
Abstract
Background:
Obstructive sleep apnea (OSA) is a multi-component disorder, which has many comorbidities, including cognitive impairment. Although its potential risk factors were unknown, they could affect the patient’s quality of life and long-term prognosis.
Objective:
The purpose of this study was to investigate the application of urinary Alzheimer’s disease-associated neurofilament protein (AD7c-NTP) levels in the assessment of cognitive impairment in OSA patients, and to analyze the predictive value of potential high-risk factors on cognitive impairment in OSA patients.
Methods:
138 young and middle-aged adults were recruited and underwent overnight polysomnographic recording, Montreal Cognitive Assessment (MoCA), and urinary AD7c-NTP test. AD7c-NTP and other factors were further applied as biomarkers to develop a cognition risk prediction model.
Results:
Compared with the control, OSA patients showed significantly lower MoCA scores and higher urinary AD7c-NTP concentrations, while the severe OSA group appeared more significant. The urinary AD7c-NTP level of the OSA cognitive impairment group was higher than that of the non-cognitive impairment group. The results of regression analysis showed that urinary AD7c-NTP level was an independent predictor of cognitive impairment in OSA patients. Based on urinary AD7c-NTP levels and other selected factors, a multimodal prediction model for assessing the risk of cognitive impairment in OSA patients was initially established.
Conclusion:
The increased urinary AD7c-NTP level could be used as a relevant peripheral biomarker of cognitive impairment in OSA patients. A model using urinary AD7c-NTP combined with other factors was developed and could accurately assess the cognition risk of OSA patients.
Keywords
INTRODUCTION
Obstructive sleep apnea (OSA) is a highly prevalent sleep disordered breathing (SDB) characterized by apnea or hypopnea during sleep which results in intermittent hypoxemia and consequent systemic inflammation. Therefore, OSA usually accompanies multi-systemic complications, such as cardiovascular and cerebrovascular diseases [1], metabolic diseases [2], chronic kidney diseases [3], and so on. Cognitive impairment, in particular, is one such important relevant comorbidity which has received widespread attention in recent years [4, 5]. OSA is considered to be an independent risk factor for cognitive dysfunction, while cognitive impairment affects the quality of life and long-term prognosis of patients with OSA [5]. What makes sense is that early prediction and effective intervention of cognitive comorbidities of OSA could delay cognitive impairment, and are regarded crucial for improving the quality of life and prognosis of patients [6]. However, up to now, the relevant factors are seemed to be complex, and the potential mechanisms involved in the decline of cognition are not fully understood. Previous studies have reported that OSA is associated with poorer cognitive performance or higher risk of mild cognitive impairment (MCI) and even dementia [7]. Compared with healthy subjects, OSA patients have poorer performance in cognitive domains such as attention [8, 9], memory [8, 10–13], executive function [8, 15], and reaction time and vigilance [16, 17]. OSA cognitive comorbidities are thought to be related to apnea hypopnea index (AHI) [17], nocturnal hypoxemia [18–20], excessive daytime sleepiness (EDS) [18], or sleep fragmentation [21], but there is no consensus among professionals.
Alzheimer-associated neural thread protein (AD7c-NTP), an identified biomarker for Alzheimer’s disease (AD), has been detected elevated in cortical neurons, brain tissue extracts, cerebrospinal fluid (CSF), and urine in the early stages of cognitive impairment [22]. AD7c-NTP levels were reported to be relatively stable and specific in a body, and were not affected by demographic factors such as education and body mass index (BMI), common chronic diseases, or subjective cognitive decline [23, 24]. Notably, high sensitivity and specificity of urinary AD7c-NTP level as AD and MCI biomarkers were comparable to those of CSF AD7c-NTP [25], providing a new idea for non-invasive screening of cognitive impairment. Urinary AD7c-NTP ELISA kit has been developed for detecting early AD/MCI and has been used clinically [26]. It is known that AD7c-NTP level is a non-invasive and handy biomarker for MCI/AD, yet there is a lack of evidence or research supporting the use of AD7c-NTP biomarkers to assess cognitive performance in OSA patients.
In this research, we evaluated the cognitive performance and urinary AD7c-NTP levels in OSA patients at different stages, as well as the associations between the cognitive states, OSA clinical characteristics, polysomnography (PSG) parameter values and urinary AD7c-NTP levels. Furthermore, we proposed a new cognition risk prediction platform named PredCI_OSA for OSA patients based on urinary AD7c-NTP biomarkers while integrated more comprehensive individual features.
METHODS
Subjects
The participants who had undergone nocturnal PSG monitoring in the sleep room of the Department of Pulmonary and Critical Care Medicine of Xuanwu Hospital were carefully selected. An abnormal breathing event was defined according to the common clinical criteria of either a complete cessation of airflow lasting 10 s (apnea) or a discernible reduction in nasal pressure signal accompanied by a decrease of 4% in oxyhemoglobin saturation or an arousal (hypopnea). Then the AHI was calculated by the average number of episodes of apnea and hypopnea per hour of sleep. The OSA group enrolled the subjects who met the diagnostic criteria of an AHI≥5 events/h, and an AHI≥30 events/h was considered as severe OSA. The control group recruited simple-snoring subjects whose AHI < 5 events/h and demographic data basically matched during the same period.
The exclusion criteria were: 1) History of severe infection, trauma or surgery in the previous 4 weeks; 2) Exacerbation of respiratory symptoms in the previous 4 weeks (dyspnea, change in sputum volume or color, need of antibiotic treatment, or hospitalization due to respiratory disease); 3) Prior or current therapy of CPAP, or received oxygen therapy within 4 weeks; 4) Combined with asthma, chronic obstructive pulmonary disease, or serious medical disorders, particularly unstable medical disorders (e.g., malignant diseases, unstable cardiac disorders, uncontrolled hyperthyroidism or hypothyroidism, etc.); 5) History of epilepsy, encephalitis, serious craniocerebral injury or brain tumor; 6) History of mental disorders (depression, anxiety, schizophrenia, etc.), and long-term use of sedative-hypnotic medication (i.e., benzodiazepines, benzodiazepine receptor agonists, tricyclic antidepressants, antipsychotics, etc.); 7) Dementia had been clearly diagnosed previously, and any cognitively impaired patient with significant functional impact; and 8) Age < 18 or > 90 years old.
In view of the fact that most of the hospital visits during the study period were young and middle-aged, we further excluded a total of 4 elderly patients over 65 years old. In the end, 138 young and middle-aged adults, including 50 mild-to-moderate OSA patients, 56 severe OSA patients, and 32 control subjects, were recruited in this study.
This study was approved by the Ethical committee of Xuanwu Hospital, Capital Medical University, Beijing, China, approval No. [2021]165.
Overnight polysomnographic recording
The participants were required to undergo PSG overnight in the sleep monitoring room of the Department of Pulmonary and Critical Care Medicine, Xuanwu Hospital, Capital Medical University, using the professional monitoring equipment produced by Compumedics in Australia. Under the supervision of a professional sleep technician, PSG signals were recorded automatically by the PSG system, including electroencephalogram, electrocardiogram, electrooculogram, chin electromyography, nasal airflow, respiratory effort, snoring, breathing movements of the chest and abdominal wall, oxygen saturation (SaO2), and body position, etc. On the following day, the sleep data were recorded on a computer by the sleep technician and automatically analyzed by the system for sleep apnea events. Then the analyzed data were recorded, including AHI, longest apnea time (LAT), lowest arterial oxygen saturation (LSaO2), percentage of sleep time when oxygen saturation lower than 90% (SLT90%), oxygen desaturation index (ODI), and percentage of time of non-rapid eye movement (NREM) stages I, II, and III, and rapid eye movement (REM) in the total sleep time (NREM I%, II%, III% and REM%). All the monitoring results were reviewed by professional sleep physicians.
Assessment of cognitive function
The Montreal Cognitive Assessment (MoCA) [27] was performed to evaluate the cognitive abilities of each subject. The MoCA test covered 7 cognitive domains, namely Visuospatial and Executive function, Naming, Attention, Language, Delayed Recall, Abstraction, and orientation, with a total score of 30 points [27]. The subject with education period limited to 12 years (≤12 y) would add one point to the final MoCA score to correct the deviation of education. The final adjusted MoCA score less than 26 points indicated cognitive impairment. The OSA group was then divided into two groups for further analysis according to the adjusted MoCA score: 34 cases in the OSA group with cognitive impairment (adj.MoCA<26 points) and 72 cases in the OSA group without cognitive impairment (adj.MoCA≥26 points).
Urinary AD7c-NTP laboratory measurements
The level of urinary AD7c-NTP were detected by an enzyme-linked immunosorbent assay (ELISA) kit (Anqun Biological Technology Co. Ltd. Shenzhen, China). Clean midstream morning urine samples provided by the participants were transported in Eppendorf tubes with boric acid (2 g/L) as a preservative. The samples were centrifuged and stored at 4°C immediately [28]. The operation was carried out according to the kit operating instructions: after the kit was equilibrated to room temperature (20–25°C), 100μl samples and standard were added to the corresponding reaction plate well and incubated at 37°C for 1 h, then washed with washing buffer (phosphate-buffered saline, PBS) five times, adding100μl biotinylated rabbit anti-AD7c-NTP antibody and incubated at 37°C for 30 min. Next, after five times of washing with PBS, 100μl of horseradish peroxidase labeled avidin was added and incubated for another 30 min at 37°C. Finally, the samples were again washed in PBS, and 50μl of chromogenic reagent A and B were added in turn, and then incubated at 37 °C for 15 min. The reaction was stopped by 50μl stop solution (sulfuric acid). The OD value for each well was read at a wavelength of 450 nm using a microplate reader (Multiskan Spectrum, Thermo Fisher Scientific, Waltham, MA, USA) after mixing the liquid in each well gently. The AD7c-NTP concentration was positively correlated with the absorbance value and calculated according to the standard curve of recombinant human AD7c-NTP peptides.
Statistical analysis
The categorical variables of the clinical characteristics were represented with numbers and percentage (n(%)), and compared using the Chi-squared test or the Fisher Exact Test. The continuous variables were tested for normality first and recorded as the mean±standard deviation (x±s) if the values obeyed the normal distribution. Then the One-way analysis of variance was performed to compare the distributions of them. The variables without normal distributions were represented by the median and interquartile ranges (P50 (P25, P75)), and the Kruskal-Wallis test was used for comparison among groups. The logarithms function was used to convert the nonnormally distributed continuous data into normal distribution, then the Analysis of Covariance (ANCOVA) was used to control the effects of confounding factors that might influence the dependent measure of interest. The associations between adjusted MoCA scores and urinary AD7c-NTP levels were assessed using the Spearman rank correlation. Similarly, partial correlation between adjusted MoCA scores and urinary AD7c-NTP levels given potential confounding factors was analyzed. The Logistic regression was used for regression analysis and model establishment, while the Receiver Operating Characteristic (ROC) curve, the area under the ROC curve (AUC), Sensitivity, Specificity, and the Calibration Curve were utilized to assess the predictive performance. The Sensitivity and Specificity in this study were calculated by the default threshold value from the R packages “pROC” [29]. An ROC curve is a plot of Sensitivity versus [1 –Specificity] and is generated by shifting the decision threshold. AUC gives a measure of classifier performance. The Calibration Curve uses bootstrapping to get bias-corrected estimates of predicted vs. observed values based on nonparametric smoothers, and then the mean absolute error in predictions is printed. Data analysis was carried out using R version 3.6.0, and the significance level was set as 0.05.
RESULTS
Comparison of clinical characteristics and PSG parameters among the control, the mild-to-moderate and the severe OSA groups
The control, the mild-to-moderate, and the severe groups were observed in 32 (23.2%), 50 (36.2%), and 56 (40.6%) subjects, respectively. The demographic and clinical features of all the participants in the three groups were summarized in Table 1. The three groups were statistically similar with respect to gender, years of education, deviation of nasal septum, subjective uncomfortableness, EDS, subjective cognitive decline, smoking, diabetes, arrhythmia, and histories of nasopharyngitis or amygdalitis (p≥0.05). Conversely, there were significant differences in respect to age, BMI, the girth of neck, years of snore time, drinking, and hypertension (p < 0.05), especially between the control and the OSA groups (Table 1).
The demographic and clinical characteristics in the control, the mild-to-moderate and the severe OSA groups
The demographic and clinical characteristics in the control, the mild-to-moderate and the severe OSA groups
DNS, deviation of nasal septum; SUC, subjective uncomfortableness, including disturbed sleep and morning headache; EDS, excessive daytime sleepiness; SCD, subjective cognitive decline, including subjective memory loss and lags in response.* p < 0.05 versus the control group;#p < 0.05 versus the mild-to-moderate group.a Kruskal-Wallis test;b Chi-squared test;c Fisher Exact Test.
PSG parameters were also compared among groups. The statistically significant differences were shown among the three groups in respect to sleep cycles (REM% and NREM%), AHI, LAT, LSaO2, SLT90%, and ODI (p < 0.05) (Table 2). Compared with the control group and the mild-to-moderate OSA group, the proportion of light sleep (i.e., NREM stage I% +II%), AHI, LAT, SLT90%, and ODI increased and LSaO2 decreased significantly in the severe OSA group (p < 0.05). Compared with the control group, the mild-to-moderate OSA group had higher AHI, LAT, SLT90%, ODI, and lower LSaO2, and the differences were statistically significant (p < 0.05) (Table 2).
The PSG parameters and the urinary AD7c-NTP concentration in the control, the mild-to-moderate and the severe OSA groups
TST, Total Sleep Time; REM, Rapid Eye Movement sleep; NREM, Non-Rapid Eye Movement sleep; I%, Percentage of stage I in total sleep time; II%, Percentage of stage II in total sleep time; III%, Percentage of stage III in total sleep time; AHI, Apnea-Hypopnea Index; LAT, Longest Apnea Time; LSaO2, Lowest arterial oxygen saturation; SLT90%, percentage of sleep time when oxygen saturation lower than 90%; ODI, Oxygen Desaturation Index; AD7c-NTP, Alzheimer-associated neural thread protein.* p < 0.05 versus the control group;#p < 0.05 versus the mild-to-moderate group.a Kruskal-Wallis test;b One-way analysis of variance.
Urinary AD7c-NTP levels in the control, the mild-to-moderate and the severe OSA groups
We compared urinary AD7c-NTP concentrations in the three groups, and the difference between the severe OSA group and the control group was statistically significant (p = 0.011) (Table 2). Since age was significantly different between these groups and was considered to be correlated with urinary AD7c-NTP level, we further analyzed the comparison after adjusting age with Analysis of Covariance. The results showed that the urinary AD7c-NTP levels in the severe OSA group were still higher than those in the control group (p = 0.019) (Table 3).
Differences in urinary AD7c-NTP levels between the control, the mild-to-moderate, and the severe OSA groups after adjustment for age
The age and urinary AD7c-NTP data of each group were converted to normally distributed data, namely Log10(Age) and Log10(AD7c-NTP).
Cognitive status in the control, the mild-to-moderate and the severe OSA groups
Overall, the adjusted MoCA scores between the severe OSA group and the other two groups were significantly different (Severe –Control: p < 0.001, Severe –Mild to moderate: p < 0.001). In the visuospatial and executive test, the scores of the severe and the mild-to-moderate OSA patients were lower than those of the control group (Severe –Control: p < 0.001, Mild-to-moderate –Control: p < 0.001). The delayed recall scores of the severe OSA patients were lower than those of the other two groups (Severe –Control: p < 0.001, Severe - Mild-to-moderate: p < 0.001) (Table 4). The subjects whose final adjusted MoCA score < 26 points were judged as cognitive dysfunction. Finally, as for cases combined with cognitive impairment, there were 3 (3/32) in the control group, while a total of 34 (34/106) in the OSA groups, including 25 in the severe group (25/56) and 9 in the mild-to-moderate group (9/50) (Fig. 1). The comparison results showed that the number of patients with cognitive impairment in the severe OSA group was significantly higher than that in the other two groups (p < 0.001) (Table 4).
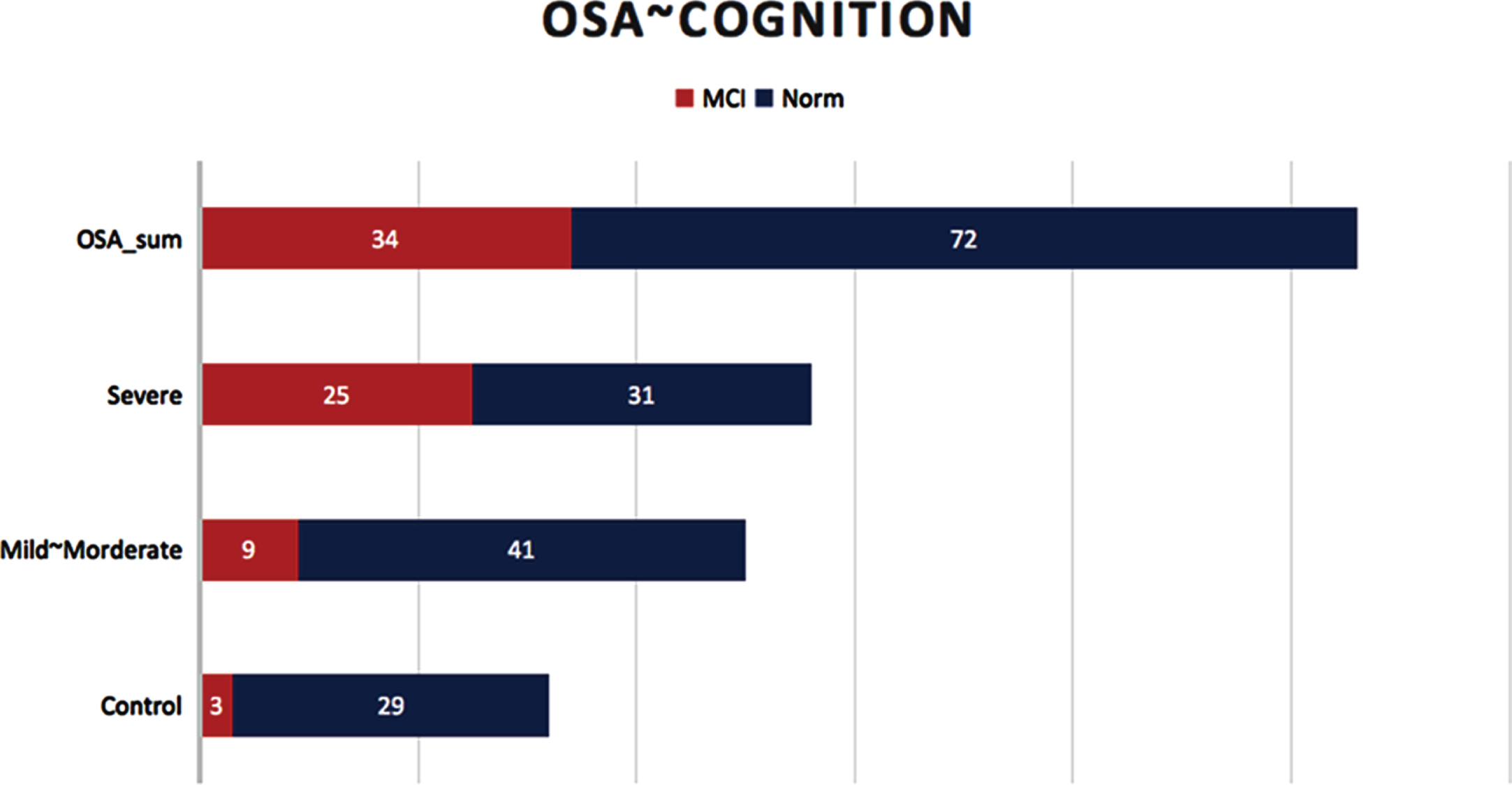
Cognitive performances of the subjects in different groups. The bars represent different groups while the length of bars represents the corresponding case numbers. For each group, the normal and poor cognitive performances were shown in different colors.
The adjusted MoCA scores and their sub-items in the control, the mild-to-moderate and the severe OSA groups
* p < 0.05 versus the control group;# p < 0.05 versus the mild-to-moderate group.a Kruskal-Wallis test;b Chi-squared test.
Correlation analysis of adjusted MoCA scores with PSG parameters and urinary AD7c-NTP concentration in the OSA groups and the control group
Table 5 showed the correlations between the adjusted MoCA scores and the PSG parameters in the control group and the OSA groups. In the control group, the adjusted MoCA score was negatively correlated with NREM I + II% (r = –0.4, p = 0.023) and was positively correlated with NREM III% (r = 0.367, p = 0.039). In the overall OSA group, the adjusted MoCA score was negatively correlated with NREM I + II% (r = –0.239, p < 0.05), AHI (r = –0.485, p < 0.01), LAT (r = –0.318, p < 0.01), SLT90% (r = –0.468, p < 0.01), and ODI (r = –0.492, p < 0.01), and was positively correlated with LSaO2 (r = 0.337, p < 0.01), (Table 5; and the correlation heatmaps are shown in Fig. 2).
Correlations between the adjusted MoCA scores and PSG Parameters in the control, the mild-to-moderate and the severe OSA groups
TST, Total Sleep Time; REM, Rapid Eye Movement sleep; NREM, Non-Rapid Eye Movement sleep; AHI, Apnea-Hypopnea Index; LAT, Longest Apnea Time; LSaO2, Lowest arterial oxygen saturation; SLT90%, percentage of sleep time when oxygen saturation lower than 90%; ODI, Oxygen Desaturation Index. * r represents Spearman rank correlation coefficient.
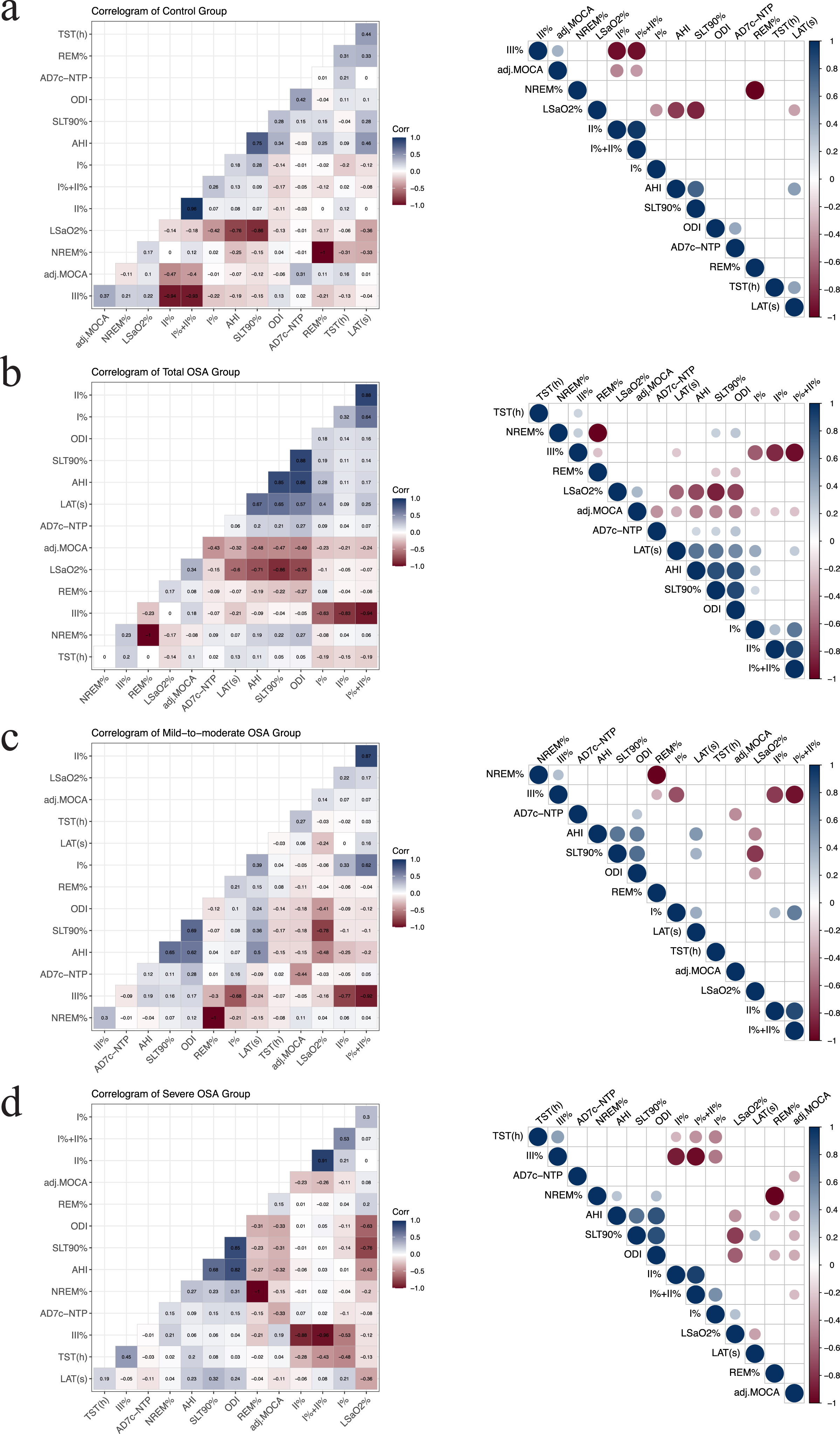
Correlations between the adjusted MoCA scores and PSG parameters and the urinary AD7c-NTP measurements in different groups. Panels a-d show heatmaps of the correlations between the adjusted MoCA scores and PSG parameters and urinary AD7c-NTP concentrations in the control group, the total OSA group, and the mild-to-moderate and the severe OSA groups, respectively. Blue represents positive correlation while red represents negative. The intensity of colors represents the strength of the correlation, and the correlation coefficient is displayed in each square (left). The right column only shows the correlation with p < 0.05, and the size of the dot represents the strength of the correlation.
Multiple studies have indicated that urinary AD7c-NTP levels are related to cognitive impairment, and the similar findings existed in the OSA patients in our study. Figure 3a and 3b show the Spearman rank correlation scatterplots between the adjusted MoCA scores and urinary AD7c-NTP measurements in the overall OSA group and its subgroups, respectively. In the overall OSA group, the MoCA scores were significantly negatively correlated with urinary AD7c-NTP concentrations (r = –0.43, p < 0.001), indicating that the OSA patients with a lower cognitive score had a higher concentration of AD7c-NTP in their urine. Similar results were also obtained in the OSA subgroups (mild-to-moderate: r = –0.44, p = 0.001; severe: r = –0.33 p = 0.012) (Table 6, Fig. 3).
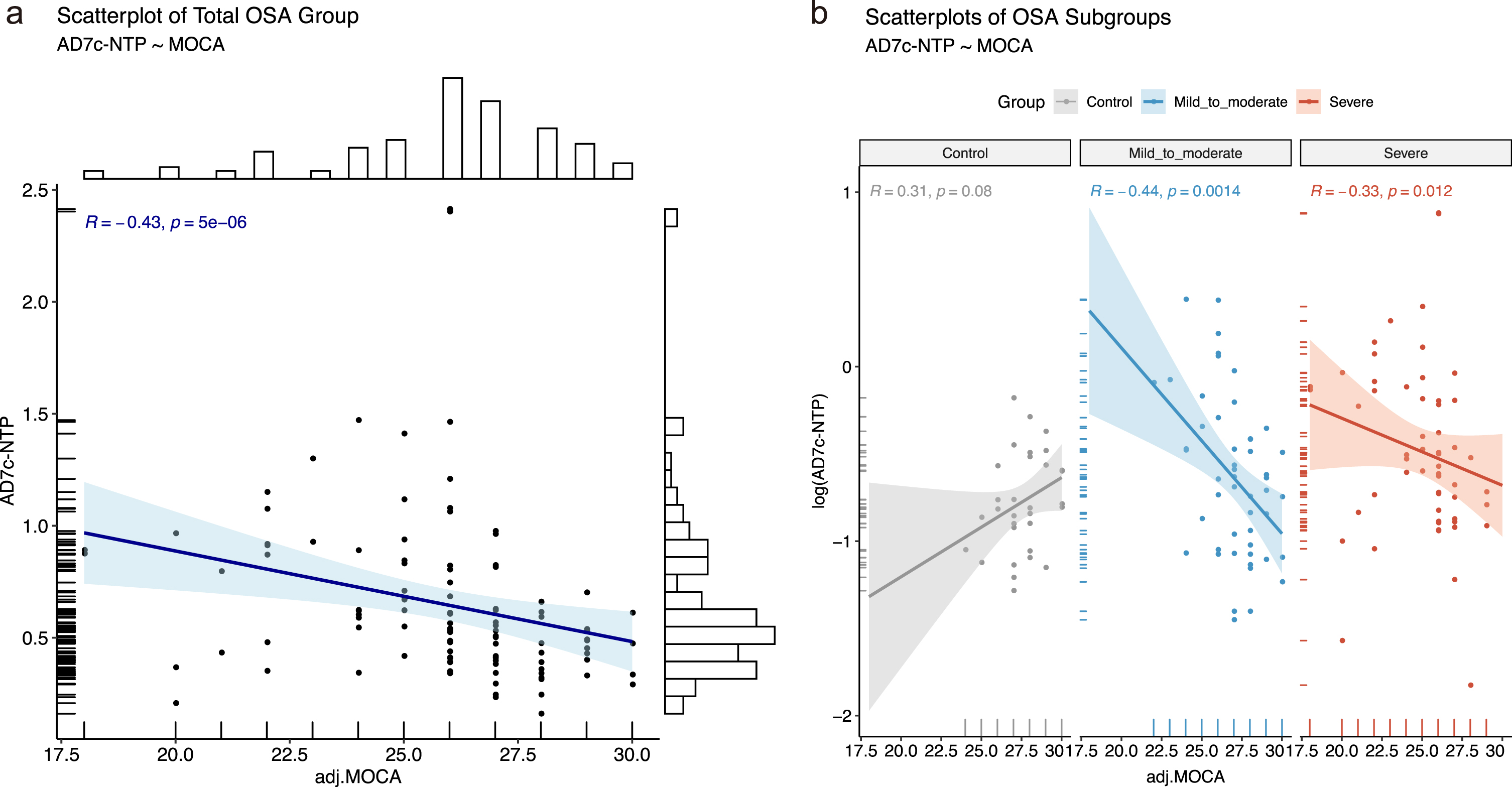
Spearman rank correlation scatterplots between adjusted MoCA scores and urinary AD7c-NTP measurements in the OSA patients. a) In the overall OSA group, adjusted MoCA scores were significantly negatively correlated with urinary AD7c-NTP concentrations (r = -0.43, p < 0.001). b) Significant correlations also obtained in the OSA subgroups (mild-to-moderate: r = -0.44, p = 0.001; severe: r = -0.33, p = 0.012).
Correlations between the adjusted MoCA scores and AD7c-NTP concentrations in the control, the mild-to-moderate and the severe OSA groups
* r represents Spearman rank correlation coefficient.
When analyzing the association between adjusted MoCA scores and urinary AD7c-NTP levels, possible confounding factors such as age also need to be considered. Therefore, we analyzed the candidate related factors of urinary AD7c-NTP concentrations in the OSA patients and further performed partial correlation analysis. The results showed that urinary AD7c-NTP concentrations had a certain correlation with PSG parameters AHI (r = 0.20, p = 0.043), ODI (r = 0.27, p = 0.005), and SLT90% (r = 0.21, p = 0.029) (Fig. 4a–c) and were also positively correlated with age in the OSA group (r = 0.26, p = 0.007) (Fig. 4d). In the OSA group, partial correlation analysis was performed on adjusted MoCA scores and urinary AD7c-NTP concentrations after adjusting for the effects of Age, AHI, ODI, SLT90%, Age+AHI, Age+ODI, Age+SLT90%, and Age+AHI+ODI+SLT90%, respectively. The results were all significant (p < 0.001) (Table 7).
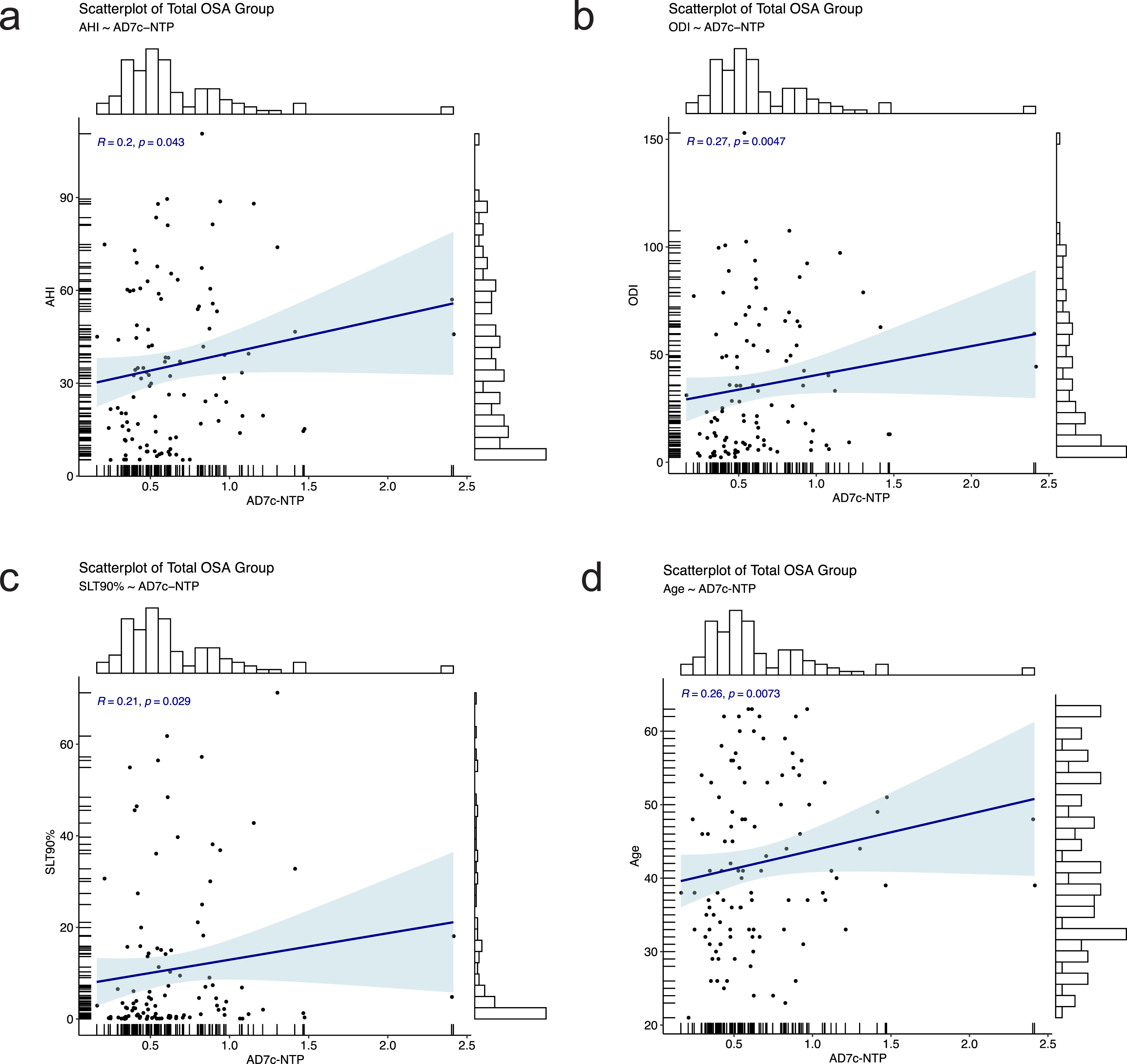
Spearman correlation between urinary AD7c-NTP measurements and PSG parameters and Age in the overall OSA group. a-c) AHI (r = 0.20, p = 0.043), ODI (r = 0.27, p = 0.005), and SLT90% (r = 0.21, p = 0.029) were significantly positively correlated with the urinary AD7c-NTP measurements. d) Urinary AD7c-NTP concentrations were also positively correlated with age in the overall OSA group (r = 0.26, p = 0.007).
Partial correlation between adjusted MoCA scores and urinary AD7c-NTP concentrations given certain confounding factors in the OSA group
* r represents Spearman rank correlation coefficient; # gp represents the number of given variables.
Differences between the OSA groups with and without cognitive impairment
As described above, we divided the overall OSA samples by the adjusted MoCA scores into two groups, the cognitive impairment group (adj.MoCA<26 points, n = 34) and the non-cognitive impairment group (adj.MoCA≥26 points, n = 72), for further analysis. Table 8 shows the differences of OSA clinical features, PSG parameters and urinary AD7c-NTP levels between the two groups.
Obviously, most of the clinical characteristics were significantly similar which reflected matching. Compared with the non-cognitive impairment group, OSA patients with cognitive impairment were older and had a higher BMI, with statistical differences (p < 0.05). Moreover, significant differences existed in certain PSG parameters and urinary AD7c-NTP levels when the two groups were compared. NREM I% +II%, AHI, SLT90%, ODI and urinary AD7cNTP level in the cognitive impairment group were higher than those in the non-cognitive impairment group (p < 0.01), LAT was longer than that in the non-cognitive impairment group (p < 0.05), while LSaO2, NREM III% were lower than those in the non-cognitive impairment group (p < 0.05) (Table 8).
The clinical characteristics, PSG parameters and urinary AD7c-NTP levels in the OSA groups with and without cognition impairment
DNS, Deviation of Nasal Septum; SUC, Subjective Uncomfortableness, including disturbed sleep and morning headache; EDS, Excessive Daytime Sleepiness; SCD, Subjective Cognitive Decline, including subjective memory loss and lags in response; TST, Total Sleep Time; REM, Rapid Eye Movement sleep; NREM, Non-Rapid Eye Movement sleep; I%, Percentage of stage I in total sleep time; II%, Percentage of stage II in total sleep time; III%, Percentage of stage III in total sleep time; AHI, Apnea-Hypopnea Index; LAT, Longest Apnea Time; LSaO2, Lowest arterial oxygen saturation; SLT90%, percentage of sleep time when oxygen saturation lower than 90%; ODI, Oxygen Desaturation Index; AD7c-NTP, Alzheimer-associated neural thread protein.aKruskal-Wallis test;bChi-squared test;cFisher Exact Test;dOne-way analysis of variance.
Cognition risk prediction model for OSA patients
The urinary AD7c-NTP level is an important candidate biomarker for cognition risk prediction. A single-term model was established based on urinary AD7c-NTP levels to observe the predictive value of this major peripheral biomarker to cognitive impairment in OSA patients. An optimized threshold of 0.543 ng/ml was derived from ROC curve analysis maximizing the area under the curve (AUC = 0.722), and the sensitivity and specificity of urinary AD7c-NTP levels in predicting cognitive impairment were found to be 79.4% and 62.5%, respectively (Fig. 5a, left). A calibration curve was used to estimate the consistency between the predicted and observed values of the model, and the mean absolute error was 0.086 based on bootstrapping (repetitions = 1000) (Fig. 5a, right).
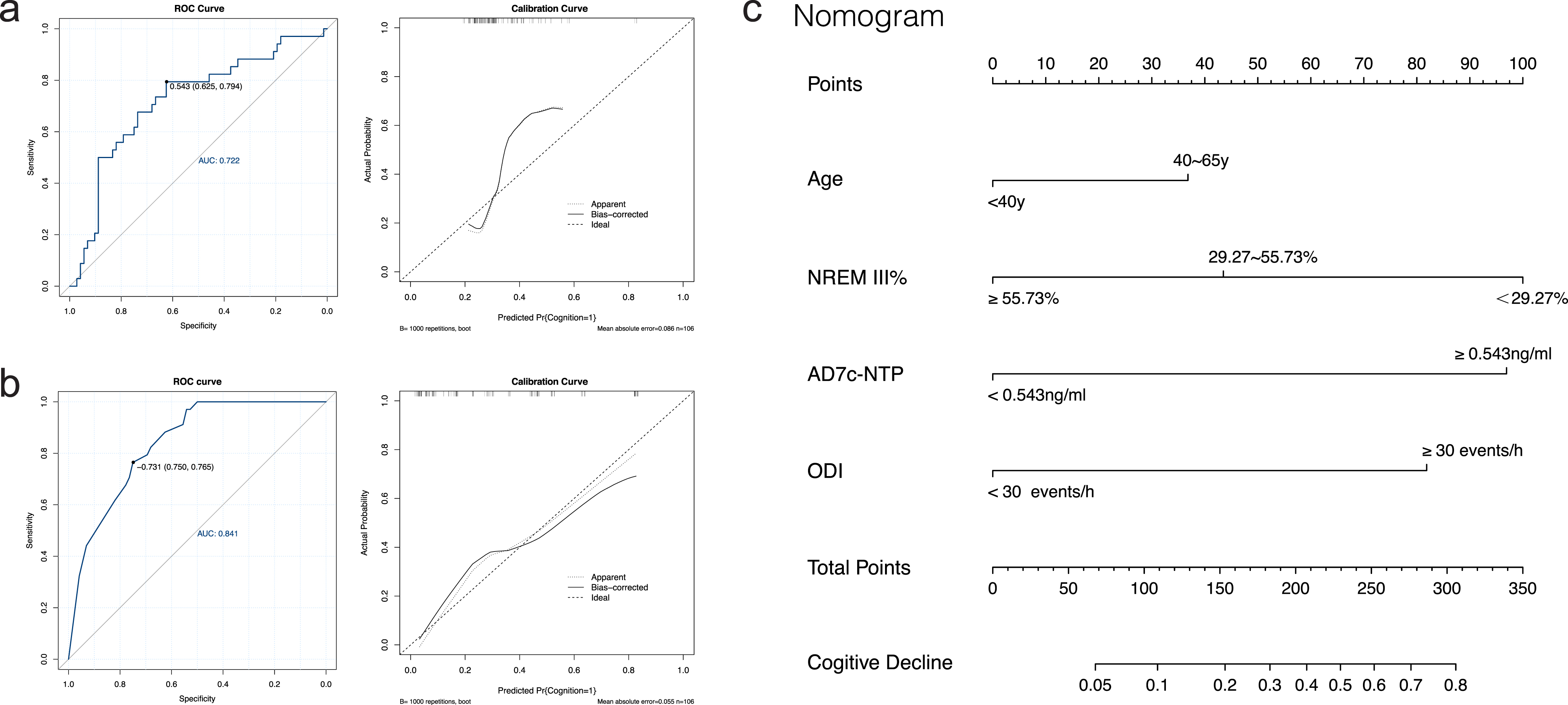
Prediction of cognitive impairment in OSA patients with the models based on urinary AD7c-NTP level and comprehensive individual features. a) The ROC curve (left) and the calibration curve (right) of the single-term model established based on urinary AD7c-NTP level. b) The ROC curve (left) and the calibration curve (right) of the multivariate regression model. c) Nomogram of the multivariate regression model to predict the risk of cognitive impairment in OSA patients.
Univariate and multivariate regression analyses were used in this part. Single-variable regression models were built and the cognitive outcomes of the participants were used as the dependent variables of the models, in which the adj.MoCA scores < 26 points were judged as cognitive impairment. The independent variables of the models were potential factors, including several clinical features, the severity of OSA, PSG parameters, and urinary AD7c-NTP levels, which may affect the cognitive function of OSA patients. Among them, the severity grading of OSA (rs = 1.301, p = 0.004), Age (rs = 1.358, p = 0.003), NREM I + II% (rs = 1.986, p = 0.019), NREM III% (rs = –1.245, p = 0.007), SLT90% (rs = 1.375, p = 0.03), ODI (rs = 1.778, p < 0.001), and urine AD7c-NTP levels (rs = 1.861, p < 0.001) were correlated with the cognitive outcomes. Table 9 describes the variable assignments, odds ratios (ORs) and statistical significances.
Univariate regression analyses of cognitive impairment in OSA patients and descriptions of independent variable assignments
SUC, Subjective Uncomfortableness, including disturbed sleep and morning headache; EDS, Excessive Daytime Sleepiness; SCD, Subjective Cognitive Decline, including subjective memory loss and lags in response; REM, Rapid Eye Movement sleep; NREM, Non-Rapid Eye Movement sleep; I%, Percentage of stage I in total sleep time; II%, Percentage of stage II in total sleep time; III%, Percentage of stage III in total sleep time; LAT, Longest Apnea Time; LSaO2, Lowest arterial oxygen saturation; SLT90%, percentage of sleep time when oxygen saturation lower than 90%; ODI, Oxygen Desaturation Index; AD7c-NTP, Alzheimer-associated neural thread protein. All continuous variables were discretized for further analysis.# The continuous variables that unable to be graded according to clinical significance temporarily were artificially divided into three groups using the equal-width binning algorithm. ***p < 0.001, **p < 0.01, *p < 0.05.
Independent variables with statistical significance (OSA Severity, Age, NREM I + II%, NREM III%, SLT90%, ODI and urinary AD7c-NTP levels) were included in the multivariate logistic regression model to further analyze the effect of each variable on the cognitive outcomes of the OSA patients. The variable assignment descriptions were the same as in Table 9, and Table 10 shows the correlation coefficient and statistical significance of each variable of the new model. To our surprise, only the urinary AD7c-NTP level was statistically significant in both univariate and multivariate regressions (rs = 1.744 and p = 0.0027 in the multivariate model), indicating that urinary AD7c-NTP level could be used as an independent predictor of OSA cognitive comorbidities. Akaike information criterion (AIC) was performed to measure the goodness of fit, and it was 113.82 in the multivariate model.
Multivariate regression analysis of cognitive impairment in OSA patients
NREM, Non-Rapid Eye Movement sleep; I%, Percentage of stage I in total sleep time; II%, Percentage of stage II in total sleep time; III%, Percentage of stage III in total sleep time; SLT90%, percentage of sleep time when oxygen saturation lower than 90%; ODI, Oxygen Desaturation Index; AD7c-NTP, Alzheimer-associated neural thread protein. ***p < 0.001, **p < 0.01, *p < 0.05.
In view of the obvious correlation between some PSG parameters (AHI, SLT90% and ODI, NREM I% +II% and III%), we further debugged the multivariate regression model. Finally, the Age, NREM III%, ODI and urinary AD7c-NTP level were selected into the final prediction model (Table 11), and its performance was assessed (Fig. 5b). The AIC, Sensitivity, Specificity, and AUC of the final model were 106.87, 76.5%, 75.0%, and 0.841, respectively (Fig. 5b, left). The calibration curve was applied to evaluate the calibration degree of the final model, and the simulation was repeated 1000 times with mean absolute error- = 0.055 (Fig. 5b, right). In the end, a nomogram was drawn to predict the risk of cognitive impairment in OSA patients (Fig. 5c). We named the final prediction model PredCI_OSA (v1.0) and developed a web platform to help users make on-line predictions automatically.
Final cognition risk prediction model for OSA patients
III%, Percentage of stage III in total sleep time; ODI, Oxygen Desaturation Index; AD7c-NTP, Alzheimer-associated neural thread protein. ***p < 0.001, **p < 0.01, *p < 0.05.
OSA is a highly prevalent disease and is considered to be an independent risk factor for cognitive impairment [5]. Unlike most diseases that cause cognitive impairment, which usually occur in elderly patients, OSA has a higher incidence in young and middle-aged people in epidemiology. Unfortunately, these age groups are also the most important labor force in society, so their cognitive deficits may have more serious consequences for both individuals and society. Therefore, early cognitive screening in OSA patients is of great necessity. It can improve patients’ awareness of sleep disorders and cognitive comorbidities, and it can also provide evidence for physicians to take effective actions to prevent and treat cognitive decline in its early stages. However, methods for assessing cognitive impairment, especially MCI, such as neuropsychological assessments and cerebrospinal fluid tests, have certain limitations and most of the time are not applicable for OSA patients. Instead, peripheral biomarkers of MCI/AD such as urinary AD7c-NTP levels can serve as good alternatives. However, up to now, little is known about the relationship between urinary AD7c-NTP levels and cognitive performance in OSA patients.
The cognitive impairment of OSA patients is mainly manifested in memory, attention, alertness, executive ability and other aspects [9]. In this study, we found that the severe OSA patients showed poorer cognitive performances compared with the other two groups, especially the control participants. This observation is consistent with previous reports [8, 14]. We further analyzed different domains of cognitive function and found that the severe OSA patients had impairments in language, delayed recall, and executive function. Although mild-to-moderate OSA seemed to have little impact on the total MoCA scores, their executive function had declined compared with the controls. This result reflects that executive function may be impaired even in the early stages of OSA. More importantly, mild-to-moderate OSA may be associated with an increased risk of developing cognitive impairment when OSA progressed without timely intervention [7].
AD7c-NTP was first isolated from the temporal lobe brain tissue of advanced AD patients. It is expressed in the axon of neurons, which specifically reflects the rate of neuron injury [30]. This biochemical marker has a historical origin that can be traced at least to two decades ago, and laboratory test methods [25] and clinical ELISA kits [26] were developed in 1998 and 2016, respectively. However, the underlying mechanisms remain unclear. Previous studies have found that increased AD7c-NTP level in neurons can promote neuroinflammation and neuronal death and amyloid-β deposition, thus participating in the development of AD. And AD7c-NTP can cross the blood-brain barrier and be filtered out via glomerular filtration, therefore, AD7c-NTP in urine can serve as a potential biomarker for the diagnosis of MCI/AD, just like that in CSF [25]. Previous studies demonstrated that AD7c-NTP level was associated with MoCA score, Mini-Mental State Examination score, and amyloid-β deposition [31–33]. In the present study, the urinary AD7c-NTP levels in OSA cases were higher than those in the controls, and were significantly negatively correlated with adjusted MoCA scores, that is, elevated urinary AD7c-NTP levels in OSA patients were associated with poor cognitive performance. This pattern of the relationship between the elevated level of urinary AD7c-NTP and the decreased cognitive ability in OSA patients was similar to that observed in patients with MCI or even AD [32, 33]. The comparison results of the OSA patients grouped by cognitive status also showed that the urinary AD7c-NTP concentration in the OSA cognitive impairment group was higher than that in the non-cognitive impairment group, suggesting that an increased urinary AD7c-NTP level may be a relevant peripheral biomarker of cognitive impairment in OSA patients.
Chronic intermittent nocturnal hypoxia, which is considered to be one of the pivotal mechanisms that can adversely affect cognitive performance, often exists in OSA patients due to repeated collapse or obstruction of upper airway during sleep. Previous studies have proposed some hypotheses about patterns of cognitive impairment caused by intermittent hypoxia, such as inflammatory cytokine release and nerve injury [34], resulting in elevated AD7c-NTP levels in patients’ urine. In our study, this assumption was demonstrated by the positive correlation of urinary AD7c-NTP levels in OSA patients with PSG parameters representing OSA severity and hypoxia (AHI, ODI, and SLT90%). However, further studies are required to explore the underlining mechanisms. Furthermore, urinary AD7c-NTP levels were shown to be age-related in this and previous studies [35]. However, after adjusting for age bias, urinary AD7c-NTP levels remained significantly different between the OSA and the control groups and were still associated with cognitive impairment in the OSA group. It suggests that the urinary AD7c-NTP is a strong predictor of cognitive impairment in OSA patients.
There is still no consensus on the concentration threshold of urinary AD7c-NTP levels for the diagnosis of cognitive impairment in OSA patients. In the general population, Chen et al. found that the effect of distinguishing MCI and non-MCI was the best when the critical value of urine AD7C-NTP concentration was set to 0.268 ng/ml, with a sensitivity and specificity of 83.3% and 90.0%, respectively [36]. The results of Ma et al. showed that the optimal cut-off value of urinary AD7c-NTP levels for the diagnosis of AD in the general population was 1.5 ng/ml, and the sensitivity and specificity of the AD prediction model were 89.3% and 84.7%, respectively [26]. In this study, we proposed an optimal cut-off value of 0.543 ng/ml to define cognitive impairment in OSA patients, with a sensitivity of 79.4% and a specificity of 62.5%. Univariate and multivariate regression analyses were performed on cognitive impairment in OSA patients using this optimal cut-off value (0.543 ng/ml) as the classification criterion. The results showed that urinary AD7c-NTP levels in both models were significantly correlated with cognitive outcomes in OSA patients, suggesting that the urinary AD7c-NTP level could serve as an independent predictor of OSA cognitive comorbidities.
In addition, there are many adverse factors that contribute to the cognitive impairment in OSA patients. Previous researches have shown that the clinical features, severity, nocturnal hypoxemia, sleep fragmentation, and other characteristics of OSA affect the cognitive function [17–21], which also can predict the cognitive status of OSA patients to a certain extent. In our study, BMI and Age were risk factors for cognitive impairment in OSA patients. Obese OSA patients typically have more severe upper airway obstruction as well as increased frequency and duration of nocturnal hypoxia, which can negatively impact cognitive function. The overall cognitive function of middle-aged OSA patients is worse than that of young adults, which may be related to age-related individual physiological changes, such as low position of the hyoid bone [37], and reduced response of genioglossus muscle to hypoxia [38]. These changes aggravate upper airway obstruction and hypoxia, and further affect the cognitive function in OSA patients. Moreover, cognitive reserve generally declines with age.
Additionally, our results showed that there was a significant difference in the indicators related to hypoxia such as ODI and SLT90%, between the cognitive impairment group and the non-cognitive impairment group, suggesting that the intermittent hypoxia may be involved in the cognitive dysfunction in OSA cases. We found that NREM III% (i.e., slow wave sleep) was significantly reduced in the OSA cognitive impairment group compared with the OSA cognitive control group. Consistent with our research, some earlier studies have demonstrated that abnormal sleep architecture were associated with cognitive decline, and suggested that sleep loss and slow wave sleep disruptions may lead to further accumulations of amyloid and tau and accelerate cognitive impairment [39, 40]. In conclusion, we have found the correlations between cognitive deficits and some test indicators, and these findings indicate that chronic intermittent hypoxia and disordered sleep structure may be involved in the cognitive impairment in OSA patients.
Our results suggest that urinary AD7c-NTP level is an independent predictor of cognitive impairment and can be used to predict cognitive status in OSA patients. Some factors that significantly associate with the cognitive scores of OSA patients, such as Age, ODI, and NREM III%, can further improve the performance of OSA cognitive prediction model. In this study, two models were established, a univariate model based on urinary AD7c-NTP levels and a multivariate model combining urinary AD7c-NTP levels and OSA clinical characteristics and PSG parameters. The results showed that the multivariate model performed better, and we named it PredCI_OSA.
In conclusion, our results supported that the cognitive impairment that occurs in OSA patients was statistically associated with urinary AD7c-NTP levels and some PSG parameters. A novel cognition risk prediction tool was proposed and a web server implementing it was initiated to facilitate application of the model more conveniently. The website is accessible freely: http://61.160.194.165 : 3080/PredCI_OSA. OSA patients only need to provide urinary AD7c-NTP concentrations, Age and PSG parameters ODI and NREM stage III% to predict cognitive risk (access through the link: http://61.160.194.165 : 3080/PredCI_OSA/tool_patients.html. In addition, researchers or laboratories can submit a TXT file in the required format to perform cognitive impairment risk prediction in batches and obtain an integrated cognitive risk score table (access through the link: http://61.160.194.165 : 3080/PredCI_OSA/tool_lab.html). To our knowledge, this is the first time to propose an OSA cognitive comorbidity prediction model based on urinary AD7c-NTP biomarkers, and the tool can be used for prediction directly with good sensitivity, specificity, and clinical application value.
There were several limitations to this study. First, the sample size was relatively small, which limited the power of the findings. The PredCI_OSA performance has not been evaluated in an independent dataset either. Besides, although individuals diagnosed with dementia were excluded, cognitive impairment due to other comorbidities cannot be totally rule out. In our confined working condition, the subjects could not be further examined to rule out the influence of other diseases on cognition. Fortunately, the subjects of this study were young and middle-aged patients with few other comorbidities which may affect cognitive function too much. And these comorbidities had no significant between-group differences, so that they did not affect the results of the correlation analysis between urinary AD7c-NTP levels and MoCA scores in OSA patients. Even so, since medical history collection was based on patients’ own report and cognitive impairment was only defined by MoCA scores, there might still be some errors that affect the accuracy of the final results. Finally, due to the cross-sectional design, the dynamic changes of these correlated factors could not be examined. Actually, the participants with high risk of cognitive decline based on preliminary screening will be selected to further CSF examination in our future work. Meanwhile, it is better to use a 24-h urine excretion instead of a spot urine sample, as AD7c-NTP levels may be affected by diurnal fluctuations. However, we expect that this study will provide help for the early detection of cognitive complications in OSA patients, and future studies are needed to explore the precise mechanisms underlying current observation.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0451r2).