
Abstract
Background:
Quadruple aberrant hyperphosphorylated tau, amyloid-β, α-synuclein, and TDP-43 pathology had been documented in 202/203 forensic autopsies in Metropolitan Mexico City ≤40-year-olds with high exposures to ultrafine particulate matter and engineered nanoparticles. Cognition deficits, gait, equilibrium abnormalities, and MRI frontal, temporal, caudate, and cerebellar atrophy are documented in young adults.
Objective:
This study aimed to identify an association between falls, probable Rapid Eye Movement Sleep Behavior Disorder (pRBD), restless leg syndrome (RLS), and insomnia in 2,466 Mexican, college-educated volunteers (32.5±12.4 years).
Methods:
The anonymous, online study applied the pRBD and RLS Single-Questions and self-reported night-time sleep duration, excessive daytime sleepiness, insomnia, and falls.
Results:
Fall risk was strongly associated with pRBD and RLS. Subjects who fell at least once in the last year have an OR = 1.8137 [1.5352, 2.1426] of answering yes to pRBD and/or RLS questions, documented in 29% and 24% of volunteers, respectively. Subjects fell mostly outdoors (12:01 pm to 6:00 pm), 43% complained of early wake up hours, and 35% complained of sleep onset insomnia (EOI). EOI individuals have an OR of 2.5971 [2.1408, 3.1506] of answering yes to the RLS question.
Conclusion:
There is a robust association between falls, pRBD, and RLS, strongly suggesting misfolded proteinopathies involving critical brainstem arousal and motor hubs might play a crucial role. Nanoparticles are likely a significant risk for falls, sleep disorders, insomnia, and neurodegenerative lethal diseases, thus characterizing air particulate pollutants’ chemical composition, emission sources, and cumulative exposure concentrations are strongly recommended.
Keywords
INTRODUCTION
Falls are usually associated with elderly high-risk populations; however, falls may occur in younger populations. Falls are the leading cause of unintentional injuries in the US. In the Verma et al. study [1], 2.0% of older adults (≥65 years), 1.1% of middle-aged adults (45–64 years), and 0.7% of young adults reported a fall-related injury in the three months prior to the study. The cost of annual unintentional fall-related injuries that resulted in a fatality, hospitalization, or treatment in an emergency department was 111 billion US dollars in 2010 [1]. In the UK, non-spinal fall-related fractures prevalence is 63.1% with 40.7% and 82.7% occurring in males and females, respectively [2]. In young females (20–29 years),>50% of fractures followed falls [2].
Heijnen and Rietdyk [3] studied 94 US undergraduate students (19.9±0.9 years) for 16 weeks. Fifty-two percent fell in the 16-week interval, injuries were reported in 16% of falls, and medical treatment was received in 4% of all falls. Most falls occurred while walking (58%), and the main cause of the fall was a slip (48%) or trip (25%). The authors emphasized the high fall and injury rate reflects the inherent instability of bipedal locomotion and indicates that falls are not a trivial problem for young adults [3]. We fully agreed with them.
Peaks among younger (20–25 years) subjects are observed across the world [4] and variables such as alcohol intake, marijuana use, type of work, use of tools, level of physical activity, prescription medications, and sleep deprivation are important risk factors among young adults [5–7]. Knechel and Chang [8] reviewed the relationship between sleep disturbances and falls and concluded based on 42 papers that people self-reporting>11 h or ≤5 h of nocturnal sleep duration may have a greater fall risk and subjective sleep fragmentation is associated with falls.
Lombardi et al. [9] reported increases in work-related injury risk with decreasing usual daily self-reported sleep hours and increasing weekly work hours, independent of industry, occupation, sex, age, education, and body mass. In the occupational setting, sleep duration and sleep difficulties are predictors for injuries [10]. Alhainen et al. [10] reported employees with short sleep (≤6.5 h) had 1.07-fold odds of workplace injuries (95% CI 1.00 to 1.14) and 1.14 times higher odds of commuting injuries (95% CI 1.04 to 1.26) compared with employees with normal sleep duration. The risk of commuting injuries was higher among those who had difficulty in falling asleep, woke up too early, or had non-restorative sleep.
Sleep is a key part of optimal neurologic function [11, 12] and neurodegenerative diseases alter circadian rhythms [13–15]. Disruption of the sleep/wake cycle occurs early in the trajectory of neurodegenerative processes and may be a risk factor for disease development [14]. The bidirectional relationship between circadian homeostasis and neurodegeneration has been discussed by numerous authors, suggesting that circadian function, sleep disorders, and sleep deprivation play an important role in the progression of neurodegenerative disorders [13–15].
Gait and cognitive abnormalities and fall risk are present in the course of neurodegenerative processes, as seen in elderly fallers [16]. Certainly, environmental factors such as air pollution also alter the circadian rhythm [17], a detrimental impact of great interest to our research group.
The combination of abnormal neural proteins including hyperphosphorylated tau, amyloid-β, α-synuclein, and TDP-43 has been documented in 202/203 forensic autopsies in Metropolitan Mexico City (MMC) residents ages 11 months to 49 years [18–20]. We have studied 4,502 young Mexican residents and documented post-traumatic stress disorder (PTSD) and probable rapid eye movement sleep behavior disorder (pRBD) in urban, college-educated adults (29.3±10.3 years), strengthening the possibility of a connection with misfolded proteinopathies in young urbanites [18–22].
In this neurodegeneration setting, it is of interest that in 575 clinically healthy subjects (21.0±5.7 years) who are residents in Mexican polluted cities, including MMC, 75.4% and 34.4% had abnormal Tinetti and Berg scores respectively and high risk of falls in 17.2% and 5.7% [23].
This young adult study examines falls, pRBD, and restless leg syndrome (RLS) in Mexican middle class, college educated young adults, residing in 100 Mexican cities. Historically, this population has been documented with Alzheimer’s disease (AD), Parkinson’s disease (PD), and TDP-43 pathology, as well as cognitive deficits, abnormal brainstem evoked auditory potentials, gait and equilibrium changes, PTSD and hemispheric cortical, cerebellar, and caudate atrophy associated to cognitive impairment [18–24]. We hypothesize that in this population there would be a strong association between falls, pRBD, and symptoms of RLS [8, 18–24].
We selected two extensively validated instruments: the REM Sleep Behaviour Disorder Single Question Screen (RBD1Q) to assess RBD [25] and the single RLS question [26]. Sleep homeostasis and plasticity [27], fall risk, and neurodegenerative diseases are at the core of our concerns in highly exposed particulate matter ultrafine particles (UFPM) and industrially produced nanoparticles (NPs) in young urbanites.
MATERIALS AND METHODS
Study area air quality
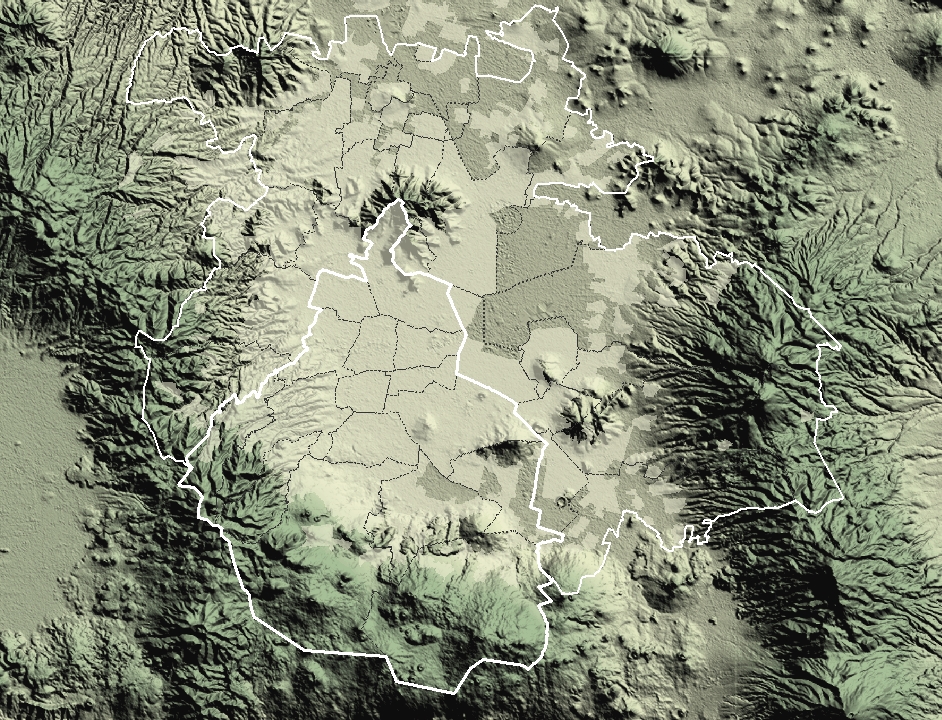
The MMC area covers ∼7,585 km2 on an elevated 2,240-meter basin surrounded by mountain ridges on three sides (Fig. 1) and its home to ∼21.8 million people, ∼5 million vehicles, and over 50,000 industrial establishments. Volatile organic compounds leaks from millions of house LP gas cylinders, hundreds of gasoline stations, gasoline and diesel cars, the use of industrial, commercial, and household solvents, as well as evaporative emissions of thousands of old diesel vehicles, combines with the emissions of nitrogen oxides from nearly 1 million diesel trucks, which, under the influence of intense solar radiation and poor ventilation, result in a strong oxidizing capacity ensuing the production of secondary pollutants [28, 29]. High daily emissions of primary and secondary pollutants in the MMC’s atmosphere have given rise to levels of fine particulate matter (PM2.5) well above the World Health Organization (WHO) guidelines and the US Environmental Protection Agency (USEPA) standards for the last 30 years (Fig. 1).

MMC map showing the location of reference PM2.5 monitoring stations. The inner white contour represents the limits of Mexico City and the secondary contour shows the MMC boundary. Time series show the trends of annual mean 24-h PM2.5 concentrations, averaged over 3 years for five representative monitoring stations of the MMC from 1990 to April 2020 and their comparison with the PM2.5 annual US EPA NAAQS, and the WHO guideline. Data were estimated from measurements reported by the manual PM network of the Secretaría del Medio Ambiente del Gobierno de la Ciudad de México (SEDEMA) under a 6-day sampling schedule. Source of data and figure: http://www.aire.cdmx.gob.mx/default.php# http://www.aire.cdmx.gob.mx/images/monitoreo/mapa-parametros/Mapa_relieve.jpg
{kind=link}
The NE MMC sector (Xalostoc) exhibits the highest PM2.5 concentrations associated with intense industrial and heavy-duty diesel traffic, while the SW (Pedregal) residential area has the lowest PM2.5 concentrations [30]. Exposures to ozone (O3) have been above the USEPA standard (annual fourth-highest daily maximum 8-h concentration, averaged over 3 years) all year long since the 1980 s [31]. Other criteria pollutants, i.e., nitrogen dioxide, sulphur dioxide, carbon monoxide, and lead, have shown a continuous decrease at or below their respective current EPA standards in the last 15 years [28, 30]. In addition, MMC residents are continuously exposed to high levels of black carbon, polycyclic aromatic hydrocarbons, and semi-volatile organic compounds from incomplete combustion of carbonaceous fuels such as gasoline and diesel [31, 32]. These emissions include traces of metals from fuel and lubricating oils, and engine, brake, and tire wear. In the last decade, MMC PM2.5 metals and metalloids have followed a trend: Si > Fe > Al > Ti > Ca > Sr > Zn > Cu > Pb > Cr > Mn [31, 32]. Equally relevant are the presence of highly toxic metals including Hg, more abundant in NE MMC where large industrial facilities including agrochemical, pigments, dyes, pulp and paper, and manufacturing industries, are located [33, 34]. A serious health concern is the fact MMC public transport commuting residents are exposed to high NPs number concentrations [35, 36]. Also, studies in MMC historically have shown that outdoor NPs in proximity to high traffic avenues could reach high numbers [37–48]. UFPMs are particles with size of less or equal to 0.1 micrometers (PM0.1). UFPMs consist of volatile and semi-volatile, carbon-bearing phases and the solid combustion vehicle-derived particles are enriched in highly reactive transition metals, especially Fe, Cu, Mn, Ti, Cr, Ni, V, Pb, and Zn [44, 45]. The abundance of metals in UFPMs follows this order: Fe > Zn > Pb > Mn > Hg > Sn > Ni > Cr > Ti > V > Ag [45]. The heavy-duty diesel old fleet is responsible for the high level of UFPMs emissions in MMC [43].
In a previous work, we had estimated the historical nanoparticle gross number concentration (PNC) for MMC based on the expected linear correlation between NPs, CO, and PM2.5 [49]. For MMC residents born prior to 2002, exposure numbers were calculated in the 300,000 cm–3, while residents born after 2002 have been exposed to PNC levels close to the overall average of 44,000 cm–3 recorded for 40 urban areas of Asia, Europe, North America, and Australia [47]. A key factor to take into account in the above-mentioned PNC estimates, is the fact that is indeed an estimate of NPs, and that altitude is associated with higher breathing rate [48]; thus, NPs inhaled by the average MMC resident are higher than any other polluted city in the world documented so far.
Study population
The study was done with residents of 100 urban areas across Mexico ranging in population from ∼21.8 million, i.e., MMC to cities with ≤10,000 residents. The research was conducted according to the Revised Helsinki Declaration of 2000 and the study was approved by the Universidad del Valle de México ethical and research committees on November 18, 2020. The data collection period was from January 19 to February 21, 2021; an online anonymous survey platform was used, and subjects taking no prescription medications for the previous year were invited to participate, followed by an explanation of the nature and purpose of the survey. The invitation was aimed to college educated adults (≥18 years), professors/students taking University classes online/ and/or working within Campus. Once the adult user consented to participate, they completed a questionnaire with the following information: Demographics, including city of residency, age, sex, formal education years, weight, and height. Fall history, need of medical treatment after the fall, time spend in social media, television viewing, computer/console gaming, discussion forums/chatting online, internet surfing, doing homework, and electronic mails, and intake of energy drinks and caffeine to keep awake. The RBD1Q assessing dream enactment with a single Yes or No response [25, 51], and the RLS unique question were applied [26, 53]. Hours of sleep, early-onset insomnia, waking after sleep onset, daytime somnolence, snoring, and insomnia symptoms, adapted/modified from the Pittsburgh Sleep Quality Index and the Hamilton Depression Rating Scale were used [54–56]. The questionnaire included questions assessing sleep onset, sleep continuity, early morning awakening, sleep duration as well as daytime symptomatology necessary for a diagnosis of insomnia [56].
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Universidad del Valle de Mexico. Adult subjects consented their anonymous participation.
Statistical analysis
We calculated the descriptive statistics of all relevant variables in each group of MMC subjects, non-MMC subjects, and all subjects together. We considered a two-sided type I error rate of 0.05 to be significant when comparing differences between group means. We investigated the volunteers’ fall characteristics, and their relationship with RBD and/or RLS responses. We performed logistic regression analysis based on whether a subject answered yes to RBD and RLS questions, and the predictor variables: Gender, Age, Residency (MMC or non-MMC), Education years, and body mass index (BMI). Next, we performed similar logistic regression analyses on each cohort of MMC residents and non-MMC residents where we remove Residency as predictor. Next, we constructed three cohorts: early onset insomnia, sleep maintenance insomnia, and early morning insomnia. Within each cohort, we calculated summary statistics of several important variables. Finally, we constructed two cohorts: subjects having early onset insomnia and those who did not. In each cohort, we calculated summary statistics of key variables. We also performed logistic regression where the response is whether a subject has early onset insomnia and the following predictors: Gender, Age, Residency, Education years, BMI, pRBD, and RLS. We performed the statistical analyses using Excel and the statistical software ‘R’ (http://www.r-project.org/).
RESULTS
Air pollution
Historical PNC estimates for MMC have been calculated in our previous works [49]. For MMC residents born after 2002, an average of 44,000 cm–3 falls within the range recorded for 40 urban areas of Asia, Europe, North America, and Australia [47]. Exposures to highly toxic NPs containing metals and metalloids from multiple emission sources, including industry, heavy diesel vehicles, and public transport are the main concern for young urbanites [35–47].
Falls, pRBD, RLS, sleep-onset insomnia, and female gender
This is a cross sectional study of 2466 middle class, college educated subjects, 60% women (Table 1); 24% responded yes to the RLS question and 28.78% to the RBD1Q.
Demographics, RLS, and RBD1Q data
Logistic regressions showed a strong association between falls and positive responses to RLS and RBD1Q questions (Table 2). Subjects who fell at least once in the last year had an OR = 1.8137 [1.5352, 2.1426] of answering yes to RBD and/or RLS questions. Separate analysis showed subjects who fell at least once in the last year have an OR = 1.7352 [1.4444, 2.0844] of answering yes to the RBD question and for those answering yes to the RLS question OR = 1.7818 [1.4645, 2.1677]. Females had a higher risk of falls and the need to see a doctor, while higher BMI was a key risk for severe outcomes. Variables such as sleep hours and residency had no impact on the risk of falling or on any sleep variable and alcohol intake was a factor in 2.95% of subjects.
Key variables examined in association with fall risk, sleep parameters, pRBD and/or RLS risk, p-values are shown
*Higher chance for a Yes answer; §Higher chance for higher BMI.
Logistic regressions were performed for checking the dependence of the events such as at least one fall during the last year on the variables BMI, sleep hours, hours on screens, internet surfing, cell phones, use of energy drinks to keep awake, pRBD, and RLS after adjusting age, gender, residency, and education years (Table 2).
Table 3 shows the majority of subjects fell outdoors between 12.01 pm and midnight and complaint of waking up very early in the morning. The average sleeping hours, the insomnia data, and the snoring affecting 41% of the subjects are also shown in Table 3.
Fall location, time of the day, average daily hours of sleep, sleepiness during the day, snoring, and characteristics of the insomnia in all subjects and MMC versus non-MMC
We also evaluated early onset insomnia (EOI) [55] and its association with pRBD and RLS. Logistic regression analysis with EOI as the response and gender, age, residency, education years, BMI, pRBD, and RLS as predictors, showed there was a higher chance of EOI for females (p = 0.0003), and subjects who have EOI have an OR of 2.5971 [2.1408, 3.1506] of answering yes to the RLS question. EOI was seen in younger individuals (29.66±10.95 years) versus subjects with no early insomnia (age 33.78±12.69 years).
Brain regions modulating waking, REM, and non-rapid eye movement sleep are involved in MMC young residents. Wake-on and rapid eye movement-off arousal systems are impacted by highly toxic and reactive nanoparticles and aberrant misfolded proteins (Fig. 2).

Distribution of misfolded proteins and neuropathological hallmarks in the brainstem and hemispheric cortex in Metropolitan Mexico City (MMC) individuals younger than 40 years of age [1, 47]. A) Singh et al. and García-Gomar et al., highly recommended papers [96, 98], are at the core of our arousal and motor brainstem description. The brainstem is an early target of misfolded proteins characteristic of Alzheimer’s disease, Parkinson’s disease, and TDP-43 pathology and pons and caudal midbrain are critical for REM sleep generation [11, 72]. B) Saturation remanent magnetization (SIRM) room temperature values from substantia nigra (SN), tectum, tegmentum, and periventricular gray (TTP) and cerebellar (CB) samples [19] used to calculate magnetite concentrations displayed CE > TTP > SN values. C-E) Cerebellar samples. C) One micron toluidine blue section showing granular, Purkinje (PC) and molecular layers with mild vacuolization of the PC/granular layer interphase. D) Electron micrograph of the Purkinje cell/molecular layer transition with extensive perivascular disrupted neurovascular unit and neuropil vacuolization. Mag×13,300 E) Purkinje cell nucleus with nanoparticles (NPs) in the midst of the heterochromatin (right) and in cytoplasmic lysosomes and mitochondria. Please note one NP in the cell Purkinje membrane (left) in close contact with an adjacent cell wall. Mag×83,300. F) Two-year-old with positive immunoreactive granular cytoplasmic hyperphosphorylated tau in substantia nigra pars compact neurons. PHF-tau8 phosphorylated at Ser199-202-Thr205 (Innogenetics, Belgium, AT-8 1:1000). DAB for brown product. G) Eleven-month-old baby, midbrain neurons showing strong nuclear TDP-43 reactivity and contrasting with negative neuronal nuclei. H) Seventeen-year-old male with hyperphosphorylated tau positive neurites in the midst of SN pars reticulata neurons. I) Same 17-year-old with nuclear strong immunoreactivity to PHF-tau8 in SN pars compacta neurons indicative of DNA damage response. J) Toluidine blue 1 micron section with sparce locus coeruleus neurons in a 33-year-old male. K) Same as J, notice partially degranulated LC neurons surrounded by vacuolated neuropil. L) Twenty-seven-year-old male LC neurons stained with TDP-43 mab2G10 (Roboscreen GmbH, Leipzig, Germany), red product. Notice the negative nuclei in ∼40% of neurons. M) Twenty-seven-year-old LC neurons showing severely degranulated neurons with negative TPD-43 nuclear staining. N-P) Locus coeruleus neurons electron microscopy. N) LC neuron with nuclear NPs and several neuromelanin granules with NPs, Mag×25,000. O) LC neuron with numerous intranuclear NPs and across the nuclear membranes, Mag×83,300. P) Close-up of a LC neuronal cytoplasm to show neuromelanin granules containing numerous NPs, present also in mitochondria with fragmented cristae. Mag×83,300. Q) Thirty-nine-year-old male median raphe neurons stained with TDP-43 exhibit granular cytoplasmic positivity and clear nuclei. DAB×60 [118]. S) Eleven-year-old pontine reticular formation neurons stained with TDP43. Note the strong cytoplasmic red positivity and the negative nuclei.TDP-43 red product Mag×20.
DISCUSSION
This study explores the association between clinical symptoms of pRBD and RLS and the risk of falls, in a young, seemingly healthy, educated, middle class Mexican adult population, 60% women, with published documentation in age-matched populations of AD, PD, and TDP-43 pathology, as well as abnormalities of cognition, olfaction, gait and equilibrium, brainstem auditory evoked potentials, and brain volumetric MRIs [1, 18–24]. This study population is very different than the average fall and sleep behavior disorder cases in the literature composed of older subjects, mostly male, with low socioeconomic status and extensive co-morbidities [50–61]. We are showing a strong association between falls, probable REM-parasomnias, and sleep-related movement disorders in young adults exposed to significant high levels of PM2.5 and UFPM/nanoparticles [1–7, 28–46]. Risk of falling was strongly associated with both pRBD and RLS and the early onset insomnia was mostly seen in females with RLS, coinciding with the literature showing RLS patients’ complaint of sleep onset problems, poor sleep quality and day-time sleepiness [56].
In the US, falls and fall-related injuries are a significant health and safety problem for adults of all ages [1] and although the statistics are driven mainly by falls among older adults, there is an urgent need to define the etiology and fall risk factors and executing prevention efforts across all ages to increase well-being and reduce health care spending [62]. Thus, identifying associations between falls, sleep disorders and neurodegenerative processes is critical to young urbanites residing in highly polluted cities.
Knechel and Chang [8] review showed an association between subjective sleep fragmentation, obstructive sleep apnea, insomnia, and increased fall risk. McDade and coworkers [59] described pRBD in association with gait changes, a key observation knowing gait disorders are common in synucleinopathies. The authors studied 42 pRBD subjects (79.9±4.7 years) and 492 age-matched controls using the Mayo Sleep Questionnaire and assessed gait velocity, cadence, and stride dynamics with an automated gait analysis system. pRBD was associated with decreased velocity, cadence, significantly increased double limb support variability and greater stride time variability and swing time variability. Their results strongly supported pRBD is associated with subtle gait changes prior to an overt clinical synucleinopathy.
Researchers have agreed that the onset of RBD precedes the development of neurodegeneration by several years [57–61]. The work of Boeve et al. [57] it is of great interest to our study: in their 172 RBD cases, 83% males, with an average age at death of 75±9 years, several diagnoses were made, including: PD (n = 151), cognitive impairment (n = 147), and autonomic dysfunction (n = 42). More importantly, Lewy body disease (LBD) (n = 77), combined LBD and AD (n = 59), multiple system atrophy (n = 19), AD (n = 6), and progressive supranuclear palsy (n = 2) were diagnosed at autopsy. In Boeve et al., 94% of RBD patients had documented synucleinopathies [57].
Galbiati and coworkers’ meta-analysis [58] showed the risk for developing neurodegenerative diseases was 33.5% at five years of RBD follow-up, 82.4% at 10.5 years, and 96.6% at 14 years. The average conversion rate was 32% after a mean duration of follow-up of 4.7±2.4 years. The two major diseases RBD patients converted to included PD in 43% and LBD in 25%. We are deeply concerned with Galbiati et al., statement: “estimated risk for RBD patients to develop a neurodegenerative disease over a long-term follow-up is more than 90% ” [58].
What is becoming clear, at least for diseases like PD, is that sleep disorders along neurocognitive and psychiatric outcomes are very common [63] and as discussed splendidly by Mizrahi-Kliger et al. [64], degeneration of non-dopaminergic cell groups and subsequent alterations in circadian rhythms and degeneration of dopaminergic neurons in the brainstem and its resulting effect on the basal ganglia are all critical. Dopaminergic degeneration could drive common complaints such as insomnia both through the resulting motor symptoms of the disease persisting through non-REM sleep and through the dopaminergic denervation of the basal ganglia [64]. The onset of synchronized beta oscillation and a parallel decrease in slow oscillatory activity during non-REM sleep could play a role [64].
Poor sleep quality is associated to hippocampal and posterior cingulate volume loss in cognitively normal older adults [65] and may have a detrimental impact on brain plasticity in mood disorders [66]. In the triad of depression, PTSD, and post-concussive symptoms, sleep disturbances could be the common denominator [67], a major concern in our female MMC populations [22]. MMC mostly females, with PTSD had an OR 2.6218 [2.5348, 2.7117] of answering yes to the pRBD question, strengthening the possibility of a connection with misfolded proteinopathies in highly air pollution exposed young women [22].
The literature of AD and sleep disorders is equally disturbing [12]. Circadian system alterations occur in AD, PD, and frontotemporal dementia [12, 68] with researchers involving glial cells, microglia, and intermittent hypoxia and an activated neuroimmune system to sleep disturbances [69, 70]. Even more preoccupying is the documentation of volumetric and structural brain changes in patients with isolated iRBD [71]. Compared with healthy controls, iRBD patients have widespread decreases of grey matter volume while the increases of grey matter volume in cerebellum, putamen, and thalamus suggest a compensatory effect in the face of neurodegenerative changes [71].
Brain MRI changes in RBD patients are a noteworthy research area [72–75]; differential atrophy of temporoparietal cortices, hippocampus, and amygdala distinguish the younger pRBD patients with a higher likelihood of DLB and lesser AD pathology in the medial temporal lobes in the work of Murray and coworkers [72]. Urso et al. [73] applied the Magnetic Resonance Parkinsonism Index (MRPI), which integrates the pons and midbrain areas and the width of middle and superior cerebellar peduncles, to RBD-PD associated patients and idiopathic RBD cases, and included PD-non-RBD patients as well. MRPI values were higher in the PD-RBD (p = 0.004) compared to PD-non-RBD patients. The authors suggested the MRPI proved to be a significant predictor of REM Behavior Disorder Screening Questionnaire scores in PD (β= 0.195, p = 0.007) and iRBD patients (β= 0.582, p = 0.003).
Sex matters in the greater male global cortical and subcortical gray matter atrophy versus females in the PD-pRBD group and caudate, pallidum, and brainstem volumes were reduced along with cognitive impairment [74]. Rémillard-Pelchat and colleagues [75] emphasized that more than a third of RBD patients have mild cognitive impairment and in their study displayed a widespread pattern of local deformation and volume atrophy in the cortical and subcortical regions, including bilateral insula, cingulate cortex, precuneus, frontal, temporal and occipital regions, brainstem, basal ganglia, thalamus, amygdala, and right hippocampal regions, compared to patients without mild cognitive impairment or controls. Brain deformation was associated with lower performance in attention and executive functions, visuospatial abilities, and higher motor symptoms severity. Thus, RBD is associated with brain structural alterations [72–75] including widespread decreases of grey matter volume and targeted grey matter increases suggesting a compensatory effect [71].
Recent studies have explored glymphatic-system dysfunction and have shown the diffusion tensor imaging (DTI) along the perivascular space (DTI-ALPS) index, is significantly lower in patients with iRBD than in healthy controls [76]. iRBD patients, also showed motor impairment that significantly increases the likelihood of developing LBD [77]. A virtual reality gait paradigm (gait performance while navigating doorways) was paired with functional fMRI in the interesting work of Ehgoetz Martens and colleagues [77] to investigate whether iRBD patients demonstrated worse motor performance and altered connectivity across frontoparietal, motor, and basal ganglia networks compared to healthy controls. iRBD patients had slower and more variable stepping compared to controls and showed an exaggerated response when navigating narrow compared to wide doorways, a phenomenon characteristically seen in PD. Strikingly, iRBD patients also demonstrated less BOLD signal change in the left posterior putamen and right mesencephalic locomotor region, as well as reduced functional connectivity between the frontoparietal network and the motor network, when navigating narrow versus wide doorways [77]. The motor impairments could certainly be a factor for gait abnormalities and risk of falling.
RLS is an interesting player amid neurodegenerative changes. A common neurological disorder affecting up to 15% of the general population [78–80], defined as a sleep-related movement disorder due to its occurrence during or shortly before sleep [81]. The diagnosis is clinical and is based on five criteria: 1) an urge to move the legs, often associated with unpleasant leg sensations; 2) induction or exacerbation of symptoms by rest; 3) symptom relief upon activity; 4) fluctuations of symptoms with worsening in the evening and at night; 5) exclusion of other medical and behavioral conditions that can mimic RLS [81, 82]. RLS predominantly affects the legs but arms, abdomen, pelvis, and the bladder and head can be involved [83, 84]. The iron-dopamine hypothesis has been put forward as a pathogenic RLS pathway [85]. A regional brain iron deficiency and/or specific genetic factors that disturb the neurotransmission of dopamine in the subcortical brain areas have been suggested in the RLS pathogenesis [86, 87]. RLS patients respond to dopamine agonists, supporting a disturbance of dopamine transmission along with a decrease in D2 receptors in the striatum [85]. Interestingly, Jiménez-Jiménez and co-workers [88] described an association between increased serum concentrations of copper, magnesium, selenium, and calcium with RLS, suggesting trace elements, including metals could be involved in the pathogenesis. However, no correlation between systemic iron parameters and substantia nigra iron deposits, as assessed by transcranial sonography, has been shown in RLS [89]. Interestingly, a higher incidence of RLS is found in PD patients than in the general population [80] linking this complaint to the neuropathologic issues suspected in our population. Since the participating volunteers were not taking any medications, we could exclude that the association between falls and RLS is due to medications used to treat RLS, including gabapentin and related compounds for which some of the most common side effects are ataxia and dizziness.
Intriguingly, depression, anxiety, and suicidal thoughts are common in RLS patients [90–92]. Authors found higher level of baseline depressive symptoms is a risk factor for restless legs symptoms in patients with clinical depression [90], while higher scores on affective temperament, depression, and anxiety scales suggest subclinical mood disorders and psychiatric comorbidities in RLS [91]. The work of Chenini et al. [92] is very relevant to MMC women. The authors studied 549 untreated RLS patients and 549 age-, sex-, and education level-matched controls and found depressive symptoms (32.5%) and suicidal thoughts (28%) were 10-fold and 3-fold higher, respectively, in patients with RLS versus controls. The data of moderate-to-severe depressive symptoms in young females and suicide risk associated with depression, impulsiveness, and RLS severity is particularly worrisome, since we have described MMC APOE4 carriers have 4.92 times higher suicide odds (p = 0.0006), and 23.6 times higher odds of NFT V (p < 0.0001) versus APOE4 non-carriers having similar cumulative CPM2.5 exposure and age [18]. Thus, it would be highly desirable to document APOE alleles in RLS patients.
The prevalence of RLS in teenagers is also a concern [93]. Pienczk-Ręcławowicz and coworkers described 2,379 students (aged 13–18 years old) residents in Gdańsk, Poland screened for Restless Legs Syndrome/Willis-Ekbom disease (RLS/WED) with the use of a questionnaire. Children and parents with RLS/WED diagnosis were tested with actigraphy at home for at least two consecutive nights. Twenty-one teens (1%) were diagnosed with definite idiopathic RLS/WED. These children were ∼11 years at the onset of symptomatology, associated with disrupted sleep, behavioral problems (irritability, aggression, hyperactivity), attention deficit, and lowered mood. We found this report very interesting and worrisome; the Port of Gdansk is one of the largest seaports in the Baltic Sea and air pollution is high [94]. Thirty-six of the 50 most polluted cities in the European Union are in Poland. Thus, the possibility of having RLS in children’s resident in highly polluted cities have to be entertained and certainly as seen in MMC residents, polluted environments are key players.
Our results must be discussed in light of the quadruple aberrant proteinopathy (Fig. 2), the presence of solid toxic nanoparticles in noradrenergic and dopaminergic nuclei, and the cerebellum, plus the significant frontal and temporal, caudate, and cerebellar atrophy. Strong associations between MoCA and caudate bilateral, frontotemporal, and cerebellar volumetric changes have been described in young MMC adults [18, 49]. Fe, Ti, Hg, W, Al, and Zn spherical and acicular nanoparticles have been identified in the substantia nigra pars compacta, locus coeruleus (LC) and cerebellum along with early and progressive neurovascular damage and cerebellar endothelial erythrophagocytosis [49]. We strongly suggest NPs could serve as a common denominator for misfolded proteins (hyperphosphorylated tau, amyloid-β (Aβ), α-synuclein, and TDP-43) and could play a role in the brainstem, cortical, and cerebellar pathology associated with sleep, gait and equilibrium alterations and resulting falls and sleep disorders (Fig. 2).
The work of Marta Bianciardi and colleagues and the work of Moruzzi and Magoun, Olszawski and Baxter and Weber and collaborators, is decisive here [95–103]. Singh et al. [96] work has been a unvaluable guide for our current work. Specifically, we went over their targeted neural populations in the brainstem associated with wakeful arousal and motor brainstem nuclei and their high interconnectivity with frontal cortex, basal ganglia, and cerebellum and selected unpublished photomicrographs from three of our works [18, 49] depicting neuropathology in the target area (Fig. 2). In particular, we have shown the extensive involvement of brainstem networks by solid nanoparticles and subcellular pathology at the level of LC and subcoeruleus, both the substantia nigra pars compacta and the reticular portion, the median and paramedian raphe, periaqueductal gray (PAG) and the dorsal raphe in young MMC residents. We have described pathology in the mesencephalic reticular formation in childhood and both the pedunculo-tegmental nucleus and the cuneiform nucleus accumulated α-synuclein [18, 19]. The medullary reticular formation is also involved very early by α-synuclein [18, 19]. García-Gomar et al. [98] described impaired structural connectivity in 14 brainstem nuclei in iRBD patients, including REM-on (subcoeruleus nuclei) and REM sleep muscle atonia (medullary reticular formation) both involved in MMC children. Pontomedullary nuclei were also involved in iRBD [98], while mesopontine regions displayed increased interconnectivity with the frontal cortex, an observation the authors associated with potential compensatory mechanisms. We fully agreed with García-Gomar et al. [98] as we observed similar compensatory phenomena in the auditory pathway in MMC residents and compensatory plasticity, increased auditory gain, cochlear synaptopathy, neuroinflammation, and AD continuum likely playing a role in the evolving auditory pathology in megacity urbanites [104].
Moreover, the significant atrophy observed in MMC adults (32.4±6.3 years) involving the caudate nuclei and cerebellar gray and white matter, along high order cortical regions commonly associated with AD, PD, and frontotemporal dementia and impacting cognition [24] are in keeping with the hypothesis sleep disorders as early components of neurodegenerative diseases [23, 68–77].
The exposure to combustion NPs could be at the core of the neuropathology in MMC residents and the MRI structural changes and would explain the strong association between falls, pRBD, and RLS. Falls are associated to everyday sleep clinical problems such as sleep-onset insomnia [55] patients showing worse balance (odds ratio [OR] = 1.33, 95% confidence interval = [1.16, 1.52]), slower gait speed (OR = 1.52 [1.34, 1.73]), worse motor symptoms, low scores in verbal fluency (OR = 1.24 [1.06, 1.43]), immediate memory (OR = 1.23 [1.08, 1.41]), and prospective memory task (OR = 1.29 [1.11, 1.50]). The risk of falls with a range of sleep disorders and neurodegenerative diseases is unquestionable [5, 57–61].
We are aware of this work limitations, our findings require further validation with a complete sleep evaluation plus the gold standard diagnosis: an overnight video polysomnography, as patients with PTSD may report dream enactment reminiscent of RBD. The screening for pRBD requires that even assuming high sensitivity, a differential parasomnias diagnosis and other disorders, i.e., obstructive sleep apnea must be ruled out. The pRBD questionnaire used in this study has been validated in patients with PD so its specificity in other populations is unclear. The main strengths of this study are the sample size of middle class, educated, young Mexican subjects, the published data on neuropathology, cognition, brainstem auditory evoked potentials, structural brain MRIs, and gait and equilibrium assessments in same target population [19–24, 104].
Conclusions
Our results strengthen the possibility of a robust connection between risk of falls, pRBD, and RLS in young adults, as an indication of early neurodegenerative processes. This information is very important for medical workers, in view of the early accumulation of abnormal neural proteins including hyperphosphorylated tau, amyloid-β peptide, a synuclein, and TDP-43 in residents exposed to high concentrations of highly reactive, oxidative and magnetic iron-rich and non-metal nanoparticles. The pathology changes start in the medulla, olfactory bulb, and the neuroenteric system, and progress as the residents aged; in the forensic study of MMC subjects ages 25.3±9.2 years, 202/203 individuals had the neuropathological hallmarks of AD, 23% of PD, and 18% of TDP-43 pathology [18, 19].
The early aberrant pathology involvement in MMC children and young adults [18–20, 49] of critical brainstem hubs associated with sleep, arousal, and motor processes as splendidly described by several researchers, including the work of García-Omar et al. and Singh et al. from Bianciardi’s group [95–103], is pivotal to explore early neurodegenerative changes. It is important to make emphasis that the main aberrant protein in our cohorts was hyperphosphorylated tau, seen in children’s lower medulla, and in relation with medullary reticular formation. We ought to point out that most of the brainstem and specifically the substantia nigra and LC and the cerebellum, Fe, Ti, Hg, W, Al, and Zn nanoparticles were identified in mitochondria, endoplasmic reticulum, Golgi apparatus, and neuromelanin and inside the nucleus in relationship with heterochromatin [49]. Strikingly, Fe and Hg NPs were seen through the nuclear pores, raising potential and powerful pathomechanisms of cell damage involving nuclear-import receptors [105,106, 105,106] engaging nuclear localization signals of cytoplasmic polypeptides and transporting them across the size selective barrier of the nuclear-pore complex into the nucleoplasm as described in the work of Odeh et al. [105] and in Basu et al. juvenile ALS cases [106].
The complex interplay between early neurodegeneration involving critical arousal and motor brainstem hubs and the high interconnectivity with cortical and subcortical regions [95–98]—involved in young MMC residents—supports a plausible relationship between fall risk and sleep disorders and evolving neurodegeneration. Strikingly, high concentrations of ferrimagnetic NPs from cerebellum > tectum/tegmentum/periaqueductal gray PAG > substantia nigra (Fig. 2) [19, 49] acquire great importance when one considers the critical brainstem hubs involved in arousal and certainly in clinical RBD cases, the complex role of the brainstem and cerebellum in emotions, affective behavior, autonomic output, sleep-wake cycles, posture, gait, and major cholinergic innervations [107–112] and the fact that as Rüb et al. stated: the very early occurrence of the AD-related cytoskeletal pathology in some of these brainstem nuclei points to a major and strategic role of the brainstem in the induction and brain spread of the AD-related cytoskeletal pathology [113].
Millions of people worldwide are being continuously exposed from intrauterine life, to ubiquitous, airborne and environmental, solid, metal and non-metal nanoparticles, highly reactive, oxidative stress generators, including E-waste metals [114–116]. We argue fall risk, pRBD, and RLS in the third and fourth decades of life are likely part of a continuum of neurocognitive, neuropsychiatric, gait, and equilibrium alterations starting in utero and childhood and reflecting ongoing quadruple misfolded proteinopathies. We are aware of the overlap between neurodegenerative diseases [22, 117] and that understanding the interplay between neurodegeneration, sleep disorders, and falls in the first four decades of life ought to be a research priority for one critical reason: identifying subjects at the earliest disease stages will shed light on mechanistic pathways that could be targeted for interventions aimed to avoid or ameliorate neurodegeneration and ultimately to prevent major neurodegenerative diseases including AD, PD, and TDP-43 diseases. Exploring early neurodegenerative changes in exposed air pollution cohorts and accurately measuring NPs will allow the identification of high-risk subjects when treatment can be most effective in arresting its progression.
It is a matter of serious concern that young women were particularly affected by pRBD and RLS; it is important these women be identified, diagnosed, followed-up, and treated.
Finally, we strongly support environmental factors, including air pollution (UFPM) are key factors in the early development of fatal neurodegenerative disease affecting millions of American citizens. Support for studies addressing pediatric and early adulthood signs of neurodegeneration is needed; there is no support for preventive efforts of AD, PD, and TDP-43 diseases that are affecting millions of Americans.