
Abstract
Background:
APOE ɛ4 genotype was correlated with exacerbation of pathology and higher risk of dementia in Parkinson’s disease (PD). Meanwhile, the differential influence of APOE ɛ4 on cognition in young and old individuals interpreted as antagonistic pleiotropy.
Objective:
To examine whether the effect of APOE ɛ4 on cognitive progression in de novo PD is age dependent.
Methods:
In this study, 613 de novo PD patients were recruited from Parkinson’s Progression Markers Initiative (PPMI). To examine the age-dependent relationship between APOE ɛ4 and cognitive changes, we added 3-way interaction of APOE ɛ4*baseline age*time to the linear mixed-effect (LME) models and evaluated the specific roles of APOE ɛ4 in the middle age group and elderly group separately. Cox regression was utilized to examine the progression of cognition in age-stratified PD participants.
Results:
Age significantly modified relationship between APOE ɛ4 and cognitive changes in most cognitive domains (pinteraction <0.05). In the elderly group, APOE ɛ4 carriers showed steeper decline in global cognition (p = 0.001) as well as in most cognitive domains, and they had a greater risk of cognitive progression (adjusted HR 1.625, 95% CI 1.143–2.310, p = 0.007), compared with non-carriers. However, in the middle age group, no significant relationships between APOE ɛ4 and cognitive decline can be detected.
Conclusion:
Our results indicated that the APOE ɛ4 allele has an age-dependent effect on cognitive decline in PD patients. The underlying mechanisms need to be investigated in the future.
Keywords
INTRODUCTION
Cognitive impairment is a common disabling non-motor symptom in Parkinson’s disease (PD) and an important factor in determining patient’s independence and life quality [1, 2]. In all patients with PD, approximately 36% of patients were already suffering mild cognitive impairment (MCI) when they were clinically diagnosed [3], and eventually up to 80% progressed to dementia [4]. Although some drugs have been reported to improve cognition in patients with PD suffering from cognitive deficits, there was insufficient evidence of medications which could delay their cognitive progression [5]. Such facts emphasize the necessity of conducting relevant clinical trials aimed at exploring medications to mitigate or halt cognitive progression in the early stages. However, in patients with PD, the speed of cognitive progression is variable, which hampers treatment trials. Some patients progressed within a few years after PD diagnosis, while others remained non-demented for more than 20 years [6]. Therefore, the identification of PD patients at high risk of cognitive degeneration at an early stage is critical.
Apolipoprotein E (APOE) ɛ4 is the most potent inherited risk factor associated with sporadic Alzheimer’s disease (AD) [7]. Recently, accumulating evidence has shown that a significant association is also found between APOE ɛ4 and cognitive disorders in PD. Previous cross-sectional studies demonstrated that the APOE ɛ4 genotype was linked to poor performance in cognitive domains such as semantic verbal fluency among PD patients [8], but other cross-section studies were unable to validate the associations between APOE ɛ4 and cognition deficits in PD [9, 10]. But to date, most longitudinal studies on PD have provided more reliable evidence indicating that APOE ɛ4 was related to future cognition decline in PD patients [11–13].
It is noteworthy that the influence of APOE ɛ4 on the function of cognition were inconsistent across the lifespan [14, 15]. Previous studies focused on the elderly population neglected to investigate whether the influences of APOE ɛ4 on capacities of cognition were different in the young and middle-aged populations from that in the elderly population [16, 17]. In fact, there is growing evidence that younger APOE ɛ4 carriers might perform even more well in terms of cognition as opposed to non-carriers [18, 19]. In middle-aged population, there was no clear cognitive signature of APOE ɛ4 genotype as in older population and the influence of APOE ɛ4 on cognition decline tends to be subtle and unclear (positive, negative, or null) [20]. However, none of the previous relevant studies assessed the age-dependent influence of APOE ɛ4 on abilities of cognition in PD individuals. The broad age range may obscure the real effects of APOE ɛ4 and confound our comprehension of the specific roles of APOE ɛ4 in cognition among PD patients of different ages. In addition, there is no uniformity regarding the affected cognitive domains. It has been suggested that APOE ɛ4 is significantly linked to cognition decline in several domains, including initiation, construction, conceptualization, and memory [21]. However, a recent longitudinal study demonstrated that APOE ɛ4 was only related to worse performance of semantic verbal fluency [13]. Therefore, the targets of our study were 1) to examine whether the influence of APOE ɛ4 on cognition deterioration is consistent across the age groups of PD patients; 2) to investigate whether the influence of APOE ɛ4 on different cognition domains is consistent.
METHODS
Participants
Parkinson’s Progression Markers Initiative (PPMI) is an ongoing, prospective, longitudinal, observational, international, multicenter study for identifying PD progression biomarkers. All PPMI standardized protocols and data can be found on the PPMI website (http://www.ppmi-info.org/study-design). Authorization for the PPMI study was obtained from the institution reviews committees of all involved institutions and written informed consents were received from each enrollee. On enrolment, de novo PD patients must be on or over thirty years old when diagnosed; must have two of the symptoms among bradykinesia, resting tremor, and rigidity or have only asymmetric resting tremor or bradykinesia; must be less than 2 years of diagnosis; must have not received treatment; must have no examiner-determined dementia; and must not be treated with drugs that may disturb with imaging of dopamine transporter or collection of cerebrospinal fluid (CSF). In order to avoid maldiagnosis, researchers performed examinations of diagnoses longitudinally. Our analyses were restricted to participants with APOE genotyping data. Considering the protective effect of APOE ɛ2 on abilities of cognition [22], patients with genotype ɛ2/ɛ4 were not included in case APOE ɛ2 might confound the impact of APOE ɛ4 on cognition decline. In order to explore the cognitive progression of PD patients, we eliminated PD patients with dementia who were defined as those scored <22 for the baseline Montreal Cognitive Assessment (MoCA) [23]. For analyses of the longitudinal data, at least two years of the follow-up period was required for participants.
APOE genotyping
DNA was obtained from the whole blood of participants, and APOE ɛ2, ɛ3, and ɛ4 alleles were defined through the genotyping of two SNPs (rs429358 and rs7412). The SNPs were genotyped by TaqMan assays on the NeuroX genotyping platform [24]. In the general population, there are six possible APOE genotypes ɛ2/ɛ2, ɛ2/ɛ3, ɛ2/ɛ4, ɛ3/ɛ3, ɛ3/ɛ4, and ɛ4/ɛ4, but the frequencies of ɛ2/ɛ2 and ɛ4/ɛ4 are about 1% and 3%, respectively [25]. Due to scale limitations, we abandoned this type of grouping by APOE genotypes. Therefore, after excluding the APOE ɛ2/ɛ4 allele, we divided the participants into APOE ɛ4+ (with one or more APOE ɛ4 allele: ɛ3/ɛ4, ɛ4/ɛ4) and APOE ɛ4–(without APOE ɛ4 allele: ɛ2/ɛ2, ɛ2/ɛ3, ɛ3/ɛ3) groups.
Clinical assessment measures
After baseline examinations, patients went through follow-up neuropsychological assessments every year. Global cognition was assessed by the MoCA. Neuropsychological testing assessed functions in several specific domains: 1) episodic memory (Hopkins Verbal Learning Test Total Recall; HVLT Total Recall, HVLT Delayed Recall, HVLT Retention, HVLT Recognition Discrimination); 2) visuospatial functioning (Benton Judgment of Line Orientation Score; BJLO); 3) working memory/executive function (Letter Number Sequencing; LNS); 4) language (Semantic Fluency Test, SFT); 5) attention/processing speed (Symbol Digit Modality Test; SDMT).
As a screening instrument for PD, MoCA is preferable over the Mini-Mental State Examination (MMSE). The MMSE has been widely applied in PD-related studies and it could identify the cognitive progression once patients develop dementia. But it is unable to assess executive function and it is not sensitive to the diagnosis of MCI. MoCA could be managed rapidly and makes it possible to identify subtle cognitive impairment in PD, while encompassing major cognition domains [26]. In this study, the definition of the cognitive state is based on MDS level I guidelines: PD with normal cognition (PD-NC) if the MoCA was scored above 26, PD with mild cognitive impairment (PD-MCI) if scored from 22 to 26, or PD with dementia (PD-D) if the MoCA was below 22 [23].
CSF biomarker measurements
The measurement methods of CSF biomarkers could be found in the PPMI biology manual [24]. CSF amyloid-β42 (Aβ42), total tau (T-tau), and phosphorylated tau (P-tau) were measured by INNO-BIA AlzBio3 immunoassay on the xMAP-Luminex platform. CSF total α-synuclein (α-syn) level was measured by Enzyme-linked immunosorbent assay [27].
Statistical analyses
The majority of cognitive scale scores did not follow a normal distribution (Supplementary Table 1). In order to achieve normal distribution, the log10 transformation was used. All analyses in this study utilized log10-transformed values. Exclusion values were considered as under or above the mean value of 3 SD. Twenty-nine participants with outliers at the baseline were excluded to avoid the effects of extreme values. We divided participants into the middle age group (40–59 years old) and the elderly group (≥60 years old) [28]. The baseline characteristics of the APOE ɛ4 carriers and noncarriers among different age groups were summarized, and we compared continuous variables and categorical variables between groups by Student’s t-tests, Mann-Whitney U tests, or chi-square tests, as appropriate.
We investigated the cross-sectional relationships of APOE ɛ4 with levels of cognition and CSF biomarkers in PD patients by linear regression models. Linear mixed-effect (LME) models tested the longitudinal relationships of APOE ɛ4 with cognitive levels and CSF biomarkers. To investigate whether the influence of APOE ɛ4 on cognition was modified by age, we added the 2-way interaction (APOE ɛ4* baseline age) and 3-way interaction (APOE ɛ4*baseline age*time) to the above two models respectively and evaluated the specific roles of APOE ɛ4 in the middle age group and elderly group separately. In order to identify the age window with the fastest rates of cognition decline in PD patients, grouping was performed in more detail. We divided the included population into four age groups (<45 years, 45–59 years, 60–74 years, >75 years) to investigate the relationships between APOE ɛ4 and change of cognition in the LME models.
The relations between APOE ɛ4 and cognition progression were tested by calculating cumulative probability risk for PD patients in different age groups using the Kaplan–Meier curves. Cognition progression was defined as the conversion from CN to MCI/dementia or that from MCI to dementia during the follow-up. Multivariate Cox regression models that corrected by age, gender, and educational level at baseline were conducted to estimate the hazard ratio (HR) of cognitive progression with 95% confidence interval (CI).
Given that the significant correlations between APOE ɛ4 and baseline CSF Aβ42 and P-tau in PD patients were present in the elderly group, we used mediation analyses to assess whether the association between APOE ɛ4 and cognition was mediated by AD pathology. We referred to the calculation methods for the parameters which can fit the linear regression models from previous studies [29]. The first equation regressed the mediator (CSF biomarkers) on the independent variable (APOE ɛ4 status). The second equation regressed the dependent variable (cognition) on the independent variable (APOE ɛ4 status). The third equation regressed the dependent variable (cognition) on both the independent variable (APOE ɛ4 status) and the mediator variable (CSF biomarkers). Below conditions must be achieved for the establishment of the mediation effects: 1) APOE ɛ4 status was related significantly to CSF biomarkers; 2) APOE ɛ4 status was related significantly to cognition; 3) CSF biomarkers were related significantly to cognition; 4) the relationship between APOE ɛ4 status and cognition was reduced but still significant when the regression model was added to include CSF biomarkers (the mediator).
To validate whether the effects of APOE ɛ4 differ depending on amyloid-β (Aβ) status, we stratified PD patients by baseline CSF Aβ. Conversion formula [30] AlzBio3 [x = (CSF Aβ42+251.55)/3.74] was used to transform measurement of CSF Aβ by Elecsys assay, and a cut-off <250 pg/mL was used to define the positivity of CSF Aβ [31]. We investigated the relationships between APOE ɛ4 and cognitive decline among the Aβ+ and Aβ–subgroups in LME models.
The statistical analyses were all performed with R4.1.1. For all tests that were two-sided, p-values below 0.05 were deemed to be significant. In all the above analyses, age, gender, and education were controlled.
RESULTS
Study participants
In total, 613 patients with PD were included, and 225 of them belonged to the middle age group and 368 to the elderly group. In the middle age group, 55 patients were APOE ɛ4+ and 170 were APOE ɛ4–. In the elderly group, 74 patients were APOE ɛ4+, and 294 were APOE ɛ4–. The demographic characteristics were shown in Supplementary Table 2. CSF Aβ42 was significantly less in APOE ɛ4+ individuals versus APOE ɛ4–individuals no matter in the total participants (p < 0.001), the middle age group (p = 0.021), or the elderly group (p < 0.001). Among performance on cognition, only HVLT retention was significantly higher in the middle age APOE ɛ4–group (p = 0.002).
Cross-sectional analyses
We observed that the relationships between APOE ɛ4 and performance of episodic memory (pinteraction = 0.006) were modified significantly by age (Supplementary Table 3). But no significant correlations were observed between APOE ɛ4 and other baseline cognitive indicators except for HVLT retention (β= –0.434, p = 0.005). APOE ɛ4 was significantly associated with lower Aβ42 levels in different age groups (Combined age: β= –0.481, p < 0.001; Middle age: β= –0.362, p = 0.039; Elderly: β= –0.567, p < 0.001) (Table 1).
Cross-sectional and longitudinal regressions according to groups in PD. Significant values are highlighted in bold. For cross-sectional analyses, linear regressions were used to examine the relationships of APOE ɛ4 status with cognition scores and CSF biomarkers. For longitudinal analyses, linear mixed-effect models were used to examine the relationship between APOE ɛ4 status and the longitudinal change of cognition scores and CSF biomarkers. The APOE ɛ4–group was defined as the reference group.
PD, Parkinson’s disease; APOE, Apolipoprotein E; MoCA, Montreal Cognitive Assessment; BJLO, Benton Judgment of Line Orientation Score; LNS, Letter Number Sequencing; SFT, Semantic Fluency Test; SDMT, Symbol Digit Modality Test; HVLT, Hopkins Verbal Learning Test; Aβ42, Amyloid-β42; T-tau, Total tau; P-tau, Phosphorylated tau; α-syn, α-synuclein.
Longitudinal analyses
Our results showed that the impacts of APOE ɛ4 on deterioration of cognition in several cognitive domains represented by global cognition (pinteraction = 0.010) were significantly modified by age (Supplementary Table 3).
Figure 1 showed the mean scores in cognition variables of the different groups across the follow-up visits. Elderly PD patients carrying APOE ɛ4 showed lower cognition scores than other groups and showed a steeper rate of cognitive decline in global functioning (MoCA), visuospatial functioning (BJLO), working memory/executive function (LNS), language (SFT), attention/processing speed (SDMT).

Longitudinal mean changes in the cognition measurements in APOE ɛ4 carriers and noncarriers of different age groups during follow-up. Elder PD patients with APOE ɛ4 showed lower cognition scores than other groups in global functioning (A), visuospatial functioning (B), working memory/executive function (C), language (D), attention/processing speed (E) ,and episodic memory (F-I), but showed a steeper rate of cognitive decline only in global functioning (A), visuospatial functioning (B), working memory/executive function (C), language (D), and attention/processing speed (E). Error bars indicate 95% confidence intervals. I bars indicate standard errors. PD, Parkinson’s disease; APOE, Apolipoprotein E; MoCA, Montreal Cognitive Assessment; BJLO, Benton Judgment of Line Orientation Score; LNS, Letter Number Sequencing; SFT, Semantic Fluency Test; SDMT, Symbol Digit Modality Test; HVLT, Hopkins Verbal Learning Test.
The findings of the LME models were presented in Table 1. In the total participants, the significant association between APOE ɛ4 and cognition progression was only observed in global cognition (MoCA, β= –0.066, p = 0.006), visuospatial functioning (BJLO, β= –0.033, p = 0.043), and executive function (LNS, β= –0.048, p = 0.021). Among elderly PD patients, not only did global cognition (MoCA, β= –0.119, p = 0.001) show faster progression in APOE ɛ4 carriers over noncarriers, but also in visuospatial functioning (BJLO, β= –0.072, p = 0.001), working memory/executive function (LNS, β= –0.104, p = 0.001), language (SFT, β= –0.087, p = 0.001), processing speed (SDMT, β= –0.053, p = 0.047) and episodic memory (HVLT Retention, β= –0.065, p = 0.011). Among middle-aged PD patients, we found a significant relationship between APOE ɛ4 and change of cognition only for processing speed (SDMT, β= 0.058, p = 0.022). Furthermore, significant relationships were found between APOE ɛ4 and a rapid increase of CSF P-tau in total participants (β= 0.033, p = 0.017) and elderly PD patients (β= 0.036, p = 0.045).
Supplementary Table 4 showed the longitudinal results for more detailed age groups. In global cognition, visuospatial functioning, and executive function, APOE ɛ4 carriers showed the most rapid cognitive decline at 60–74 years of age. As for language and episodic memory domain, the age window of fastest cognitive decline is over 75 years of age.
APOE ɛ4 and cognitive progression risk
The survival curves for APOE ɛ4 and cognitive progression were calculated in age-stratified de novo PD participants and were exhibited in Fig. 2. Kaplan-Meier analyses showed the significant difference in APOE ɛ4 carriers and noncarriers among the elderly group (p = 0.021), but not among the middle age group (p = 0.390). And from Cox proportional-hazards models, we can see a significant relationship between APOE ɛ4 and the higher risk of cognitive transformation in elderly groups (adjusted HR 1.625, 95% CI 1.143–2.310, p = 0.007) (Supplementary Table 5).
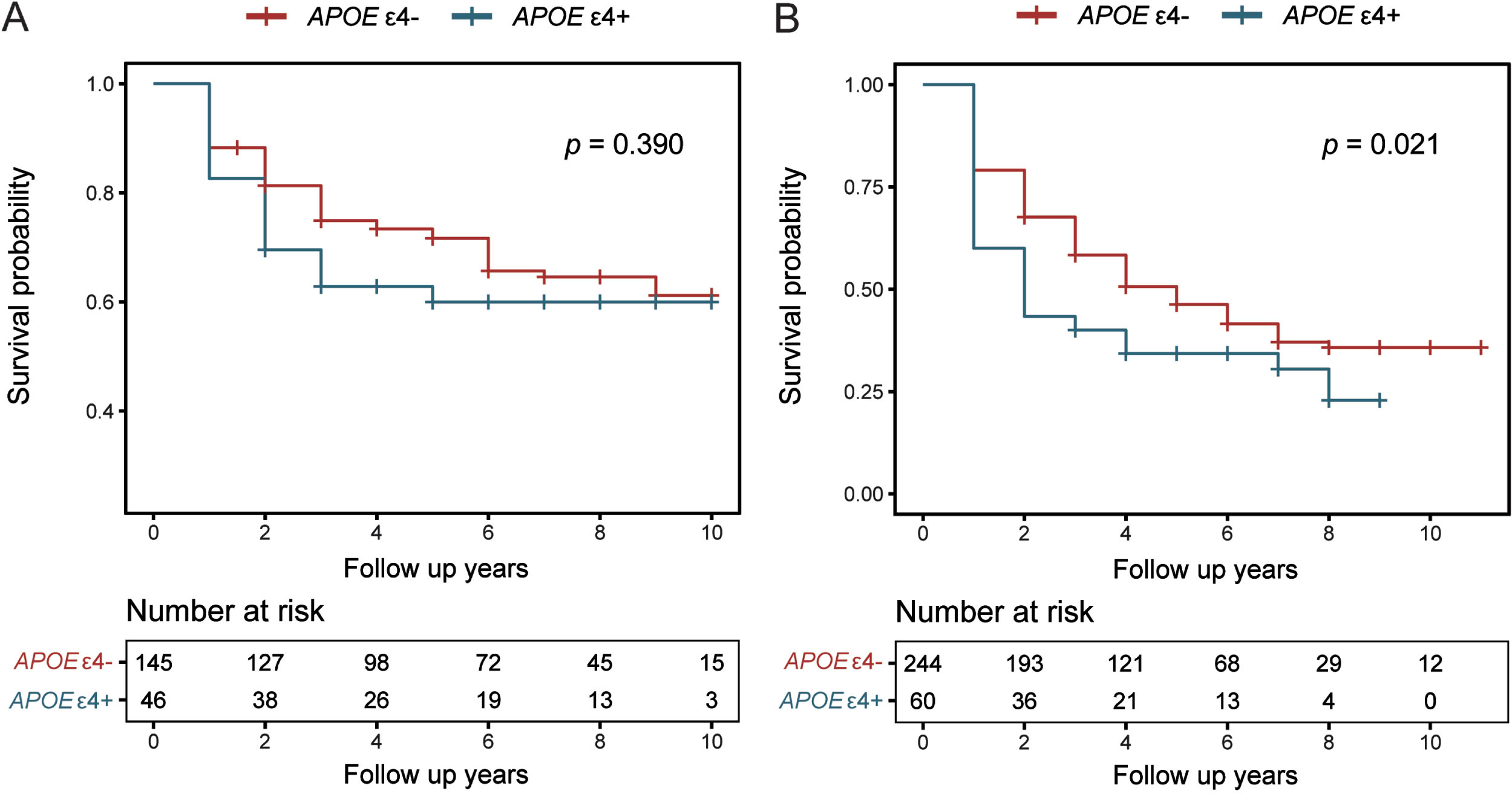
Kaplan–Meier curves showed survival probability of cognition progression in de novo PD patients during 11-year follow-up according to different age groups. A) Middle age. B) Elderly. APOE, Apolipoprotein E; PD, Parkinson’s disease.
Causal mediation analyses
To investigate whether AD biomarkers were potential modulators of APOE ɛ4 on cognitive progression in PD patients, we further performed mediation analyses in the elderly group. Figure 3 showed the relationships between APOE ɛ4 and cognitive decline were mediated by baseline CSF Aβ42. In the elderly group, in the first equation, APOE ɛ4 was associated significantly with lower Aβ concentrations (p = 0.001). In the second regression, APOE ɛ4 showed significant relationships with more rapid cognitive decline in global cognition (MoCA, p = 0.005), visuospatial functioning (BJLO, p = 0.012), and working memory/executive function (LNS, p = 0.003). In the third equation, when putting baseline CSF Aβ42 and APOE ɛ4 into the model, we found that the impacts of APOE ɛ4 on these cognition domains were still present but were significantly diminished. The effect was considered to be partially mediated, with the percentage of mediation ranging from 19.17% to 29.25%. Since there was no significant relationship between P-tau and cognitive progression, the conditions for establishing mediation effects were not met, the mediation relationships of P-tau between APOE ɛ4 and cognitive decline have not established, and the results of the mediation effect were not significant (Supplementary Table 6). Our findings suggest that Aβ can, at least in part, modulate the influence of APOE ɛ4 on cognitive impairment.
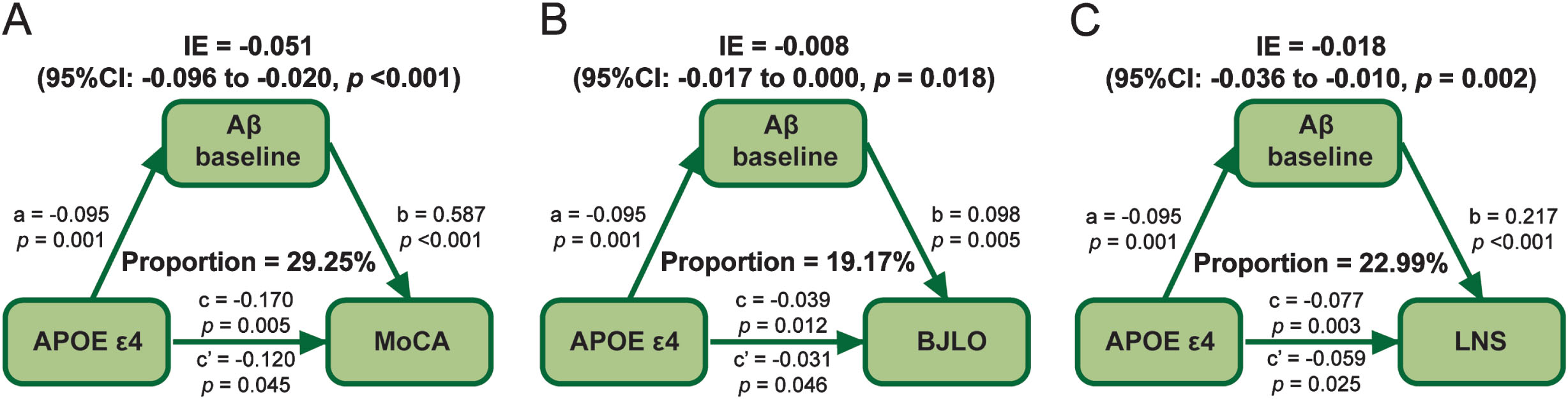
Mediation analyses with cognitive domains, MoCA, BJLO, and LNS as cognitive outcomes in the elderly group. The relationship between APOE status and global cognition measured by MoCA (A), as well as cognition domain of visuospatial (B), and executive (C) function, was mediated by Aβ. IE, indirect effect. The path a, regression model of Aβ on APOE ɛ4. Path b, regression model of the cognition change rates on Aβ. Path c, regression model of cognition change rates on APOE ɛ4. Path c′, regression model of cognition change rates on both APOE ɛ4 and Aβ. APOE, Apolipoprotein E; MoCA, Montreal Cognitive Assessment; BJLO, Benton Judgment of Line Orientation Score; LNS, Letter Number Sequencing.
Subgroup analyses
We performed subgroup analyses to investigate the influence of APOE ɛ4 on cognitive progression changes with different Aβ statuses in PD patients. In the middle age group, neither in the Aβ+ nor in the Aβ–subgroup did PD patients with APOE ɛ4 allele show more rapid cognitive decline than non-carriers. In the elderly group, we observed APOE ɛ4-related cognitive decline only in the Aβ+ subgroup, and only in global cognition (MoCA, β= –0.181, p = 0.007), visuospatial functioning (BJLO, β= –0.092, p = 0.011), and language (SFT, β= –0.122, p = 0.004) were significant (Fig. 4).
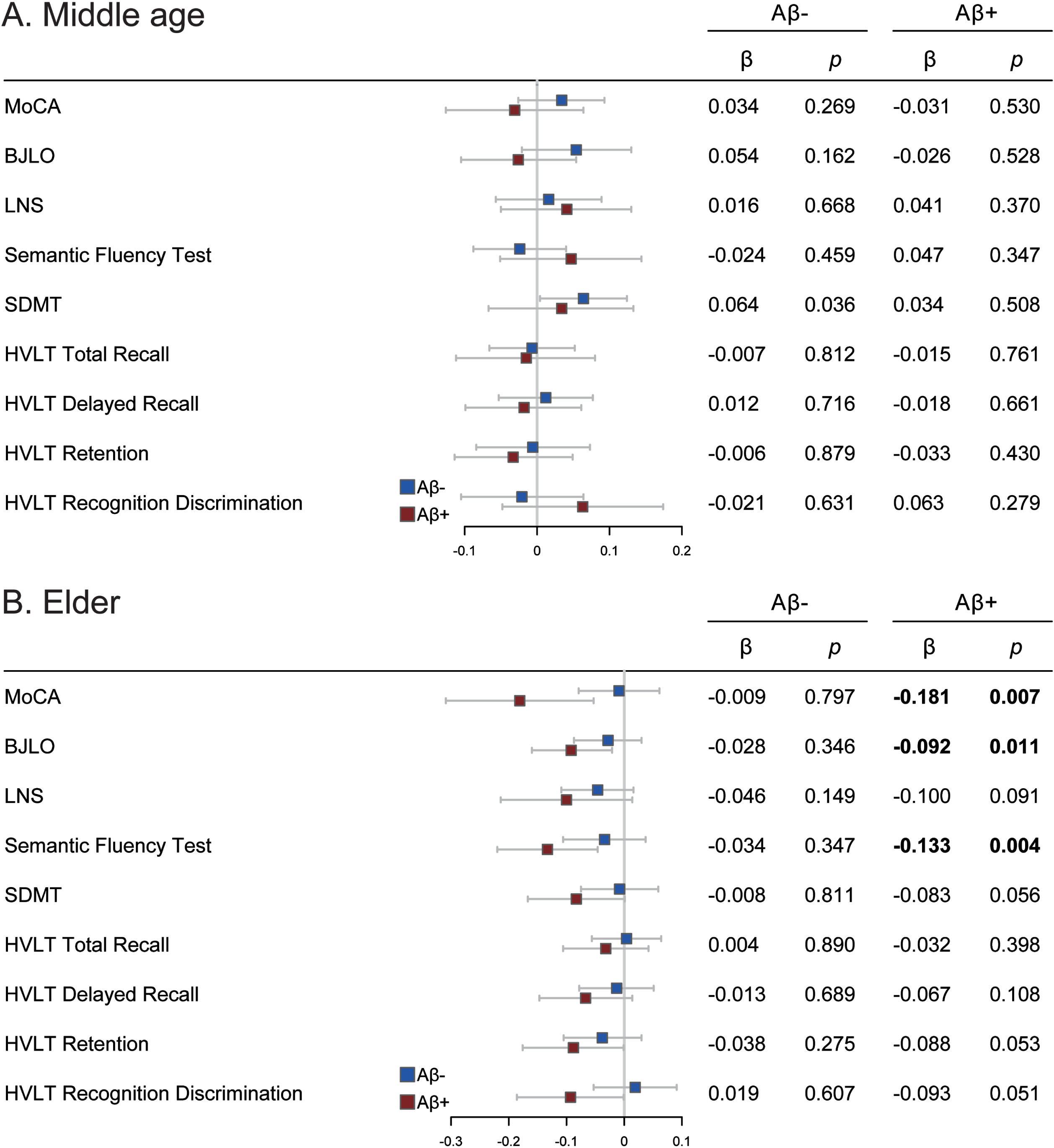
Effects of APOE ɛ4 on cognition in different Aβ subgroups among de novo PD patients. The APOE ɛ4–was used as the reference group. APOE, Apolipoprotein E; PD, Parkinson’ s disease; MoCA, Montreal Cognitive Assessment; BJLO, Benton Judgment of Line Orientation Score; LNS, Letter Number Sequencing; SFT, Semantic Fluency Test; SDMT, Symbol Digit Modality Test; HVLT, Hopkins Verbal Learning Test.
DISCUSSION
With this well-designed prospective longitudinal cohort, we explored the influence of APOE ɛ4 on cognitive ability in different age groups of de novo PD patients. Our results indicated that in PD individuals, 1) the APOE ɛ4 allele differentially influences cognition depending on age, and the relationship of APOE ɛ4 with rapid cognition decline seemed to only exist in the elderly PD population; 2) the effects of APOE ɛ4 were consistent across most cognitive domains. To our knowledge, this is the first study to demonstrate that APOE ɛ4 had age-dependent effects on cognitive progression in PD.
The mechanisms underlying the association between age and APOE ɛ4-related cognition decline remain incompletely understood. Some have attributed this association to the inefficiency of neural repair in APOE ɛ4 carriers [32]. There is evidence that neural repair-related processes are less effective when the APOE ɛ4 rather than the APOE ɛ3 directs the production of APOE, and that APOE ɛ4 carriers have less sprouting of hippocampal granule cell mossy fibers after neural injury [34]. The inefficiency of neural repair in APOE ɛ4 carriers is not evident in young people. But as neuropathology and other burdens increase, APOE ɛ4 carriers had inadequate ability to recover in old age, leading to a breakdown in cognitive resilience and an accelerated cognitive decline. In addition, some studies had used the antagonistic pleiotropy hypothesis to explain the associations between age and APOE ɛ4-related cognitive decline [35]. Antagonistic pleiotropy is a concept in evolutionary biology that proposes some genes which may affect fitness in different ways at different life stages. Specifically, the APOE ɛ4 allele confers cognitive benefits to carriers early in life but causes an accelerated cognitive decline in their advanced age. It has been proposed that APOE ɛ4 achieves antagonistic polymorphism through compensatory mechanisms. In youth, APOE ɛ4 carriers achieve cognitive parity and even cognitive dominance through higher levels of brain activation and recruitment of more brain areas [35, 36]. This compensatory alteration may be beneficial to cognition function in the short term, but it might create a greater pathological burden with long-term deleterious effects on cerebrovascular health. As the pathological burden accumulates sufficiently, compensatory recruitment in ɛ4 carriers will begin to fail and brain activation will decrease, marking the onset of an accelerated cognitive decline [35, 36]. The key to verifying the validity of both hypotheses (insufficiency of neural repair and antagonistic polymorphism) lies in the question of whether APOE ɛ4 has a beneficial effect on cognition early in life, which was still unclear. Some studies suggest that ɛ4 carriers have better cognitive abilities at a younger age [18, 37]; however, not all studies support such results [14, 38]. Future research in this area will help us to better understand the underlying mechanisms.
Several previous longitudinal studies suggested that APOE ɛ4 can contribute to cognitive decline in PD patients [21, 39], while a study has only shown cognitive decline in a single domain [13]. The reason for this discrepancy may lie in the different age distributions of the included populations, with the average age of the former being over 65 years old and that of the latter study being only 61 years old. Since these previous studies did not stratify participants by age, age might have masked the true influence of APOE ɛ4 on cognitive progression. Remarkably, the majority of cross-sectional analyses indicated that APOE ɛ4 was irrelevant to cognitive impairment [9, 40], which contradicted the longitudinal results, and the antagonistic pleiotropy theory may explain this inconsistency. APOE ɛ4 carriers tend to have higher cognitive levels than non-carriers in youth, which allows their cognition to be on a par with that of non-carriers at the beginning of an accelerated cognition decline in their old age, explaining the non-significant differences in some cross-sectional analyses.
The APOE ɛ4 allele has been proven for affecting cognition primarily through amyloid accumulation in the brain [22]. Prior studies also indicated that in PD patients, brain amyloid deposition is involved in cognitive impairment [41]. However, rare studies have explored whether APOE ɛ4 acts on cognition through its effect on Aβ in patients with PD. Our study finds that, in PD patients, Aβ significantly mediated the relationship between the ɛ4 allele and decline in cognitive performance. In addition, a significant APOE ɛ4-related cognition decline was only observed in the Aβ positive group, suggesting that APOE ɛ4 and Aβ may jointly facilitate the deterioration of cognition in PD. It has also been previously reported that PD patients with low Aβ, having one or more APOE ɛ4 alleles, exhibited a steeper rate of cognition decline [42]. Some studies claimed that APOE ɛ4 also affected tau-mediated neurodegeneration [22]. However, we found that the influence of APOE ɛ4 on cognition function was not mediated by tau pathology. This is probably because the participants included in this study were non-demented individuals, in whom tau aggregation is rarely seen [43].
There are several limitations in the study that we should acknowledge. Firstly, the frequency of APOE ɛ4/ɛ4 homozygous is about 3% in the population [25]. Given the scale limitations, this study could not examine whether APOE ɛ4 has a dose-dependent effect on PD cognitive progression, and a larger study cohort in the future is warranted. Secondly, we were unable to prevent sample attrition due to loss of follow-up, which is inherent to longitudinal cohort studies and may have subtle implications on the results. Last but not least, since all analyses were exploratory, we did not make any adjustments to control for type II errors.
Conclusion
In this longitudinal study, we proved that in the de novo PD patients, there are age differences in the effect of the APOE ɛ4 allele on cognition. The mechanisms underlying the age-dependent effect of APOE ɛ4-related cognition decline in PD need to be further explored.
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants from the National Natural Science Foundation of China (82071201, 81971032), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01), Research Start-up Fund of Huashan Hospital (2022QD002), Excellence 2025 Talent Cultivation Program at Fudan University (3030277001), and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University.
Parkinson’s Progression Markers Initiative (a public–private partnership) is funded by the Michael J Fox Foundation for Parkinson’s Research and funding partners, including AbbVie, Allergan, Avid Radiopharmaceuticals, Biogen, BioLegend, Bristol-Myers Squibb, Celgene, Denali, GE Healthcare, Genentech, GlaxoSmithKline, Lilly, Lundbeck, Merck, Meso Scale Discovery, Pfizer, Piramal, Prevail Therapeutics, Roche, Sanofi Genzyme, Servier, Takeda, Teva, UCB, Verily, Voyager Therapeutics, and Golub Capital. Data used in the preparation of this article were obtained from the Parkinson’s Progression Markers Initiative (PPMI) database (http://www.ppmi-info.org/data). For up-to-date information on the study, visit ![]() .
.