteritis, and traveler’s diarrhea [25].
The compound, 17-hydroxy-12-(hydroxymethyl)-10-oxo-8 oxapentacyclomethyl hexopyranoside, is a membrane lipid and oleic acid is a C18 fatty acid [27, 28]. Endothelial cells produce adhesion molecules such as 17-hydroxy-12-(hydroxymethyl)-10-oxo-8 oxapentacyclomethyl hexopyranoside after being stimulated with various inflammatory cytokines that promote production of tumor necrosis factor-alpha (TNF-α), eventually playing an important role in atherogenesis leading to various cardiovascular conditions such as hypertension and dyslipidemia [27, 28]. Oleic acid is the preferred substrate for acyl-CoA: cholesterol acyltransferase and diacylglycerol acyltransferase, the enzymes responsible for cholesteryl ester and triglycerol synthesis, respectively [29]. Excessive amounts of such compound may indicate an association with several pathological conditions (e.g., obesity, diabetes mellitus, and steato-hepatitis) [29]. Therefore, presence of such compounds in higher concentration in our novel phenotype (dual decliners) may open possibilities to identify possible biomarker to early detect dual decliners.
The compounds we identified (17-hydroxy-12-(hydroxymethyl)-10-oxo-8 oxapentacyclomethyl hexopyranoside and oleic acid) were also identified in studies conducting untargeted metabolomics in plasma samples to discover the early diagnostic biomarkers of AD [30–35] confirming our observation. However, a potential biomarker (ornithine) identified in plasma samples of people diagnosed as MCI, and AD patients [33, 36] were absent in our sample. We suspect analysis methods used (gas-chromatography coupled with mass spectrometry in precipitated protein derived from plasma [33] and a capillary electrophoresis electrospray ionization time-of-flight mass spectrometry [36]), ethnicity (Spain [33], Japan [36]), and health status (none of the studies reported dual-decliners) may have influenced the metabolomes identified in those studies.
Among the compounds at a significantly lower concentration in pure cognitive decliner group, 1,3-nonanediol acetate and 4-(2-Carboxyethyl)-2-methoxyphenyl beta-D-glucopyranosiduronic acid is typically used in alcohol swabs, perfumes, food additives [30, 31]. Palmitelaidic acid, myristoleic acid, and oleic acid, on the other hand, are dietary fatty acids [31] suggesting that the cognitive decliner group may have had a low dietary fatty acid. A significantly lower concentration of this compound in pure cognitive decliner needs further evaluation in future research on this topic.
A limitation of the study is that blood samples were collected at the baseline and our participants were not identified as dual-decliners, cognitive-decliners, or motor-decliners at the time of blood sample collection. The finding that dual-decliners at baseline presenting four compounds at higher concentrations at the baseline when compared with non-decliners supports the importance of follow up metabolomics analyses in these groups.
The finding that dual-decliners present similar metabolomics profiles but with four compounds at higher concentrations when compared with non-decliners supports the importance of elucidating changes in these compounds with subsequent metabolomics analyses over waves of follow up in these groups and replication in other samples. Although the blood sample is collected before the decliners are detected, this may inform the early-stage alterations of the metabolites predating the onset of functional decline and could be the value of the metabolites to inform potential biomarkers to track or for early intervention.
Footnotes
ACKNOWLEDGMENTS
We acknowledge The Metabolomics Innovation Centre (https://metabolomicscentre.ca/?utm_source=foodb&utm_medium=banner&utm_campaign=tmic-campaign) for their contribution in data analysis.
FUNDING
The salary support of the corresponding author (MS) was funded by Parkwood Institute Research-Specific Endowments (PIRSE) fellowships award.
CONFLICT OF INTEREST
Munira Sultana and Manuel Montero-Odasso are Editorial Board Members of this journal but were not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.