
Abstract
Background:
Observational studies have found that vitamin D supplementation is associated with improved cognition. Further, recent Mendelian randomization (MR) studies have shown that higher vitamin D levels, 25(OH)D, may protect against Alzheimer’s disease. Thus, it is possible that 25(OH)D may protect against Alzheimer’s disease by improving cognition.
Objective:
We assessed this hypothesis, by examining the relationship between 25(OH)D levels and seven cognitive measurements.
Methods:
To mitigate bias from confounding, we performed two-sample MR analyses. We used instruments from three publications: Manousaki et al. (2020), Sutherland et al. (2022), and the Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021).
Results:
Our observational studies suggested a protective association between 25(OH)D levels and cognitive measures. An increase in the natural log of 25(OH)D by 1 SD was associated with a higher PACC score (BetaPACC score = 0.06, 95% CI = (0.04–0.08); p = 1.8×10-10). However, in the MR analyses, the estimated effect of 25(OH)D on cognitive measures was null. Specifically, per 1 SD increase in genetically estimated natural log of 25(OH)D, the PACC scores remained unchanged in the overall population, (BetaPACC score = –0.01, 95% CI (–0.06 to 0.03); p = 0.53), and amongst individuals aged over 60 (BetaPACC score = 0.03, 95% CI (–0.028 to 0.08); p = 0.35).
Conclusions:
In conclusion, our MR study found no clear evidence to support a protective role of increased 25(OH)D concentrations on cognitive performance in European ancestry individuals. However, our study cannot entirely dismiss the potential beneficial effect on PACC for individuals over the age of 60.
Keywords
INTRODUCTION
According to the Canadian Census Bureau, the population of individuals aged 85 years and older is projected to triple over the next 25 years to 2.5 million [1]. Further, the incidence of dementia-related diseases increases exponentially for individuals 90 years and older [2]. Therefore, identifying therapeutic targets and enhancing our understanding of age-related neurodegeneration is necessary.
Some studies have demonstrated a higher prevalence of low 25-hydroxyvitamin D 25(OH)D levels in the elderly population [3, 4]. Further, cognitive decline and loss of autonomy in the elderly, which are key drivers of Alzheimer’s disease (AD), have been observed in individuals with hypovitaminosis D [5]. There is a wide range of pathways through which vitamin D may influence brain health, including inflammation, thrombosis, and growth factors [6, 7]. Several observational studies have suggested that vitamin D may play a role in modulating neuronal development, increasing senescence, reducing sensory and social acuity [8–10]. Meta-analyses of the association of vitamin D and the incidence of stroke and the risk of dementia found a dose-response association between vitamin D levels and the occurrence of these conditions [11, 12]. Since vitamin D levels can be increased with relative safety, doing so could potentially help to protect against cognitive decline.
The preclinical Alzheimer’s cognitive composite score (PACC) [13] tests multiple cognitive parameters. The meta-analysis from which the score was derived demonstrated a strong association of the score with the gene encoding for the apolipoprotein E ɛ4 polymorphism [14]. These genetic variants are clear risk factors AD, implying that the PACC score provides a way to assess cognitive impairment related to AD, as they share some underlying biological determinants.
Gaining insight into the causal estimated effect of vitamin D on cognitive function is crucial for enhancing our comprehension of widespread findings from observational study data demonstrating an association of 25(OH)D with cognitive function. However, such studies may be biased by confounding, and previous work has shown that several observed associations between vitamin D levels and disease outcomes cannot be corrected by vitamin D supplementation in large-scale randomized trials, however we note that the individuals studied did not necessarily have low 25(OH)D [15–22]. What is therefore needed is a method to test the relationship between vitamin D levels, but with less bias from confounding.
Mendelian randomization (MR) is a genetic epidemiology causal inference method that uses instrumental variables to reduce bias from confounding and reverse causation [23, 24]. In contrast to the aforementioned observational studies, a one-sample MR study within a meta-analysis investigating the impact of vitamin D on cognition yielded no clear evidence that 25(OH)D levels are a causal factor of cognitive performance [25]. Additionally, different ways to measure cognition (including memory and global cognition scores) amongst the different cohorts made the cognition measurements heterogeneous. Finally, the study employed just two SNPs (CYP2R1, DHCR7) associated with 25(OH)D, thus reducing the variance explained in 25(OH)D levels and, consequently the study’s statistical power.
On the other hand, recent MR studies have demonstrated that higher 25(OH)D levels protect against AD [26]. Since cognition is an important risk factor for AD, it would be important to better understand if higher 25(OH)D levels were protective for cognition and if these results depended upon age.
Therefore, to better understand the influence of circulating 25(OH)D levels on cognition, we undertook a large-scale observational study, testing the association of 25(OH)D with cognitive scores in up to 26,622 individuals in the Canadian Longitudinal Study of Aging (CLSA) (Supplementary Table 1). Next, we used MR to better understand if these associations were influenced by confounding using SNPs from three publications: Manousaki et al. (2020) [28], Sutherland et al. (2022) [30], and the Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021) [31] as genetic instruments (Fig. 1). The results provide insights into the estimated effect of 25(OH)D levels on cognition in humans.
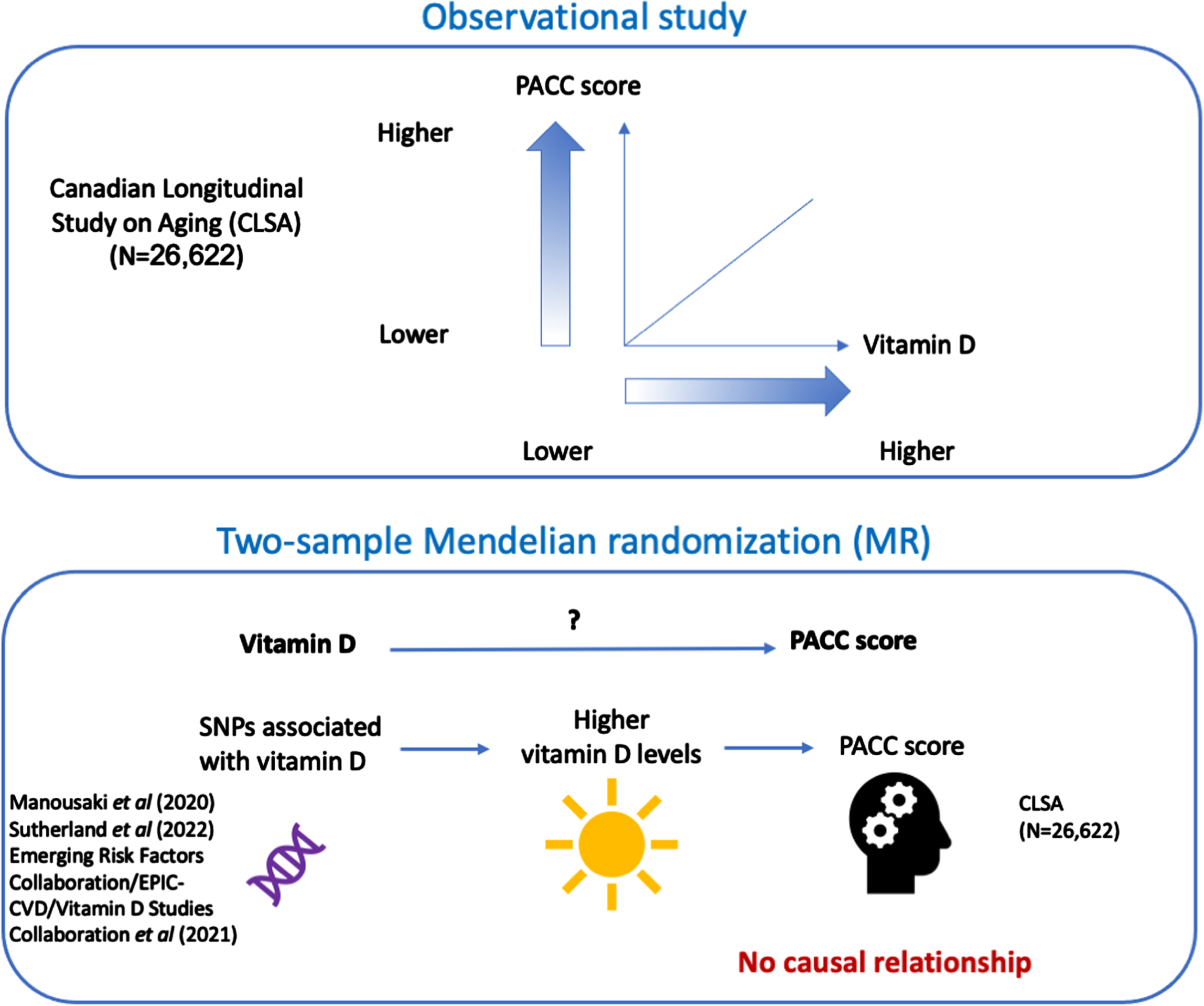
Overview of the design and main results of this study.
METHODS
Observational associations
Using linear regression, we tested the association of log-transformed 25(OH)D with each cognition score (AFT, AFT2, MAT, REYI, REYII, COLTIME) and with the composite cognition score, the PACC score. These scores are described below in Study Outcomes. Since 25(OH)D is confounded by various factors [20] (anthropometric variables, lifestyle habits, and more), we identified covariates available in the CLSA cohort to add to our regression model to partially control for this potential bias. Cognition scores were adjusted for age, sex, smoking status (answered on a questionnaire with possible answers: Yes (I currently smoke), No (I don’t smoke and I never have), Former (I don’t smoke now but I have in the past), high nutritional risk indicator (answered on a questionnaire with possible answers: Not at high nutritional risk, and High nutritional risk), and BMI classification for adults aged 18 and over (the classification includes underweight, normal weight, overweight, obese –Class I, obese –Class II, obese –Class III). Cognition scores were inverse normal transformed. All measures were assessed at baseline and included at most 26,622 individuals. We repeated the analysis stratifying the regression model by sex. To control for multiple testing, we considered Bonferroni significant those associations with p < 7.1×10-3 (which is equal to 0.05/7, where 7 is the number of cognitive scores tested). All patients gave informed consent in the originalstudy [27].
Instrumental variables for 25(OH)D
Instrumental variables were defined as independent genome-wide significant SNPs (p < 6.6×10-9) for 25(OH)D levels in 443,734 individuals as per the genome-wide threshold defined by Manousaki et al. (2020) [28]. Identification of independent loci excluded high collinearity (R2 > 0.9) SNPs within a 20,000 kilobase window. Details on the conditionally independent approach, imputation quality control, missingness rates, excluded individuals, and software tools employed in the GWAS are provided in detail by Manousaki et al. (2020) [28]. This approach yielded 138 independent SNPs. In order to ensure that we are able to recover all the variants from the outcome GWAS, we restricted our study to SNPs with a MAF > 5%. When a SNP was not present in the results for the GWAS of the PACC, AFT, AFT2, COLTIME, REYI, REYII, and MAT score, we alternatively looked up a proxy SNP in linkage disequilibrium, with an R2≥0.8 using the 1000 G European reference panel [29] (Supplementary Table 2). Therefore, we limited our analysis to 80 SNPs for which we estimated the variance explained in 25(OH)D. We computed the variance explained using the following formula: r2 = 2β2 f (1 – f), where β and f denote the estimated effect of the SNP on 25(OH)D level and the MAF, respectively. Which we then used to calculate the F-statistic (formula F: r2 (N-2)/(1-r2)) where r2 is the variance explained and N denotes the sample size.
Next, we repeated our analysis by utilizing instrumental variables chosen in two separate studies and assessed the variants’ pertinence to 25(OH)D levels. These variants were evaluated for their statistical power, biological specificity, and risk of bias caused by horizontal pleiotropy. The first study included 35 variants derived from 307,601 unrelated UK Biobank participants of white European ancestry which had an association which replicated for 25(OH)D in the SUNLIGHT consortium [30] (Supplementary Table 3). The second study included 21 variants derived from 431,489 individuals, comprising 67,992 from the Vitamin D Studies Collaboration (VitDSC), 14,941 from the European Prospective Investigation into Cancer and Nutrition— Cardiovascular Disease (EPIC-CVD), and 348,556 from the UK Biobank [31] (Supplementary Table 4).
Study outcomes
The PACC score is a composite score which tests episodic memory, timed executive function, and global cognition. The composite measure can precisely recognize early signs of cognitive changes prior to mild cognitive impairment (MCI) [13]. Concerning the individual scores, the Rey auditory verbal learning test – trial 1 and 5-min delayed recall (REYI, and REYII respectively) scores represent the number of words correctly recalled within a 90-s span. The first assesses verbal episodic memory, whereas the second assesses delayed recall. The mental alteration test (MAT) score assesses the number of correct consecutive numeric and alphabetical alternations in 30 s. The time to say the ink color of each color name (COLTIME measured in seconds) ascertains the executive and the set switching cognitive domains. Finally, animal fluency (AFT & AFT2) assesses the number animals recited in 60 s. Table 1 summarizes the individual cognitive scores in CLSA.
CLSA cognitive measurements used in this study
For each of the cognition scores (PACC, AFT, AFT2, MAT, COLTIME, REYI, REYII) we retrieved the effect size estimates of these 80 variants derived from GWAS performed in the CLSA [21] to perform our MR study. GWAS summary statistics for the cognition scores are available in the GWAS catalogue (See Data Availability section). Since 92.6% of CLSA participants are of European ancestry [27], our analysis focused on individuals with European ancestry individuals (N = 21,065). Population structure was assessed through principal component analysis as detailed elsewhere [27]. We employed REGENIE v3.2.5 [32] to perform association tests, which we adjusted for sex, age, and the first 20 principal components. We stratified our analysis based on age, testing the causal relationship for the entire cohort and for individuals aged 60 and above (N = 13,678). This approach allowed us to compare the effect of age on the cognitive scores.
Mendelian randomization
Units
For the cognition scores, one standard deviation change in cognitive scores was expressed according to a one standard deviation increase in genetically predicted natural log of 25(OH)D (which was measured in nmol/l).
Two-sample MR
We performed the two-sample MR analyses using multiplicative random effect inverse-variance weighted (referred to as IVW(re)) analysis to estimate the effect of 1 SD increase in standardized natural log-transformed 25(OH)D on 1 SD of PACC, AFT, AFT2, REYI, REYII, MAT, COLTIME scores. We additionally stratified our analysis by age (individuals above 60 years of age versus all individuals) when estimating the effect on cognitive scores. Our analyses were performed with the package TwoSampleMR (v 0.5.6) [33] in R(v4.2.0). We considered significant MR results with a p < 7.1×10-3 (Bonferroni threshold accounting for multiple testing for the seven cognition scores: 0.05/7).
MR assumptions
Three main assumptions are required in MR analyses. The first MR assumption requires that the genetic instrument must be strongly associated with the exposure. For all sets of instruments, we selected the genome-wide significant variants based on the significance threshold specified in their respective publications (Supplementary Tables 2–4).
The second MR assumption stipulates that genetic instruments should not be correlated with confounders that are a common cause of the exposure and the outcome [34].
The third MR assumption requires the instruments to influence the outcome only via their effects on the exposure (the exclusion restriction assumption), i.e. that horizontal pleiotropy does not influence the results. We, therefore, investigated for the presence of directional horizontal pleiotropy in our study. First, we calculated MR Egger regression slope and intercept, in addition to IVW median and IVW mode. MR-Egger is a weighted linear regression which allows the estimation of an intercept as a measure of the average horizontal pleiotropic effect and produces a slope coefficient that is less prone to bias from directional horizontal pleiotropy. MR-Egger relaxes the exclusion restriction assumption and is valid under the Instrument Strength Independent of Direct Effect (InSIDE) assumption wherein associations of the genetic variants with the 25(OH)D would be independent of direct effects of the genetic variants on the cognitive score. Additionally, we performed a weighted median analysis which weights MR estimates by the effect size/standard error. This approach leverages the fact that causal estimates from non-pleiotropic instrumental variable are more probable to converge toward the median. This approach provides reliable causal estimates when at least 50% of the weight from variants are valid instruments. Additionally, we assessed Cochran’s Q test. The test yields an I2 index which gives an estimate of the amount of heterogeneity amongst IVs (I2 index≤25%, is considered low heterogeneity, and a I2 index > 50% is considered high heterogeneity). Finally, we employed MR-PRESSO global test, which can detect the presence of pleiotropic outlier SNPs. By undertaking this variety of sensitivity analyses, and comparing results using these approaches, each one with different underlying assumptions, we could assess, to some degree, whether our findings were biased by horizontal pleiotropy. We considered results significant when P-values were < 0.05 for all horizontal pleiotropy tests (MR-Egger intercept test, Cochran’s Q test, MR-PRESSO global test).
This study was conducted in accordance with the STROBE-MR guideline [29] (STROBE-MR checklist is provided in Supplementary Material.
Association of late-onset AD polygenic risk score and cognition traits
The effect size estimates of 22 variants associated with the risk of late-onset AD in European ancestry individuals were obtained from the Polygenic Score Catalog (PGS Catalog). Briefly, the PRS was derived using a clumping and thresholding approach from both the UK Biobank and the IGAP cohorts. Further details of the PRS can be obtained from Zhang et al. (2020) [35] and data is available through the accession: PGS000334. We calculated the risk score for everyone in the CLSA and performed a linear regression adjusting for age, sex, and the first 20 principal components for all the cognition traits (PACC, AFT, AFT2, MAT, REYI, REYII, COLTIME). We employed PRSicev2.3.5 [36] for both PRS computation and association.
LD score regression analysis
We next examined the genetic correlation between the PACC score in older individuals and clinically diagnosed AD and AD-by-proxy [37] in European ancestry individuals using summary statistics GWAS. We used linkage-disequilibrium score regression (LDSC v1.0.1) [38] to calculate the genetic correlation between the PACC score in older adults and AD. We performed the analysis using 1000Gp3v5 LD reference data and high-quality variants from HapMap3 as recommended by the LDSC software package.
RESULTS
Observational associations
All of the associations (Table 2) between log-transformed 25(OH)D and the seven cognitive scores (the individual scores and the composite score) adjusted for age, sex, smoking status, nutritional index, and BMI classification were Bonferroni significant (p < 7.1×10-3). While the direction of effect between 25(OH)D and most of the cognition scores was positive, we observed a negative association between the vitamin D and the performance in the executive and set switching tests. These tests gauge the time taken to name ink colors (COLTIME). This means that higher 25(OH)D levels were associated with improved COLTIME. Thus higher 25(OH)D was consistently associated with improved cognition in observational associations. We repeated the analyses above, but this time stratifying by sex. Our findings revealed that the direction of effect for all the cognition traits remained consistent with the model in which we controlled for sex. The noticeable difference is that the results were more significant in males than females.
Observational associations between the natural log 25(OH)D and cognitive scores in CLSA. Associations were adjusted for age, sex, smoking status, BMI classification, and high nutritional risk indicator using linear regression. Sex-stratified associations were adjusted for all the previously mentioned covariates except for sex using linear regression. Scores are presented in standard deviation units, and vitamin D is log 25(OH)D. AFT, Number of different animals recited in 60 s; REYI, Number of words (or variants) correctly recalled in 90 s (immediate recall); REYII, Number of words recalled in 90 s (delayed recall); MAT, Number of correct consecutive numeric and alphabetical alternations in 30 s; COLTIME, Time to say ink color of each color name (in seconds); N, sample size; Beta (95% CI), association of an increase in one unit of log 25(OH)D with each cognitive score, measured in standard deviation units. 95% confidence intervals are displayed in parentheses
Instrumental variables for 25(OH)D
We used 80 common (MAF > 5%) independent SNPs (Supplementary Table 2) explaining 3.8% of the variance in 25(OH)D levels, with an F-statistic of 214.75 as instruments in our MR study. 16 SNPs were absent from the PACC score GWAS and were replaced by proxies in high LD (r2 > 0.8). TwoSampleMR (v 0.5.6) identified rs10832289, rs11182550, and rs13336347 as palindromic and were therefore removed from further analyses. An additional 5 SNPs (rs145432346, rs200641845, rs3775150, rs201501563, rs62130059) were removed from further analyses because proxies in the PACC score GWAS could not be found. Of the 35 variants from Sutherland et al. (2022) [30], 5 were replaced by proxies (Supplementary Table 3). Out of the 21 variants from Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021) [31], one (rs187639972) could not be retrieved in the exposure GWAS, and 4 were replaced by proxies (Supplementary Table 4).
GWAS of the PACC score
We performed a genome-wide study of the PACC score in European ancestry individuals from the CLSA. Our analysis was stratified by age, encompassing individuals aged 60 years and above (N = 13,678), as well as the entire cohort (N = 21,065). When we restricted our analysis to individuals aged 60 and older, we found a strong association (p = 3.5×10– 7) between the PACC score and the well-characterized missense apolipoprotein APOE variant, rs429358 (Supplementary Figure 1). When we did not restrict by age, the association was attenuated (p = 2.5×10– 4). This locus plays an important role in dementia and AD[39–41].
Mendelian randomization: Cognitive scores as outcomes
For the PACC score, using the set of 80 instruments selected based on MAF and p, MR showed that the genetically predicted increase per 1 SD in natural log of 25(OH)D had no clear estimated effect on the PACC score estimated in the general population (BetaPACC–All = –0.01, 95% CI –0.06–0.03, p = 0.53). Results were consistent in individuals over 60 (BetaPACC–Age >60 = 0.03, 95% CI –0.028–0.08, p = 0.35) (Fig. 2A, Tables 3 and 4). Using the set of instruments from Sutherland et al. (2022) [30], MR also showed no estimated effect on the PACC score (BetaPACC–All = –0.01, 95% CI –0.05 –0.03, p = 0.78; BetaPACC–Age >60 = 0.03, 95% CI –0.02–0.08, p = 0.22) (Fig. 2B). Finally, using the set of instruments from the Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021) [31], MR showed no effect on the PACC score (BetaPACC–All = –0.01, 95% CI –0.05–0.03, p = 0.71; BetaPACC–Age >60 = 0.04, 95% CI 0.0007–0.08, p = 0.05) (Fig. 2C).
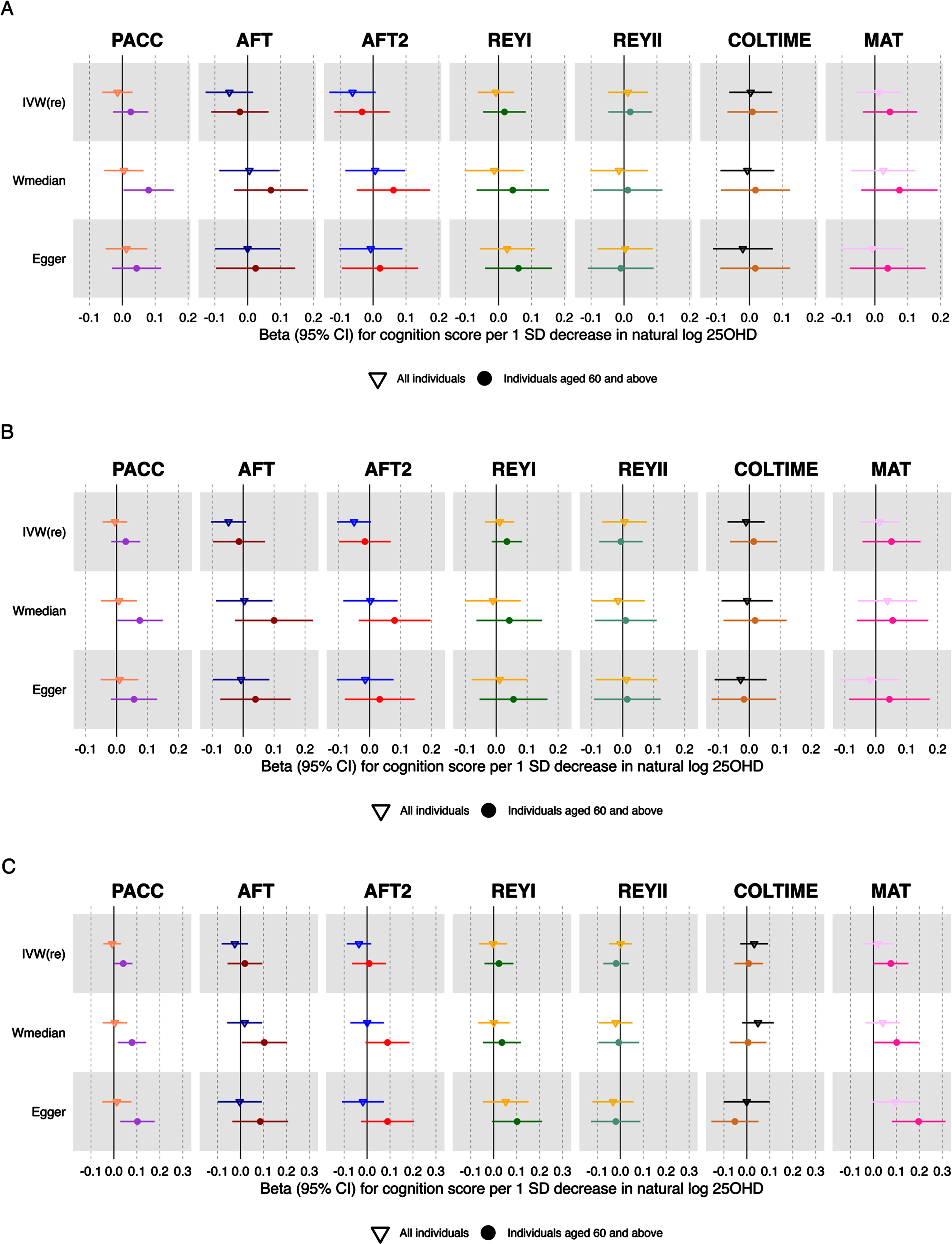
Forest plot of MR studies investigating the genetically predicted increase in the natural log 25(OH)D on PACC, AFT, AFT2, REYI, REYII, COLTIME, and MAT scores. Forest plots of the main study and the sensitivity analyses. Significance threshold as a Bonferroni p < 7.1×10– 3. MR, Mendelian randomization; IVW(re), random effect inverse weighted variance; Wmedian, weighted median; 25(OH)D, 25-hydroxyvitamin. PACC, AFT, AFT2, REYI, REYII, COLTIME, and MAT are defined in Table 1. A) Forest plot utilizing 80 instruments chosen from the pool of 138 SNPs that are conditionally independent and possess a minor allele frequency (MAF) greater than 5%, while also having a p < 6.6×10– 9. B) Forest plot utilizing 35 instruments from Sutherland et al. (2022) [30]. C) Forest plot utilizing 21 instruments from the Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021) [31].
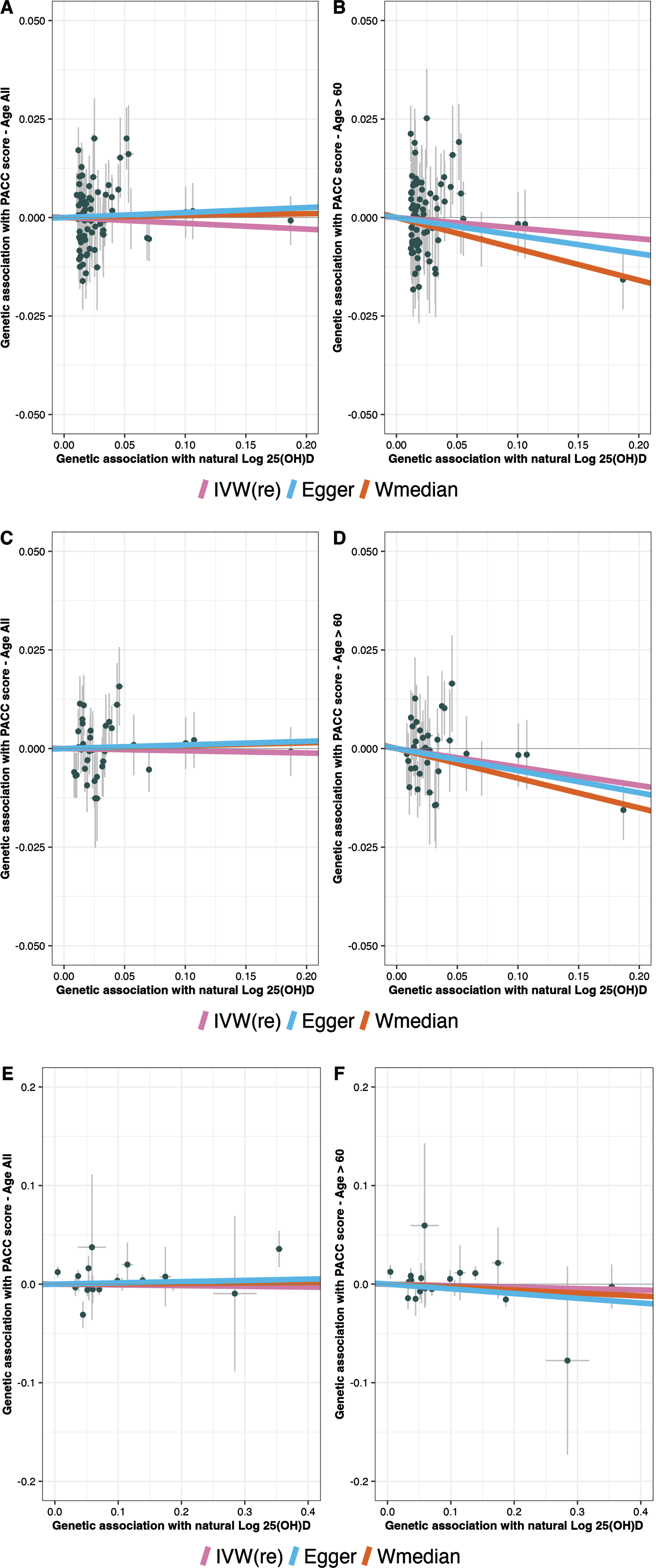
Scatter plots of the genetically predicted increase in natural log 25(OH)D MR analyses. A) PACC score for all individuals. B) PACC score for individuals aged 60 years and above. A genetically predicted increase in the natural log of 25(OH) D does not have a clear effect on a 1 SD of PACC score (for all individuals: beta = –0.02, 95% CI: –0.060– 0.030, p = 0.53; for individuals 60 years and more: beta = –0.03, 95% CI: –0.08–0.03, p = 0.33. Panels A and B presents the MR results which utilize 80 instruments from the pool of 138 SNPs that are conditionally independent and possess a minor allele frequency (MAF) greater than 5%, while also having a p < 6.6×10– 9. Panels C and D presents the MR results which utilize 35 instruments from Sutherland et al. (2022) [30]. Panels E and F presents the MR results which utilize 21 instruments previously published in Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021) [31]. Each dot represents a genetic instrumental variable. Three lines represent causal estimate (βIV) by the inverse variance weighted (IVW) method (pink), MR– Egger method (blue), and Weighted median method (orange). Error bars represent 95% CIs. MR, Mendelian randomization. For visualization purposes, (B) the IVW line was dashed since it overlaps with the MR-Egger line.
For AFT, AFT2, REYI, REYII, MAT, and COLTIME, the MR results were consistent with those from the PACC score. There was no discernible estimated effect of genetically predicted increase per 1 SD in the natural log of 25(OH)D on any of these scores (Tables 3 and 4).
MR effect estimates per 1 standard deviation (SD) increase in genetically predicted increase in the natural log of 25(OH)D on cognitive scores (measured in SDs) for individuals aged 60 and above in the CLSA. IVW(re), inverse variance weighted multiplicative random effects. Wmedian, weighted median. (1) 80 instruments selected from the 138 conditionally independent SNPs from Manousaki et al. (2020) [28], (2) 35 instruments from Sutherland et al. (2022) [30], (3) using 21 instruments from the Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021) [31]
MR effect estimates per 1 standard deviation (SD) increase in genetically predicted increase in the natural log 25(OH)D on cognitive scores (measured in SDs) for individuals of all ages in the CLSA. IVW(re): inverse variance weighted multiplicative random effects. Wmedian: weighted median. (1) 80 instruments selected from the 138 conditionally independent SNPs from Manousaki et al. (2020) [28], (2) using 35 instruments from Sutherland et al. (2022) [30], (3) using 21 instruments from the Emerging Risk Factors Collaboration/EPIC-CVD/Vitamin D Studies Collaboration (2021) [31]
Sensitivity analysis
We computed MR-PRESSO, Egger’s regression, and Cochran’s Q test to assess the robustness of our results. Our sensitivity analyses shown in Table 5 for the PACC score and the other cognitive scores show that by and large, there is low to moderate heterogeneity since I2 values were below 29%. The only moderately elevated heterogeneity value (I2 = 28.3%; I2 Pvalue = 0.014) was for the AFT score when considering individuals in the entire cohort regardless of age. Additionally, the MR-PRESSO global test, which can detect horizontally pleiotropic outlier SNPs, found pleiotropic SNPs for the AFT score in individuals 60 years and older. Assessing the distortion of the causal estimate before and after outlier correction, the MR results changed. We found that MR-Egger intercept test, MR-PRESSO global test and distortion test did not detect horizontal pleiotropy (p-values > 0.05). We therefore did not identify evidence of directional horizontal pleiotropy in the MR-results.
MR sensitivity analysis
Associations of Alzheimer’s disease PRS and cognition traits
We tested the association between seven cognition scores (PACC, AFT, AFT2, COLTIME, MAT, REYI, and REYII) and the AD PRS in the strata of individuals over 60 years of age (Fig. 4A). Most of the cognition scores were associated with the AD PRS. The direction of effect of the association for each significant trait was negative, except for COLTIME (Supplementary Table 5), as expected, given that this cognitive test provides higher scores for worsened performance. Taken together, this suggests that in individuals over 60, the AD PRS was associated with worsened cognition. Such associations were generally attenuated when taking the entire cohort into account.
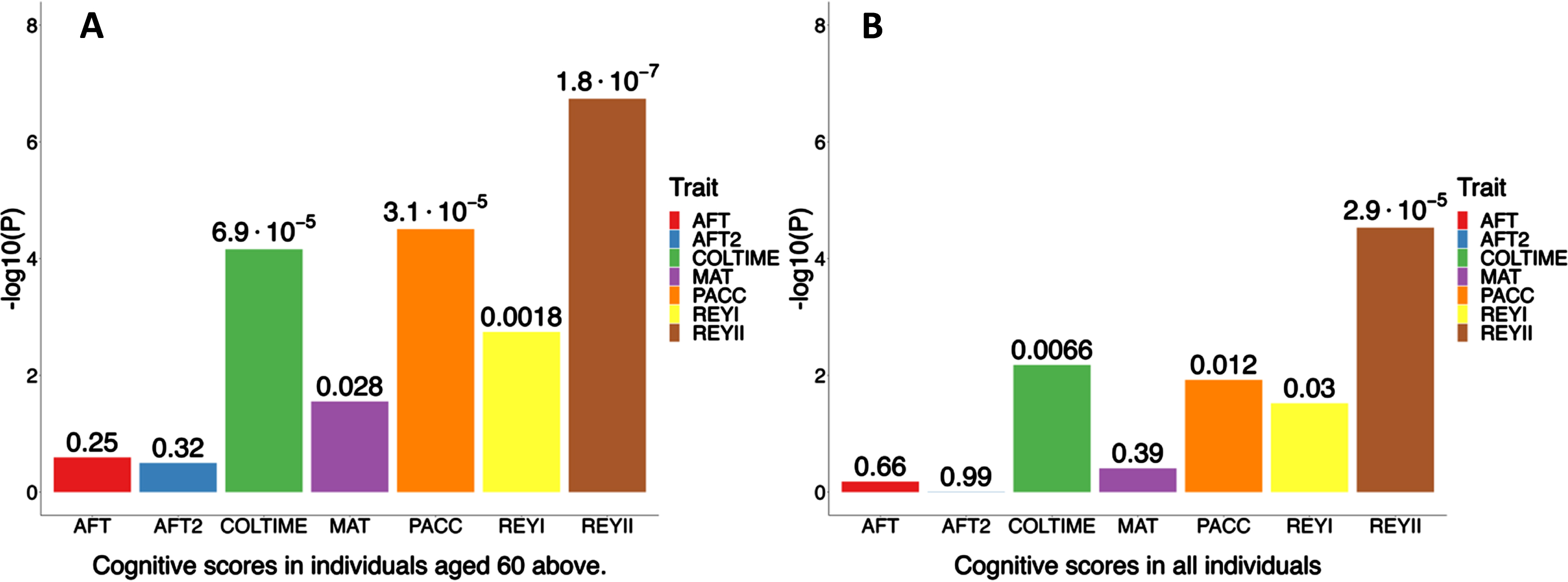
Association of Alzheimer’s disease PRS Cognition scores with cognition scores in CLSA. A) Demonstrates the Alzheimer’s disease PRS association among individuals aged 60 and above (N = 14,234–14,906). B) Illustrates the Alzheimer’s disease PRS association for all individuals (N = 21,840–22,381). The chart displays the associations between polygenic risk scores (PRS) for various cognitive measures including animal fluency score (AFT), animal fluency score 2 (AFT2), Stroop score (COLTIME), mental alteration score, preclinical Alzheimer’s cognitive composite score (PACC), Rey auditory verbal learning score 1 (REYI), and Rey auditory verbal learning score 2 (REYII). The y-axis represents the -log10 p-value indicating the association strength between Alzheimer’s disease PRS and each cognition score. Each bar is annotated with the corresponding p-value representing the association between Alzheimer’s disease PRS and the cognition score. All associations are adjusted for age, sex, and the first 20 principal components.
Genetic correlation of Alzheimer’s disease and the PACC score in older individuals
To quantify the shared genetic etiology of cognition, as measured by the PACC score and AD, we used LD score regression. We found a negative genetic correlation with AD (r g = –0.39 [95% CI –0.53–0.23], p = 0.01 [LDSC]). This suggests that the genetic factors improving cognition, as measured by the PACC score tended to be associated with a reduced risk of AD.
DISCUSSION
In this study, we carried out an observational study followed by a two-sample MR to ascertain both the observational and the genetically estimated effect of 25(OH)D levels on cognitive outcome test scores. We found that higher 25(OH)D levels were associated with improvements in all cognition measures. We then used MR, which reduces bias from reverse causation and confounding, to test for causal effects. The findings of the MR study did not support a causal relationship between a genetically determined increase in the natural log of 25(OH)D levels and either the PACC score or the cognitive scores, although our study is not able to fully exclude a possible benefit on PACC for individuals over 60 years.
While vitamin D supplementation could be beneficial in certain contexts [15] (i.e., hypovitaminosis D), results from observational studies need to be considered carefully. For instance, an observational study published in 2014 [42] with a diverse and small cohort (N = 382; 41.4% individuals from European ancestry, 29.6% individuals from African American ancestry, 25.1% individuals from Latino/Hispanic ancestry) suggested that lower vitamin D levels are associated with a higher rate of cognitive decline. However, this was not supported by an MR study in a cohort of 153,187 individuals of European ancestry. The study focused exclusively on the genetic associations of two canonical variants of 25(OH)D, namely rs12785878 (associated with a decrease in vitamin D-decreasing allele, G), located near the gene encoding 7-dehydrocholesterol reductase (DHCR7), and rs12794714 (linked with reduced vitamin D-decreasing allele, A) situated near 25-hydroxylase (CYP2R1) on global cognition score. (Beta:–0.00; 95% CI: (–0.01, 0.01); p = 1.0), and memory cognitive score (Beta: –0.00; 95% CI: (–0.01, 0.00); p = 0.6). Additionally, a previously published observational study, a MR study, and a clinical trial on the effect of 25(OH)D on cognitive scores are consistent with our study [25, 43].
How 25(OH)D may protect against AD in humans is unknown. MR has shown a protective estimated effect of 25(OH)D on AD in humans [26, 45]. Additionally, previous and novel evidence demonstrated that cognition is protective against AD [45, 46]. Therefore, we hypothesized that 25(OH)D might protect against AD in humans by higher cognition. However, our results suggest no observed estimated causal effects of 25(OH)D on the PACC score (a synthesis of cognition scores). Cognitive abilities tend to decline with age, and age-related cognitive conditions such as dementia and AD are more prevalent in older individuals. Therefore, it is reasonable to assume that the potential benefits of vitamin D on cognition might be more pronounced or relevant in older age groups, as they are at higher risk of cognitive decline. While some analyses on the PACC scores in individuals over 60 years were compatible with a potential benefit, our MR results did not provide consistent evidence for improved cognition by higher 25(OH)D in this age group.
Our study also has several limitations. Since MR depends mainly on three causal inference assumptions (relevance, independence, and exclusion restriction) any violation of these could invalidate our results. To address these assumptions, we performed several sensitivity analyses investigating horizontal pleiotropy and heterogeneity (MR-Egger, MR-PRESSO, Cochran’s Q test). Our causal estimate between 25(OH)D and REYI score in older individuals was considered to have a moderate amount of heterogeneity. After removing outlying SNP through MR-PRESSO, the causal estimate remained the same. This suggests that the MR results are not likely to be strongly biased by directional horizontal pleiotropy. Further, our study focuses on individuals of European ancestry, therefore, conclusions and interpretation of the results may not be generalizable to other ancestries. This again emphasizes the need for large-scale studies assessing the genetic determinants of disease in individuals of non-European ancestry. Last, our study tests only the linear relationship between 25(OH)D levels and outcomes in the population. Whether effects exist at very low levels of 25(OH)D cannot be discerned using the approaches we have employed here.
In conclusion, our MR study found no clear evidence to support the role of 25(OH)D concentrations and cognitive performance in European ancestry individuals.
AUTHOR CONTRIBUTIONS
Yann Ilboudo (Conceptualization; Formal analysis; Methodology; Software; Writing – original draft; Writing – review & editing); Satoshi Yoshiji (Formal analysis; Methodology; Writing – review & editing); Tianyuan Lu (Conceptualization; Formal analysis; Visualization; Writing – review & editing); Guillaume Butler-Laporte (Conceptualization; Formal analysis; Methodology; Visualization; Writing – review & editing); Sirui Zhou (Formal analysis; Methodology; Visualization; Writing – review & editing); J. Brent Richards (Conceptualization; Funding acquisition; Methodology; Resources; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We thank all the participants, the UK Biobank coordinating team, and the CLSA (Project# 1906026 and 190208) coordinating team for their approval, valuable time, generosity, and contributions to the data collection.
FUNDING
The Richards research group is supported by the Canadian Institutes of Health Research (CIHR: 365825; 409511, 100558, 169303), the McGill Interdisciplinary Initiative in Infection and Immunity (MI4), the Lady Davis Institute of the Jewish General Hospital, the Jewish General Hospital Foundation, the Canadian Foundation for Innovation, the NIH Foundation, Cancer Research UK, Genome Québec, the Public Health Agency of Canada, McGill University, Cancer Research UK [grant number C18281/A29019] and the Fonds de Recherche Québec Santé (FRQS). JBR is supported by a FRQS Mérite Clinical Research Scholarship. Support from Calcul Québec and Compute Canada is acknowledged. TwinsUK is funded by the Welcome Trust, Medical Research Council, European Union, the National Institute for Health Research (NIHR)-funded BioResource, Clinical Research Facility and Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust in partnership with King’s College London. These funding agencies had no role in the design, implementation or interpretation of this study.
CONFLICT OF INTEREST
JBR’s institution has received investigator-initiated grant funding from Eli Lilly, GlaxoSmithKline and Biogen for projects unrelated to this research. He is the CEO of 5 Prime Sciences (www.5primesciences.com), which provides research services for biotech, pharma and venture capital companies for projects unrelated to this research. TL is an employee of 5 Prime Sciences.
DATA AVAILABILITY
All GWAS summary statistics used in this study are made publicly available through the GWAS catalog. 25(OH)D and cognitive scores GWAS summary statistics (All ages and individuals 60 and older) can be downloaded through accession numbers in the table below. Further inquiry can be directed to the corresponding author.