
Abstract
Background:
The Boston Naming Test (BNT) is the most widely used measure to assess anomia. However, it has been criticized for failing to differentiate the underlying cognitive process of anomia.
Objective:
We validated the color-picture version of BNT (CP-BNT) in a sample with diverse neurodegenerative dementia diseases (NDDs). We also verified the differential ability of the composite indices of CP-BNT across NDDs groups.
Methods:
The present study included Alzheimer’s disease (n = 132), semantic variant primary progressive aphasia (svPPA, n = 53), non-svPPA (n = 33), posterior cortical atrophy (PCA, n = 35), and normal controls (n = 110). We evaluated psychometric properties of CP-BNT for the spontaneous naming (SN), the percentage of correct responses on semantic cuing and word recognition cuing (% SC, % WR). Receiver operating characteristic analysis was used to examine the discriminatory power of SN alone and the composite indices (SN, % SC, and % WR).
Results:
The CP-BNT had sufficient internal consistency, good convergent, divergent validity, and criterion validity. Different indices of CP-BNT demonstrated distinct cognitive underpinnings. Category fluency was the strongest predictor of SN (β= 0.46, p < 0.001). Auditory comprehension tests highly associated with % WR (Sentence comprehension: β= 0.22, p = 0.001; Word comprehension: β= 0.20, p = 0.001), whereas a lower visuospatial score predicted % SC (β= –0.2, p = 0.001). Composite indices had better predictability than the SN alone when differentiating between NDDs, especially for PCA versus non-svPPA (area under the curve increased from 63.9% to 81.2%).
Conclusion:
The CP-BNT is a highly linguistically relevant test with sufficient reliability and validity. Composite indices could provide more differential information beyond SN and should be used in clinical practice.
INTRODUCTION
Language assessment is a core component of most neuropsychological evaluations, and visual confrontation naming is often used as a measure of language domain [1]. Modern neuroimaging and neurobiological studies have elaborated neural mechanisms underlying visual confrontation naming, by which linguistic transformation occurs, ranging from perceptual recognition of visual stimuli, to activation of semantic representations, lexical retrieval, and articulation of phonological form [2]. Each stage of this complex process relies on the activation of neural networks that cover several cortical areas, as well as their interconnecting fiber pathways [2, 3]. As a result, it is not surprising that the confrontation naming test is sensitive to brain damage and is often utilized as one of many tests to evaluate possible anomia and suspected cognitive impairment in neurological diseases.
The most commonly used confrontation naming test is the Boston naming test (BNT) which was developed in the English language background [4]. Despite its widespread popularity, the BNT has been criticized for its cultural bias when used in a non-English context [5]. It has been widely accepted that if the BNT is to be applied to another cultural and linguistic population, it is necessary to adopt culturally relevant modifications [6]. The adaptation of the Chinese version of BNT reflects the process of cross-cultural acculturation. In the 2000 s, Cheung et al. selected 30 items from the original 60 items based on their cultural relevance in the Chinese context. The phonemic cue was then replaced by a three-word recognition paradigm due to the fact that spelling is not crucial in Chinese ideograms [7]. This modified version of BNT was validated with 61–75% diagnostic effectiveness for predicting mild cognitive impairment (MCI) and 75–78% for mild Alzheimer’s disease (mild AD) in Chinese older adults [8, 9]. However, a high false positive rate (FPR) still limits its clinical applicability [9, 10]. In 2022, our team modified the black-and-white version of BNT (BW-BNT) by replacing the thirty-line drawings with colored, visually realistic images. Validity study suggests that this color-picture version of BNT (CP-BNT) has better reliability and validity than the BW-BNT, particularly in terms of false positive rate, which decreased from 45.5% to 9.9% for the MCI and from 17.8% to 9.9% for the mild AD [5, 9]. These findings suggest that the high FPR with BW-BNT is not due to item difficulty but rather misperceptions produced by poor-quality line drawings [5, 9].
Another major limitation with the BNT is that it fails to reflect the contemporary development of naming conceptualization and fails to identify what the specific stage of naming is impaired [5]. For example, spontaneous naming scores do not distinguish between failure of word retrieval and failure of semantic knowledge. Several studies have suggested that this issue could be solved by qualitative analysis of semantic cues (SC) and phonemic cues (PC) [11, 12]. An individual can benefit from PC but not SC, suggesting that the semantic domain may not necessarily impaired. If a PC does not improve naming performance, implying that the semantic domain may be compromised. This yields the prediction that understanding cuing effects may emerge as a valuable paradigm for detecting word retrieval deficit and semantic breakdown, but this has yet to be systematically validated across clinical groups [5].
For the first time, the CP-BNT was validated in a distinct and diverse NDDs sample: the semantic variant of primary progressive aphasia (svPPA), non-semantic variant of primary progressive aphasia (non-svPPA), AD, and posterior cortical atrophy (PCA). Each group is characterized by selective cortical lesions and focal impairment involved in the naming process, and four groups cover the whole cognitive processes underlying visual confrontation naming tasks [13–17]. The whole sample, therefore, constituted an excellent model for studying psychometric properties and differential power of CP-BNT. The primary aim of this study was to investigate the reliability and validity of CP-BNT in a Chinese sample with NDDs and to explore the cognitive basis underlying different CP-BNT indices including the spontaneous naming (SN) score, the percentage of correct responses on semantic cuing (% SC) and the percentage of correct responses on word recognition cuing (% WR). We supposed that the composite indices of CP-BNT (SN, % Sc and % WR) would provide more hints for the differentiating diagnosis of anomia and eventually improve the discriminatory power of CP-BNT among different subtypes of NDDs.
METHODS
Participants
This study included participants who visited the language and memory impairment clinic, Department of Neurology, Xuanwu Hospital, Capital Medical University, Beijing, from January 2015 to December 2021. All patients were consecutive referrals with the goal of informing differential diagnosis and treatment planning. All participants underwent comprehensive assessments with medical history, neurological and physical examination, a neuropsychological battery, laboratory tests, and MRI/CT scan. The clinical diagnosis was made in a multidisciplinary consensus meeting using international diagnostic consensus criteria. For AD, the clinical core diagnostic criteria of NIA-AA were used [18, 19]. The diagnosis of primary progressive aphasia (PPA) was based on the international consensus [13]. The PPA participants were further classified into semantic variant PPA (svPPA), nonfluent agrammatic variant PPA (nfvPPA), and logopenic variant PPA (lvPPA). PCA was diagnosed on the current research criteria [20]. Participants were excluded if they had any of the following conditions: 1) incomplete neuropsychological battery or MRI/CT scan; 2) other medical illnesses that could interfere with cognitive functioning; 3) any other major systemic, psychiatric or neurological diseases such as cerebral vascular diseases, Parkinson’s disease, encephalitis, traumatic brain injury; and 4) non-degenerative lesions on routine MRI/CT such as focal or diffuse brain damage. Control participants were recruited from the community or the spouses of patients by means of advertisements. They underwent a rigorous clinical evaluation including standardized clinical interview, neurological examination, cognitive tests, imaging and laboratory blood tests. They were assessed as being in cognitive normal and good health.
The final sample consisted of 110 cognitive normal controls (NC), 132 patients with AD, 53 patients with svPPA, 19 patients with nfvPPA, 16 patients with lvPPA, and 33 patients with PCA. We combined the lvPPA and nfvPPA as the non-semantic PPA group (n = 35) because they had naming difficulty due to word retrieval deficit or phonological paraphasias but had relatively reserved semantic function [13, 14]. This study was approved by the ethics committee of Xuanwu Hospital, and all participants or their caregivers provided written consent.
Cognitive and language assessment
All participants were administered a neuropsychological battery, including the Chinese version of the Montreal Cognitive Assessment (MoCA) [21]; the modified World Health Organization-University of California Los Angeles Auditory Verbal Learning Test Immediate Recall (AVLT-I) and Delayed Recall (AVLT-D) [22]; the forward and backward digit span; the trail making tests part A and part B (TMT-A and TMT-B); the Rey Complex Figure copy test (RCF copy). The assessment of language included the color-picture version of BNT, category fluency for animal for 60 s, a single-word comprehension task, a sentence comprehension test and a sentence repetition task based on a detailed speech and language battery [23]. The clinical dementia rating scale (CDR) was used to evaluate the global cognitive ability [24].
Administration of the color-picture version of Boston naming test
The CP-BNT consists of thirty color pictures presented on a computer screen one at a time (see Fig. 1). The rules of administration and scoring were reported elsewhere [9]. We reported three direct descriptive scores and two indirect descriptive scores, which are commonly used in the BNT research [8, 10]. The score of spontaneous naming (SN) was the number of items correctly named spontaneously, ranging from 0 to 30. The score of semantic cuing (SC) was the number of correct responses after giving the semantic cue, as well as the scores of word recognition (WR), ranging from 0 to 30. Two additional descriptive scores, the percentage of correct responses on semantic cuing and word recognition (% SC and % WR), were calculated for each participant by dividing the number of correct responses during semantic cuing or word recognition curing by the number of errors preceding the cuing. This ratio was then multiplied by 100, ranging from 0% to 100%. The % SC and % WR represent the extent of benefit from cuing which are more direct to demonstrate the cuing effectiveness than the SC and WR.
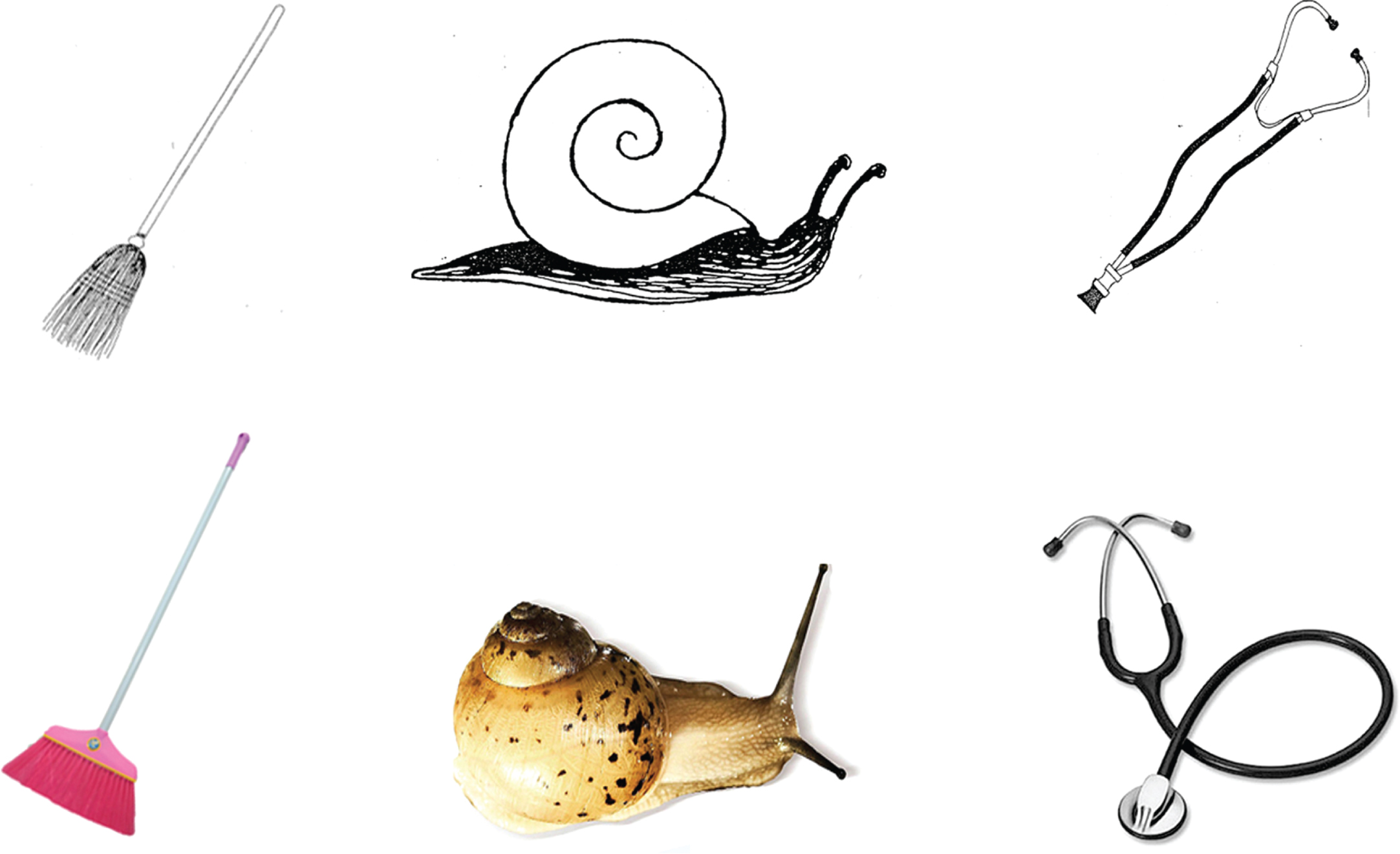
Original line drawings of BW-BNT and the color pictures of CP-BNT for item broom, snail, and stethoscope.
Statistical analyses
Demographic data, cognitive and language measures were analyzed using the Kruskal-Wallis test for continuous variables and χ2 test for categorical variables, followed by pair-wise comparisons with Bonferroni correction. Convergent and divergent validity were assessed between each CP-BNT index (SN, % SC, and % WR) and neuropsychological and language measures, using Spearman’s correlation coefficient, given the non-normal distribution of CP-BNT indices. To control for false-positive errors, the criterion for statistical significance was set at p < 0.01 (two-tailed) for the Spearman analysis. We conducted multiple stepwise regression analysis to assess the explanatory variables (demographic, cognitive, and language variables) that could predict the CP-BNT index (SN, % SC, and % WR). We adjusted the SN score using linear regression model with SN as the dependent variable and age and education as the independent variable. Each patient group (AD, PCA, non-svPPA, and svPPA) was separately combined with the control group in model fitting. After model fitting, the prediction value for each participant was used as the adjusted SN (SNadj). We conducted the receiver operating characteristic (ROC) analyses to examine the predictability of the SNadj to discriminate each patient group from NC and to discriminate between NDDs. Further, ROC analyses were conducted by composite indices (SNadj, % SC, and % WR) to discriminate between NDDs. We calculated Cronbach’s α to examine the internal consistency of the raw SN. Tests were 2-tailed and a p-value of 0.05 was used for statistical significance, except for the non-parametric Spearman analysis. All statistical analyses were performed using IBM SPSS windows version 22 (SPSS Inc., Chicago, IL, USA).
RESULTS
Descriptive results
Table 1 shows the demographic information and scores of all neuropsychological measures. Of the 110 NCs, 49.1% were male, with the mean age of 66.2 (ranging 55–75, SD = 6.0) years and mean education of 12.2 years (SD = 3). Compared to the NC, PCA, non-svPPA, and svPPA groups were significantly younger (p < 0.01), and AD, svPPA, and non-svPPA groups had significantly lower educational levels (p < 0.01, p < 0.05 for non-svPPA). All patient groups significantly differed from the NC in all neuropsychological measures, except that the svPPA group had normal performance in the RCF copy. Pair-wise comparisons between patient groups were presented in Supplementary Table 1. Each patient group was characteristic of their respective clinical variant profile on the neuropsychological tests.
Demographic data, performances of cognitive measures and CP-BNT indices for all participants
*Patient group versus NC p < 0.05; **Patient group versus NC p < 0.01. CP-BNT, Color-picture version of Boston naming test; NC, normal control; AD, Alzheimer’s disease; svPPA, semantic variant of primary progressive aphasia; non-svPPA, non-semantic variant of PPA; PCA, posterior cortical atrophy; MoCA, Montreal cognitive assessment; CDR, Clinical dementia rating; AVLT-I, the modified World Health Organization-University of California Los Angeles Auditory Verbal Learning Test Immediate Recall; AVLT-D, the modified World Health Organization-University of California Los Angeles Auditory Verbal Learning Test Delayed Recall; TMT, Trail making tests; SN, spontaneous naming; SC, semantic cue; WR, word recognition; % SC, the percentage of correct responses on semantic cuing; % WR, the percentage of correct responses on word recognition.
Performance of the CP-BNT in NC and NDDs groups
For the SN, there were significant differences between each patient group and NC (p < 0.01), and this remained for SNadj (p < 0.01). Among the four patient groups, the svPPA scored the lowest on the SN (mean = 6.4, SD = 4.3), followed by the non-svPPA (mean = 17.7, SD = 5.1), the PCA (mean = 20.0, SD = 5.2), and the AD group (mean = 23.5, SD = 3.6). There were significant differences between the svPPA and other patient groups (p < 0.01), as well as the AD and non-svPPA groups (p < 0.001). (Table 1 and Supplementary Table 1)
In terms of % SC, svPPA patients also scored the lowest (mean = 0.9%, SD = 3.0%), followed by the non-svPPA (mean = 5.2%, SD = 8.0%), and the AD (mean = 12.3%, SD = 17.1%). The PCA group had the highest % SC (mean = 20.0%, SD = 5.2%), which was even significantly higher than that of the NC (p < 0.001).
Regarding the % WR, there were significant differences between each patient group and NC (p < 0.01). The svPPA got the lowest (mean = 44.7%, SD = 24.6%), then the PCA < non-svPPA<AD<NC. Significant differences were also found between AD and svPPA (p < 0.001), non-svPPA and svPPA (p < 0.001).
Reliability of SN score
The internal consistency of the CP-BNT was good according to standard criteria (α= 0.767).
Convergent and divergent validity
Table 2 displays the correlations between CP-BNT indices and scores of other measures. The SN had the strongest relationship to the language relative tests, including category fluency (Spearman’s ρ= 0.76, p < 0.01) and sentence comprehension (ρ= 0.72, p < 0.01). The SN was moderately associated with the global cognitive status tests and episodic memory test, including MoCA (ρ= 0.64, p < 0.01), CDR global score (ρ= – 0.61, p < 0.01), and AVLT-I (ρ= 0.60, p < 0.01). The lowest correlation was found between the SN and RCF copy (ρ= 0.36, p < 0.01).
Correlations between CP-BNT indices and other neuropsychological measures (Spearman rho coefficient)
*Statistical significance was set at p < 0.01 (two-tailed). 1. MoCA: Montreal Cognitive Assessment; 2. CDR: Clinical dementia rating; 3. AVLT-I: the modified World Health Organization-University of California Los Angeles Auditory Verbal Learning Test Immediate Recall; 4. AVLT-D: the modified World Health Organization-University of California Los Angeles Auditory Verbal Learning Test Delayed Recall; 5. Digit span forward; 6. Digit span backward; 7. TMT part A: Trail making test part A; 8. TMT part B: Trail making test part B; 9. Rey complex figure copy; 10. Category fluency; 11. Sentence repetition; 12. Word comprehension; 13. Sentence comprehension; 14. SN, Spontaneous naming; 15. % SC: the percentage of correct responses on semantic cuing; 16. % WR: the percentage of correct responses on word recognition.
The % SC was weakly associated with the word comprehension (ρ= 0.25, p < 0.01), the RCF copy (ρ= –0.20, p < 0.01) and CDR global (ρ= –0.15, p < 0.01). The % WR had medium associations with language-relevant tests, including category fluency (ρ= 0.52, p < 0.01), sentence comprehension (ρ= 0.50, p < 0.01), and word comprehension (ρ= 0.48, p < 0.01), and a weak association with the RCF copy (ρ= 0.25, p < 0.01).
Predictors of CP-BNT indices
Multiple stepwise regressions showed five variables significantly predicting the SN score, and the category fluency was the strongest predictor (β= 0.46, p < 0.001, Supplementary Table 2). Three variables significantly predicted the % SC, with the lower score of RCF copy strongly associated with the higher % SC (β= –0.2, p = 0.001). For the % WR, the regression model included four variables and two comprehension tests highly predicted the score of % WR (Sentence comprehension: β= 0.22, p = 0.001; Word comprehension: β= 0.20, p = 0.001).
Criterion validity: Differentiating NDDs from NC
Using SNadj, the AUC was 90.7% (95% CI: 86.6–94.8%) for AD, 94.8% (95% CI: 91.2–98.4%) for PCA, 94.8% (95% CI: 91.2–98.5%) for non-svPPA, and 99.6% (95% CI: 99.1–100.0%) for svPPA (Fig. 2).
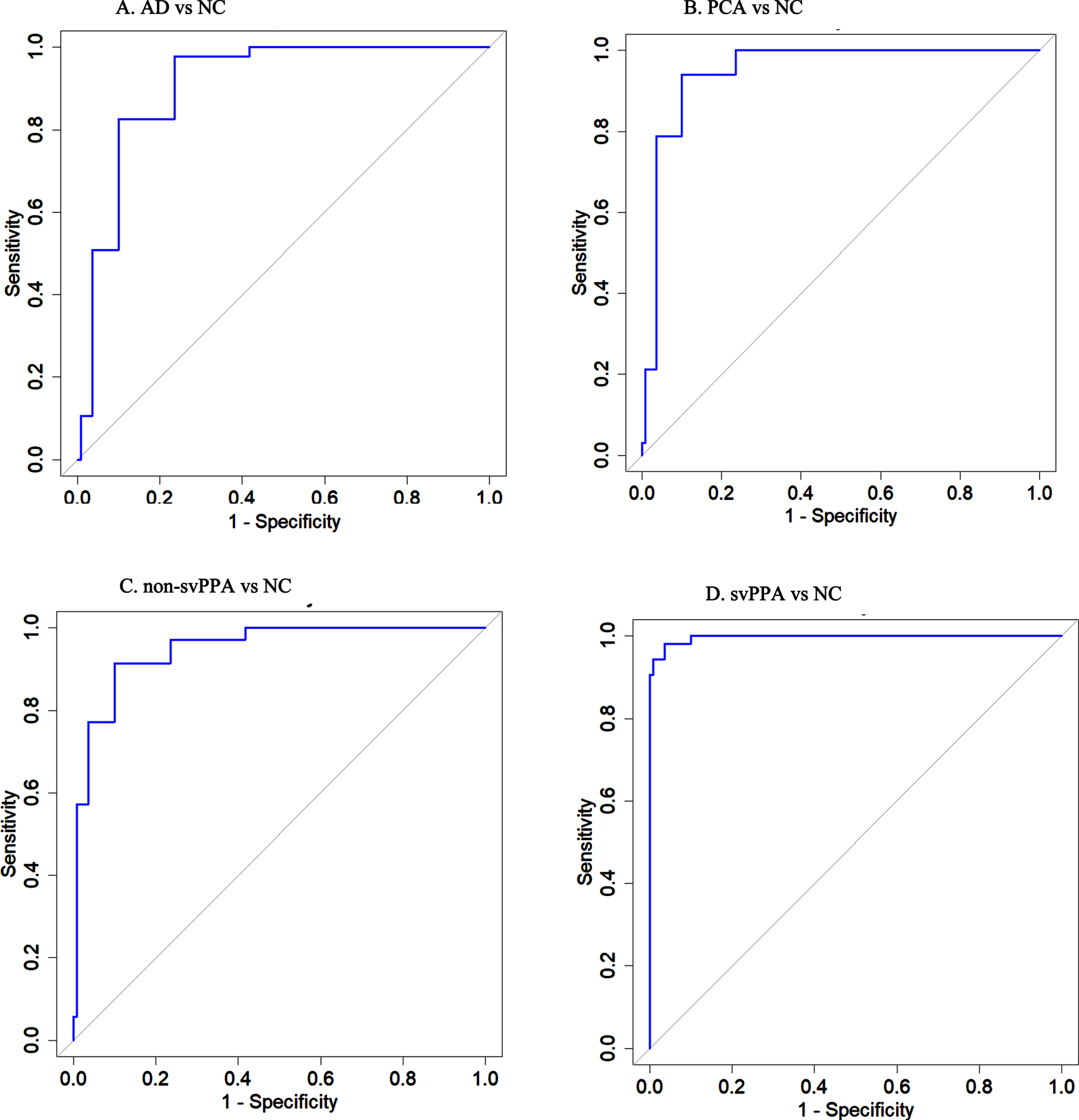
ROC curves for four pathological groups versus normal controls with adjusted SN score. A) ROC curve for Alzheimer disease versus NC (AUC = 90.7%, 95% CI: 86.6–94.8%). B) ROC curve for Posterior cortical atrophy versus NC (AUC = 94.8%, 95% CI: 91.2–98.4%). C) ROC curve for non- semantic variant primary progressive aphasia versus NC (AUC = 94.8%, 95% CI: 91.2–98.4%). D) ROC curve for semantic variant primary progressive aphasia versus NC (AUC = 99.6%, 95% CI: 99.1–100.0%).
Table 3 presents the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), diagnostic effectiveness, and Likelihood ratio for a positive test result (LR+) for four patient groups versus the NC. At the cutoff value of 25, the SNadj exhibited varying diagnostic accuracy for patient groups, with the svPPA group having the highest sensitivity (100%) and diagnostic effectiveness (93.3%), whereas the AD group had adequate sensitivity (82.6%) and diagnostic effectiveness (86%).
The diagnostic ability of adjusted-SN between patient group and NC
Adjusted-SN, Spontaneous naming adjusted with age and education; NC, normal control; AD, Alzheimer’s disease; PCA, Posterior cortical atrophy; svPPA, Semantic variant primary progressive aphasia; non-svPPA, non-semantic variant primary progressive aphasia; PPV, Positive predictive value; NPV, Negative predictive value; LR+, Likelihood ratio for a positive test result.
Criterion validity: Differentiating among NDDs
Table 4 shows that composite indices (SNadj, % SC and % WR) had greater AUC than the SNadj alone. The greatest improvement of predictability was observed for PCA versus non-svPPA (AUC from 63.9% to 82.1%), followed by that of PCA versus AD (from70.1% to 77.6%), and AD versus non-svPPA (from75.9% to 79.3%). There was mild improvement for svPPA versus non-svPPA (from 95.9% to 97.9%), svPPA versus PCA (from 97.1% to 99.0%), and svPPA versus AD (from 98.3% to 99.2%).
The differentiating ability of SNadj and composite indices to differentiate among NDDs
SNadj, score of spontaneous naming adjusted by age and education; NDD, neurodegenerative dementia disorder; AD, Alzheimer’s disease; svPPA, semantic variant of primary progressive aphasia; non-svPPA, non-semantic variant of primary progressive aphasia; PCA, posterior cortical atrophy; AUC, Area under the ROC curve; 95% CI, 95% Confidence interval; Δ AUC, AUC for composite indices minus AUC for SNadj, which indicates the improvement of AUC.
DISCUSSION
To the best of our knowledge, this is the first validation of multiple indices of BNT in a widely sampled cohort with diverse NDDs. The results support that the CP-BNT is a reliable and valid measure highly correlated with language function and global cognitive level and has good capability to differentiate NDDs from normal control. The results show that each CP-BNT index has unique cognitive underpinnings and that the use of composite indices could further improve the predictability of CP-BNT in differential diagnoses of NDDs.
Correlation and regression analysis of the SN revealed a wide range of associations with multi-cognitive domains, including category fluency, global cognitive status, episodic memory, executive function, and visuospatial skills, in particular, category fluency was the strongest predictor of the SN. Our results are consistent with previous studies that BNT is a test highly related to the semantic-lexical function and can be used to measure the presence and severity of anomia [25, 26]. For NDDs with anomia but no aphasia, the development of anomia could be considered as one of the clinical hallmarks of progressive global cognitive deterioration [27, 28]. In the case of AD, regardless of the BW-BNT or CP-BNT, MCI patients performed slightly worse than the NC, while mild AD patients scored significantly lower than the NC group [9, 12]. According to the controlled semantic cognition framework, global cognitive function, which integrates working memory, processing speed, visuospatial skill and so on, affects the efficacy of search and retrieval in the semantic cognition [29–31].
The multivariable analysis revealed that the lower visuospatial ability was the most significant predictor for the % SC. If naming difficulty stems from perceptual deficits, the semantic activation elicited by impaired visual perception is insufficiently specified. Semantic cuing could help achieve the threshold for semantic activation by providing additional semantic information [2, 32]. This might explain why the PCA group obtained the highest % SC among all NDDs groups and even higher than the NC group. To date, few studies have reported the relationship between the % SC and perceptual defects. Tallberg IM. reported that visual association misinterpretations that occur in normal subject naming are more likely to be disclosed by semantic cuing [33]. Similar phenomena have been observed in comparative studies of the BW-BNT and CP-BNT [7, 9]. Using the BW-BNT, % SC was recorded as high as 33.83% to 22.1% in the NC group, whereas it dropped to 13.3% with the CP-BNT. The decrease in % SC could be attributed to the change in picture type, as colored pictures reduce the possibility of misperception caused by black-and-white line drawings. The abnormally high % SC may suggest visual perceptual errors in the first levels, before semantic activation takes place.
Additionally, according to previous studies, individuals are more likely to obtain a lower value in % SC than in % PC or % WC, reflecting the fact that individuals, whether or not they have severe semantic impairment, would not gain significantly naming improvement from the semantic cuing [11, 12]. From the neurobiological and neuropsychological viewpoints, semantic cuing, based on the same semantic-lexical process as the spontaneous naming, would not raise more additional semantic activation for semantic normal or semantic impairment individuals. This could explain why % SC showed weak correlations with other cognitive variables.
The index % WR, on the contrary, has a wide range of relationships with other measures. The strongest predictors of this index were comprehension tests. These results suggest that word recognition cuing mainly relies on lexical-semantic processes including auditory perception and semantic networks. In the semantic core and control network, the anterior temporal lobe (ATL) is the core area for semantic representation. In addition, the fusiform gyrus has been suggested to be crucial for word comprehension, serving as a hub for integrating auditory and conceptual processing [30, 34–36]. Simultaneously, the semantic control system also participates in this process through top-down modulation of the semantic hub [31, 36]. In this study, the svPPA demonstrated an early and predominant deficit in % WR due to its ATL lesions. PCA patients demonstrated a significant decrease in % WR, possibly explained by atrophy in the fusiform gyrus [37]. The AD and non-svPPA groups showed mild declines in % WR, suggesting relatively reserved semantic cognitive functions. Contrary to the SN, % WR reflects the presentation and severity of lexical-semantic dysfunction in NDDs.
This study revealed that each index of CP-BNT had distinct underlying cognitive bases and that different subtype of NDDs presented unique features of anomia corresponding to their lesion location. The SN demonstrated high discriminatory power to predict NDDs from the NC, but the discriminant value was discounted when differentiating between subtypes of NDDs. From an empirical point of view, the combination of indices (SNadj, % SC, and % WR) could provide more cognitive and location information beyond the SN alone. This hypothesis is supported by the results of ROC analysis. The composite indices had better predictability for a certain subtype of NDDs in comparison with the SNadj, particularly for PCA versus non-svPPA (from 63.9% to 81.2%, ΔAUC = 18.3%). Thus, we suggest that the composite indices of CP-BNT should be considered in clinical applications, as it empirically provides more differential hints and quantitatively improves predictability.
This study has several advantages as the CP-BNT is a major cultural adaptation of BNT for the Chinese language context in the last two decades. First, this study enrolled a diverse sample of NDDs with AD, PCA, svPPA, and non-svPPA, which provides special models for investigating the relationship between anomia and selective neural degeneration in NDDs. Based on this model, this study shed light on the association between % SC and visuospatial impairment, allowing for a better understanding of the cognitive basis underlying semantic cuing and the % SC. Second, the word recognition cues provide new access to measure lexical-semantic function, which reinforces the BNT as a language test in the neuropsychological battery to assess both word production and comprehension. Finally, given that clinicians have long been overly reliant on SN scores, this study emphasizes the importance of composite indices which substantially improved the CP-BNT’s capability to distinguish between NDDs.
There are several limitations in this study. First, the normal control group in this study is not a truly representative of the general population. Because younger and/or high-educated individuals are more willing to participate as volunteers, these demographic differences between NC and patients may affect the diagnostic accuracy of CP-BNT, even though we adjusted the SN with age and education in the analysis. Second, there is obviously lower sample size for patients with visuospatial deficits, because AD and PPA patients with severe visuospatial impairments were excluded for their incomplete neuropsychological battery. This may result in limited effect size of visuospatial ability and underestimated predictability of % SC.
In summary, our findings support that CP-BNT is a reliable and valid language test and has better acculturation in the Chinese language context. In addition to the spontaneous naming, this study deepens our understanding of the role of % SC and % WR, their underlying cognitive mechanisms and clinical relevance. Furthermore, this study evidences that composite indices, which provide more cognitive information beyond the SN, quantitively improve the differential ability of CP-BNT for NDDs subtypes. Therefore, we suggest that composite indices of the CP-BNT may emerge as a useful paradigm for assessing naming performance in the future and can be utilized in conjunction with other markers of NDDs to aid in clinical decision-making.
Footnotes
ACKNOWLEDGMENTS
We thank all participants and their families for their time and contribution to this study.
FUNDING
This research was supported by the Beijing Natural Science Foundation (No. L182049) and the National Key R&D Programme of China (2017YFE0118800).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.