
Abstract
Background:
Pathological and clinical features of Alzheimer’s disease (AD) are in temporal discrepancy and currently accepted clinical tests provide the diagnosis decades after the initial pathophysiological events. In order to enable a more timely detection of AD, research efforts are directed to identification of biomarkers of the early symptomatic stage. Neuroinflammatory signaling pathways and inflammation-related microRNAs (miRNAs) could possibly have a crucial role in AD, making them promising potential biomarkers.
Objective:
We examined the expression of circulatory miRNAs with a documented role in AD pathophysiology: miR-29a/b, miR-101, miR-125b, miR-146a, and miR-155 in the plasma of AD patients (AD, n = 12), people with mild cognitive impairment (MCI, n = 9), and normocognitive group (CTRL, n = 18). We hypothesized that these miRNA expression levels could correlate with the level of participants’ cognitive decline.
Methods:
The study participants completed the standardized interview, neurological examination, neuropsychological assessment, and biochemical analyses. miRNA expression levels were assessed by RT-PCR.
Results:
Neurological and laboratory findings could not account for MCI, but miR-146a and -155 were upregulated in the MCI group compared to the control. miR-146a, known to mediate early neuroinflammatory AD events, was also upregulated in the MCI compared to AD group. ROC curve analysis for miRNA-146a showed 77.8% sensitivity and 94.4% specificity and 66.7% sensitivity and 88.9% specificity for miR-155.
Conclusion:
Determination of circulatory inflamma-miRs-146a and -155 expression, together with neuropsychological screening, could become a non-invasive tool for detecting individuals with an increased risk for AD, but research on a larger cohort is warranted.
INTRODUCTION
Life expectancy has doubled in the world since the beginning of the 20th century, leading to an increased incidence of Alzheimer’s disease (AD), as a disease of the elderly. AD is responsible for 60–70% of all dementia diagnoses [1]. Ninety-five percent of patients diagnosed with AD are sporadic cases and remaining 5% have familial gene mutations [2]. Among people who are 65 years and older, 10% are thought to have this progressive and ultimately fatal neurodegenerative disorder [1]. This global, increasing trend of AD is independent of their socio-economic status, and the financial burden due to AD is in range of cardiovascular diseases and carcinoma [3]. These facts identify AD as an insufficiently recognized problem, making the biomedical research in the dementia field a priority. In that regard, timely detection and slowing down of the disease course are of critical importance.
Difficulty of AD identification in a timely manner lies in the facts that pathological (AD-P) and clinical features (AD-C) of the disease are in temporal discrepancy and that clinical tests provide the diagnosis only when the first symptoms appear. Currently accepted biomarkers have relatively low specificity [4] and enable diagnosis sometimes even a few decades after the cascade of the pathophysiological processes has been initiated [5]. In addition, current treatments only alleviate symptoms, but do not have an effect on the causal mechanism, which has not yet been fully elucidated [6]. AD presents itself as the continuum from asymptomatic disease to dementia [7,8, 7,8] and AD-C typically include incremental loss of memory and cognitive functions, involving the language, visuospatial, and executive domains [9]. However, at the beginning of the AD continuum, around 30% of individuals are estimated to have some level of AD-P, sometimes even significant brain changes, but no apparent symptoms [10]. Recently, the criteria for identification of subtle clinical manifestations prior to the objective evidence, subjective cognitive decline (SCD) due to AD, are structured and proposed as a useful concept [11]. However, there are still inconsistent and heterogeneous findings, regarding their clinical utility [12]. Therefore, the currently accepted diagnostic standard tools for an objective assessment [13] identify patients mainly in mild cognitive impairment (MCI) stage. A possibility of unambiguous clinical identification of this symptomatic AD stage, considered as early phase in the disease trajectory, make MCI a suitable ground for investigation of early pathological processes of the disease. Besides, the available data imply possibility to effectively slow down disease process in MCI stage, since there are cases of MCI which progress to dementia due to AD, but also those who remain stable over time [14]. Therefore, many research efforts are currently directed towards the identification of biomarkers of MCI stage. These biomarkers could not only contribute to the understanding of the early clinical stage itself and slowing down of the disease progress, but they could ultimately lead to AD diagnosis in preclinical stage and development of causative therapeutic modalities.
According to the results of the genetic studies of the early-onset familial forms of AD, irregular amyloid-β (Aβ) metabolism represents the initial molecular mechanism, ultimately leading to both AD-P and AD-C [15]. Currently, there are two biomarkers of extracellular Aβ accumulation: low cerebrospinal fluid (CSF) Aβ [16] and abnormal tracer retention on amyloid positron emission tomography (PET) imaging [17]. In addition, biomarkers of tau pathology [18] and biomarkers of neuronal injury in brain regions typical for AD [19] are also included in AD diagnostic guidelines [17]. The amyloid cascade, which has been proposed as the leading AD mechanism, might be very early pathophysiological event of the disease [20], but it is probably not the primary causative mechanism [21, 22,] and certainly, it does not offer enough explanations of AD pathogenesis alone [23]. Thus, several biological pathways have been proposed as leading mechanisms of AD and MCI [24, 25], and inflammation has emerged as a substantial driver of AD. There are studies that show increased levels of inflammatory markers in AD patients, as well as an association between AD risk genes and innate immune function [25–27]. The importance of inflammation in neurodegenerative processes of AD were observed for the first time 30 years ago, in a study that reported positive effects of chronic anti-inflammatory therapy on decreasing the incidence and progression of AD [28]. Epidemiological studies have also shown positive correlations between dementia and data on previous infection [29]. A number of confirmations followed, based on experimental studies on animal models [30] as well as clinical research [31], but also functional and structural changes in AD brain [32]. Eventually, based on the vast evidence [25–32], neuroinflammation is placed in the focus of the research in AD field, with promising potential to identify biomarkers of early phases of AD.
microRNAs (miRNAs) are small, endogenous, highly conserved, non-coding RNAs that regulate gene expression at the post-transcriptional level through RNA interference [33, 34]. miRNAs have been shown to be involved in fundamental cellular processes such as cell proliferation, differentiation, migration, and apoptosis [35]. A series of studies demonstrated their implication in a variety of human brain dysfunctions involving neuroinflammation and oxidative stress [36]. Specifically, immune- and inflammation-related miRNAs are reported to have possibly crucial role in neuroinflammatory signaling pathways of AD [37,38, 37,38].
Based on a detailed literature review, the analysis of the following circulatory miRNAs was conducted in the present study: miR-29a/b, miR-101, miR-125b, miR-146a, and miR-155. They have a role in the leading pathways of AD, such as: inflammation, oxidative stress, and innate immunity, and also in the specific processes involved in the formation of the abnormal protein deposits¾amyloid plaques and neurofibrillary tangles [39].
The presented study compared miRNA expression profiles in plasma of the three groups of patients: 1) those with AD (AD group), 2) those who subjectively have normal cognitive function, but objective tests show they have mild cognitive impairment (MCI group), and 3) those people who subjectively and objectively have normal cognitive function (CTRL group). In hope to identify future potential biomarkers for early stages of AD, we hypothesized that the expression levels of the selected circulatory miRNAs could correlate with the level of cognitive decline in participants.
MATERIALS AND METHODS
Ethical statement
The study protocol was approved by the Ethical Committee of the Clinical Center of Montenegro (No. 03/01-11417/1) and by the Committee for Medical Ethics and Bioethics of the Faculty of Medicine of the University of Montenegro (No. 3824/4). All the procedures were conducted in accordance with the Declaration of Helsinki.
Participants and group assignment
The present retrospective-prospective, multidisciplinary study enrolled 39 subjects, out of total 51 examined individuals (Fig. 1). They were divided into three groups: 18 healthy controls (CTRL), 9 patients with MCI, and 12 patients with previously diagnosed AD. Written informed consent to participate in the study was obtained from all participants or their legal representatives.
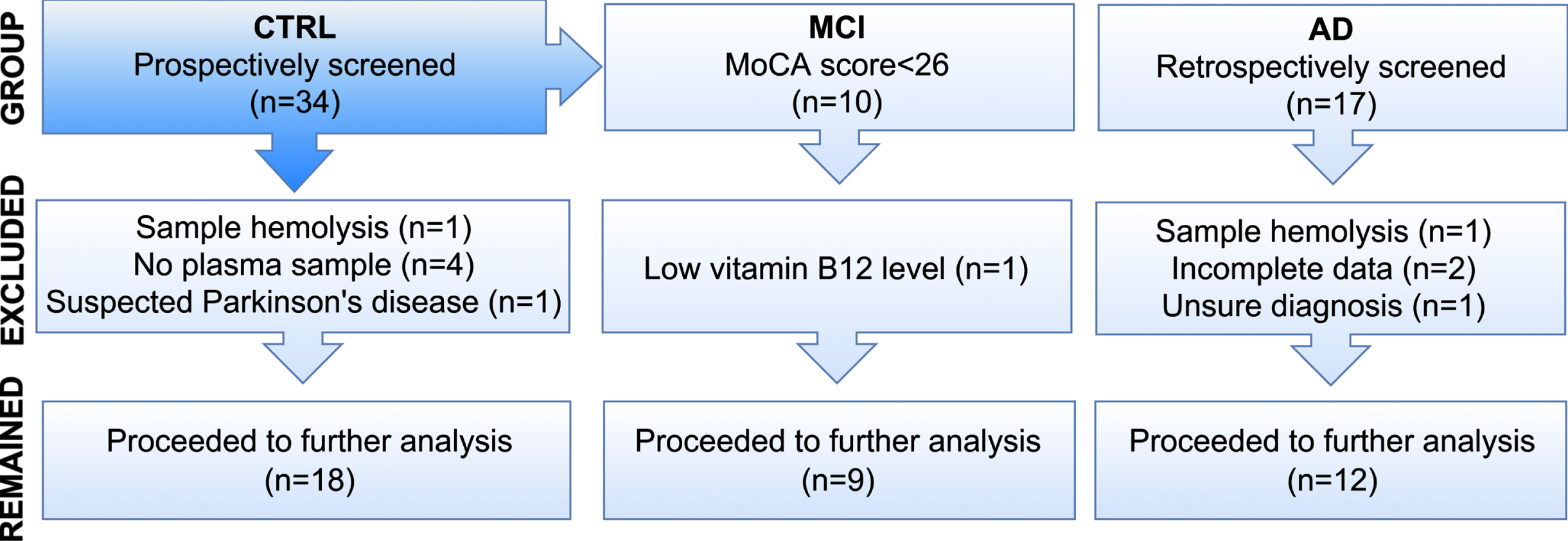
Recruitment process. CTRL, healthy volunteers with normal cognitive function; MCI, healthy volunteers with subjectively normal cognitive function, but with mild cognitive impairment detected by neuropsychological screening; AD, participants diagnosed with AD.
All the participants filled a questionnaire designed to standardize the process of the clinical interview and to obtain comparable demographic and clinical data (Table 1). Subsequently, they underwent the neurological and neuropsychological assessment, as well as peripheral blood sampling, for standard diagnostic and experimental laboratory analyses.
Demographic and clinical features of the examinees
SD, standard deviation; Physical activity, walking≥30 min at least 5 days per week; History of smoking, current or former smokers; Coffee consumption, consumption of 3 or more cups daily; Played music, practicing of any kind of music (playing an instrument, singing, dancing), currently or previously in life.
AD patients were recruited during their regular follow up appointments, at the Neurology Clinic of the Clinical Center of Montenegro. The other two groups of patients were volunteers recruited at the Faculty of Medicine.
For all participants excluding criteria were: presence of neurological disorder (other than AD, for AD group), psychiatric, systemic and poorly controlled chronic diseases, history of drug and alcohol abuse, and current acute illness. The Geriatric Depression Scale-15 (GDS-15) was performed to exclude depressive disorder. Those patients who scored 9 or more points on GDS-15 had major depression disorder and were excluded from the study [40]. In addition, in control subjects, neuropsychological screening test results [Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA)] below 26 were considered as excluding criteria. Nine participants who subjectively did not have cognitive impairment, but their MoCA score was lower than 26 formed a group with MCI. In these participants cognitive impairment was accidentally discovered.
A number of cases were excluded from the study, either because patients met exclusion criteria or plasma samples were inadequate (Fig. 1).
Clinical evaluation
Neurological examination
An interview according to the defined questionnaire, together with neurological examination, was conducted by a neurologist, at the Faculty of Medicine or at the Clinical Center of Montenegro. All the volunteers for the study, including those who denied neurological disorders during an interview, underwent detailed neurological examination, in order to thoroughly select participants for the study and identify exclusion criteria (Fig. 1).
Patients with AD were previously diagnosed at Clinical Center of Montenegro, according to the criteria of the National Institute of Aging and Alzheimer’s Association (NIA-AA) [41]. At the time of the recruitment, they were neurologically re-evaluated for the purpose of research and identification of potential comorbidities defined as exclusion criteria. Results of the laboratory tests were used to confirm the presence of some of the participants’ diseases, self-reported by the participant during the recruitment interview (Table 1).
Neuropsychological assessment
The neuropsychological examination of all participants was conducted by a doctor or a psychologist certified for neuropsychological assessment, which included: short assessment of SCD, MMSE, MoCA, and GDS-15. In AD patients, depression was previously excluded as a differential diagnosis, so the GDS-15 was not performed again.
Although the present study recruited people for the control group, who felt mentally and physically healthy, SCD was assessed through an open question as an additional check. Among the healthy volunteers, several participants unexpectedly had MoCA scores indicating they have an MCI, so they formed an MCI group. MoCA test score was used for the final selection of subjects for MCI group, since literature data consistently confirm its potential for improved detection of MCI and superiority compared to MMSE [42].
Laboratory examination
Biochemical laboratory analyses helped to identify conditions which are among excluding criteria (Fig. 1), or to check parameters of special interest for particular chronic disease of our study participants, which would exclude them from the study (e.g., HbA1 C>10). The following analyses were conducted for each study subject: complete blood cell count, glycemia, lipid status, liver enzymes, urea and creatinine, electrolyte status, thyroid function, folate, vitamin B12, and C-reactive protein as an inflammatory marker.
Analysis of miRNA expression profiles
Sample processing and miRNA extraction
Ten milliliters of peripheral venous blood were collected from each participant into BD Vacutainer® Venous Blood Collection Tubes (cat. No. 367525) containing EDTA. The tubes were kept on ice and processed within 1 h from the blood collection. Plasma was separated from the whole blood by centrifugation at 1.900×g for 10 min at 4°C, followed by an additional centrifugation step at 3.000×g for 15 min at 4°C, to remove remaining cellular nucleic acids attached to cell debris. All samples were aliquoted in RNAse/DNAse-free tubes and stored immediately at –80°C until further analysis. MiRNA was isolated from plasma by using miRNeasy Serum/Plasma Advanced Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. The miRNA concentration was determined using Qubit microRNA Assay Kit (Q32880, Invitrogen, Thermo Fisher Scientific) on a Qubit 3.0 fluorimeter (Q33216, Invitrogen, Thermo Fisher Scientific, USA).
Quantification of miRNAs by RT-PCR
Two μl miRNA from each sample was reversely transcribed to cDNA using TaqMan Advanced miRNA cDNA Synthesis kit (A28007, Applied Biosystems, USA) and analyzed with TaqMan Advanced microRNA Assays (A25576, Applied Biosystems, USA) for miR-29a/b, miR-101, miR-125b, miR-146a, and miR-155. qRT-PCR was run on an Applied Biosystems 7300 Real Time PCR system (Applied Biosystems, USA). The expression levels of target genes were normalized by using the mean expression levels of miR-361-5p gene, selected as the most stable internal control miRNA (between miR-186-5p, miR-1255a, and miR-361-5p) by the NormFinder algorhitm (Andersen CL, Jensen JL, Ørntoft TF). Normalization of real-time quantitative reverse transcription-PCR data: a model-based variance estimation approach to identify genes suited for normalization, applied to bladder and colon cancer data sets [43]. Expression of every target gene was calculated using the 2-ΔΔCt method. Every sample was retrotranscribed twice and run in triplicate each time.
Statistical analysis
All statistical analyses were performed using GraphPad Prism 9.3.1 (GraphPad Software, San Diego, CA, USA) and the statistical software R. The results were considered statistically significant when p < 0.05. Continuous variables were analyzed with the t-test or one-way ANOVA, whereas categorical variables were analyzed with the χ2 test or Fisher’s exact test. Results of all continuous variables were first tested for normality of distribution by D’Agostino-Pearson and Shapiro-Wilk tests. Associations between miRNA expression and clinical variables were explored using Mann–Whitney and Kruskal-Wallis tests, as appropriate. Pearson correlation coefficients were computed as well. Receiver operating characteristic (ROC) curve analysis was done to evaluate all the five selected miRNAs as potential prognostic biomarkers.
RESULTS
Demographic and clinical features of the study participants
A summary of the demographic and clinical characteristics of study participants is given in the Table 1. There was no significant difference in age among the groups. Male and female examinees were almost equally represented in the groups. Participants of all the study groups had on average similar level of education.
As expected, MoCA scores among the groups were significantly different, with the lower values in patients with AD and MCI, compared to subjects in the control group (p < 0.0001, Table 1).
Hypertension, hyperlipidemia, and diabetes mellitus were the most common diseases among the study participants, but their prevalence was not significantly different among the groups. Frequency of habits, like smoking, coffee consumption, regular physical activity, and hobbies related to music, was similar among the groups. None of the participants had history of significant alcohol consumption.
MCI subjects without SCD were accidentally discovered by neuropsychological examination
None of the healthy volunteers in the study reported SCD (Table 2). The percentages of the volunteers with normal cognitive performance and those who scored under 26 on neuropsychological screening tests are given in the Table 2. MoCA and MMSE results were in correlation (r = 0.725; p < 0.01), but MoCA proved to be more sensitive since CI would not be discovered in 22.2% of examinees if they were evaluated by MMSE only (Fig. 2). When compared, MCI and control groups were not significantly different regarding the scores below 9 (p = 0.36730, data not shown).
Cognitive performance of the healthy volunteers

Correlation of Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE) scores of the healthy volunteers.
Neurological examination of the control and MCI groups did not indicate presence of the central nervous system disease. The participants denied history of cerebrovascular or other neurological disease that could cause cognitive decline in the MCI group. Also, biochemical analyses of blood samples showed that none of the volunteers included in the study had thyroid dysfunction, B12 deficiency, severe anemia, acute or poorly controlled chronic condition that could cause cognitive decline.
miR-146a and miR-155 are upregulated in MCI subjects
Using the qRT-PCR method, in the CTRL, MCI, and AD groups, the expression level of the following circulatory miRNAs was determined: miR-29a/b, miR-101, miR-125b, miR-146a, and miR-155. Statistical analysis did not show any significant difference in the expression level of miR-29a/b, miR-101, and miR-125b among the examined groups (p = 0.1512, p = 0.4374, p = 0.3020 respectively, data not shown).
Circulatory miRNA-146a expression levels were found to be upregulated in MCI group, compared to both the CTRL (p = 0.0121) and AD group (p = 0.0089). Expression level of miR-146a in the control subjects, however, was not significantly different from those with AD (p > 0.9999) (Fig. 3A).
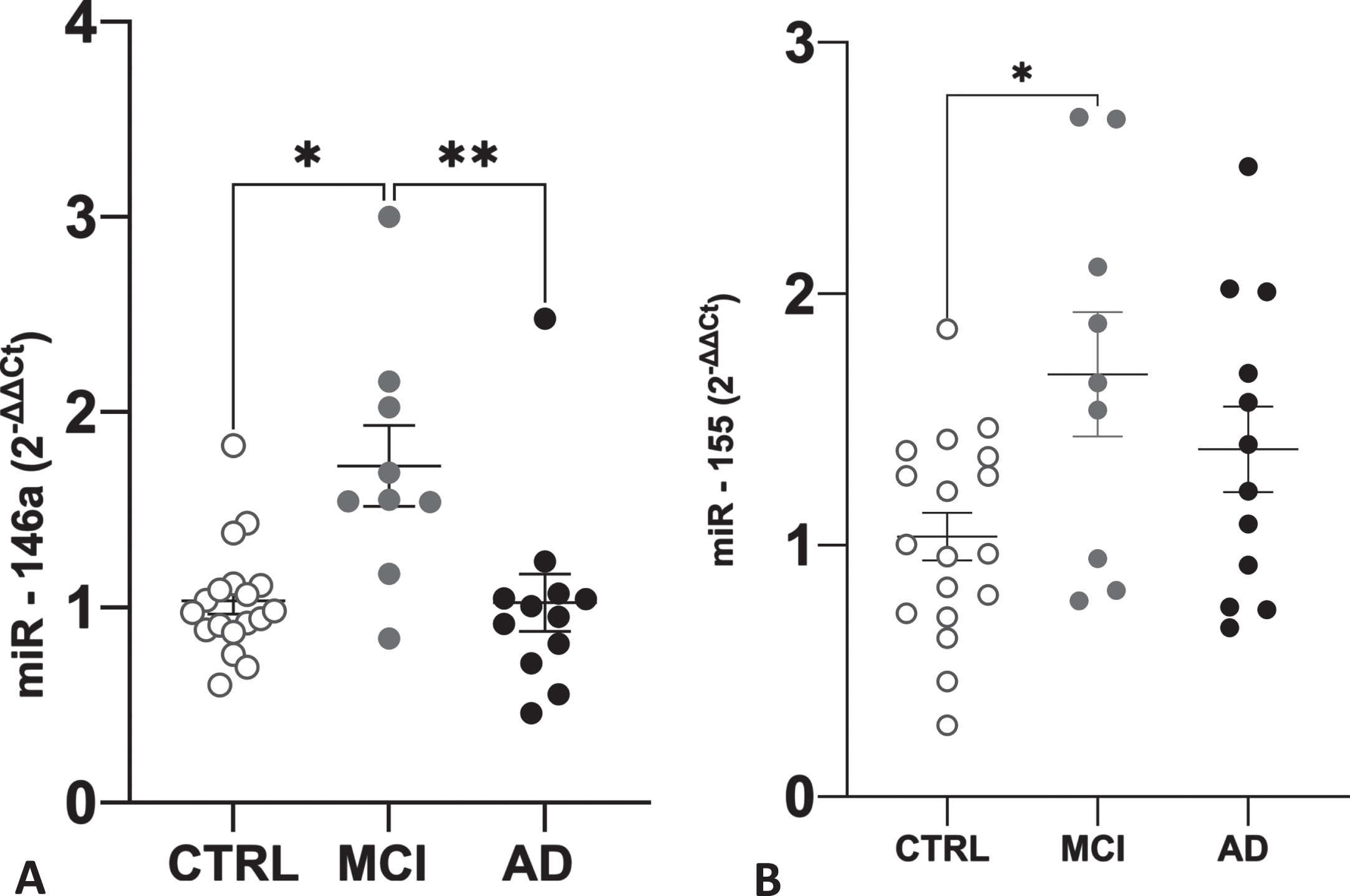
A) Comparison of the circulatory miR-146a expression levels B) Comparison of the circulatory miR-155 expression levels. CTRL, control group; MCI, participants with mild cognitive impairment; AD, patients with Alzheimer’s disease. *p < 0.05, **p < 0.01.
Similar pattern of expression among the groups was found for miR-155. Its expression level was significantly higher in participants with MCI, compared to the CTRL (p = 0.0187), but there was no difference in miR-155 levels between control and AD groups (p = 0.2241).
In order to have a more precise insight in sensitivity and specificity of these miRNAs in discrimination of healthy and diseased individuals and assess their potential to serve as a diagnostic test, ROC curve analysis was performed (Fig. 4A–C). For the miR-146a expression values of control and MCI groups, AUC was 0.8642 (95% MCI, 0.6852–1.0), with 77.8% sensitivity and 94.4% specificity (Fig. 4A), whereas for the data on miR-146a expression in participants with MCI and AD, AUC was 0.8519 (95% MCI, 0.6684-1.000) with 88.89% sensitivity and 83.33% specificity (Fig. 4B). When miR-155 expression level in the MCI and control groups was analyzed, AUC was 0.7654 (95% CI, 0.5474 to 0.9834), with 66.7% sensitivity and 88.9% specificity (Fig. 4C). Therefore, ROC curve analyses showed that both miR-146a and miR-155 had significant diagnostic value and could differentiate MCI from normal controls, and miR-146a could differentiate MCI from AD patients as well.

Receiver operating characteristic (ROC) curve analysis of altered miRNAs. A) ROC for miR-146a in control and MCI groups; B) ROC for miR-146a in MCI and AD groups; C) ROC for miR-155 in control and MCI groups. CTRL, control group; MCI, participants with mild cognitive impairment; AD, patients with Alzheimer’s disease.
Moreover, although the expression of miR-155 was not different between MCI and AD group, the expression levels of miR-146a and miR-155 plotted together on a two-dimensional scatter plot illustrate a unique expression pattern of these selected inflamma-miRs that differentiates those with MCI from healthy individuals and from those with AD (Fig. 5).
miR-146a and miR-155 expression levels are unchanged during the course of manifested AD
Since miR-146a and miR-155 demonstrated the potential for detection of early cognitive impairment (Figs. 3 and 4), we wanted to test whether these miRNAs could also be upregulated earlier in the course of AD (Table 3). To that aim, expression values of miR-146a and miR-155 were compared between the patients diagnosed with AD less than one year before the moment of recruitment and those who had AD for one year or longer. The difference in the expression level was not statistically significant (p = 0.1120, p = 0.8810, respectively, data not shown). The correlation of miR-146a and miR-155 expression level with years of AD duration was not statistically significant (p = 0.7638; p = 0.3027, respectively, data not shown).
Time frame of the disease course in AD patients
Data are presented as mean±standard deviation.
DISCUSSION
The present study enrolled patients with AD and volunteers without subjective cognitive decline, but interestingly, neuropsychological screening tests indicated that 33.3% of the apparently healthy subjects had MCI (Table 2). Neurological and laboratory findings could not explain their neuropsychological performance. However, in MCI group, the two circulatory miRNAs, miR-146a and miR-155, were upregulated compared to the control group of patients. The expression level of miR-146a was also significantly higher in MCI compared to AD group (Fig. 3). In patients with already diagnosed AD, miR-146a and miR-155 were not upregulated earlier in the course of the disease, compared to the later phases. Finally, ROC curve analyses suggested that these miRNAs could serve as non-invasive biomarkers of early cognitive impairment (Fig. 4).
Subjective cognitive decline is known as a phenomenon of self-experienced cognitive decline that may represent the first manifestation of AD, when objective impairment in cognition is still not present [11, 44]. Accidentally revealed MCI in healthy subjects who did not report SCD, and that we found in the present study (Table 2), has not been clinically recognized so far, to the best of our knowledge. Neuropsychological screening tests indicated that 33,3% of the apparently healthy subjects had MCI (Table 2), which could not be explained by neurological examination and laboratory findings. Many studies showed importance of SCD for early prediction of development of clinically manifested AD [11, 46]. Moreover, neuroimaging techniques revealed distinctive brain alterations related to the symptoms of SCD [44, 47]. However, there are some critical points in the process of SCD evaluation that might be too subjective, affected by the individual cultural background and susceptible to the influence of various social factors and inter-personal relations at the moment of evaluation [12]. Our decision to use simple, open questions for SCD evaluation instead of structured questionnaires was in part driven by these facts. Results of neuropsychological screening tests used, MoCA and MMSE, were in correlation (r = 0.725; p < 0.01), but MoCA proved to be more sensitive, which is consistent with previously published data [42]. MCI would not have been discovered in 22.2% of the examinees, had they been evaluated by MMSE only (Fig. 2). Moreover, if the evaluation of SCD was not followed by an objective assessment, none of the participants with cognitive impairment would have been identified. Thus, our results certainly raise a question of reliability of subjective comprehension of cognitive functioning and emphasize significance of objective neuropsychological assessment. In order to rule out other causes of cognitive decline, history of other diseases, brain injury, and the list of medications were reviewed, and statistically significant difference in age among the groups was not found, which confirmed there was no significant difference among the groups (Table 1). The participants were also checked for vitamin B12 deficiency, thyroid dysfunction, anemia, and other acute or chronic conditions that could cause MCI. Finally, no significant variability in neurological examination or scale of depression was observed. However, it is worth noting that the extent of neurological evaluation in the presented study was limited to non-invasive and inexpensive tests and also, determined by the fact that AD patients have been retrospectively recruited.
The MCI group had significantly higher level of miR-146a and miR-155 expression, in comparison to the healthy control subjects (Fig. 3). Various studies conducted in humans or animal models and cell cultures, over the last ten years, unambiguously demonstrated involvement and significance of miR-146a and miR-155 in pathogenesis of AD [34, 48–52]. miRNA-146a was among the first miRNAs found to be highly expressed in AD brain, specifically in anatomical regions affected by the disease, but not in the other, control regions of the same brain [53]. Authors of the recent bioinformatics study created a miRNA-target interactions network constituted of 8 miRNAs and found that nodes in the network with the highest number of edges include miR-146 [54]. As for miR-155, its expression was found to be increased in AD rats, and its inhibition improved the impaired memory in this animal model [55].
When considering the continuum of clinical presentation of AD, it is of special interest to identify miRNA signature patterns of MCI stage, since it is estimated that up to 22% of individuals clinically defined as MCI, progress to AD within one year [56]. Circulatory miR-146a is known to be significantly upregulated in patients with MCI who later develop AD, compared to those who do not convert to AD [48]. Also, higher miR-146 expression level was found in APOE E4 carriers, and it correlated with neuroimaging hallmarks of AD and increased CSF 42 amino acid amyloid-β (Aβ42) concentration [48]. An interaction among MCI-associated genes and miR-155 was emphasized in the study by Strafella et al., which also found that miR-146 and miR-155 signaling pathways significantly interact in pathophysiological cascade of AD and other neurodegenerative diseases [57]. Taken together, these findings suggest that AD could be an underlying cause of the accidentally discovered mild cognitive impairment in volunteers in our study, who had increased expression of miRs-146a and -155, compared to the control group.
Closer understanding of miR-146a and -155 involvement in particular pathophysiological pathways of AD, further explains the significance of their increased expression level in MCI group. miR-146a, known for its importance in modulating the innate immune response and inflammatory events in brain cells [58], has been recently proposed as highly significant in neuroinflammatory mechanisms of AD [34, 60]. For example, in primary human neuronal-glial (HNG) cell co-cultures, miR-146a transcription was found to be induced by certain stress factors, such as the pro-inflammatory cytokine IL-1, known to be elevated in AD brain [58]. More recent research of inflammatory processes in AD also revealed significance of miR-155 in these pathways [33, 60]. This miRNA was shown to be early and strongly upregulated in 12-month triple transgenic mouse AD model [49], but also in Aβ-activated microglia and astrocytes, contributing to the production of inflammatory mediators such as IL-6 and IFN-β, inducing the decrease of activity of cytokine signaling suppressor (SOCS-1) [33]. Moreover, these studies revealed not only involvement of miR-146a and miR-155 in neuroinflammatory AD pathways, but also their interactive points in that cascade [57]. On the other hand, it is well established that neuroinflammation contributes to AD pathogenesis [25–32], and there is evidence that strongly suggests that it is initial and vital component in the AD pathophysiological cascade [61–65]. In an animal model, activation of microglia, which are key mediators of neuroinflammation among the innate immune cells, has been observed at the pre-plaque stage of AD [61]. Also, increased microglial activation has been detected in people with MCI, in the absence of amyloid tracer uptake [62, 63]. Genome-wide association studies found that mutations of microglial or innate immune genes, such as CD33, TREM2, and complement receptor type 1, are associated with an increased occurrence of AD in the population [64, 65], which also supports the neuroinflammatory concept as initiating in AD. All these data go in favor of hypothesis that an increase in expression levels of inflamma-miR-146 and -miR-155 in MCI subjects could be explained by their involvement in inflammatory pathways, characteristic for the early phase of AD pathophysiological events.
The presented results also showed that the expression levels of miR-146a and miR-155 were not statistically different between control and AD subjects and interestingly, miR-146a was still upregulated in MCI compared to AD group. More thorough insight in neuroinflammatory AD events and engagement of miR-146a and miR-155 in those pathways, could offer an explanation for such a result. Although essentially defensive, the immune response can cause harmful consequences if it is induced too strongly or for too long [32, 66]. Thus, at some time point, there is an activation of homeostatic mechanisms to limit destructive inflammatory events in AD [67, 68]. Published data clearly indicate that miR-146a also has a role in suppression of pathological neuroinflammatory response in AD. Primarily induced by pro-inflammatory cytokines [58, 70], miR-146a in turn downregulates proteins in overactive neuroinflammatory signaling pathways, contributing to their limitation [60]. Consequently, it is possible that this negative regulatory feedback mechanism ends with decreased expression of miR-146a. This consideration is supported by the research on primary neuronal cultures or neuroblastoma cell lines bearing Swedish mutation as AD cell models, which showed that miR-155 and miR-146a were highly expressed in microglia, responding to Aβ as a stress-related factor, with more prominent role of miR-155, which is found to be responsible for microglia polarization to pro-inflammatory M1 phenotype. Moreover, subsequent increase in inflammatory cytokines was followed by reduction of miR-146a expression, while miR-155 upregulation persisted [71]. Another study by the same authors [72] showed that presence of Aβ in different assembly states interacts with microglia leading to an inflammation cascade in young cells and that response is lost in aged cells, suggesting a differential response along the progression of AD. Temporal discrepancy of miR-146 and miR-155 expression during an inflammatory response was confirmed in animal model as well [73]. Increased expression of miR-155 induced overactive acute, but also chronic inflammation, even in a miR-146a-deficient mice.
These results are in line with our findings of miR-146a and miR-155 expression levels in clinical context. Significant miR-146a upregulation in MCI compared to control corresponds with its dominant role early in the disease process, through the initiation of inflammatory cascade and interaction with mediators of inflammation. Normalization back to control levels in AD group probably reflects suppression of miR-146a by homeostatic, anti-inflammatory mechanisms, characteristic for the chronic stage. On the other hand, miR-155 expression implicates its persistent activity, as a reflection of continuous, chronic, although self-limiting inflammation and continuous microglial engagement in that process.
However, other studies showed that disease progression in AD mouse models was followed by increased miR-146a expression in brain tissue [50], and also, it was observed in the same model ex vivo, that density of plaques and synaptic pathology were in correlation with miR-146a expression. Differences in methodological approach could be responsible for an opposite observation. Similarly, Lukiw et al. found that miR-146a levels measured in neocortex and limbic system increased, as the severity of AD advanced [58].
The number of participants is the limiting aspect of our study, thus, the research on the larger group is warranted in the future. Moreover, lack of the complete neurological evaluation in CTRL and MCI groups, that includes some invasive and expensive tests, might represent another limiting point of our study, but, at the same time, it has opened new directions for the future cohort study with the MCI group. Regular follow ups, screening of molecular and clinical inflammatory markers with complete neurological assessment at later time points, will potentially confirm AD as a cause of their cognitive impairment, as well as neuroinflammation as a key pathophysiological event. Also, cross-cultural validity of MoCA cutoff score and its adjustment for our region should be explored in the future. Eventually, results of our study imply that SCD evaluation through an open question might not always be reliable tool to indicate CI in elderly. Therefore, proposed structured evaluation form [11] should be considered as an assessment tool in the future studies.
Our results show that when analyzed together, the specific expression patterns of miR-146a and miR-155 are able to differentiate MCI group from the control as well as from the AD group of participants (Fig. 5). AUC value of 0.8642 for miR-146a, with 77.8% sensitivity and 94.4% specificity (Fig. 4A), and AUC value of 0.7654 for miR-155, with 66.7% sensitivity and 88.9% specificity (Fig. 4C), clearly suggests their potential diagnostic significance for MCI detection. More research is needed to determine if these miRNAs could be used for detection of early AD stages in general population, as well as in patients with other comorbidities that were not included in this study.

Joint expression pattern of the selected inflammatory miRNAs differentiates the MCI group from the other two groups of participants. The graph represents a two-dimensional scatter plot of miRNA-146a and -155 expression levels. Each data point shows expression levels of miRNA-146a and -155 in plasma sample of one study participant, and it is labeled according to the associated diagnosis (CTRL, control; MCI, mild cognitive impairment; AD, Alzheimer’s disease). The data clustering is illustrated by the superimposed star plot showing the mean value for a group in the center each cluster, which is surrounded by the 95% confidence area in the shape of the ellipse.
Finally, our results on miRNA expression in patients with already diagnosed AD, which showed that miR-146a and miR-155 were not upregulated earlier in the course of the disease, compared to the later phases, additionally support their potential significance in detection of patients in MCI stage.
Conclusions
This study accidentally identified that a certain number of patients with cognitive decline in Montenegrin population remain undetected. SCD evaluation should be important and possibly critical aspect of the successful and timely detection of cognitive decline, but neuropsychological screening instruments should be routinely administered to elderly in Montenegro, even if the patient does not complain of problems related to cognitive functioning.
The upregulation of miR-146a and miR-155 could have utility in serving as a non-invasive, biofluid biomarker for the diagnosis of MCI due to AD and thus, potentially, also for monitoring of drug treatment efficacy and for making prognosis for the patients in early stages of AD.
Moreover, this study also identified the potential of neuropsychological screening instruments and molecular markers, which could together significantly improve our ability to diagnose AD in very early stage, and could possibly become routine non-invasive tools for detection of early AD.
Although determination of inflamma-miR-146a and -155 circulatory levels might represent a novel non-invasive biomarker for detection of an early stage of cognitive impairment due to AD, the research on the larger patient’s cohort is warranted. Additionally altered miRNA and/or small non-coding RNA (sncRNA) levels may be uncovered and further improve the use of non-invasive, biofluid biomarkers for the diagnosis, drug treatment efficacy monitor and prognosis of early AD stages.
Footnotes
ACKNOWLEDGMENTS
This work has been presented in the 16th CONy Congress and was awarded First Prize for Alzheimer’s Disease and Dementia.
This research is funded by the scientific research project DEMONSTRATE, through the grant awarded by the Ministry of Science of Montenegro, Grant Agreement No. 01-781/2.
For the realization of this study, we would like to thank our collaborators on the DEMONSTRATE project – Dr. Apollonia Tullo, Dr. Flaviana Marzano, Dr. Sergio Giannattasio, and Dr. Antonella Bobba from the Institute of Biomembranes, Bioenergetics and Molecular Biotechnologies – CNR in Bari, as well as to Dr. Nicoletta Guaragnella from the Department of Biosciences, Biotechnologies and Biopharmaceutics, University of Bari “Aldo Moro”.
We would especially like to thank neuropsychologist Tijana Vuković, for her contribution in the realization of this study.