
Abstract
Background:
Clinical trials now test promising therapies in the preclinical stages of Alzheimer’s disease (AD). Participant willingness to enroll in different types of preclinical AD trials is understudied and whether the FDA approval of aducanumab affected these attitudes is unknown.
Objective:
To evaluate preferences toward three preclinical AD trial scenarios and whether the FDA approval of aducanumab changed willingness to participate among potential trial participants.
Methods:
Through an electronic survey, we asked enrollees in a recruitment registry age 50-79 to rate their willingness (using a 6-point Likert scale) to enroll in three hypothetical preclinical AD trial scenarios: an in-clinic infused monoclonal antibody intervention, a home-infused monoclonal antibody intervention, and an oral BACE inhibitor intervention. We administered the survey before and after the FDA approval of aducanumab. We used a generalized estimating equation model to assess group differences in preference for the trial scenarios. We used a paired t-test to determine if willingness to participate (using total willingness across three scenarios as the outcome) changed after the FDA decision.
Results:
At baseline, the mean participant willingness was highest in the in-clinic infusion scenario. There was no significant change in willingness to participate, overall, after the FDA decision. Participants who were independently aware of the FDA’s decision (prior to the second survey) demonstrated reduced willingness to participate; participants unaware of the FDA decision demonstrated no change.
Conclusion:
Willingness to participate in preclinical AD trials may have been negatively affected by the FDA’s decision to approve aducanumab among those aware of the decision.
INTRODUCTION
On June 7, 2021, the US Food and Drug Administration (FDA) granted accelerated approval to Biogen’s aducanumab (Aduhelm™), a monoclonal antibody that reduces fibrillar amyloid-β (Aβ) levels in the brains of people with Alzheimer’s disease (AD) [1]. The decision was controversial. The clinical benefits of aducanumab were tested in two Phase III trials, ENGAGE (NCT 02477800) and EMERGE (NCT 02484547), with similar study designs. The trials were halted based on an interim futility analysis and in post-hoc analyses showed conflicting results [2, 3]. Based on the available findings from these and earlier phase trials of aducanumab, an FDA Advisory Committee voted uniformly against full regulatory approval. The FDA granted accelerated approval to aducanumab based on the demonstrated ability of the treatment to lower brain amyloid. The reliance on Aβ as a surrogate was viewed by some as premature [4]. The initial prescribing information for aducanumab indicated only “Alzheimer’s disease”, without further restrictions based on disease severity, and did not require confirmation of the presence of brain amyloid. The FDA and Biogen later updated the prescribing information to match the patient populations enrolled in the two registration trials. The drug is expensive; initially priced by Biogen at $56,000/year and later reduced to $28,000/year, without factoring in other associated costs, such as recommended magnetic resonance imaging (MRI) scans to assess treatment safety. The Centers for Medicare and Medicaid Services limited coverage of aducanumab to patients enrolled in qualified clinical trials [5]. In addition to peer reviewed publications [6–9], the decision and in particular the associated controversies resulted in substantial coverage by lay media (e.g., [10–12]).
While the trials of aducanumab tested the drug’s safety and efficacy in patients with symptomatic AD, many in the field believe that treatments targeting AD biology hold greatest promise earlier in disease, before overt symptom onset [13]. Numerous secondary prevention trials [14] enrolling cognitively unimpaired participants who demonstrate biomarkers of disease such as elevated brain amyloid levels are underway [15–19]. Recruitment to these trials, also known as preclinical AD trials, is challenging [20]. Whether people have preferences in trial type and whether the FDA decision to approve aducanumab will impact recruitment of participants to preclinical AD trials is unknown. We examined these questions through a pre/post design survey study among older cognitively unimpaired participants enrolled in a recruitment registry.
METHODS
Study design
On May 27, 2021, we sent email invitations to participate in a survey study to 1,090 participants in the University of California, Irvine (UCI) Consent-to-Contact Registry [21]. To be eligible, participants were required to be between the ages of 50 and 79, to live within 50 miles of UCI, and to have indicated at enrollment in the registry that they were willing to consider studies that involve investigational drugs [21]. We excluded participants who self-reported a diagnosis of AD, mild cognitive impairment, or a neurological condition at registry enrollment. Data collection was performed through REDCap [22]. The survey was closed on the day of the FDA approval of aducanumab. Informed consent was acknowledged by clicking the survey link. The study was approved by the UCI Institutional Review Board.
The survey included a short primer (Supplementary Material 1). The primer asked participants to consider a hypothetical 4-year trial that required participants to have a positron emission tomography scan to measure the amount of brain amyloid and enrolled only those with elevated brain amyloid levels, who were at increased risk for dementia. The hypothetical trial was described as involving multiple visits to the study center and procedures including twice annual MRIs and cognitive assessments every 6 months. Participants would have a 50% chance of receiving a drug or placebo. At the conclusion of the primer, participants were asked to rate their willingness to participate in three trial scenarios: 1) an anti-amyloid monoclonal antibody infused monthly at a clinic, 2) an anti-amyloid monoclonal antibody infused monthly at home, or 3) daily administration of an oral β-site amyloid precursor protein cleaving enzyme (BACE) inhibitor (a drug that prevents the formation of Aβ). The scenarios were presented in random order. Each scenario described the mode of administration and the associated risks of the study treatment. For the monthly monoclonal antibody treatment scenarios, risk was described as including that about 25% of people taking the drug experienced a swelling in the brain that usually did not cause symptoms and resolved with time. For the BACE inhibitor treatment scenario, risk was described as including that about 25% of people taking the drug (at higher doses than would be used in the preclinical AD trial) experienced worsening of memory and thinking skills that resolved after stopping the medication. Possible responses ranged from extremely unlikely to extremely likely to participate on a 6-point Likert scale (Range of 1-6 for each scenario). The baseline survey also assessed six demographic variables: age, sex, race, ethnicity, years of education and family history of AD.
On June 15, 2021, we sent a follow-up survey to participants who completed the initial questionnaire. A new primer addressed the FDA approval of aducanumab (Supplementary Material 2). Identical questions (relative to the initial survey) assessed willingness to participate in the three hypothetical trial scenarios. We also collected information on whether participants were independently aware of the FDA approval of aducanumab and the manner in which they learned of the approval decision. The scenarios were presented in identical order to that used at baseline for each participant.
Statistical analyses
To characterize the study population, we used sample proportions for categorical variables and means and standard deviations (SD) for continuous variables.
We treated the study as having two co-primary objectives: to assess participant preferences among trial scenarios and to assess the impact of the FDA approval on participant willingness to participate in preclinical AD trials. For our first co-primary outcome, we used a generalized estimating equation (GEE) model for repeated measures analysis clustered on subject to assess group differences in preference for the three trial scenarios at baseline. The outcome was the participant response (on a 6-point Likert scale) to the trial scenarios, modeled as a continuous variable. Each participant had three observations, one for each scenario. Given the balanced nature of the data and the small numbers of repeated measures per participant, an unstructured working covariance structure was assumed. A multivariate Wald test was conducted to assess whether there are overall differences in willingness between trial scenarios. To identify characteristics associated with willingness conditional upon trial type at baseline, we ran a GEE model adjusting for age, sex, race, ethnicity, years of education, and family history of AD, which were a priori selected as potential confounders. To control familywise type I error across the two co-primary endpoints at 0.05, we conducted two-sided level 0.025 tests for each co-primary endpoint.
For our second co-primary outcome, we used the sum of the willingness to participate scores across the three trial scenarios (Range: 3-18) and a paired t-test to test the hypothesis that willingness to participate changed after the FDA approval of aducanumab. As secondary analyses, we assessed whether specific characteristics were associated with changes in responses. We ran a multivariable linear regression model to identify predictors of change in willingness to participate (pre-to-post) for the combined overall willingness scores across scenarios, adjusting for each demographic term at baseline.
In exploratory analyses, we compared change in responses based on participants’ awareness of the FDA approval decision (aware independent of the survey versus not aware) using a paired t-test for total willingness scores and for each trial scenario. Further, we fit a GEE model to test the hypothesis that the continuous outcomes of change differed by trial scenario. We considered potential effect modification by participants’ prior awareness of the FDA approval decision by including an interaction term between trial scenario and prior knowledge of the approval (aware independent of the survey versus not aware). A multivariate Wald test of interaction between prior knowledge of the FDA approval and trial scenario was performed.
Finally, in an attempt to operationalize meaningful willingness scores and changes in scores we re-ran each of the above analyses using dichotomous outcomes. We considered participant willingness as “highly likely to participate” if the scores were ≥15 for the combined overall willingness scores (range 3-18) and ≥5 for individual trial scenarios (range 1-6). No adjustment for multiplicity was made for secondary and exploratory results.
RESULTS
Participant characteristics
Three hundred and sixty-nine (34%) participants responded to the baseline survey and among these, 273 (74%) completed the follow-up survey (Fig. 1). Participant demographics are described in Table 1. Demographic characteristics between the follow-up completers and non-completers were comparable.

CONSORT flow diagram.
Study participant demographics
Differential willingness by trial type
The mean (SD) willingness score at baseline was 3.82 (1.54) for the infusion treatment in the clinic, 3.78 (1.51) for the infusion treatment at home, and 3.57 (1.59) for the BACE inhibitor treatment. In our unadjusted GEE model assessing differential willingness for the three trial scenarios, the average willingness score of the BACE inhibitor trial was 0.16 points lower than that for the in-clinic infusion trial (95% CI: -0.26, -0.06) at baseline. The average willingness score for the home infusion trial was 0.06 points lower than the score for the in-clinic infusion trial (95% CI: -0.13, 0.01) at baseline. The Wald test showed significant overall differences in willingness between trial scenarios (χ2 = 9.1; d.f.=2; p = 0.01). We found that having a family history of AD (est: 0.47; 95% CI: 0.16, 0.78; p = 0.003) and uncertainty about family history of AD (est: 0.68; 95% CI: 0.26. 1.11; p = 0.002) were associated with higher willingness to participate at baseline, conditional upon trial type (Table 2). Analyses using dichotomous outcomes showed similar trends.
Characteristics associated with willingness conditional upon trial type at baseline
Note* higher scores indicate higher willingness.
Within-subject change in willingness
In our second co-primary analysis, we did not observe a significant change in total willingness score after the FDA approval of aducanumab (mean of difference = 0.36; t = 1.540; p = 0.125). The mean (SD) total willingness score was 11.0 (4.2) at baseline and 10.9 (4.1) at follow-up. When we assessed characteristics associated with change in responses (continuous outcome) in a multivariable linear regression model, uncertainty about family history of AD (est: -1.62; 95% CI: -3.06, -0.19; p = 0.03) was significantly associated with change (negative association) in willingness (Table 3). Analyses of the dichotomized outcome yielded similar results. Those with family history (OR: 1.96; CI: 1.05, 3.67; p = 0.04) and those who were uncertain of having a family history of AD (OR: 2.52; CI: 1.13, 5.64; p = 0.02) were more likely to change their willingness score from above 5 to below 5 (negative change) compared to those with no family history. Female participants were more likely than males to change their willingness score from below 5 to above 5 (positive change) (OR: 2.61; CI: 1.05, 6.52; p = 0.04).
Linear regression of characteristics associated with change in response (post-pre)
Prior knowledge of FDA approval of aducanumab and information source
Among participants completing the follow-up survey, 156 (57%) reported independent knowledge of the FDA decision (i.e., were aware of the decision prior to completing the follow-up survey), while 117 (43%) reported no such knowledge. The sources of information among those who had prior knowledge of the FDA decision is reported in Table 4. Print, television, radio, and online news media were the most common sources of learning about the decision. When we compared individuals with independent knowledge of the FDA approval decision to those without this knowledge, we observed a difference in the relative change in willingness to participate (Fig. 2). Those with prior knowledge of the FDA approval demonstrated a significant reduction in total willingness score (paired t-test; mean of difference = -0.66; t = 2.16; p = 0.03); those with no knowledge demonstrated no change (paired t-test; mean of difference = 0.03; t = -0.09; p = 0.9). For the individual scenarios, those with independent knowledge of the FDA decision demonstrated a decrease in willingness to participate in the in-clinic infusion trial (paired t-test; mean of difference = -0.30; t = 2.73; p = 0.007); no significant differences were observed for the home infusion (mean of difference = -0.23; t = 2; p = 0.05) or BACE inhibitor (mean of difference = -0.13; t = 1; p = 0.3) trials. Participants with no prior knowledge of the FDA decision demonstrated no change in willingness to participate in any individual trial scenario (all paired t-tests, p > 0.05). Overall, in our GEE model, the association between trial scenario and change in total willingness did not significantly differ by prior knowledge of FDA approval (p = 0.29) (Table 5). We did, however, observe a difference between those with and without prior awareness in the directionality of change for the BACE inhibitor trial. Among participants with prior awareness, there was a positive change relative to the infusion clinic scenario (est: 0.17; CI: -0.03, 0.37). Among participants without prior awareness there was a negative change (est: -0.09; CI: -0.35, 0.18). Analyses using dichotomous outcomes of change showed no statistically significant results.
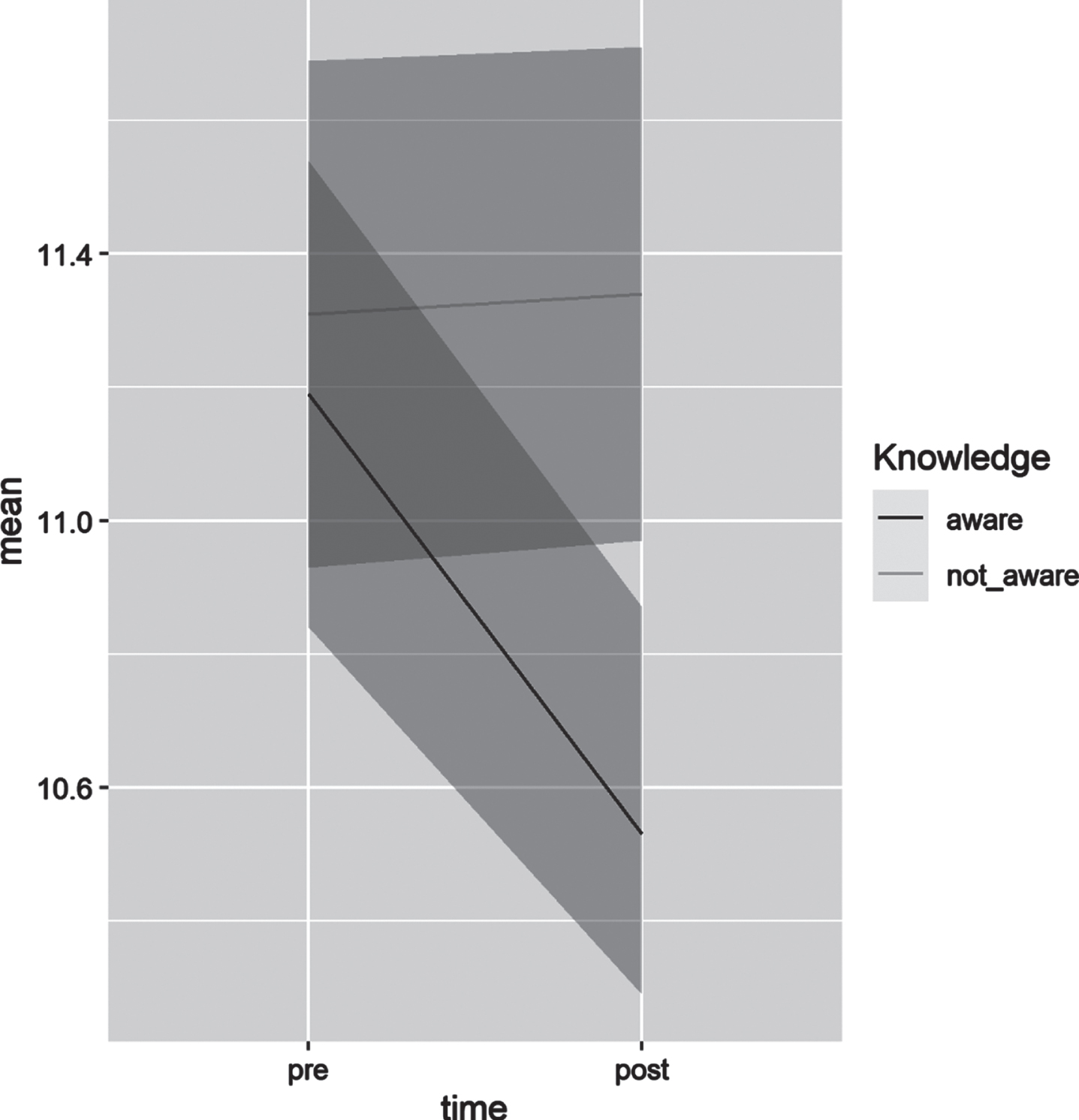
Change in mean willingness score by awareness of FDA’s decision to approve aducanumab independent of study. For each time point, a 95% confidence interval is provided (shading).
Difference in change in willingness by trial scenario with interaction between\\ prior knowledge and trial scenario
*p = 0.29 for multivariate Wald test of interaction between prior knowledge of the FDA approval and trial scenario. This model adjusted for age, sex, race, ethnicity, education, and family history of AD.
DISCUSSION
In this study, we found that willingness to participate in preclinical AD trials was reduced among those independently aware of the FDA’s approval of aducanumab, whereas willingness was not changed among potential participants unaware of this decision. These findings may suggest that the approval decision and the media coverage it received, much of which focused on controversies associated with the decision, may have reduced public trust in the national AD research ecosystem [23]. Researchers may need to consider the implications of these results, as well as other factors that may result in recruitment bias to trial sample selection and result generalizability [24].
Challenging clinical trial recruitment is a key barrier to AD research progress [25, 26]. Successful recruitment requires making potentially eligible participants aware of trials, but also compelling them to overcome barriers to participation and to make a choice to enroll [27]. Media coverage (also known as ‘earned media’) may provide a unique mechanism of substantially increasing trial awareness, while also offering compelling messages to affect willingness to participate. For example, positive coverage in a nationally syndicated column of a previous preclinical AD trial produced a large number of screens and randomizations, propelling the study to full accrual [28]. Similarly, in a mobile health smoking cessation trial for women, earned media coupled with social media produced approximately three times more participants than the planned total accrual [29]. More recently, the COVID-19 pandemic has spurred clinical trials with high public urgency and media coverage was a key component of trial recruitment strategies [30, 31]. Alternatively, negative coverage by the media has been reported as an obstacle to recruitment in some clinical trials. In a study investigating willingness to enroll in HIV vaccine trials, periods of media coverage of scientific setbacks and breakthrough infections were accompanied by increased reports of safety concerns and reduced overall willingness to participate among potential enrollees [32]. Qualitative data from focus groups of cancer trial clinical research associates have shown that while media coverage was perceived as increasing awareness of trials, negative coverage was perceived as substantially slowing accrual [33].
Other aspects of this study may be important to future preclinical AD trial designs. The results differ from previous studies that found participant willingness to be higher for trials of approved compared to investigational medications [34, 35]. The primer for the follow-up survey clarified that while the FDA had approved aducanumab for people with AD, it was not approved as a preventative therapy. It is possible that participants in this study recognized this distinction and therefore did not adjust their follow-up responses. Alternatively, the controversies around aducanumab’s approval may have counteracted any increase in willingness that otherwise would have resulted from FDA approval, though we did not observe an increase in willingness to participate after FDA approval among those who were unaware of the decision.
We found small differences in participant preferences for specific trial treatment scenarios. The scenarios were based on AD therapies that have been tested in preclinical AD trials, namely BACE inhibitors [36] and monoclonal antibodies against Aβ [37]. BACE inhibitor therapies were tested in symptomatic and asymptomatic populations at doses sufficient to substantially reduce amyloid production and were discontinued due to safety concerns in these trials [38]. Anti-amyloid monoclonal antibody therapies remain under investigation in both symptomatic and asymptomatic populations. While there were no significant differences between the monoclonal antibody infusion treatment scenarios (in the clinic and at home), participant willingness was lower for the BACE inhibitor scenario compared to the in-clinic monoclonal antibody trial scenario (BACE was not different from the home-infusion scenario). Our data do not instruct on why this difference was observed, though a distinguishing factor between the scenarios was safety. The BACE inhibitor scenario described a risk of worsening cognitive performance, compared to risk of amyloid imaging abnormalities [39] (described as most often asymptomatic) for the monoclonal antibody scenarios. We also recognize that the small point estimates may indicate that these differences are not adequate to impact a participant’s actual decision to enroll in a trial. Indeed, no statistically significant differences in willingness were observed between trial scenarios in our analyses using dichotomous outcomes comparing the proportions who indicated a high likelihood of participation. This may suggest a willingness of participants to continue to consider participation in BACE inhibitor trials or even to enroll in platform trial approaches that include randomization to arms of differing treatment modalities [40].
This study had limitations. Subjects were presented with hypothetical scenarios and not actual opportunities to enroll in trials. Participation in clinical trials requires a thorough informed consent process that was not possible in the current approach. For example, we offered incomplete descriptions of treatment safety in the trial scenarios [41, 42]. It is unclear whether the observed reduction in willingness among those aware of the FDA decision, approximately 1-point on a 15-point scale, would translate to actual differences in enrollment decisions. When we assessed for categorical changes in willingness, we found no differences. The survey was kept brief in an effort to maximize participant responses. This approach, however, prevented collection of additional data pertaining to the rationale behind participants’ responses. Factors not assessed in this study may have influenced participants’ responses (e.g., previous experiences with trials). We did not directly measure participant trust or the impact of the FDA approval on trust. The study had limited inclusion of participants from underrepresented racial and ethnic groups, preventing examination of the observed findings for potential differences in these highly important groups, in whom lack of trust is already a barrier to participation [43, 44]. The participants were also a subset (i.e., those willing to consider trials of investigational treatments) of a recruitment registry, and therefore are likely to be a highly motivated group interested in AD research— though this may be a population key to completing preclinical AD trials [45]. Finally, negative press for aducanumab began before the FDA decision (e.g., coverage of the halted trials and the FDA advisory panel meeting) and before the baseline survey. We did not measure participants’ awareness of these events at baseline.
Conclusions
This study had important strengths, including a pre/post design that permitted within-subject assessment of the impact of the FDA approval of an AD therapy on willingness to participate in AD research. We found that willingness to participate in trials may have been negatively affected by media coverage of the decision among some potential participants in future AD research. These results may be important for researchers to consider as they plan future preclinical AD trials, in particular, the risk of recruitment bias and potential impact on generalizability.