
Abstract
Background:
There is limited epidemiological research on the incidence of young onset dementia (YOD). Estimates of YOD incidence in New Zealand are extrapolated from international studies that do not reflect New Zealand’s population and ethnic diversity.
Objective:
To determine the incidence of YOD in the geographical area served by the Waikato District Health Board
Methods:
All new inpatient and outpatient in the age range 30–64 years with a documented diagnosis of dementia at Waikato Hospital between 1 January 2014 –31 December 2016 were identified. Incidence rates were calculated by 5-year age-band, sex, and ethnicity.
Results:
64 incident cases of YOD were included. Incidence rates for all cause YOD were 13.3 (95% CI 10.3–17.0) and 22.7 (95% CI 17.5–29.1) per 100,000 person-years in the age range 30–64 years and 45–64 years respectively. The incidence rate in Māori (20.0, 95% CI 11.4–32.4) was higher compared to non-Māori (12.0, 95% CI 8.9–15.9), but this difference was not statistically significant (p = 0.09).
Conclusion:
The incidence of YOD in this study is similar to global estimates. Incidence may be higher in Māori compared to non-Māori, highlighting the need for culturally appropriate approaches to dementia prevention, intervention, and care.
INTRODUCTION
Young onset dementia (YOD) is defined as dementia occurring before the age of 65 years [1] and, while uncommon compared to late onset dementia, is estimated to account for 8–10% of all dementias [2]. The etiologies underpinning the clinical presentation of YOD are more heterogeneous than late life dementias [1], with the most common causes of YOD identified in prevalence studies being Alzheimer’s disease, vascular dementia, and frontotemporal dementia [3]. Individuals with YOD place significant demands on health services due to their unique medical and psychosocial needs and the challenges associated with providing care for them [4, 5]. The development and provision of appropriate YOD services requires an understanding of the size of the patient population to guide appropriate allocation of resources to meet their needs [6].
There is limited global epidemiological data on the incidence of YOD, with published incidence rates in the literature ranging from 11 to 24.4 per 100,000 person-years depending on the study population and study design. Mercy et al. [7] identified YOD cases diagnosed in specialist memory and dementia clinics in Cambridgeshire, UK, between 2000–2006 and reported a rate of 11.5 per 100,000 person-years in 45–64 year olds. Sanchez Abraham et al. [8] identified all patients diagnosed with YOD between 2005–2011 in a closed population of 17,614 people attending a hospital based geriatric care department in Mar del Plata, Argentina. They identified 14 YOD cases, corresponding to an incidence rate of 11 per 100,000 person-years in 21–64 year olds. Garre-Olmo et al. [9] identified all YOD cases from a standardized clinical registry of new dementia cases in a geographically defined general population in the Health Region of Girona, Spain between 2007–2009 and reported an incidence of 13.4 per 100,000 person-years in the 30–64-year-old population. More recently, Kvello-Alme et al. [10] have reported a YOD incidence of 14.8 and 25.0 per 100,000 person-years in 30–64- and 45–64-year-olds, respectively, in Trøndelag county, Norway, between 2015–2017. Carcaillon-Bentata et al. [11] used administrative data from the French national health data system to estimate the incidence of YOD in France in 2016. An incident case was defined as any individual with a documented diagnosis of YOD in 2016 that was not present in previous years. Using this definition, the authors reported an age- and sex-standardized incidence rate of 24.4 per 100,000 person-years in the 40–64-year-old population. Chiari et al. [12] prospectively identified all newly diagnosed YOD patients in Modena province, Italy, between 2017–2019 and reported an incidence of 13.2 and 22.1 per 100,000 person-years in the 30–64- and 45–64-year-old population respectively.
There are no epidemiological studies on the incidence of YOD in Aotearoa, New Zealand. Previously reported prevalence has been extrapolated from international studies; however, the study populations in these studies are likely not representative of the unique ethnic and demographic makeup of New Zealand [13]. The main ethnic groups identified in the 2018 New Zealand census are 70.2% European, 16.5% Māori, 15.1% Asian, and 8.1% Pacific peoples. As such, this study aims to determine the incidence of YOD over a three-year period between 2014–2016 in a region of New Zealand that is broadly representative of the national population.
METHODS
This study received ethical approval from the Northern A Health and Disability Ethics Committee (HDEC), approval number 16/NTA/189.
Population
This incidence study covers the Waikato District Health Board (WDHB) catchment area. WDHB serves a population of approximately 400,000 (9.6% of the New Zealand population), with a 30–64-year-old population of 159,813 at census 2013 [14]. The age and sex structure of the WDHB population mirrors that of the New Zealand population. However, the region has a higher proportion of M
Patients
New Zealand guidelines for the assessment of cognitive impairment recommend all patients under the age of 65 years be referred for specialist assessment [16], so it is considered unlikely the diagnosis of YOD would be made by general practitioners in primary care. Waikato Hospital is the sole tertiary center providing specialist care for the region and receives all referrals for the assessment of cognitive impairment. There is no centralized referral pathway for cognitive impairment so the diagnosis of YOD can be made by psychiatrists, neurologists, or geriatricians across a number of different services including specialist memory services, mental health services for the elderly, neurology, and the intellectual developmental disorder team (IDDD). Accepted referrals to these services usually undergo a comprehensive assessment including neuroimaging and neuropsychological assessment, with a consensus diagnosis reached in a multidisciplinary setting but the diagnostic procedure is not standardized between services. Some diagnoses of dementia are made in the private sector by neurologists and these diagnoses are not generally made in a multidisciplinary setting.
Case ascertainment
Incident YOD cases aged 30–64 years were ascertained through two sources (Fig. 1).
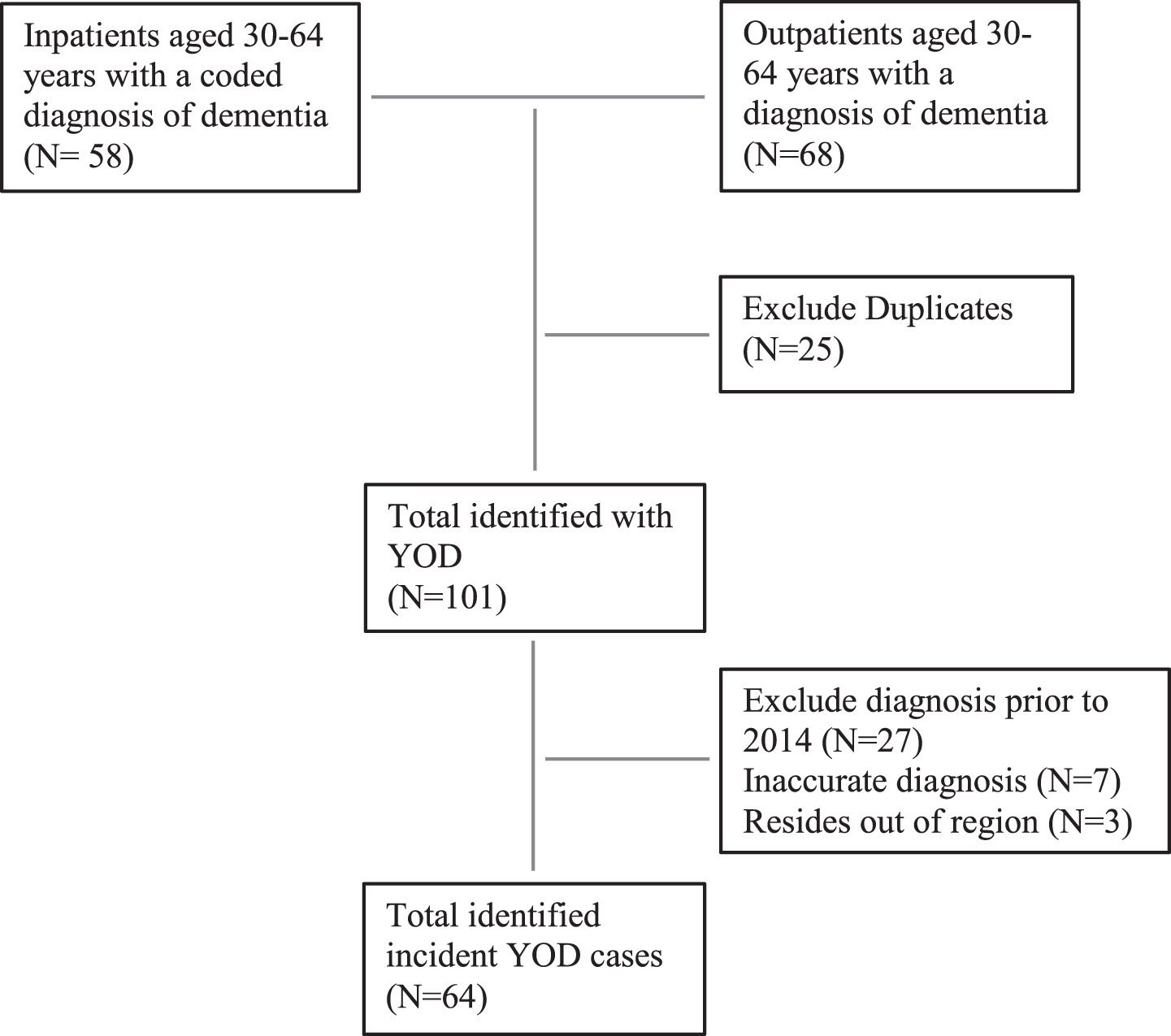
Flow diagram for YOD case ascertainment.
(i) Outpatient services
All WDHB services receiving referrals for the assessment of cognitive impairment were identified, with referral records reviewed for the Memory service, IDDD, neurology outpatient clinics, and Mental Health Services for Older People (MHSOP). In addition, one of four private neurologists in the region agreed to participate in this study. Adult Mental Health Services (AMHS) and Community Alcohol and Drug Services (CADS) reported they did not diagnose dementia and referred any patients with cognitive concerns to the Memory service or MHSOP for diagnostic workup and review.
All referrals to these outpatient services were reviewed for incident cases, defined as patients aged 30–64 years who were resident in the WDHB region and received an initial diagnosis of dementia in the three-year period 1 January 2014 and 31 December 2016. The raw data received from all sources were filtered to only include those aged 30–64 years at referral date. Data from all outpatient sources was combined to form a single database and duplicate individuals removed via unique National Health Index (NHI) identifier. A total of 5,432 unique outpatients were identified and their electronic records manually screened by one researcher (DW) for any documented evidence of subjective or objective cognitive impairment, or a diagnosis of dementia. Following this initial screen, the records were then reviewed independently by three researchers (DW, LF, EM) to confirm a diagnosis of dementia and dementia subtype.
(ii) Inpatient services
All inpatient hospitalizations to Waikato Hospital have their diagnoses recorded in a searchable database so all inpatient hospital discharges aged 30–64 years with a coded ICD-10 diagnosis of dementia during the study period were identified. The clinical records of these inpatients that had a coded diagnosis of dementia were checked manually and independently by three researchers (DW, LF, EM) to confirm both the diagnosis of dementia and that the initial diagnosis was made within the study period.
Statistical analysis
Patients identified with YOD from outpatient and inpatient services were combined in one spreadsheet and a final removal of duplicates by NHI was carried out in Excel. Incidence rates of dementia were calculated in 5-year age bands, by sex, for ages 30–64, as well as for the total age groups of 30–64 and 45–64 years. Incidence rates of dementia were also calculated for M
RESULTS
A total of 64 patients were identified who met the inclusion criteria for this study. Of these, 29 (45.3%) were female and the mean age at diagnosis was 58.3 years. Table 1 presents the diagnosis subtypes and age at diagnosis of incident YOD by sex. Of those with a confirmed diagnosis subtype, Alzheimer’s disease dementia (21.9%) was the most common diagnosis followed by vascular dementia (20.3%). Unspecified dementia accounted for 23.4% of diagnoses. Age at diagnosis was lowest for HIV (35.0) and highest for progressive supranuclear palsy (64.0 years). We did not identify any cases aged under 35. While age at diagnosis was broadly similar between males and females, a higher proportion of females were diagnosed with Alzheimer’s disease dementia (31.0% females versus 14.3% males) but this difference did not reach statistical significance (p = 0.38).
Diagnosis and age at diagnosis (AAD) for incident cases of dementia, by sex, 2014–2016
AD, Alzheimer’s disease dementia; FTD, frontotemporal dementia; DLB, dementia with Lewy bodies; PDD, Parkinson’s disease dementia; PSP, progressive supranuclear palsy; ARD, alcohol related dementia; HIV, human immunodeficiency virus; ID, intellectual disability; ADEM, acute disseminated encephalomyelitis.
Table 2 presents the overall dementia incidence rates by age and sex. The incidence of YOD in the age range 30–64 years was 13.3 (95% CI 10.3–17.0) and in the age range 45–64 years was 22.7 (95% CI 17.5–29.1) cases per 100,000 person-years YOD incidence increased with age, from 1.5 cases per 100,000 person-years (95% CI 0.0–8.5) in the 35–39 age band to 57.2 cases per 100,000 person-years (95% CI 39.8–79.5) in those aged 60–64 years at the time of diagnosis. There was no statistically significant difference in incidence rate between the sexes (males 15.3 versus females 11.6 cases per 100,000 person-years, p = 0.28).
Age- and sex-specific incidence rates of dementia, 2014–2016
*per 100,000 person years.
Table 3 presents the incidence of YOD by ethnicity. A quarter of the identified cases identified as M
Incidence of dementia aged 30–64 by ethnicity, 2014–2016
*per 100,000 person-year.
DISCUSSION
To the best of our knowledge, this is the first population-based study to investigate the incidence of YOD in a NZ population. The incidence rate of all-cause dementia in the age range 30–64 and 45–64 years was 13.3 and 22.7 per 100,000 person-years respectively. These rates are comparable to those from Spain [9], Norway [10], and Italy [12] which report incidence rates in the 30–64- and 45–64-year-old age groups of 13.2–14.8 and 11.5–25.0 cases per 100,000 person-years, respectively. The incidence in the age range 45–64 years is much higher than that reported in the UK by Mercy et al. [7] of 11.5 per 100,000 person-years.
The mean age at diagnosis in our study was 58.3 years and this is comparable with other studies which report a mean age at diagnosis of 57.2–62.0 years [9–12]. This study did not identify any sex differences in the incidence of YOD. While our finding is supported by some studies such as Garre-Olmo et al.’s in Spain [9], other studies have demonstrated a sex difference but not consistently in favor of the same sex. A higher incidence of YOD in females was described by Kvello-Alme et al [10] in Norway (13.3 males versus 16.4 females per 100,000 person-years in the age range 30–64 years), while Carcaillon-Bentata et al. [11] in France reported a higher incidence in males (26.9 males versus 20.1 females per 100,000 person-years in the age range 40–64 years).
In this study, we report a higher incidence of YOD in Māori of 20.0 per 100,000 person-years compared to non-M
The differential risk between M
The etiology of YOD is heterogeneous and this is reflected in the 9 different subtypes identified in this study. In line with other YOD studies [7–10], Alzheimer’s disease dementia (21.9%) was the most commonly diagnosed subtype, followed by vascular dementia (20.3%). The diagnosis of unspecified dementia (23.4%) in this study was high compared to < 5% reported in international studies [7–10]. This finding likely reflects the lack of standardized diagnostic criteria across the different specialties diagnosing YOD.
This study has a number of strengths. Waikato DHB is a well-defined geographic area with a population that is broadly representative of the New Zealand population age-sex structure. This means the findings can be applicable to the New Zealand population. Secondly, the regional dementia pathway guidelines to primary care practitioners recommend all patients aged under 65 with suspected cognitive impairment are referred for specialist assessment. Almost all referrals are through the public hospital system with only a minority of referrals for cognitive impairment receive a specialist assessment in the private sector. This means that all diagnoses of YOD are made by specialist services and should be captured in this comprehensive review of hospital inpatient and outpatient records. Thirdly, the diagnosis of YOD is generally made in a multidisciplinary team setting so is based on a suite of assessments and investigations.
There are some limitations of this study. This was a retrospective study of YOD diagnoses made across multiple departments, so the approach to assessment and subsequent diagnosis was not standardized. This may explain the high proportion of ‘unspecified dementia’ diagnoses as many of the recorded YOD diagnoses did not specify a subtype. Secondly, dementia is under diagnosed with undetected dementia in the community estimated at over 60% [21] so case ascertainment may not be complete and our findings an underestimate of the true incidence of YOD. Early detection and diagnosis of dementia facilitates the provision of appropriate services for individuals and their families or carers, and ultimately improves prognosis. The high rates of undiagnosed dementia are driven by a combination of factors including both socio-demographic factors affecting health care access and the clinical detection of dementia in primary and secondary care [21]. While the current diagnosis of dementia is largely based on clinical assessment, it is likely that advances in our understanding of laboratory biomarkers and imaging techniques in the coming years will improve rates of detection, diagnosis, and subsequent management of dementia [22].
This study also only included those patients who were aged < 65 years at the time of diagnosis so does not include those diagnosed at a later age but with symptom onset prior to the age of 65 years. Only one of the four private neurology clinics allowed access to their patient database to identify YOD cases so there is a possibility some incident cases were missed. Thirdly, while the referral guidelines for primary care recommend specialist assessment of younger referrals with cognitive impairment, it was not feasible to review primary care records as the diagnosis of dementia is not collated in a centralized database. This means there is a small possibility some diagnoses were made in primary care and therefore missed.
Understanding the epidemiology of YOD is crucial to inform the development of appropriate services for patients and their families and carers. Generalizing the YOD incidence rates reported in this study to the New Zealand population [23] gives an estimated 300 incident cases of YOD per year in 2020, and this is expected to increase in line with population growth and the aging population structure. The higher YOD incidence in Máori is likely due to the higher burden of dementia risk factors and highlights the need for tailored dementia prevention interventions, as well as the need for culturally appropriate services for patients diagnosed with YOD and their carers.