
Abstract
Background:
People with mild cognitive impairment (MCI) receive fewer guideline-concordant treatments for cardiovascular disease (CVD) than people with normal cognition (NC).
Objective:
To understand physician perspectives on why patients with MCI receive fewer CVD treatments than patients with NC.
Methods:
As part of a mixed-methods study assessing how patient MCI influences physicians’ decision making for acute myocardial infarction (AMI) and stroke treatments, we conducted a qualitative study using interviews of physicians. Topics included participants’ reactions to data that physicians recommend fewer CVD treatments to patients with MCI and reasons why participants think fewer CVD treatments may be recommended to this patient population.
Results:
Participants included 22 physicians (8 cardiologists, 7 neurologists, and 7 primary care physicians). Most found undertreatment of CVD in patients with MCI unreasonable, while some participants thought it could be considered reasonable. Participants postulated that other physicians might hold beliefs that could be reasons for undertreating CVD in patients with MCI. These beliefs fell into four main categories: 1) patients with MCI have worse prognoses than NC, 2) patients with MCI are at higher risk of treatment complications, 3) patients’ cognitive impairment might hinder their ability to consent or adhere to treatment, and 4) patients with MCI benefit less from treatments than NC.
Conclusion:
These findings suggest that most physicians do not think it is reasonable to recommend less CVD treatment to patients with MCI than to patients with NC. Improving physician understanding of MCI might help diminish disparities in CVD treatment among patients with MCI.
INTRODUCTION
Mild cognitive impairment (MCI) is common, affecting up to 1 in 5 older adults (65+) and more than 5 million older Americans [1]. Although patients with MCI have an elevated dementia risk (3–15% per year) [2], many of them remain stable or revert to normal cognition (NC) (15–55%) [3]. Many patients with MCI live years, an average of 10 years in one study, with good quality of life and face competing health risks of aging, like cardiovascular disease (CVD) [4–6].
CVD, which includes both cardiac disease and stroke, is a leading cause of death and morbidity in older adults with MCI and NC. However, evidence suggests that patients with MCI are less likely than patients with NC to receive guideline-concordant, effective treatments for CVD and other health conditions [7–11]. However, patients with MCI want to receive the same treatments as patients with NC [12]. The reasons that patients with MCI receive fewer guideline-concordant CVD treatments than patients with NC are uncertain. Although we know physicians recommend fewer CVD treatments to patients with pre-existing dementia, it is unclear how pre-existing MCI influences physician recommendations for CVD treatments [13–15]. However, preliminary evidence suggests physicians frequently recommend less treatment in general to patients with MCI compared to those with NC, and some physicians conflate MCI and dementia in practice [16, 17]. Based on these findings, one potential explanation for patients with MCI receiving fewer effective treatments for CVD is that physicians recommend fewer CVD treatments to patients with MCI than to patients with NC [17, 18], similar to their undertreatment of patients with dementia. Our focus on CVD allowed our team to limit the scope of our study to examine more closely the influence of patient cognition on physician decision making for treatment.
We conducted a multi-center, descriptive qualitative study of physicians across three specialties to explore the influence of patient MCI on physician decision-making and recommendations for guideline-concordant CVD treatments. We asked physicians to reflect on the pilot data suggesting that older adults with MCI receive or are recommended fewer CVD treatments than those with NC and explain why physicians might recommend less treatment to patients with MCI [17].
METHODS
Study design
We conducted a descriptive qualitative study using in-person, semi-structured interviews [18]. These interviews were part of a larger mixed-methods study that looked at the influence of patient MCI on physician CVD treatment recommendations as well as patient and surrogate preferences for CVD treatment [10, 17]. Using criterion sampling [19], we recruited physicians in the specialties of cardiology, neurology, and general medicine (internal medicine, family medicine, and geriatrics). We chose these specialties because these three specialties care for most cases of acute myocardial infarction (AMI) and acute ischemic stroke (AIS) which are the leading CVD contributors to death and disability, as well as the focus of the larger study [12, 18]. Additionally, we only included physicians that provided inpatient care at least part of the time to limit our sample to those physicians who likely provided care for these acute CVD events like AMI or AIS. First, the Principal Investigator (DAL) recruited by email and telephone physician champions in each of the three specialties from three hospital systems and affiliated private practices outside the research team’s institution in the state of Michigan. We did not include physicians at our institution because they might have been exposed to our pilot study on the topic [16, 17]. Then, the physician champions contacted attending and fellow physicians in their specialties by email and telephone. Once eligible physicians expressed interest to the physician champions in being contacted by our study team, a member of our team would attempt to recruit and consent the physician. We required participants to be board certified and provide inpatient care at least part of the time. We aimed to interview a minimum of 3 physicians in each specialty at each site. Physician champions received consulting fees at $1,000/day. Physicians participating in the study received $100 after completing the interview. The University of Michigan Institutional Review Board approved the study.
Data collection
A trained qualitative research consultant (CDK) conducted the interviews either in-person or by videoconference. Interviews took place at physicians’ offices. The interviewer’s occupation was qualitative research consultant (CDK) at the time of the study [20]. The interviewer did not know the physician participants before study onset. The participants’ knowledge of the interviewer was limited to knowing their occupation, the reasons for doing the research, and the purpose of the interview. The interviewer told participants that they were a qualitative research consultant and not a medical professional. Another member of the research team was present to take notes. The interview duration was approximately 60 minutes.
The interviewer used one of two standard guides (Supplementary Material), one of which was designed for neurologists and generalists and focused on AIS treatments while the other, which was designed for cardiologists and generalists, focused on AMI treatments. In both cases, the interviewer began with reading definitions of MCI and dementia, “mild cognitive impairment or MCI is defined as objective cognitive impairment that is not severe enough to cause significant difficulties with activities of daily living. In a typical older adult with MCI, his family reports mild difficulty remembering recent conversations, dates, and appointments. He functions independently. He does not require help with dressing, bathing, grocery shopping, or taking medicines, but he uses reminders more. In contrast, dementia is defined as objective cognitive impairment that is severe enough to cause significant difficulties with activities of daily living. In a typical person with early-stage dementia, his family reports moderate difficulty remembering recent conversations, dates, and appointments. He is not able to function independently. He requires help with one or more of: dressing, bathing, grocery shopping, or taking medicines. While the distinction between MCI and early-stage dementia can be fuzzy at times, please try to distinguish between MCI and dementia in our conversation as best as you can” [18].
Then the interviewer shared data from previous studies regarding treatment differences between patients with MCI and NC that were not explained by differences in patient or hospital factors. The study data in the cardiology interview included the following finding: older patients with MCI prior to AMI were less likely than patients with NC to receive cardiac catheterization, percutaneous coronary intervention (PCI), coronary artery bypass graft surgery, and cardiac rehabilitation after AMI [7]. Study data in the neurology interview included the following findings: neurologists recommended fewer treatments for AIS to older clinical vignette patients with pre-existing MCI and even fewer treatments to older patients who had early-stage dementia compared to those with NC [21] and neurologists were less likely to recommend carotid endarterectomy, carotid stenting, or inpatient rehabilitation after stroke to older clinical vignette patients with pre-existing MCI and early stage dementia compared to those with NC [17]. Both the cardiology and neurology interview asked participants to react to the following finding: cardiologists and neurologists asked older clinical vignette patients with MCI for their preferences for AMI and AIS treatments less frequently than those with NC [17]. Participants were asked whether they agreed or disagreed with the physicians and to postulate why patients with MCI received or were recommended fewer CVD treatments. Specific interview questions and visual aids provided during the interviews can be found in Figs. 1 and 2.
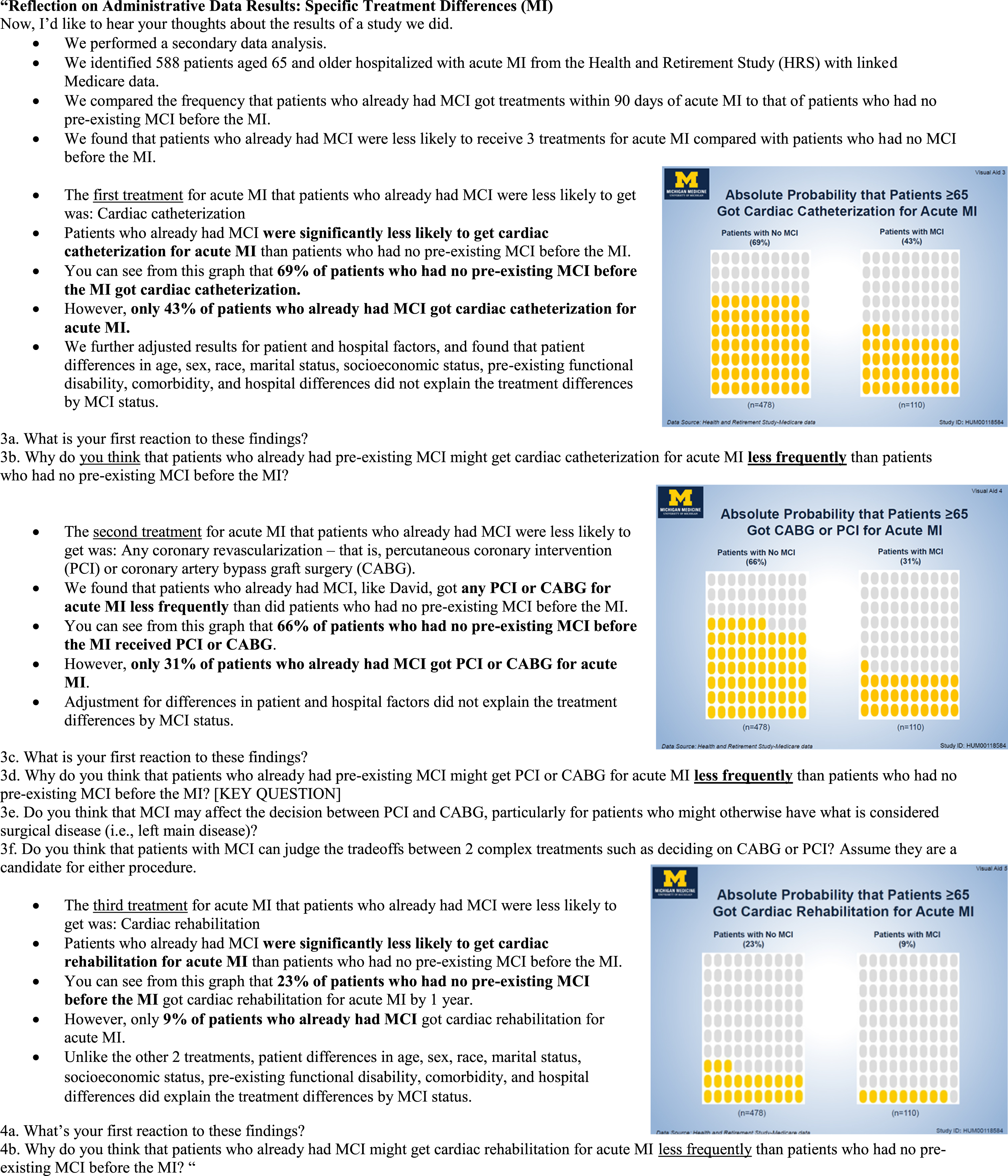
Excerpts from the cardiology interview guide showing the key questions and visual aids.
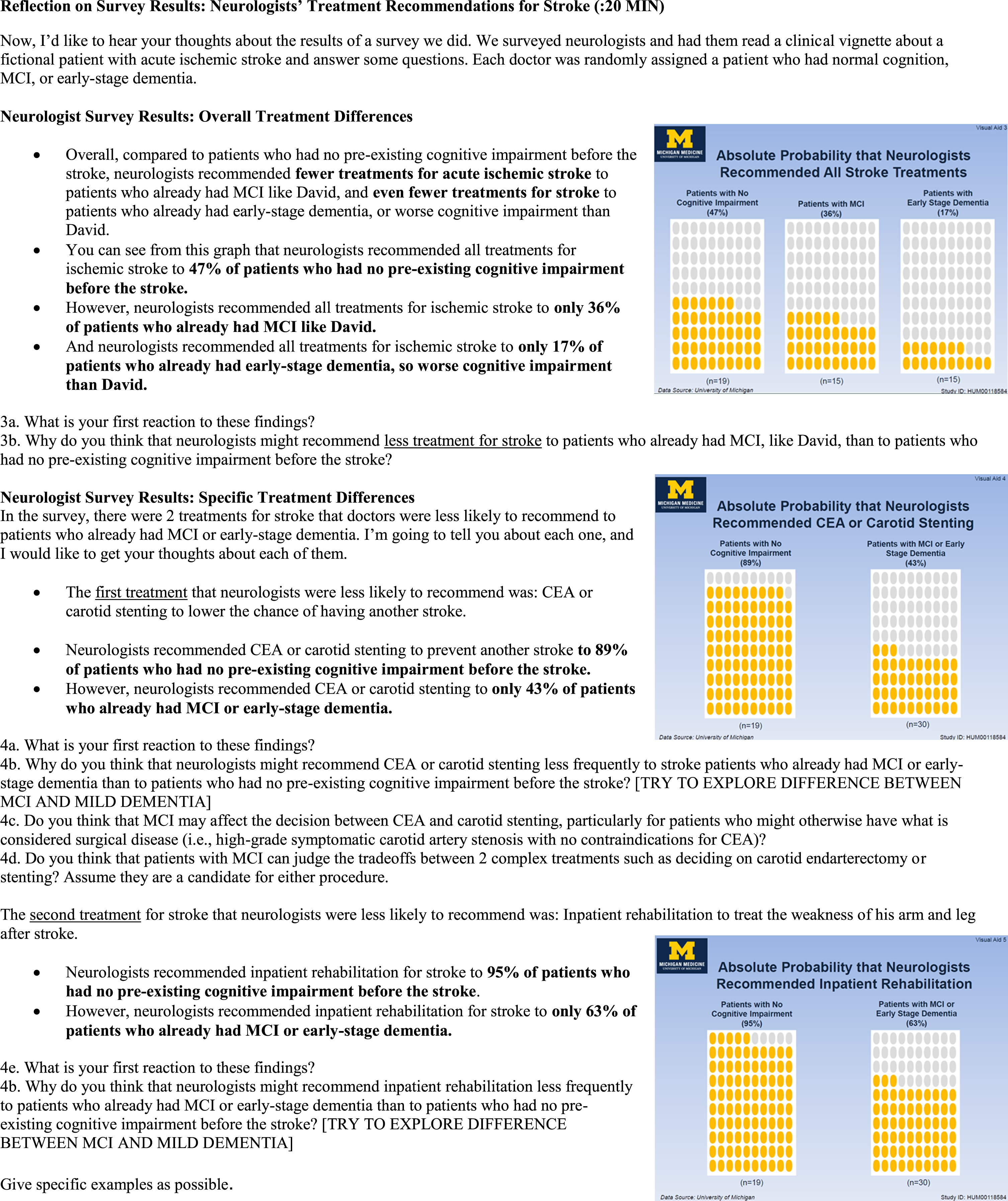
Excerpts from the neurology interview guide showing the key questions and visual aids.
All interviews were audio recorded, professionally transcribed, de-identified, and uploaded into the Dedoose web application (Dedoose Version 8.0.35, 2018, https://www.dedoose.com/).
Data analysis
We used a descriptive qualitative methodology grounded in a naturalist philosophy, wherein the goal is to be “data-near,” reporting findings in their everyday terms, rather than more highly theorized [22]. The underlying epistemology is pragmatist, which emphasizes the “practical meaning of knowledge in specific contexts” and largely subjectivist, that is, the belief that knowledge of reality is socially constructed by participants and researchers [23, 24]. We accepted data as representing our participants’ subjective perceptions and saw our role as researchers as co-constructing knowledge (through interaction with participants and influencing the analysis process), and as using our skills to describe the phenomenon based on our interpretations of participants’ perceptions as described by them. This approach supports our goal of producing concrete findings for real-world practice [23].
We identified unifying and recurrent themes using qualitative content analysis [25]. The analysis team consisted of a vascular neurologist (DZ), internal medicine physician (DAL), qualitative researchers (JF, CK), and study staff (BKR, EMB). We used an inductive approach, identifying and refining codes through independent review of transcripts and team discussion. To ensure coding reliability, each coder, prior to coding transcripts independently, coded a subset of transcripts and achieved a kappa score of ≥0.80 compared to a “gold standard” sample of interview excerpts that had been coded by the senior project manager (BKR) and senior author (DAL) using a consensus process. To maintain coding reliability throughout the coding process, one third of transcripts were coded by two coders and the entire analysis team discussed discrepancies in bi-weekly meetings. In the second stage, after coding was complete, the team reviewed the data organized under each code and developed themes and sub-themes in each domain through discussion. For example, when coding participant reactions to physicians giving less treatment to patients with MCI than patients with NC, we organized the reactions into two themes: “participants thought treating patients with MCI less than patients with NC is unreasonable” and “participants thought treating patients with MCI less than patients with NC is reasonable.”
RESULTS
Of 77 eligible physicians, 31 provided physician champions permission to be contacted by our study team. Of these 31 contacted physicians, 22 completed the interview (eight cardiologists, seven neurologists, and seven primary care physicians). All participants were board certified and 36% of the participants reported having a family member or friend with dementia. Table 1 presents additional participant characteristics. Figure 3 presents the recruitment diagram. We stopped data collection after 22 interviews because thematic saturation was achieved, meaning that no further themes were revealed through continued interviews.
Physician participant demographics
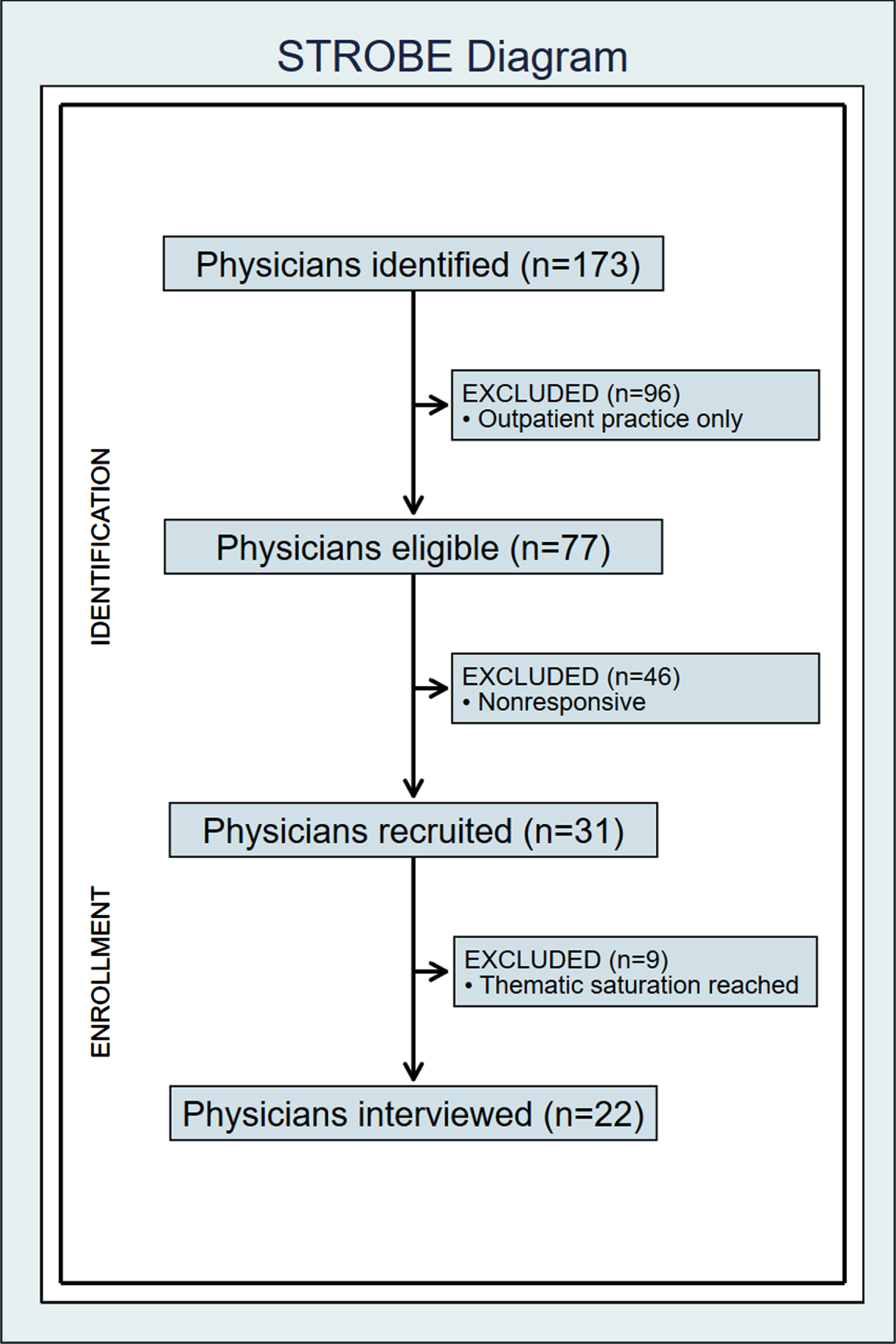
Physician recruitment diagram
Participants had two reactions to the data showing that patients with MCI receive or are recommended fewer treatments for CVD than patients with NC. Most participants showed negative reactions to the data or thought recommending fewer CVD treatments to patients with MCI than to patients with NC is unreasonable. Fewer participants thought recommending fewer CVD treatments to patients with MCI than to patients with NC could be considered reasonable.
More than half of the participants showed strong negative reactions toward the treatment disparities between patients with MCI and NC. Many stated that all patients, regardless of cognitive status, should be treated the same. One participant said, “I’m shocked, actually. And my thought would be those neurologists are setting that patient up, those with mild cognitive impairment or early-stage dementia, basically signing them up for nursing home care for the rest of their life.” In contrast, some participants thought that it may be reasonable that physicians recommended fewer CVD treatments to people with MCI, noting ideas like, “We’re not usually as aggressive in terms of recommending acute treatment or prevention treatment to someone with dementia as opposed to someone with no cognitive impairment.”
Why might physicians recommend less treatment for AMI and stroke to patients with MCI than patients with NC?
We categorized our participant responses into 4 themes that represented potential reasons that physicians might recommend less AMI and stroke treatments to patients with MCI compared to patients with NC. Patterns of the 4 themes appeared in interview transcripts in all three physician specialty groups, across individual CVD treatments, and among physicians who both agreed and disagreed with the AMI and stroke treatment differences. Representative quotations from the physician interviews are in the text and Table 2.
Interview themes and representative quotes
The 4 themes or reasons that participants thought it might be reasonable for patients with MCI to be treated for AMI and stroke less than patients with NC were: 1) Physicians may believe patients with MCI have worse prognoses than do patients with NC, 2) Physicians may believe that patients with MCI are at higher risk of treatment complications than patients with NC, 3) Physicians assume that patients’ cognitive impairment might hinder their ability to consent or adhere to treatment, and 4) Physicians may think that patients with MCI benefit less from treatments than patients with NC. We will present these themes in order of frequency of reporting with the most common one first. Representative quotes are presented in the text or Table 2.
Physicians may believe patients with MCI have worse prognoses than do patients with NC
Nearly three quarters of participants thought that physicians may expect that patients with MCI have poorer prognoses (shorter life expectancy, worse quality of life, and more cognitive decline) compared to patients with NC. A majority of participants postulated that physicians might assume patients with MCI have worse outcomes after CVD events than patients with NC. Some participants stated that physicians might assume that patients with MCI might not live as long or experience the same quality of life as patients with NC. One participant remarked that for patients with MCI, “I would imagine [physicians] think life expectancy and quality of life is less.”
Physicians may believe that patients with MCI are at higher risk of treatment complications than patients with NC
About two-thirds of participants reported that physicians might recommend fewer AMI and stroke treatments to patients with MCI because physicians assume that patients with MCI have a higher risk of treatment complications than patients with NC. Additionally, participants postulated that patients with MCI might be more likely than patients with NC to have comorbidities, like diabetes, that increase overall treatment risks. Six out of eight cardiologists and five out of seven primary care physicians interviewed felt that greater comorbidity may help explain why patients with MCI receive fewer treatments, while only three out of seven neurologists noted this as a possible explanation. Participants expressed concern that patients with MCI might be at higher risk of worsening cognitive status than patients with NC as a complication of the treatment. Some participants postulated that certain treatments (e.g., coronary artery bypass graft surgery) could trigger delirium or conversion to dementia in patients with MCI. One participant reflected, “People might be more worried about complications related to dementia and the pathophysiological process that happens in the brain, and could they be at higher risk complications related to treatments...”
Physicians assume that patients’ cognitive impairment might hinder their ability to consent or adhere to treatment
More than half of participants thought that physicians might assume patients with MCI are less able or less likely to adhere to AMI and AIS treatments and this assumption was a factor in physicians’ decisions to recommend fewer treatments. A participant noted, “Probably the physicians would be thinking that they will not be trusted with their compliance to medications. So, that’s why they will try a less invasive approach. They would think that this is an old patient, who has mental disabilities, so, is not sure about his compliance.” This concern about patient adherence impacting treatment recommendations may have been more common in cardiologists (5/8) than neurologists (3/7) and primary care physicians (3/7). In addition to adherence issues, participants thought that physicians might assume that patients with MCI are not capable of consenting for treatment. Over 40% of participants noted that physicians may assume that patients with MCI are unable to consent for treatment, with comments such as, “Maybe they think that the patient doesn’t understand what they’re consenting for.” Additionally, many participants thought physicians might assume that patients with MCI are more likely to miss follow up appointments than patients with NC, perhaps conflating patients with MCI with patients with dementia. A primary care physician stated, “Well, because they have dementia and they are easy to forget their appointments and easy to have a lack of support system or a lack of resources, or maybe, you know, say the patient is supposed to call or arrange for their ride, and you know the patient might have forgotten to do this.”
Physicians may think that patients with MCI benefit less from treatments than patients with NC
Most participants postulated that physicians may assume that patients with MCI receive less benefit from AMI or AIS treatments than patients with NC. One participant rationalized that, “As the patient’s baseline function status goes down, the likelihood that they benefit from a certain treatment goes down.” Others noted that the perceived lack of treatment benefit may have played a part in physicians recommending fewer treatments to patients with MCI than to patients with NC.
DISCUSSION
Most participants showed negative reactions to the data or thought recommending fewer CVD treatments to patients with MCI than to patients with NC is unreasonable. Fewer participants thought recommending fewer CVD treatments to patients with MCI than to patients with NC could be considered reasonable. Reasons that physicians might undertreat CVD in patients with MCI, as postulated by the participants, fell under 4 main categories: 1) Physicians may believe patients with MCI have worse prognoses than do patients with NC, 2) Physicians may believe that patients with MCI are at higher risk of treatment complications than patients with NC, 3) Physicians assume that patients’ cognitive impairment might hinder their ability to consent or adhere to treatment, and 4) Physicians may think that patients with MCI benefit less from treatments than patients with NC.
Our results suggest that, although participants do not think it is reasonable to recommend less treatment to patients with MCI, common misconceptions about the MCI diagnosis may exist among physicians and contribute to potential undertreatment of CVD. Physicians may have several misconceptions around the meaning of an MCI diagnosis. Participants in our study stated that physicians might believe that patients with MCI have worse prognoses, experience greater risk from treatments, difficulty adhering to and consenting treatment, and benefit less from treatment than patients with NC. These assumptions may explain why physicians might recommend less guideline-concordant treatment for CVD to patients with MCI than patients with NC. Although clinicians assume that older patients with MCI have a limited life expectancy and inevitably progress to dementia [16, 17], some older patients with MCI live up to a decade on average and AD/ADRD is not inevitable, as many patients remain stable and others revert to NC [2, 26]. Although physicians might have observed that patients with MCI have worse outcomes after AMI and stroke in their practice, the prognoses of older patients with MCI after AMI and stroke are unclear because there is not a good evidence base in the literature. There is a scientific need for prognostic models to estimate the impact of MCI on AMI and stroke outcomes in older patients. Filling physician knowledge gaps with such modeling would help address common misconceptions about MCI and help inform physician decision making in practice.
Our results align with previous research that suggests physicians recommend post-stroke rehabilitation for patients with dementia and pre-existing cognitive impairment less often than for patients with normal cognition [27]. This is due to physician belief that patients with cognitive impairment would benefit less from the rehabilitation than other patients [27]. In this study, physicians noted that they may be more likely to recommend post-stroke rehabilitation to patients with cognitive impairment if the rehabilitation could be adapted to those patients’ needs, for example with longer timescales, to improve the chances of patient success. These findings, paired with the results of our study, suggest a need for more patient-centered, guideline-concordant care for older adults with MCI and dementia.
Our study has several strengths. The sample included a racially diverse group of male and female physicians who had a range of ages. We included early-career physicians still in training (fellows) and later-career attending physicians. Participants practiced in a range of settings, including academic, community-based, private, or Veterans Health Affairs settings. We continued interviews until we achieved thematic saturation. Although we kept our sample to three specialties (cardiology, neurology, and general medicine), our sample included physicians with a wide range of clinical experience. The neurologist group included some physicians with specialized training in cognition, and the primary care group included some physicians in internal medicine, geriatrics, and family medicine. Participants’ perspectives from varied demographic groups, career stages, settings, and clinical specialties contributed to the data’s scope and richness.
Our study has limitations. We did not capture the perspectives of physicians in all specialties that care for older adults with MCI. Nevertheless, participants were in three of the most common specialties that care for the population with or at risk for MCI. We did not collect information on neurology subspecialty of participants; however, we did not exclude any neurology subspecialties during recruitment. We did not have a sufficient sample size to rigorously assess differences in perspectives by specialty and hospital; however, our analysis emphasized common themes across specialties. We do not have information on the characteristics of the nine physicians who were eligible for the study but not interviewed, therefore, those who completed the interviews might be different from those who did not. However, all 31 recruited physicians were volunteer participants and the 22 who completed the interview were simply able to schedule the interview at an earlier date. We found no evidence that the distribution of the three physician specialties differed between the group of 22 physicians who participated and the group of 9 physicians who did not (p = 0.33 using Fisher’s exact test). Although physicians with academic affiliations may differ from those without academic ties, it is plausible that physicians in the two groups have comparable experiences caring for older adults with MCI. The source data shown in the visual aids indicated that one treatment difference between older adults with MCI and those with normal cognition (cardiac rehabilitation) may have been explained by patient factors (e.g., older age, greater comorbidity, worse functional status more common in those with MCI) [7]. However, our participants in this qualitative study were still able to provide their perspectives on why treatments may have been different in those with MCI, and therefore this finding from our prior work is unlikely to impact our current findings.
Having a greater understanding of how physicians view MCI and the role these perspectives play in their clinical decision making carries valuable implications for the care of older adults and the training of providers about MCI. Our results suggest that incorrect physician assumptions might contribute to older patients with MCI being undertreated for CVD. Identifying physician misconceptions about the MCI diagnosis is pivotal in improving the CVD care patients with MCI receive. This is important because older patients with MCI do not want less treatment for AMI and stroke than those with NC [12]. Older patients with MCI and their care partners want to participate in AMI and stroke treatment decisions [12]. Improving physician education on the MCI diagnosis and the preferences of MCI patients could help address the treatment disparity between patients with MCI and NC. Previous studies have shown that physicians may conflate MCI and dementia in practice [18]. It is possible that this conflation leads to physicians offering less care to patients with MCI, as physicians frequently offer less care to people with dementia [14]. Therefore, ensuring that physicians have proper training in distinguishing between the two diagnoses could help reduce undertreatment in patients with MCI. Decision support tools are also potential strategies to improve the quality of care and reduce the impact of physician misconceptions on physician behavior [28, 29]. We need to optimize educational curriculums and create decision support systems that help providers deliver guideline-concordant, patient-centered care to older patients with MCI suffering CVD events, like AMI and stroke, and other diseases.
Conclusion
Many physicians believe it is unreasonable for patients with MCI to receive less guideline-concordant treatment for CVD than patients with NC. Despite this, physician participants were able to provide potential justifications for why other physicians recommend less treatment to patients with MCI. Physicians may believe that patients with MCI have worse prognoses, face greater risks from treatments, are less likely to comply with treatment, and benefit less from treatments compared to cognitively normal patients. This suggests that physicians might have common misconceptions about what an MCI diagnosis means about a patient’s prognosis and risk of treatment. These beliefs may lead physicians to recommend fewer CVD treatments to patients with MCI.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0495r1).