
Abstract
Background:
Recent innovative non-pharmacological interventions and neurostimulation devices have shown potential for application in the treatment of Alzheimer’s disease (AD). These include photobiomodulation (PBM) therapy.
Objective:
This pilot study assesses the safety, compliance with, and efficacy of a brain-gut PBM therapy for mild-to-moderate AD patients.
Methods:
This double-blind, randomized, monocentric sham-controlled study started in 2018 and ended prematurely in 2020 due to the COVID-19 pandemic. Fifty-three mild-to-moderate AD patients were randomized, 27 in the PBM group and 26 in the sham group. All patients had 40 treatment sessions lasting 25 min each over 8 weeks and were followed for 4 weeks afterwards. Compliance with the treatment was recorded. Safety was assessed by recording adverse events (AEs), and efficacy was evaluated using neuropsychological tests.
Results:
The PBM therapy proved to be safe in regard to the number of recorded AEs (44% of the patients), which were balanced between the PBM and sham groups. AEs were mainly mild, and no serious AEs were reported. The majority of the patients (92.5%) were highly compliant, which confirms the feasibility of the PBM treatment. Compared to the sham patients, the PBM patients showed lower ADAS-Cog comprehension subscores, higher forward verbal spans, and lower TMT-B execution times, which suggests an improvement in cognitive functions.
Conclusion:
This study demonstrates the tolerability of and patient compliance with a PBM-based treatment for mild-to-moderate AD patients. It highlights encouraging efficacy trends and provides insights for the design of the next phase trial in a larger AD patient sample.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) represents a serious public health problem, for which no clearly efficient treatment is currently available [1, 2]. Therefore, therapies that could delay the onset, slow the progression, and improve the symptoms of AD are urgently needed. Drug development for AD is challenging and still has a high failure rate. To date, most clinical trials have targeted amyloid-β and tau, the two main biological features of AD, but the results of these trials can be viewed as mixed or controversial at best, and disappointing at worst [3–6]. These results, which are based on the amyloid hypothesis of AD physiopathology, emphasize the need to develop combination therapies and expand the AD therapy toolbox to include other targets [7, 8].
Many biochemical processes other than the amyloid-β metabolism and tau hyperphosphorylation are affected in AD, including mitochondrial dysfunction, oxidative stress, and inflammation [9, 10]. Chronic neuroinflammation is a well-established hallmark of AD, attributed to the release of numerous cytokines and toxic products, such as reactive oxygen species (ROS), by activated microglia cells. This ROS production combined with the widely described altered brain glucose metabolism in AD patients reflect the impaired mitochondrial functions.
In recent years, innovative non-pharmacological treatments such as photobiomodulation (PBM), transcranial magnetic stimulation, transcranial electromagnetic treatment, transcranial direct or alternating current stimulation, and deep brain stimulation have been developed to treat neurological and psychiatric disorders and have demonstrated a potential for application in the treatment of AD [11–17]. PBM is a safe, non-invasive, and non-thermal therapy that uses red or near-infrared (NIR) light to stimulate the complex IV of the mitochondrial respiratory chain, resulting in adenosine triphosphate synthesis [18]. PBM is known to improve tissue healing, promote cell survival, and reduce inflammation and oxidative stress [18–20]. In recent pilot clinical trials, PBM treatment has been shown to improve neuropathology and disease progression in mouse models of AD and to provide cognitive improvement trends in patients with dementia and AD [21–25]. PBM is considered to induce neuroprotection by direct stimulation into or onto the skull, but indirect (remote) PBM stimulation through targeting another part of the body (e.g., abdomen or leg) can also induce a neuroprotective effect [26–30]. While the mechanism by which this occurs remains unknown, some researchers hypothesize that it probably involves the stimulation of one or more circulating molecules or cell types. Specific targets, such as the gut or the mouth that contain microbial ecosystems, could also be stimulated and influenced by PBM [31–34]. The effect of light on metabolomics and the microbiome is increasingly being studied as a novel mechanism called photobiomics [32]. When applied to both the head and abdomen, PBM treatment induced an improvement in all parameters in the Aβ25–35-injected mouse model, including memory performance associated with markers of oxidative stress, neuroinflammation, apoptosis, amyloid-β processing, and tau hyperphosphorylation [30]. Recent studies have indicated a connection between the gut-brain axis and the potential role of microbiota in the development of many neurodegenerative diseases, including AD [35–37]. This dynamic bidirectional communication between gut and brain occurs via the immune system, the vagus nerve, the enteric nervous system, and microbial metabolites. Therefore, targeting the microbiome-gut-brain axis with an innovative PBM therapy could be a valuable disease-modifying treatment for AD.
The medical device RGn530 used for brain-gut PBM therapy consists of a modular helmet and an abdominal belt, each of which is composed of NIR low-level lasers, NIR light-emitting diodes (LEDs), and red LEDs, as well as a static magnetic field (SMF) (Fig. 1). The technical specifications of the optical components are described in Table 1. Transcranial SMF stimulation has been shown to safely reduce motor and somatosensory cortex excitability in healthy subjects [38–40].
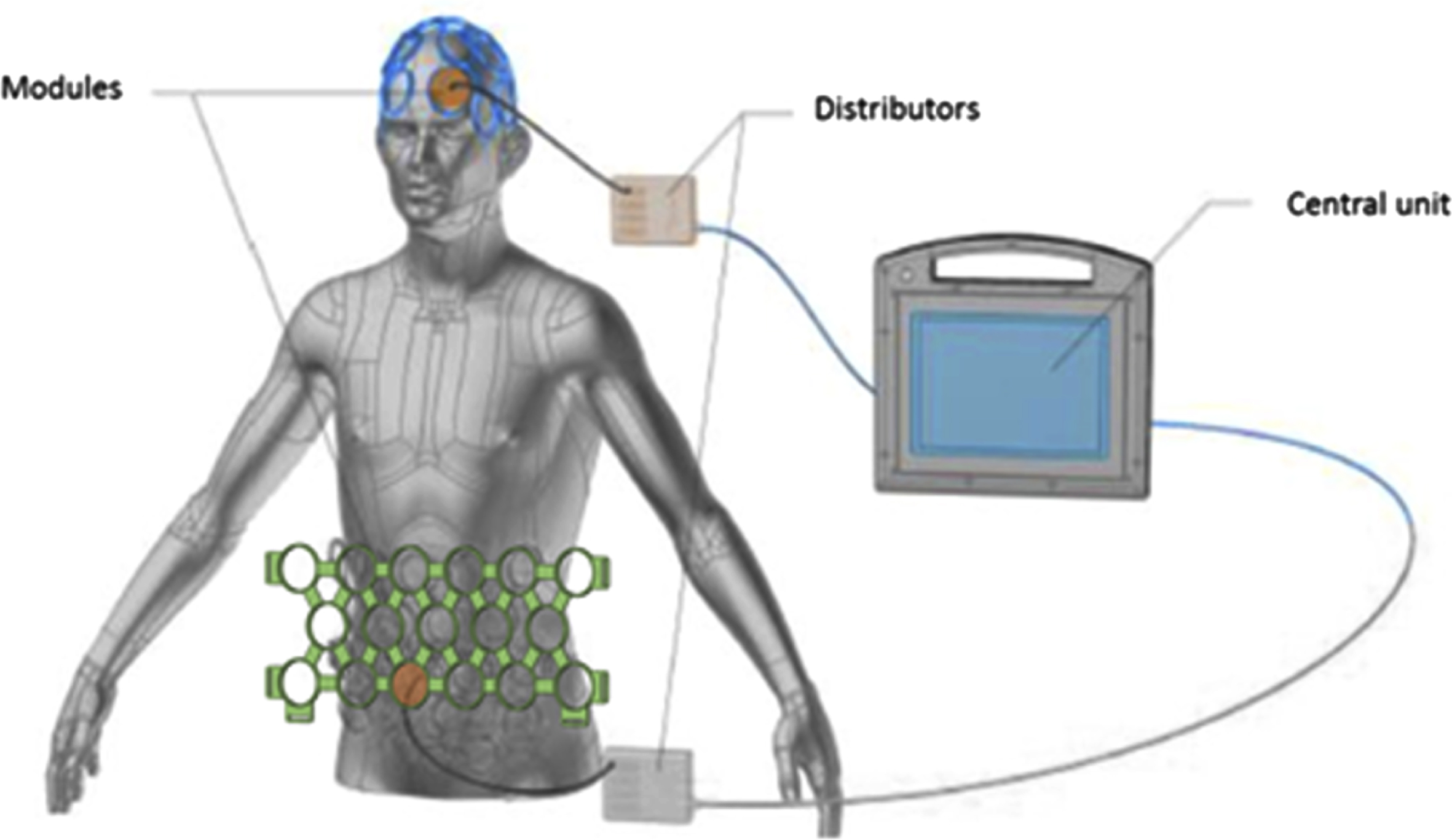
PBM device. Main components of the PBM device (REGEnLIFE RGn530), including the central unit, the helmet, the abdominal panel integrated modules, and two distributors that centralize the connections.
Technical specifications of the REGEnLIFE RGn530 for PBM therapy
Following the introduction of this innovative PBM therapy with such promising results, the objective of the present pilot clinical study is to evaluate safety, tolerance, overall compliance, and effectiveness of this PBM therapy compared to a placebo-sham procedure in patients with mild to moderate AD. This evaluation is based on clinical examination, biological parameters, and cognitive performance. Could the action on mitochondria and neuroinflammation by PBM therapy at the brain-gut level be translated into clinical benefits for patients with AD?
Despite the challenges of developing effective therapies, the PBM treatment could have valuable potential as an innovative and widely applicable therapeutic strategy for AD.
MATERIALS AND METHODS
Study design
This study was a double-blind, randomized, monocentric, sham-controlled clinical trial (NCT03672474). Randomization of patients to one of the treatment groups (PBM or sham) was stratified by gender, age (cut-off at 85 years old), and the Mini-Mental State Examination (MMSE) score for inclusion (cut-off at 21 points). The study duration was 12 weeks; each patient had 40 treatment sessions lasting 25 min each over a period of 8 weeks, from D1 to D60 (with 5 sessions per week), and were followed for a 4-week period after treatment discontinuation. The patients had five mandatory visits, namely the inclusion visit (V0:30 to 10 days before V1) and the treatment initiation visit (V1, D0), followed by a follow-up visit during the treatment (V2 on D30), a follow-up visit just after the end of the treatment (V3 on D60) and a last follow-up visit, 30 days after the end of the treatment (V4 on D90). The study design protocol is summarized in Fig. 2.

Schematic of the study design protocol.
Study population
Patients eligible for enrolment were between 55 and 85 years old and had been diagnosed with AD according to the international diagnosis criteria of McKhann et al. [41] at a mild to moderate stage, as determined by an MMSE score of between 16 and 26. They provided written consent to participate in the study. Patients on symptomatic treatment specific to AD (memantine, acetylcholinesterase inhibitors) and psychotropic treatment (anxiolytics, anti-depressants, neuroleptics) were allowed to participate, but those treatments had to be maintained at fixed doses during the 4 weeks prior to inclusion and throughout the study.
Exclusion criteria included genetic forms of AD, any physical or major neurosensory problems liable to interfere with the tests, epilepsy or other non-neurodegenerative diseases of the central nervous system, chronic psychosis or psychotic episodes, alcohol or drug addiction, and major skin lesions on the treatment application regions.
All eligibility criteria are described in Table 2.
Demographic and clinical characteristics at inclusion, according to treatment group (Analysis population, N = 53)
[a] MMSE is scored from 0 to 30, with a higher score indicating better performance. [b] ADAS-Cog is scored from 0 to 70, with higher scores (≥18) indicating greater cognitive impairment. Comprehension sub-score is scored from 0 to 5. [c] Forward verbal span score is the number of correct responses. ADAS-Cog, Alzheimer’s Disease Assessment Scale-cognitive Subscale; MMSE, Mini-Mental State Examination; PBM, photobiomodulation; TMT, Trail Making Test.
Investigational medical device
The PBM medical device, RGn530, developed by REGEnLIFE, consists of a helmet and an abdominal belt, both with integrated modules composed of several lighting source emitters. Those emitters are comprised of three pulsed laser diodes in the NIR spectrum (850 nm), three LEDs in the NIR spectrum (850 nm), and three LEDs in the red spectrum (660 nm). The photonic emissions are pulsed at a 10 Hz frequency through a ring-shaped magnet, creating an SMF. The helmet and abdominal belt are connected to a central unit. The sham device was identical to the PBM device, but all NIR emissions were inactivated, and red emissions were reduced to 10% of the emission power, as these emissions can be visible to the naked eye on the side of the modules. The magnetic field of the sham device was reduced by 50%. Research staff and patients were thus completely blinded to the treatment group allocations.
During treatment, patients sat in a semi-recumbent position. The helmet and abdominal belt were positioned by the research staff according to user instructions. The helmet and abdominal belt were covered by a lightproof cap and blanket, so that the patients and the PBM operators did not have to wear laser safety glasses. Treatment was administered by the graphical user interface available on the central unit. The parameters associated with the treatment (power density, wavelength, fluence, pulse repetition frequency, timing, and magnetic field) could not be modified by the user. Each session ended automatically once the treatment cycle was complete.
Study assessments
Compliance with study treatment was recorded from the first (V1) to the last treatment session (V3 or earlier in the event of early withdrawal). The date, start time, and length of the session were recorded at each session. When appropriate, the reason why a session was not performed was recorded.
Safety assessments included the recording of all adverse events (AEs), from the time of the patient signing the informed consent to the completion of the study, independent of the severity of the AEs or their relationship to the investigational device. All events were coded with the MedDRA dictionary version 24.0. Patients underwent a physical examination (including weight, abdominal circumference, arterial blood pressure, and heart rate) at V0, V2, V3, and V4. Blood samples were collected at V0, V2, and V3 for standard laboratory parameters assessment.
Efficacy evaluation at V0, V3, and V4 was based on neuropsychological tests, including the Alzheimer’s Disease Assessment Scale-cognitive Subscale (ADAS-Cog) as the primary efficacy outcome, and the MMSE. The validated French ADAS-Cog version of the cognitive scale, which includes 11 tasks, was used to evaluate the cognitive domains of memory, language, and praxis (scored from 0 to 70, with higher scores indicating worse performance) [42]. The MMSE is a short screening tool that includes 30 questions to evaluate cognitive impairment and is scored from 0 to 30, with higher scores indicating normal cognitive functions. A score between 21 and 25 suggests mild AD, between 10 and 20 moderate AD, and below 10 severe AD [43]. Executive functions and attention were evaluated by employing parts A and B of the Trail Making Test (TMT) and verbal spans were investigated according to the Wechsler Adult Intelligence Scale-IV (WAIS-IV). The TMT is an executive function test composed of two tasks (parts A and B), which engage various cognitive processes, such as selective attention, motor activity, and cognitive flexibility [44]. The time to accomplish a task, the number of correct moves, and the number of errors were recorded. The verbal span evaluation of the WAIS-IV requires the subject to recall information in either a forward or a backward order [45, 46]. The number of correct responses constitutes the score.
All efficacy assessments are exhaustively described in Table 2.
Sample size and power
We expected the ADAS-cog scores of the sham group to vary from those of the PBM group by no more than 0.4 points and expected the differences to reach 3.4 points by V3, with an SD of 5.5 [47]. The number of participants required to show a significant difference was estimated at 29 per group, based on 80% statistical power and a 5% two-sided α-level. We planned to include a total of 64 patients, expecting 10% early withdrawals.
Statistical analyses
All statistical analyses were performed using the SAS® statistical package version 9.2 (SAS Institute Inc., Cary, NC, USA).
The demographics, clinical data at inclusion, treatment compliance, and efficacy assessments of the analysis population, composed of patients who had provided informed consent and had been randomized regardless of the number of treatment sessions attended, were analyzed.
The demographics and clinical data at inclusion were only descriptive. The participation rate (%) was defined as the number of treatment sessions received/total number of planned sessions*100. Compliance with treatment was categorized as follows: very good compliance, participation rate ≥75%; good compliance, participation rate [60–75%]; poor compliance, participation rate <60%. The ADAS-Cog, MMSE, TMT A and B scores, and verbal spans were calculated as described in the literature [42–46].
Safety analyses were performed on the safety population, which was composed of all patients who had attended at least one treatment session.
For quantitative variables, the normality of the distribution hypothesis was verified graphically and with the use of the Shapiro-Wilk test. If verified, distribution was compared with a two-sided Student’s t-test; if not, a Mann-Whitney-Wilcoxon test was performed instead. Qualitative variables were compared using a Chi-square test. The Chi-square test was replaced by Fisher’s exact test if the expected frequency in any of the cells of the contingency table was less than 5. All the tests were two-sided. A test was considered to be significant when the associated p-value was lower than a significance threshold of 5%.
RESULTS
Patient disposition
Between August 2018 and January 2020, 60 patients were recruited to participate in this study in the unique study center, with 53 of those patients (88.3%) being randomized. The number of included patients was smaller than planned, as the study had to end prematurely due to the COVID-19 pandemic. Among the seven patients (11.7%) not randomized, six (10%) did not meet the study’s eligibility criteria, and one patient (1.7%) secondarily refused to participate in the study. After randomization, 27 patients were allocated to the PBM group and 26 to the sham group.
Overall, 88.7% of the patients completed the study according to the protocol (i.e., up to V4, D90). Six patients (three patients per treatment group) withdrew from the study by refusing further participation. The median study duration was 98 days (range, 8–168 days) for the analysis of the population as a whole, with 105 days (range, 9–168 days) as the median for the PBM group and 96.5 days for the sham group (range, 42–164 days).
Demographic and clinical characteristics at inclusion
The baseline patient demographics and clinical characteristics are summarized in Table 2. The patients in the analysis population were mainly female (N = 31; 58%), with a mean (standard deviation [SD]) age of 73 (6.7) years (range, 55–84 years). The median time since the onset of AD symptoms and AD diagnosis was 3.5 years (range, 1–14 years) and 1.4 years (range, 0–9 years), respectively. At inclusion, 52.8% of patients were on psychoanaleptics, including rivastigmine (17.0%), donepezil (9.4%), galantamine (5.7%), and memantine (7.5%). The mean (SD) screening MMSE score was 20.4 (3.5); the mean (SD) ADAS-Cog total score and comprehension sub-score were 21.7 (7.8) and 1.2 (1.0), respectively; the mean (SD) TMT B execution time was 203.9 (82.4) s; and the mean (SD) forward verbal span score was 5.2 (1.1).
Safety and tolerability
The safety population was composed of the 50 patients who had received at least one treatment session (26 in the PBM group and 24 in the sham group). During the study, 36 AEs were recorded for 22 patients (44.0%), 13 (50.0%) in the PBM group and nine (37.5%) in the sham group, without any statistically significant differences between the treatment groups (Table 3). The most commonly reported AEs were nasopharyngitis (4.0%), post-prandial hyperglycemia (4.0%), and falls (4.0%). Although these AEs were experienced by patients in the PBM group, the study investigator declared that none of it was related to the treatment administered by the investigational medical device. All reported AEs were of mild or moderate severity (data not shown), and no serious AEs was reported.
Summary of AEs and most commonly reported AEs according to treatment group (Safety population, N = 50)
[a] Patients with at least one AE (%) [number of events]. [b] AEs occurring in 4% or more of participants. *χ2 test. **Fisher’s exact test. AE, adverse event; PBM, photobiomodulation.
One patient (4.2%) of the sham group experienced an AE (headache, grade 2), which led to their withdrawal from the study. Two patients (one in the PBM group and one in the sham group) experienced three AEs (epistaxis twice and post-treatment session headache, all grade 1) and one AE (headache, grade 2), respectively, which were declared to be related to the investigational medical device by the study investigator.
The analysis of vital signs and biological parameters did not raise any safety concerns during the course of the study (data not shown).
Compliance with treatment
As shown in Table 4, patients in the analysis population attended a median number of 37.0 treatment sessions (range, 1–40) during the study, resulting in a median participation rate of 92.5% (range, 3–100). The majority of the patients (76.0%; N = 38) underwent between 30 and 39 sessions, eight patients (16.0%) attended the 40 planned treatment sessions, and seven patients (13.2%) attended less than 10 sessions (missing values indicate patients who did not attend any sessions).
Compliance with treatment, according to treatment group (Analysis population, N = 53)
[a] Participation rate (%) = 100 * number of attended sessions/number of planned sessions (i.e., 40). [b] Very good compliance: participation rate ≥75%; Good compliance: 60% ≤ participation rate <75%; Poor compliance: participation rate <60%. *Fisher’s exact test. **Two-sided Wilcoxon-Mann-Whitney test. PBM, photobiomodulation.
Treatment compliance was thus defined as “very good” for 92% of the patients (N = 46) and ‘poor’ for the remainder (8%, N = 4). No significant differences were observed between the treatment groups.
Efficacy outcomes
The main efficacy outcomes are presented in Fig. 3. The reduced sample size observed in some efficacy assessments has to be considered when interpreting the results.
Changes from baseline over time in the ADAS-Cog total score – the primary efficacy outcome of the study – showed no statistically significant difference in the mean [SD] change from baseline to V3 (0.9 [4.9] versus 1.9 [4.1]) and to V4 (0.3 [4.9] versus 1.5 [5.7]) in the PBM group compared to the sham group, respectively (Fig. 3A). However, change from baseline in the ADAS-Cog comprehension sub-score showed a statistically significant difference at V3 between the treatment groups, in favor of PBM (mean [SD] change from baseline of –0.4 [0.9] versus 0.3 [0.9], p = 0.029) (Fig. 3B).
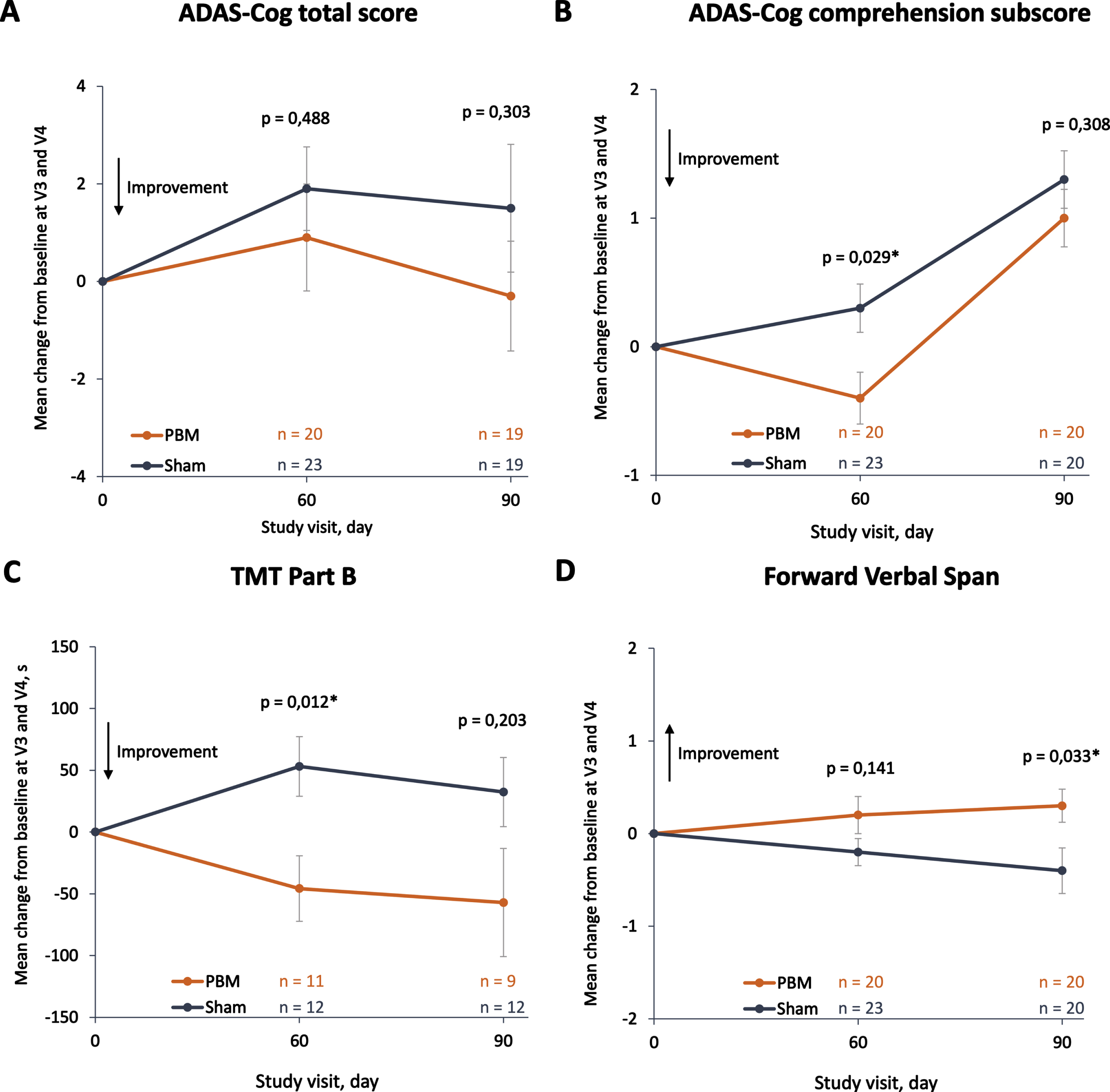
Efficacy outcomes according to treatment groups (Analysis population, N = 53). Mean changes from baseline to V3 (D60, end of treatment) and V4 (D90) between PBM group and sham group in (A) ADAS-Cog total score, scored from 0 to 70 with higher scores indicating normal cognitive functions; (B) ADAS-Cog comprehension sub-score, scored from 0 to 5; (C) TMT part B execution task in seconds; and (D) forward verbal span, where the score is the number of correct responses. Error bars indicate the standard error of the mean. p-values were calculated with the Student’s t-test or Wilcoxon-Mann-Whitney test, with a significance threshold defined at 5%. ADAS-Cog, Alzheimer’s Disease Assessment Scale-cognitive Subscale; PBM, photobiomodulation; s, second; TMT, Trail Making Test.
Among the other efficacy assessments done in this study, two executive functions and verbal memory tests showed statistically significant differences between the treatment groups. An improvement in the execution time of the TMT task B between baseline and V3 was observed in the PBM group compared to the sham group (mean [SD] respective change of –45.8 [88] sec versus 53.1 [83.8] sec, p = 0.012) (Fig. 3C). Even if it was not statistically significant, this difference was also observed at V4 (mean [SD] respective change of –57.4 [131.3] sec and 32.4 [97.0] sec, p = 0.203). No significant differences were observed in the execution time of the TMT task A between the treatment groups (data not shown). The change from baseline to V4 in the forward verbal span score demonstrated a statistically significant difference between the PBM group and the sham group, in favor of the PBM treatment (mean [SD] respective change of 0.3 [0.8] sec and –0.4 [1.1] sec, p = 0.033) (Fig. 3D). No statistically significant differences were observed between the treatment groups in the backward verbal span score (data not shown).
Efficacy outcomes are described in Table 5.
Evolution of cognitive performance scores between V0 (inclusion) and V3 (D60), by treatment group (Full Analysis Set, N = 53)
Change = score at D60 - score at inclusion. [a] Not performed and incomplete evaluations have been added to missing values. *p-value, Student’s test (Two-sided). **p-value, Wilcoxon-Mann-Whitney test (Two-sided). ADAS-Cog is scored from 0 to 70. ADAS-Cog total score at V0 of patient #15 was manually changed from 26 to 21 following an error in data reporting not detected during the monitoring process. Comprehension score is a sub-score from ADAS-Cog. MMSE is scored from 0 to 30. Forward verbal spans scores are the number of correct responses. TMT B score is the time (in seconds) to perform the tasks. ADAS-Cog, Alzheimer’s Disease Assessment Scale-cognitive Subscale; MMSE, Mini-Mental State Examination; TMT, Trail Making Test; PBM, Photobiomodulation; NS, not significant; Q1, first quartile; Q3, third quartile; SD, standard deviation.
DISCUSSION
The present study aimed to evaluate the safety, feasibility, and efficacy of PBM in mild-to-moderate AD patients. The PBM therapy was proven to be safe with regard to the number of patients who experienced AEs (N = 22, 44%), which was balanced between the PBM and sham groups. The majority of reported AEs were not severe, with no serious AEs being reported during the course of the study. AEs reported as related to the investigational device by the investigator (N = 2, 4.0%) included post-treatment session headaches, which is probably due to the ergonomic design of the helmet. Only one patient from the sham group experienced an AE that led to an early withdrawal from the study. These results confirm the excellent tolerance profile of PBM treatment.
The treatment protocol was time-consuming and required a strong commitment from the patients, as they were asked to come to the hospital 5 days per week for a period of 8 weeks. Nevertheless, the majority of the patients (92.5%) were highly compliant. Seven patients were declared non-compliant, mainly because of restrictions in the available transportation to the hospital due to the COVID-19 pandemic lockdown. These results confirm the feasibility of this PBM protocol and demonstrate that both patients and medical teams are willing to benefit from and administer this alternative therapy.
Even though no differences were observed in the total ADAS-Cog score (primary efficacy endpoint) and certain outcomes between the PBM group and sham groups, some secondary endpoints show encouraging efficacy trends. Compared to the sham group, patients who received PBM treatment showed an increase in the ADAS-Cog comprehension sub-score and in the forward verbal span score, suggesting improvements in language comprehension and verbal memory. The TMT part B execution time was lower in patients treated with PBM than in those treated with the sham device, suggesting a positive effect of PBM on executive functions. In the PBM group, no significant improvements or positive trends were observed in the MMSE score or any sub-scores. However, in the most recent systematic review, some of the 10 included studies conducted on the use of PBM therapy for patients with dementia described improvements in total MMSE score and sub-scores [48]. These studies were performed on a limited number of patients with different types of dementia. This highlights the need for large-scale randomized controlled clinical trials with AD patients at specific stages.
Study limitations
Our study has several limitations that could explain why the primary efficacy endpoint was not achieved. The sample size, which was already limited due to the pilot nature of the study, had to be reduced due to the premature end of study as a result of the COVID-19 pandemic restrictions. In addition, the goal of the primary efficacy endpoint— a 4-point decline in the ADAS-Cog total score of the intervention group compared to the sham group— was probably too ambitious. This goal was based on results obtained during a Phase III trial that evaluated the efficacy of donepezil versus a placebo. We now expect, however, that this delta should be reduced to 2 to 3 points, to align with the results observed in most of the acetylcholinesterase inhibitor trials [49, 50].
Study strengths and considerations for future studies
Despite these limitations, our study provides unprecedented data on the PBM treatment for AD. First, this is the largest randomized sham-controlled trial that evaluated the safety of, patient compliance with, and efficacy trends in some secondary endpoints of PBM therapy in mild-to-moderate AD patients. A small number of studies on PBM therapy for dementia or AD patients have been published, but those were not sham-controlled and/or were performed with a small sample of patients. Moreover, this study provides valuable insights for the design of the next development phase, which should aim to ensure the safety and demonstrate the effectiveness of the PBM therapy. The photonic technology can still be improved for greater efficacy, as well as the delivered dose, considering the last publications [51, 52]. Sample size will be significantly increased for more reliable results with greater precision and power. A longer treatment period will be considered, supported by the positive tolerance profile of the device observed during this study’s 8-week treatment period. A 6-month treatment period could allow for a comparison of the effects of PBM treatment with those of acetylcholinesterase inhibitors, for which the mean treatment duration in clinical trials is usually 26 weeks [49, 50].
In preclinical studies, PBM treatment has been shown to have a positive impact on mouse gut microbiota by reversing bacterial communities in AD mouse models to healthy conditions [31, 53]. The impact of the PBM therapy on microbiota should be investigated through the analysis of bacterial taxa in feces samples from the patients.
Conclusions
The present study demonstrated the tolerability and feasibility of the novel PBM-based treatment for mild-to-moderate AD patients. Despite its reduced statistical power due in part to the premature study termination related to the COVID-19 pandemic, this study also highlights encouraging efficacy trends on certain outcomes. This safe and non-invasive treatment mode constitutes a viable and attractive alternative approach to traditional methods of managing AD patient, with the additional benefit that it could even be administered in the patients’ homes. The present study also provides valuable insights for the design of the next phase trial, which should address the cognitive benefits of the PBM treatment in a larger sample of AD patients. PBM therapy as a disease-modifying treatment could potentially offer a safe, well-tolerated method with medical and economic benefits to treat AD.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the patients and their families for their participation, the entire REGEnLIFE team and Dr. Patrick Lemoine for their support, and all the ICTA PM collaborators who contributed to this study.
This work was sponsored by REGEnLIFE and supported by Bpifrance, Région Occitanie (Occitania region).