
Abstract
To investigate an association of serum liver enzymes with Alzheimer’s disease (AD) diagnosis and cognitive performance, we performed logistic and linear regression analyses in 781 patients with AD and 405 cognitively normal subjects. We found that alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels had significant positive associations with cognitive performance and were significantly decreased in AD patients. The alkaline phosphatase level and AST to ALT ratio were significantly negatively associated with cognitive performance and were significantly increased in AD patients. This suggests that these liver enzymes might be implicated in the pathogenesis of AD.
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia, accounting for an estimated 60% to 80% of cases [1]. The prevalence and the average annual incidence were reported to be 5.0 and 0.4% in people aged 65–74, 13.1 and 3.2% in people aged 75–84, 33.2 and 7.6% in people aged 85 and older, respectively, in the United States [1]. AD is characterized by the formation of extracellular amyloid-β (Aβ) plaques and intracellular neurofibrillary tangles [2]. Aβ homeostasis reflects the complex interaction between the brain and periphery, including the liver [3]. Nho et al. found that a higher aspartate aminotransferase (AST) to alanine aminotransferase (ALT) ratio and lower ALT levels in blood were associated with AD diagnosis, poor cognitive performance, and biomarkers of Aβ [4], but these findings have not been validated in independent cohorts. In addition, studies on the association of blood alkaline phosphatase (ALP) levels with AD have yielded conflicting results [5, 6]. In this study, we investigated whether there was a significant association of serum liver enzymes, including AST, ALT, the AST to ALT ratio, ALP and albumin levels, with AD diagnosis and cognitive performance.
METHODS
We retrospectively performed a case-control study of a consecutive series of patients aged 60 years and older who visited the Seoul National University Bundang Hospital from January 2013 to October 2020. We included patients with AD who met the criteria for probable AD dementia outlined in the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups [7] and cognitively normal (CN) subjects. Participants whose z-scores for all cognitive domains, including language, memory, visuospatial and executive function, were higher than –1.0 standard deviations of the age-, sex-, and education-adjusted norms were diagnosed as cognitively normal. Participants who did not have liver function test data within one year from the date of initial diagnosis were excluded. Furthermore, we excluded participants with other medical problems, such as hepatocellular carcinoma and gallbladder cancer, which could lead to significant impairment in liver function. Patients were also excluded if they had outliers of liver function parameters that were determined as 3 times the interquartile ranges. Although we retrospectively analyzed patients with AD and CN subjects, the diagnosis was made during the outpatient clinic visit.
All participants underwent a comprehensive neuropsychological assessment including assessments of four cognitive domains: language, memory, visuospatial, and executive function. Subjects’ raw scores on individual cognitive tests were converted to a standardized z-score based on age-, sex-, and education-adjusted norms [8]. Then, we determined the z-score for each cognitive domain from the z-scores for individual tests: the Korean Boston Naming Test [9] for language; the Seoul Verbal Learning Test 20-min delayed recall test for memory; the Rey Complex Figure Test [10] for visuospatial function; and the mean of the z-scores of the Controlled Oral Word Association Test [11] and the Korean Color–Word Stroop test [12] for executive function.
To measure serum levels of AST (normal range <40 U/L [13]), ALT (normal range <40 U/L [13]), total bilirubin (normal range 0.2∼1.0 mg/dL [14]), alkaline phosphatase (normal range 30∼115 U/L [15]), and albumin (normal range 3.5–5.0 g/dL [16]), venous blood samples were taken from all participants after a 12-h overnight fast. All assays were analyzed using a Beckman Coulter AU 5800 autoanalyzer in the Department of Laboratory Medicine at Seoul National University Bundang Hospital.
We compared medial temporal atrophy (MTA) on brain MRI between patients with AD and CN subjects, and MTA was rated by neurologists who were blinded to the clinical information [17]. MTA was individually assessed in the left and right hemispheres using a 5-point scale (0 = absent, 1 = minimal, 2 = mild, 3 = moderate, and 4 = severe). The mean MTA scores of the left and right hemispheres were calculated for each participant. Linear regression analysis was performed to investigate the association between each liver enzyme and domain-specific cognitive performance in all participants using two models. Covariates in model 1 included age, sex, education, hypertension, diabetes mellitus and dyslipidemia, whereas covariates in model 2 included age, sex, education, body mass index (BMI), APOE ɛ4 carrier status, hypertension, diabetes mellitus, and dyslipidemia. We also performed an exact matching analysis [18] to balance covariates including age and sex between the two diagnostic groups, followed by logistic regression analysis to estimate the association between diagnostic status and each liver enzyme. The R package MatchIt was used for the exact matching analysis [18]. The exact matching analysis can improve parametric statistical models and reduce model dependence by preprocessing data with nonparametric methods [18]. In the logistic regression analysis, covariates in model 1 included education, hypertension, diabetes mellitus, and dyslipidemia, whereas covariates in model 2 included education, BMI, APOE ɛ4 carrier status, hypertension, diabetes mellitus, and dyslipidemia. We performed all analyses using R software, version 4.0.3. The false discovery rate (FDR) [19] correction was used to adjust for multiple testing.
The protocol for the study has been approved by Institutional Review Board of the Seoul National University Bundang Hospital and conforms to the provisions of the Declaration of Helsinki.
RESULTS
We identified 781 AD patients and 405 CN subjects (see Fig. 1 for our study design). The demographic information of our study subjects is depicted in Table 1. Table 2 shows the results of the association of liver enzymes with diagnostic groups and cognition. After adjustment for multiple comparisons, ALT levels had significant positive associations with all cognitive domains, and AST levels had significant positive associations with language, memory and executive function. Furthermore, ALP levels were significantly negatively associated with memory and visuospatial function and the AST to ALT ratio was significantly negatively associated with memory, visuospatial and executive function. Total bilirubin levels had a significant positive association with visuospatial function, and albumin levels had a significant positive association with memory, visuospatial and executive function. In the matched AD and CN subjects, AST (odds ratio (OR) 0.949, 95% confidence interval (CI) 0.914–0.983, p value 0.009) and ALT levels (OR 0.953, 95% CI 0.925–0.981, p value 0.004) were significantly decreased in AD patients, while the AST to ALT ratio (OR 1.966, 95% CI 1.096–3.617, p value 0.039) and ALP levels (OR 1.020, 95% CI 1.008–1.033, p value 0.004) were significantly increased in AD patients. Neither the total bilirubin levels nor the albumin levels were significantly altered in AD patients.
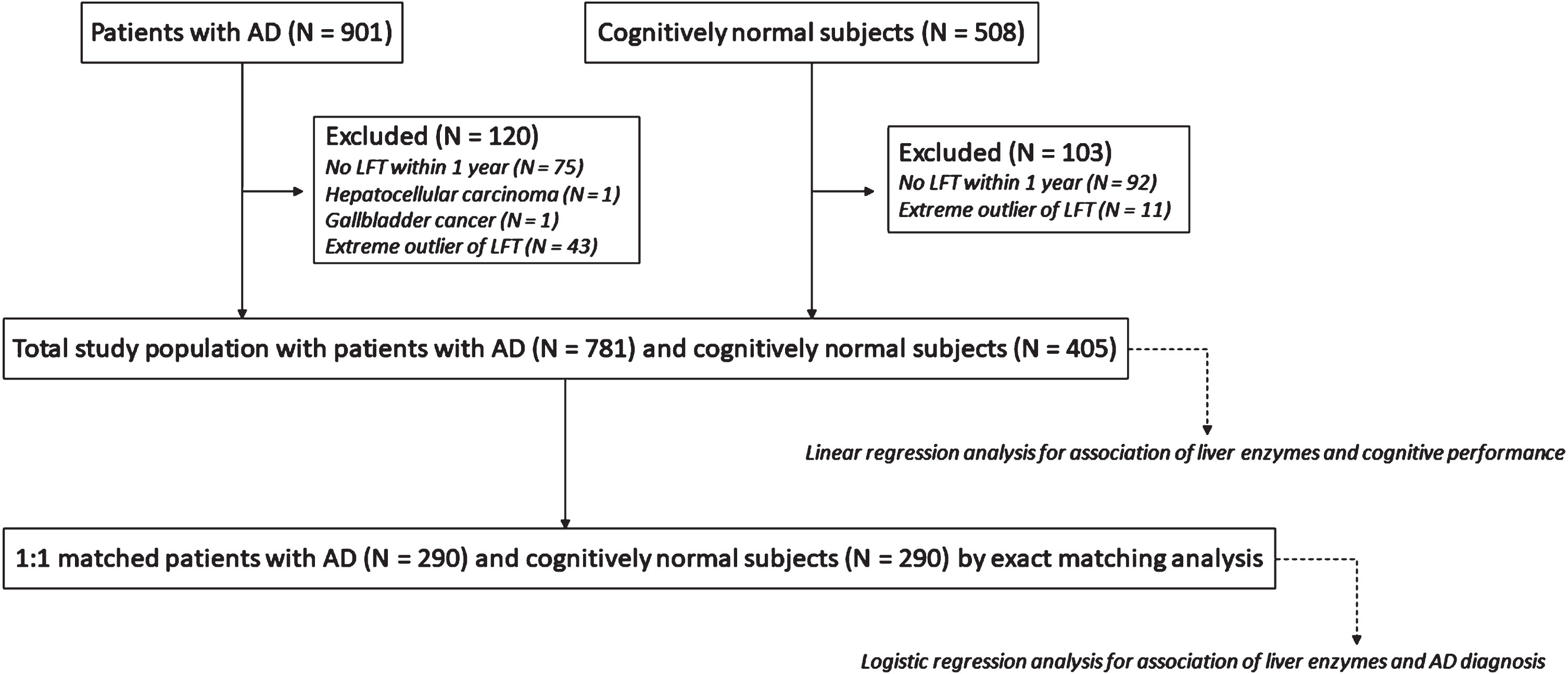
Flow chart showing our study design. AD, Alzheimer’s disease; LFTs, liver function tests.
Demographic information and laboratory results
Values are n (%), unless indicated otherwise. aThe Mann-Whitney U test or chi-square test was used to determine the P value for comparisons between groups, as appropriate. bThere were 267 missing values among 405 CN subjects and 293 missing values among 781 AD patients before exact matching. There were 186 missing values among 290 CN subjects and 93 missing values among 290 AD patients after exact matching. cThere were 103 missing values among 405 CN subjects and 209 missing values among 781 AD patients before exact matching. There were 72 missing values among 290 CN subjects and 85 missing values among 290 AD patients after exact matching. dThere were 98 missing values among 405 CN subjects and 14 missing values among 781 AD patients before exact matching. There were 66 missing values among 290 CN subjects and 3 missing values among 290 AD patients after exact matching. AD, Alzheimer’s disease; ALT, alanine aminotransferase; ALP, alkaline phosphatase; APOE, apolipoprotein E; AST, aspartate aminotransferase; BMI, body mass index; CN, cognitively normal; IHD, ischemic heart disease; IQR, interquartile range; MMSE, Mini-Mental State Examination; MTA, medial temporal lobe atrophy.
Regression results for the association of liver enzymes with diagnostic group differences and cognition
aAdjusted p value for FDR to correct for 6 tests of associations between liver enzymes and diagnostic status. bAdjusted p value for FDR to correct for 24 tests of associations between liver enzymes and 4 cognitive domains. cLogistic regression analysis was conducted to assess the association of liver enzymes with diagnostic status after adjusting for education, hypertension, diabetes mellitus and dyslipidemia in 290 patients with AD and 290 exactly matched CN subjects. dLogistic regression analysis was conducted to assess the association of liver enzymes with diagnostic status after adjusting for education, hypertension, diabetes mellitus, dyslipidemia, BMI and APOE ɛ4 carrier status. Among 290 patients with AD and 290 exact matched CN subjects, 157 participants were excluded from the analysis due to missing BMI values or APOE ɛ4 carrier status. eLinear regression analysis was conducted to assess the relationship of liver enzymes with cognitive performance after adjusting for age, sex, education, hypertension, diabetes mellitus and dyslipidemia in 781 patients with AD and 405 CN subjects. fLinear regression analysis was conducted to assess the relationship of liver enzymes with cognitive performance after adjusting for age, sex, education, BMI, APOE ɛ4 carrier status, hypertension, diabetes mellitus and dyslipidemia. Among the 781 patients with AD and 405 CN subjects, 439 participants were excluded from the analysis due to missing BMI values or APOE ɛ4 carrier status. AD, Alzheimer’s disease; ALP, alkaline phosphatase; ALT, alanine aminotransferase; APOE, apolipoprotein E; AST, aspartate aminotransferase; BMI, body mass index; CI, confidence interval; CN, cognitively normal; FDR, false discovery rate; IQR, interquartile range; OR, odds ratio; SE, standard error.
DISCUSSION
In general, an increase in serum AST and ALT has clinical significance because injury to hepatocyte membranes leads to the release of AST and ALT into the blood [20]. Although our results demonstrated that serum AST and ALT levels were significantly lower within their normal ranges in AD patients, which had been observed in a previous study [4], the exact meaning of these results remains unknown. Reduced ALT levels might be associated with decreased hepatic degradation of Aβ because the total hepatocyte number is decreased during hepatic aging processes [21]. Impaired hepatic Aβ degradation could be one of the factors that contributes to increased brain Aβ accumulation and AD [22]. Our results also reproduced the findings of a positive association of the AST to ALT ratio with AD diagnosis and poor cognitive performance, as reported in a previous study [4]. In our study, serum ALP levels were significantly higher in AD patients within their normal range, as demonstrated in a previous study [6]. Although tissue-nonspecific ALP is known to facilitate the aggregation of intracellular tau and directly damage neurons [2], the exact role of ALP in the pathogenesis of AD remains unknown.
Interestingly, silymarin, which is extracted from the seeds of Silybum marianum plants and frequently administered for liver disorders, also has therapeutic potential for AD [23]. The efficacy of silymarin in both diseases suggests that AD and liver disorders may share a common mechanism of pathogenesis.
A limitation of our study is that we could not assess amyloid or tau biomarkers to confirm AD pathology. The question of whether altered liver enzymes are related to amyloid pathology could be answered by association analysis between live enzymes and amyloid levels.
In summary, lower AST and ALT and higher ALP within normal ranges were associated with AD diagnosis and poor cognitive performance. This suggests that these liver enzymes might be implicated in the pathogenesis of AD.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the National Research Foundation of Korea grant funded by the Korean government (Ministry of Science and ICT) (No. 2020R1C1C1013718). We thank Jimin Yang and Min Jae Baek of Seoul National University Bundang Hospital for help in processing the data and Medical Research Collaborating Center of Seoul National University Bundang Hospital for providing statistical assistance.