
Abstract
Background:
Research on posterior cortical atrophy (PCA) has focused on cognitive decline, especially visual processing deficits. However, few studies have examined the impact of PCA on activities of daily living (ADL) and the neurofunctional and neuroanatomic bases of ADL.
Objective:
To identify brain regions associated with ADL in PCA patients.
Methods:
A total of 29 PCA patients, 35 typical Alzheimer’s disease (tAD) patients, and 26 healthy volunteers were recruited. Each subject completed an ADL questionnaire that included basic and instrumental subscales (BADL and IADL, respectively), and underwent hybrid magnetic resonance imaging and 18F fluorodeoxyglucose positron emission tomography. Voxel-wise regression multivariable analysis was conducted to identify specific brain regions associated with ADL.
Results:
General cognitive status was similar between PCA and tAD patients; however, the former had lower total ADL scores and BADL and IADL scores. All three scores were associated with hypometabolism in bilateral parietal lobes (especially bilateral superior parietal gyri) at the whole-brain level, PCA-related hypometabolism level, and PCA-specific hypometabolism level. A cluster that included the right superior parietal gyrus showed an ADL×group interaction effect that was correlated with the total ADL score in the PCA group (r = –0.6908, p = 9.3599e–5) but not in the tAD group (r = 0.1006, p = 0.5904). There was no significant association between gray matter density and ADL scores.
Conclusion:
Hypometabolism in bilateral superior parietal lobes contributes to a decline in ADL in patients with PCA and can potentially be targeted by noninvasive neuromodulatory interventions.
INTRODUCTION
Posterior cortical atrophy (PCA) is an early-onset neurodegenerative syndrome characterized by visual processing deficits and cognitive dysfunctions [1, 2]. Research on PCA has largely focused on cognitive decline and there is little known about the effect on activities of daily living (ADL) that can occur in the early stages, and which is more severe than in typical Alzheimer’s disease (tAD) [3, 4]. Most patients with PCA experience disease onset between the ages of 45 and 65 years and ADL impairments impose a heavy burden on these individuals, their families, and the healthcare system [5 –7].
Few studies have explored the factors affecting ADL in patients with PCA. One study showed that multiple factors contributed to the deterioration of ADL in PCA patients, including cognitive dysfunctions such as memory and attention/orientation deficits and behavioral symptoms such as low mood, disinhibition, and apathy [3]. However, no study has reported on the neural correlates thereof. ADL impairments in patients with tAD were found to be significantly associated with frontal, temporal, and parietal hypometabolism [8 –10]. Unlike with tAD, patients with PCA exhibit distinct patterns of atrophy in the parietal and occipital lobes [11]. Thus, brain areas involved in ADL in patients with PCA may also differ from those in tAD patients. Balint syndrome and Gerstmann syndrome, which are the most common clinical symptoms of PCA, manifest as space perception deficits, simultanagnosia, agnosia, or acalculia, etc., and involve the parietal lobe; they are known to adversely affect object or environment recognition and consequently have a negative impact on ADL [12 –14]. The parietal lobe also participates in other functional neural circuits involved in cognition and behavior such as attention, memory, and apathy, which may contribute to the decline in ADL in PCA patients [3 , 15–17]. However, it is unclear if ADL impairments in PCA involve the parietal lobe.
In this study, we used magnetic resonance imaging (MRI) combined with 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) scanning and ADL assessment to identify brain regions associated with ADL in patients with PCA. We hypothesized that the parietal lobe is associated with ADL impairments in this population.
MATERIALS AND METHODS
Ethics
This study was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University on Human Clinical Research and was conducted according to the principles outlined in the Declaration of Helsinki. All participants or their families provided written informed consent.
Participants
Between August 2017 and October 2021, 29 PCA patients, 35 tAD patients, and 26 healthy controls were recruited at the Neurology Department of Xuanwu Hospital, Beijing, China. Each PCA patient met the 2017 diagnostic criteria for PCA [2], and patients with tAD met the 2010 International Working Group diagnostic criteria [18]. The diagnosis was established by a senior neurologist based on a detailed clinical evaluation, neuropsychological assessment, and brain MRI. Patients had no prior history of conditions that could affect cognition such as cerebrovascular disease or brain trauma or significant psychiatric illness unrelated to dementia. Patients were excluded if they had ophthalmic diseases or early symptoms suggesting underlying corticobasal dementia, dementia with Lewy bodies pathology, or prion disease [19 –21]. Volunteers were recruited as healthy controls if they had no subjective complaints related to cognition and had a score within the normal range on global cognition scales (Mini-Mental State Examination [MMSE] >26, Montreal Cognitive Assessment [MoCA] >24, and Clinical Dementia Rating [CDR] = 0).
Neuropsychological assessment
A standard battery of tests was used for neuropsychological assessment including the MMSE and MoCA for general cognitive function [22, 23] and CDR for disease severity [24]. The Rey–Osterrieth Complex Figure (ROCF) test and Line Bisection (LB) test were used to assess visuospatial function [25, 26]; the World Health Organization University of California-Los Angeles Auditory Verbal Learning Test (AVLT) was used to assess memory [27]; the Digit Span Test (DST) forward and backward were used for attention and executive function [28]; the Boston Naming Test (BNT) was used for naming [29]; and the Neuropsychiatric Inventory-Questionnaire (NIQ), Hamilton Anxiety Scale (HAMA), and Hamilton Depression Scale (HADA) was used for psycho-behavioral symptoms [30 –32].
ADL were assessed with the revised version of the ADL scale, which has been extensively employed in China [33]. This scale includes 20 items, of which 8 are used for basic ADL (BADL) assessment (i.e., eating, dressing, washing, sitting down or standing up, moving in a room, defecation, bowel control, and showering) and 12 are used to evaluate instrumental ADL (IADL) (i.e., traveling in a bus, moving around near the station, cooking a meal, medicine management, doing easy housework, doing complicated housework, washing clothes, cutting toenails, shopping, using a telephone, financial management, and staying home alone). The score for each item ranges from 1 to 4 as follows: 1 = completely independent, 2 = have some difficulty, 3 = need some assistance, and 4 = completely dependent. The total ADL (TADL) score was obtained by summing the scores of the 20 items and BADL and IADL scores were obtained by summing the scores of related sub-items.
18F-FDG-PET/MRI data acquisition
18F-FDG-PET and T1 scans were simultaneously acquired on a hybrid 3.0 T time-of-flight PET/MRI scanner (Signa PET/MR; GE Healthcare, Madison, WI, USA) after injection of 3.0 MBq/kg 18F-FDG via a venous cannula [34]. Static 18F-FDG-PET data were acquired with the following parameters: matrix size = 192×192, field of view (FOV) = 350×350 mm2, and pixel size = 1.82×1.82×2.78 mm3, and included corrections for random coincidences, dead time, scatter, and photon attenuation. T1 data were acquired with the following parameters: repetition time (TR) = 6.9 ms, echo time (TE) = 2.98 ms, inversion time = 450 ms, flip angle = 12°, matrix size = 256×256, FOV = 256×256 mm2, slice thickness = 1 mm, 192 sagittal slices with no gap, voxel size = 1×1×1 mm3, and acquisition time = 4 min 48 s. The default attenuation correction sequence was carried out based on brain MRI, automatically prescribed, and acquired with the following parameters: liver acceleration volume acquisition-Flex axial acquisition, TR = 4 ms, TE = 1.7 ms, slice thickness = 5.2 mm with a 2.6-mm overlap, 120 slices, pixel size = 1.95×2.93 mm, and acquisition time = 18 s.
18F-FDG-PET data preprocessing
Image preprocessing was performed using SPM12 software in MATLAB (MathWorks, Natick, MA, USA). Each image was first normalized to an FDG-PET–specific template registered to the Montreal Neurological Institute standard space. Spatially normalized images of all subjects were then smoothed with an isotropic Gaussian kernel with 8-mm full width at half-maximum before performing the statistical analysis. PET scan intensity was normalized using the whole cerebellum as a reference region to create standardized uptake value ratio images.
MRI data preprocessing
Computational anatomy toolbox 12 (CAT12) was used to preprocess T1 data based on SPM12. We used MRICRON software to convert the DICOM files into nifti format and used the default settings of the CAT12 toolbox and East Asian Brains International Consortium for Brain Mapping template to preprocess images for voxel-based morphometry. We segmented T1-weighted 3-dimensional images into gray matter (GM), white matter (WM), and cerebrospinal fluid partitions; and performed high-dimensional registration and normalization of each subject’s GM and WM partitions in native space to the standard Montreal Neurological Institute space by exponentiated lie algebra normalization using diffeomorphic anatomic registration. An 8-mm full width at a half-maximum Gaussian kernel was used to smooth the images.
Statistical analysis
Statistical analyses were carried out with SPSS v26.0 (IBM, Armonk, NY, USA) and MATLAB software. Continuous data are presented as mean±standard deviation whereas categorical data are presented as absolute values. Inter-group differences in demographic and neuropsychological data were evaluated with the Kruskal–Wallis H test. Statistical significance was set at p < 0.05.
Inter-group differences in brain metabolism/GM volume were assessed by analysis of covariance. Voxel-wise multivariable regression analysis was conducted to determine the correlation between changes in brain metabolism/GM volume and TADL, BADL, and IADL scores. To determine which brain regions were specifically involved in ADL impairments in PCA patients, we conducted a regression analysis that included the following three levels: 1) whole-brain level, using whole brain regions as an independent variable; 2) PCA-related level using a mask that included brain regions with hypometabolism/changes in GM volume in PCA patients compared with normal controls as an independent variable; and 3) PCA-specific level using a mask that included brain regions with hypometabolism/GM atrophy in PCA patients compared with tAD patients as an independent variable. With level 1 and 2 regressions, we identified brain regions that were the major contributors to ADL impairments in PCA patients; we then used level 3 regression analysis to confirm that these relationships were specific to PCA.
We also performed voxel-wise regression analyses with the ADL×group interaction effect as the dependent variable in the whole patient population to determine whether brain regions associated with ADL performance differed between PCA and tAD patients. The additional regression was performed to further determine whether the brain regions associated with ADL impairments in the PCA group were unique to PCA. The threshold for the neuroimaging analysis was set at voxel-wise family-wise error (FWE)-corrected p < 0.05, with age, sex, and education as covariates.
RESULTS
Demographic characteristics of patients and results of neuropsychological assessment
Patients’ demographic data and performance in the neuropsychological tests are shown in Table 1. There were no differences in age, sex, or education level across the PCA, tAD, and healthy control groups. The PCA group performed worse than the tAD group in the TADL test (PCA versus tAD, 42.79±10.82 versus 35.77±11.12, p < 0.001) as well as the BADL subscale (PCA versus tAD, 11.86±3.55 versus 9.79±2.73, p < 0.001) and IADL subscale (PCA versus tAD, 30.93±8.13 versus 25.97±9.00, p < 0.001). There were no differences between PCA and tAD patients in general cognition level including the MMSE and MoCA tests. Compared with the tAD group, PCA patients performed worse in visuospatial function and attention including in the ROCF test (PCA versus tAD, 1.00±2.75 versus 8.32±6.70, p < 0.001), LB test (PCA versus tAD, 0.35±0.50 versus 0.86±0.36, P < 0.001), and DST forward (PCA versus tAD, 5.52±1.81 versus 6.85±1.60, p < 0.001). There were no differences between the two groups in other cognitive and psychological tests.
Demographic and neuropsychological features of the study population
ADL, Activities of Daily Living; AVLT, Auditory Verbal Learning Test; BADL, Basic Activities of Daily Living; BNT, Boston Naming Test; CDR, Clinical Dementia Rating; DST, Digit Span Test; F, female; HAMA, Hamilton Anxiety Scale; HAMD, Hamilton Depression Rating Scale; HC, health control; IADL, Instrumental Activities of Daily Living; LB, Line Bisection; M, male; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; NPI-Q, Neuropsychiatric Inventory-Questionnaire; PCA, posterior cortical atrophy; ROCF-c, Rey-Osterrieth Complex Figure copy; tAD, typical Alzheimer disease.
Metabolic changes and GM atrophy patterns detected by 18F-FDG-PET/MRI
Metabolism patterns for the three groups are shown in Fig. 1 and Supplementary Table 1, whereas GM atrophy patterns are shown in Supplementary Figure 1 and Supplementary Table 2. Differences in GM atrophy patterns across groups were similar to the metabolic changes. Compared with healthy controls, patients with PCA had brain hypometabolism/GM atrophy mostly limited to bilateral parietal, occipital, and temporal lobes (voxel-wise FWE-corrected p < 0.05, cluster size >40). The tAD group showed more extensive hypometabolism/GM atrophy including in bilateral hippocampi and temporal, frontal, and parietal lobes (voxel-wise FWE-corrected p < 0.05, cluster size >40). Compared with the tAD group, hypometabolism/GM atrophy regions of the PCA group were more concentrated in the bilateral parietal and occipital lobes.
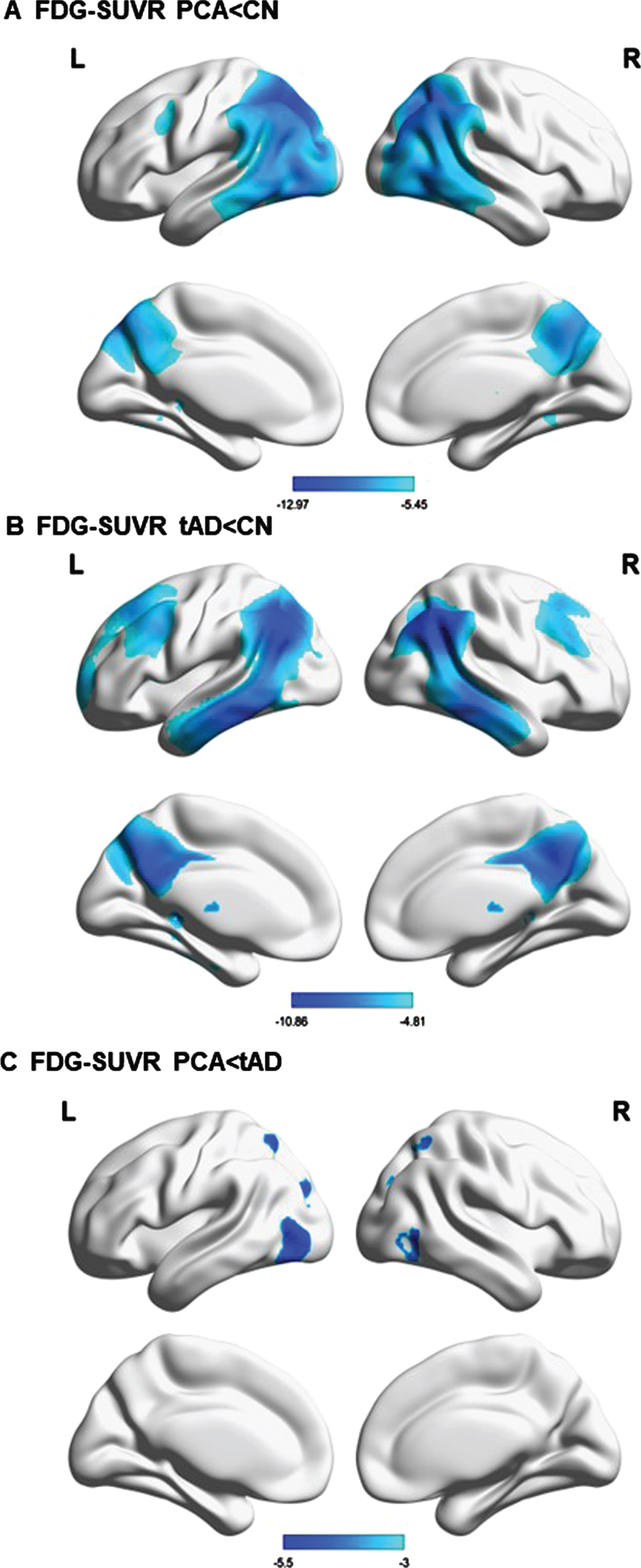
GM hypometabolism profiles across groups. A–C) Hypometabolism pattern of PCA group versus healthy controls (A), tAD group versus healthy controls (B), and PCA group versus tAD group (C) (p < 0.05, FWE-corrected, minimum cluster size 40 voxels). T values are color-coded from cyan to blue.
Neurofunctional basis of ADL in PCA
Results of the regression analysis of ADL at the whole-brain level are shown in Fig. 2 and Table 2, and level 2 and level 3 analyses were shown in Supplementary Figure 2 and Supplementary Table 3. Bilateral superior parietal lobe hypometabolism was associated with TADL, BADL, and IADL scores at all analysis levels. At all three levels, TADL was mainly associated with bilateral parietal lobes including the right superior parietal gyrus, right inferior parietal gyrus, right angular gyrus, and left superior parietal gyrus (threshold was set at voxel-wise FWE-corrected p < 0.05). Although BADL and IADL scores were highly correlated (r = 0.686, p < 0.001), they differed in terms of their association with brain glucose metabolism. Specifically, BADL was mainly associated with the bilateral parietal lobe located in the right superior parietal gyrus, right inferior parietal gyrus, and left superior parietal gyrus (with the threshold set at voxel-wise FWE-corrected p < 0.05), whereas IADL was mainly associated with bilateral superior parietal gyrus (with the threshold set at voxel-wise FWE-corrected p < 0.05).
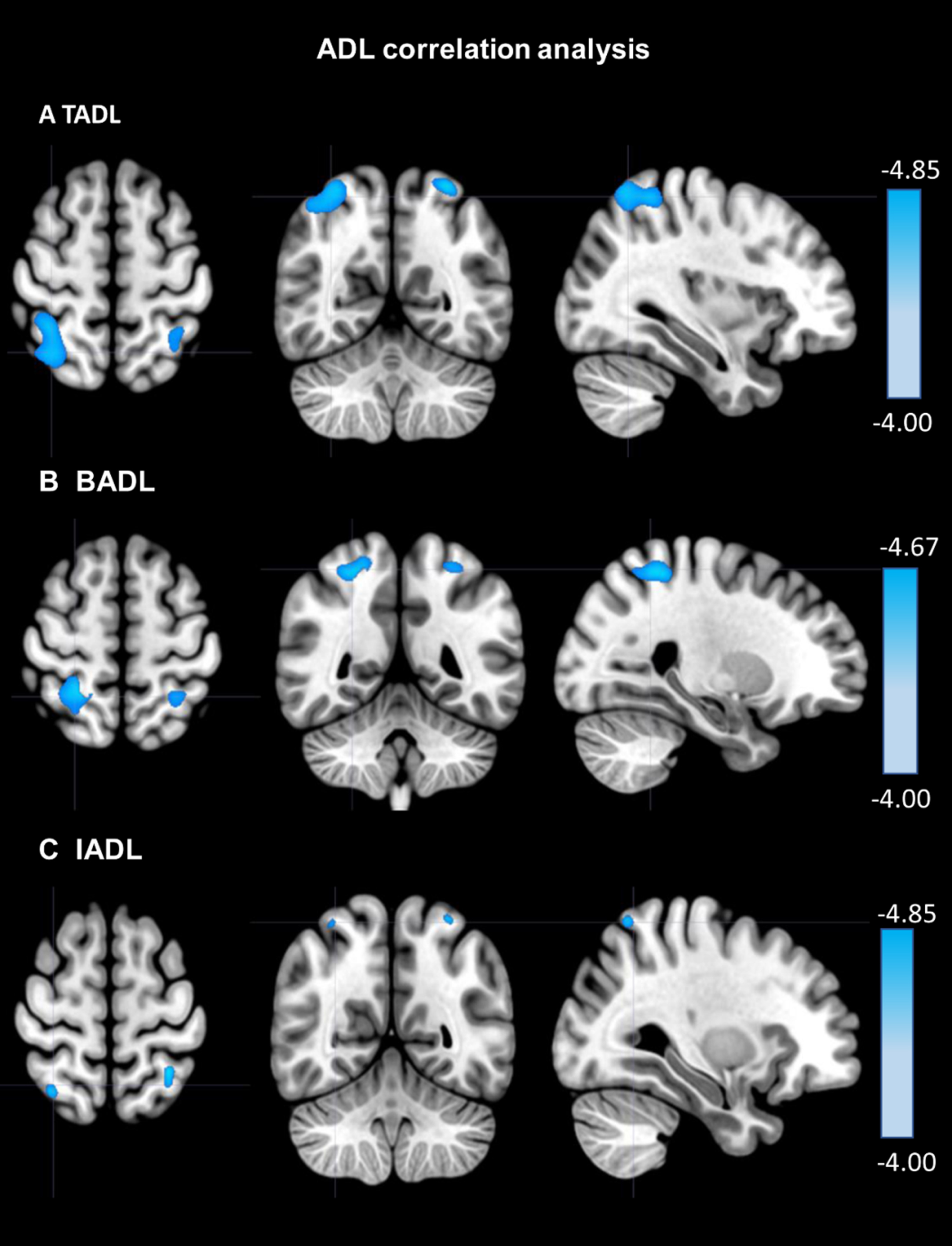
Hypometabolism in brain regions correlated with ADL in the PCA group at the whole-brain level. A–C) Brain areas correlated with TADL (A), BADL (B), and IADL (C) at the whole-brain level are shown (p < 0.05, FWE-corrected, minimum cluster size 40 voxels). T values are color-coded from cyan to blue.
Brain regions showing hypometabolism correlated with ADL at the whole-brain level in patients with PCA
BADL, Basic Activities of Daily Living; IADL, Instrumental Activities of Daily Living; MNI, Montreal Neurological Institute; PCA, posterior cortical atrophy; TADL, Total Activities of Daily Living.
One cluster that included the right superior parietal gyrus representing the ADL×group interaction effect was identified (at a threshold of uncorrected p < 0.005) (Table 3). After extracting values for metabolism in the cluster, we found that the ADL score was strongly correlated with the metabolic changes in the PCA group (r = –0.6908, p = 9.3599e–5) whereas no correlation was observed in the tAD group (r = 0.1006, p = 0.5904).
Brain regions showing a correlation with ADL score×group interaction effect1
MNI, Montreal Neurological Institute. 1Age, sex, and education level served as control variables and the interaction was evaluated with a generalized linear model (uncorrected p < 0.005, cluster size >40).
Neuroanatomic basis of ADL in PCA
Voxel-wise regression analyses revealed no significant association between GM density and TADL, BADL, and IADL scores.
DISCUSSION
This was the first study to explore the neurofunctional basis of ADL impairments in PCA. Our results revealed that hypometabolism in bilateral superior parietal lobes may contribute to the decline of ADL in patients with PCA.
In our study, bilateral (especially superior) parietal lobes were found to be abnormal specifically in the PCA group compared with tAD patients. This corresponded with worse TADL, BADL, and IADL scores and greater deficits in visuospatial functions (visuo-constructive ability and visuospatial neglect evaluated with the ROCF copy test and LB test, respectively) and attention in patients with PCA, as demonstrated by multiple regression analysis at three levels. One cluster mainly located in the right superior parietal gyrus showing an ADL×group interaction effect was significantly correlated with the TADL score in the PCA group. The superior parietal lobe is known to be associated with visuo-constructive ability, visuospatial neglect, and attention deficits and is an interface of multiple neural pathways such as the dorsal visual pathway and frontoparietal attention network [15 , 36–39]. Damage to this area may therefore cause visual-cognitive symptoms that can negatively affect a PCA patient’s ability to carry out ADL.
Previous FDG-PET studies have reported that metabolic changes in the posterior hemisphere were associated with cognitive deficits in patients with PCA. Oculomotor apraxia was found associated with hypometabolism in the left parietal lobe, left posterior cingulate gyrus, and left medial parietal cortex [40]. Performance in the Shape Detection, Silhouettes, and Dot Counting tests were correlated with FDG uptake in the right parieto-occipital cortex [41]. Aphasia, apraxia, and global cognition were associated with brain areas located in the left hemisphere’s ventral and dorsal visual streams, and environmental agnosia and apperceptive prosopagnosia were associated with the ventral and dorsal visual streams of the right hemisphere [42]. These core symptoms in PCA are related to metabolic changes in the parietal lobe. It was previously shown that cognitive deficits may contribute to the decline of ADL in PCA [3]. Our results provide evidence that hypometabolism in the parietal lobe is related to ADL deterioration in PCA patients.
There were no significant results in the voxel-wise regression analyses that examined the association between GM density and ADL scores. FDG-PET is sensitive to synaptic and neuronal dysfunction, but several studies have found that FDG-PET combined with MRI can reveal more neural correlates of AD or other types of dementia and improve the diagnostic accuracy of these diseases compared with MRI or FDG-PET alone [43, 44].
The brain hypometabolism/GM atrophy pattern and clinical features of PCA patients in our study were consistent with the results of previous studies, indicating that our data are reliable. The hypometabolism and GM atrophy in the PCA group were mainly observed in the parietal lobe, occipital lobe, and temporoparietal junction, whereas in the tAD group, they were present in bilateral hippocampi, temporal lobe, frontal lobe, and precuneus. A direct comparison between the PCA and tAD groups revealed a PCA-specific hypometabolism/GM atrophy pattern in the parietal and occipital lobes, consistent with earlier studies [11, 45]. TADL, BADL, and IADL scores were lower in the PCA group than in the tAD group, supporting the finding that ADL impairments are more severe in PCA than in tAD [3]. Visual processing deficits are the main clinical symptoms of PCA [7] and we found that visuo-constructive ability (evaluated with the ROCF copy test) and visuospatial neglect (evaluated with the LB test) were more profoundly altered in PCA patients than in the tAD patients.
Our study had some strengths. First, the sample size of patients with PCA was adequate and the tAD group served as a control group to assess neurodegeneration specific to PCA. Second, FDG-PET is a sensitive imaging modality that can reflect synaptic dysfunction in the brain [35]. Third, our results are reliable because we analyzed ADL as BADL and IADL at three levels (whole-brain, PCA-related, and PCA-specific). We also performed a regression analysis of the ADL×group interaction effect in the whole patient population to further confirm that the brain regions associated with ADL impairments in the PCA group were unique to PCA. Finally, we conducted detailed neuropsychological testing to establish the distinct clinical features of PCA.
There were also several limitations to this study. First, not all PCA diagnoses were validated by pathology. Second, the cross-sectional study design did not allow us to conclude the causal relationship between parietal lobe damage and ADL; a longitudinal study is needed to better understand the role of bilateral superior parietal lobes in ADL impairments in patients with PCA. Third, the sex distribution of PCA patients differed from that of healthy controls, although the difference was not statistically significant. The high proportion of females in the PCA group may reflect their greater susceptibility to PCA [42]. This sex disparity warrants exploration in future studies with a larger sample size.
Conclusion
Hypometabolism of the bilateral superior parietal lobe may play an important role in the decline of ADL in PCA patients. This suggests a potential target for future noninvasive neuromodulatory interventions such as transcranial alternating current or magnetic stimulation that can improve patient’s quality of life with PCA.
Footnotes
ACKNOWLEDGMENTS
The authors thank all the study participants.
FUNDING
This work was supported by grants from the Beijing Municipal Science and Technology Committee (no. 7202060) and National Natural Science Foundation of China (nos. 82271464 and 81971011).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The datasets used and analyzed in this study are available from the corresponding author on reasonable request.