
Abstract
Background:
Olfactory dysfunction appears prior to cognitive decline, and thus it has been suggested to be an early predictor of Alzheimer’s disease. However, it is currently not known whether and how olfactory threshold test could serve as a quick screening tool for cognitive impairment.
Objective:
To define olfactory threshold test for screening cognitive impairment in two independent cohorts.
Methods:
The participants are comprised of two cohorts in China, 1,139 inpatients with type 2 diabetes mellitus (T2DM, Discovery cohort) and 1,236 community-dwelling elderly (Validation cohort). Olfactory and cognitive functions were evaluated by Connecticut Chemosensory Clinical Research Center test and Mini-Mental State Examination (MMSE), respectively. Regression analyses and receiver operating characteristic (ROC) analyses were carried out to determine the relation and discriminative performance of the olfactory threshold score (OTS) regarding identification of cognition impairment.
Results:
Regression analysis showed that olfactory deficit (reducing OTS) was correlated with cognitive impairment (reducing MMSE score) in two cohorts. ROC analysis revealed that the OTS could distinguish cognitive impairment from cognitively normal individuals, with mean area under the curve values of 0.71 (0.67, 0.74) and 0.63 (0.60, 0.66), respectively, but it failed to discriminate dementia from mild cognitive impairment. The cut-off point of 3 showed the highest validity for the screening, with the diagnostic accuracy of 73.3% and 69.5%.
Conclusion:
Reducing OTS is associated with cognitive impairment in T2DM patients and the community-dwelling elderly. Therefore, olfactory threshold test may be used as a readily accessible screening tool for cognitive impairment.
INTRODUCTION
Alzheimer’s disease (AD) is one of the most common progressive age-related neurodegenerative diseases affecting approximately 50 million people worldwide [1, 2]. There is no effective therapies for AD, therefore, it is in urgent need to develop methods for early-stage diagnosis [2, 3]. Mild cognitive impairment (MCI) is considered as a prodromal stage of AD, which services as a window period to stem the progression to AD when therapeutic intervention was received [4]. Early diagnostic of MCI is extremely important to slow the progression of the disease and delay the onset of AD, and screening in a large population is the unique tool for early diagnosis [5]. However, current methods used for AD diagnosis are not suitable for screening, for instance, cerebrospinal fluid (CSF) biomarkers reflecting tau and amyloid-β (Aβ) require invasive methods, while brain imaging, such as PET and MRI, is too expensive [6].
Olfactory dysfunction is considered as an early predictor of neurodegeneration and is associated with late-life cognitive impairment [7 –10], and olfactory testing may be a useful tool for screening cognitive decline progression due to its independent of intelligence quotient and education [9, 11]. Multiple longitudinal clinical studies have demonstrated that the degree of olfactory impairment predicts the incidence of MCI and the progression from MCI to AD in the elderly, which will hopefully be a quick, convenient, affordable, and widespread screening method for MCI/AD [8, 10]. There are three types of olfactory detection methods commonly used [9 , 12]: 1) Discrimination: distinguishing a different odor among several identical odors; 2) Identification: connect a scent to matching text or pictures; and 3) Odor detection threshold: the concentration of molecules that an individual can recognize. The odor identification and discrimination test were mostly used to explore the relationship between olfaction and cognition. Odor identification has been suggested to be associated with cognitive decline, MCI, and/or AD dementia [13, 14].
In our previous studies, we used combination markers, including age, APOE ɛ4 genotype, olfactory threshold score (OTS) and peripheral glycogen synthase kinase-3β (GSK-3β), plasma Aβ 42/40 for diagnosis of cognitive impairment in type 2 diabetes mellitus (T2DM) patients [6, 15]. We found that the reduced OTS by itself diagnose cognitive decline with a moderate efficiency. On a practical note, olfactory threshold test is quick and easy to operate, making it ideal for clinical screening in the elderly.
In the present study, we try to explore whether the cutoff value of OTS could be used as a screening tool for cognitive impairments in our previously established two high risk populations: 1,139 T2DM patients as Discovery cohorts and 1236 community-dwelling elderly as Validation cohorts.
METHODS
Participants
Discovery cohort: 1,139 T2DM inpatients (64.8±8.0 years old) were recruited from January 2012 to November 2019 from five medical centers in Wuhan, China, partly had been reported in our previous study [6, 15]. The T2DM patients were diagnosed by following the World Health Organization (WHO) National Diabetic Group Criteria of 2006 [16]. The inclusion and exclusion criteria were as presented previously [6, 15]. Briefly, the inclusion criteria included: 1) age ≥45 years; 2) long-term residence (≥5 years); and 3) having ability to complete the neuropsychological test and write informed consent. The exclusion criteria were as follows: 1) having dementia before T2DM; 2) having history of either head trauma, stroke, brain tumor, coma, transient ischemic attack, epilepsy, or other central nervous system diseases that could cause dementia; 3) having auditory/visual disorders, thyroid disease, history of using possible or known drugs affecting cognitive function abuse, alcohol addiction, diagnosed depression, schizophrenia and other psychiatric disorders such as acute stress disorder, post-traumatic stress disorder, acute transient psychosis; and 4) olfactory loss and rhinitis, severe cold.
Validation cohort: A total of 1,545 elderly community-dwelling residents (71.4±5.7 years old) in Wuhan were told for free physical examinations. The exclusion criteria were the same as above. Another 135 who did not complete cognitive test, 159 who did not complete olfactory test, and 15 who did not complete ethic were excluded.
The study protocol was approved by the Medical Ethics Committee (NCT01830998, Clinical Trials.gov), Tongji Medical College, Huazhong University of Science and Technology. All participants had provided written informed consent.
Cognitive test
All participants underwent conventional medical history and physical examinations. The Mini-Mental State Examination (MMSE) test was conducted by two experienced inspectors with neurology training. Cognitive impairment was diagnosed based on Petersen’s criteria [17]: 1) memory complaint, 2) normal activities of daily living, 3) normal general cognitive function, 4) the abnormal memory ability for the age, and 5) MMSE scores at 24–26 was diagnosed as MCI, and MMSE scores at 10–23 was diagnosed as dementia.
Olfactory threshold test
All participants were tested with the Connecticut Chemosensory Clinical Research Center (CCCRC) olfactory assessment. Olfactory detection threshold test used the diluted times of butanol into 12-grade concentrations (2.3×10–5 % –4%), started from a low concentration to highest concentration of 4%. The deionized water was used as the control. The value of threshold was set at which level butanol could be correctly identified at the same dilution for four consecutive times. If one of the four times could not be correctly identified, the concentration was increased until four times could be recognized continuously. The olfactory detection threshold scores (OTS) are shown in Fig. 1. A higher score indicated a better olfactory function.
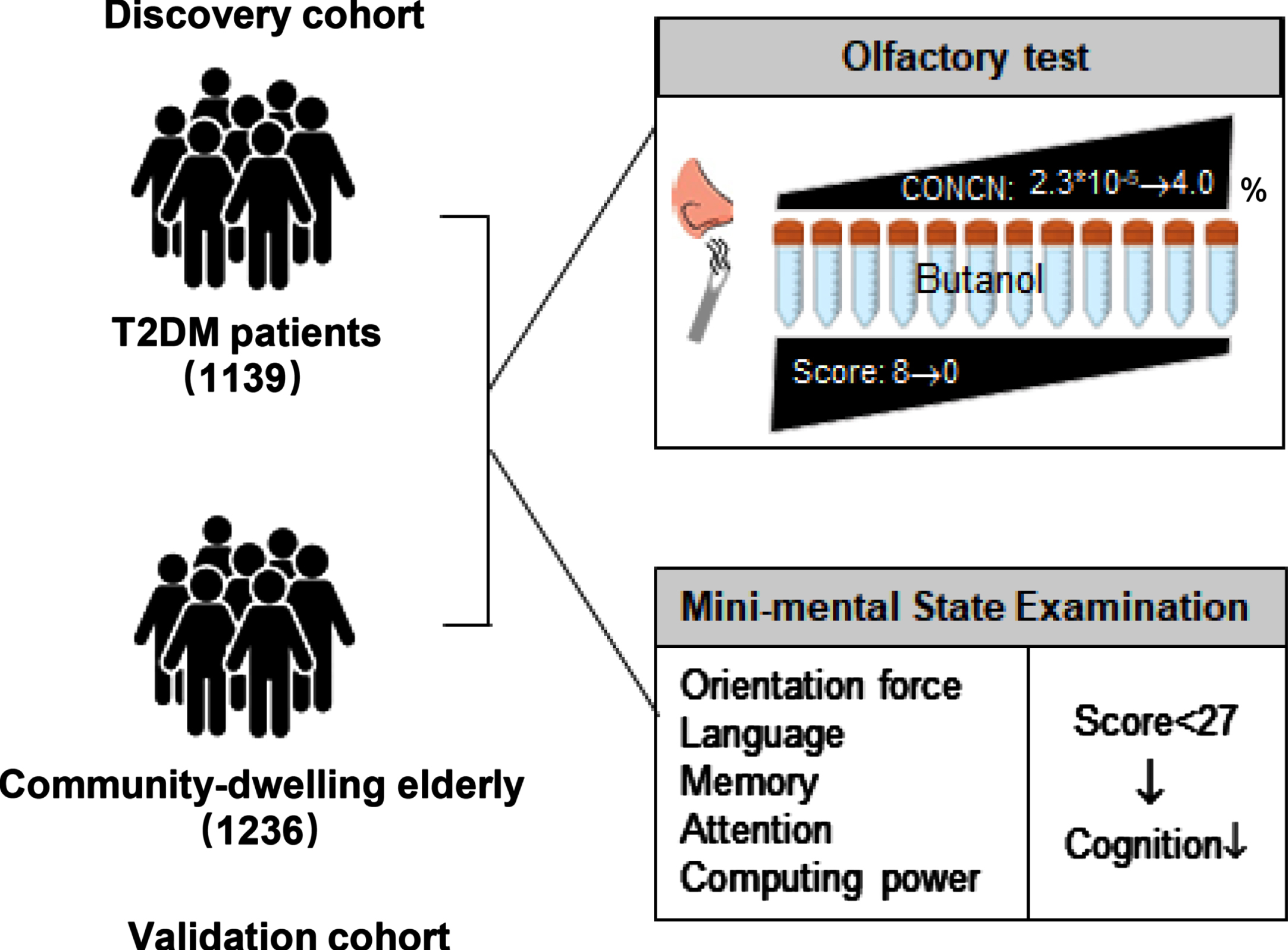
Study profile.
Covariates of the study population
Demographic and health information, including age, sex, family history of diabetes, diabetes duration, insulin treatment, and diabetic complications, were collected using a semi-structured questionnaire. History of diseases, including hypertension, hyperlipidemia, and coronary heart disease. Hemoglobin A1c (HbA1c) and fasting blood glucose were acquired by medical records in hospitals.
Statistical analysis
Continuous variables were presented as mean±SD or median (interquartile range: 25–75%), categorical variables were presented as number (proportion). Patients were divided into three groups, Q1 (range 0-2), Q2 (range 3–5), and Q3 (range 6–8) according to OTS. Multiple comparison test was performed to compare each variable among the three groups. Comparisons among groups were tested statistically by the χ2 test for non-continuous variables and by one-way ANOVA (analysis of variance) for continuous variables, followed by Tukey–Kramer multiple test for normally distributed continuous variables and by the Kruskal–Wallis H test for the non-normally distributed variables.
Spearman’s rank correlation was analyzed between MMSE score and OTS. Multiple linear regression analysis was performed to determine variables that significantly correlated with the OTS and MMSE score. Logistic regression analysis and receiver operating characteristic curves (ROC) were used to calculate the sensitivity, specificity, and area under the curve (AUC) and determine the cut-off points for dividing. The cut-off point with the highest values (sensitivity + specificity) was considered the best. The following formula was used, when calculating diagnostic accuracy: diagnostic accuracy = (the number of true positives + the number of true negatives)/total number of subjects.
Data were analyzed using SPSS 26.0 IBM software and Prism 8.0 (GraphPad). p value <0.05 was considered as statistically significant.
RESULTS
Participant characteristics
Table 1 showed the demographics for the participants in the Discovery and Validation cohorts. The Discovery cohort was composed of 1,139 T2DM patients, in which 465 (40.8%) were male, and mean (SD) age was 64.8 (8.0) years. The participants in Validation cohorts were 1,236 community-dwelling older adults who accepted free check-ups, with mean age of 71.4 (5.7) and 519 (42%) males. Variables were grouped according to OTS tertile cut-offs. In Discovery cohort, Q1 participants who had the worst odor function, generally showed lower MMSE score with older age and higher HbA1c, fasting blood glucose, higher prevalence of APOE ɛ4 carriers, or MCI/dementia. Lower education level and higher prevalence of drinking were also presented in Q1 of Validation cohorts.
Participants characteristics
Median (IQR), Mean (SD); OTS, olfactory threshold score; MMSE, Mini-Mental State Examination; CN, cognitive normal; CI, cognitive impairment; MCI, mild cognitive impairment; DD, duration of diabetes; CHD, coronary heart disease. p-value: χ2 test for categorical variables, Tukey–Kramer multiple test or Kruskal-Wallis test for continuous variables.
Association between odor threshold scores and cognitive performance
Many factors affect cognitive and olfactory function, some of which were commonly recognized, such as age, APOE ɛ4, and education level (Supplementary Table 1). MMSE scores were higher across OTS (all the participants were divided into 9 groups) and presented a positive correlation in an almost linear manner (Spearman r = 0.35, p < 0.001 in Discovery cohort, Fig. 2A; r = 0.24, p < 0.001 in Validation cohort; Fig. 2B). When the population was divided into cognitive normal (CN) and cognitive impairment (MCI + dementia, CI) groups, we observed that the CI group had lower OTS than CN group (t-test, p < 0.0001, Fig. 2C, D).

Association of olfactory function and cognitive performance. A, B) MMSE score was positively correlated with the OTS (Spearman r = 0.35, p < 0.001, n = 1,139 in Discovery cohort (above); r = 0.24, p < 0.001, n = 1,236 in Validation cohort (below)). C, D) The CI group had lower OTSs than CN group (unpaired t-test, p < 0.0001), in the two cohorts. CN, cognitive normal; CI, cognitive impairment.
By univariable and multivariable logistic regression analysis, we confirmed the association of lower OTS with cognitive impairment in both Discovery cohort (OR = 0.66 (0.60, 0.72), p < 0.001) and the Validation cohort (OR = 0.69 (0.64, 0.76), p < 0.001), and this association was still significant after adjusted by the potential confounders, such as age, sex, APOE ɛ4 state, education level and others (Table 2).
Logistic regression analyses of the association between odor threshold score and the risk of cognitive impairment
OTS, olfactory threshold score; CHD, coronary heart disease; DD, duration of diabetes.
Discrimination performance of the odor threshold score
ROC analysis was shown by the value of the AUC, a measure of how well OTS was able to discriminate CN individuals from MCI, or dementia, or cognitive impaired (MCI + dementia, CI). OTS could distinguish respectively MCI (AUC = 0.70 (0.66∼0.74), p < 0.0001, Fig. 3A), dementia (AUC = 0.72 (0.66∼0.77), p < 0.0001, Fig. 3C), and CI (AUC = 0.71 (0.67∼0.74), p < 0.0001, Fig. 3E) from CN in both Discovery cohort and Validation cohort (MCI versus CN, AUC = 0.63 (0.59, 0.65), p < 0.0001, Fig. 3B; dementia vs. CN, AUC = 0.64 (0.61, 0.68), p < 0.0001, Fig. 3D; CI vs. CN, AUC = 0.63 (0.60, 0.66), p < 0.0001, Fig. 3F). However, OTS failed in discriminating MCI from dementia (p > 0.05, Fig. 3G, H).
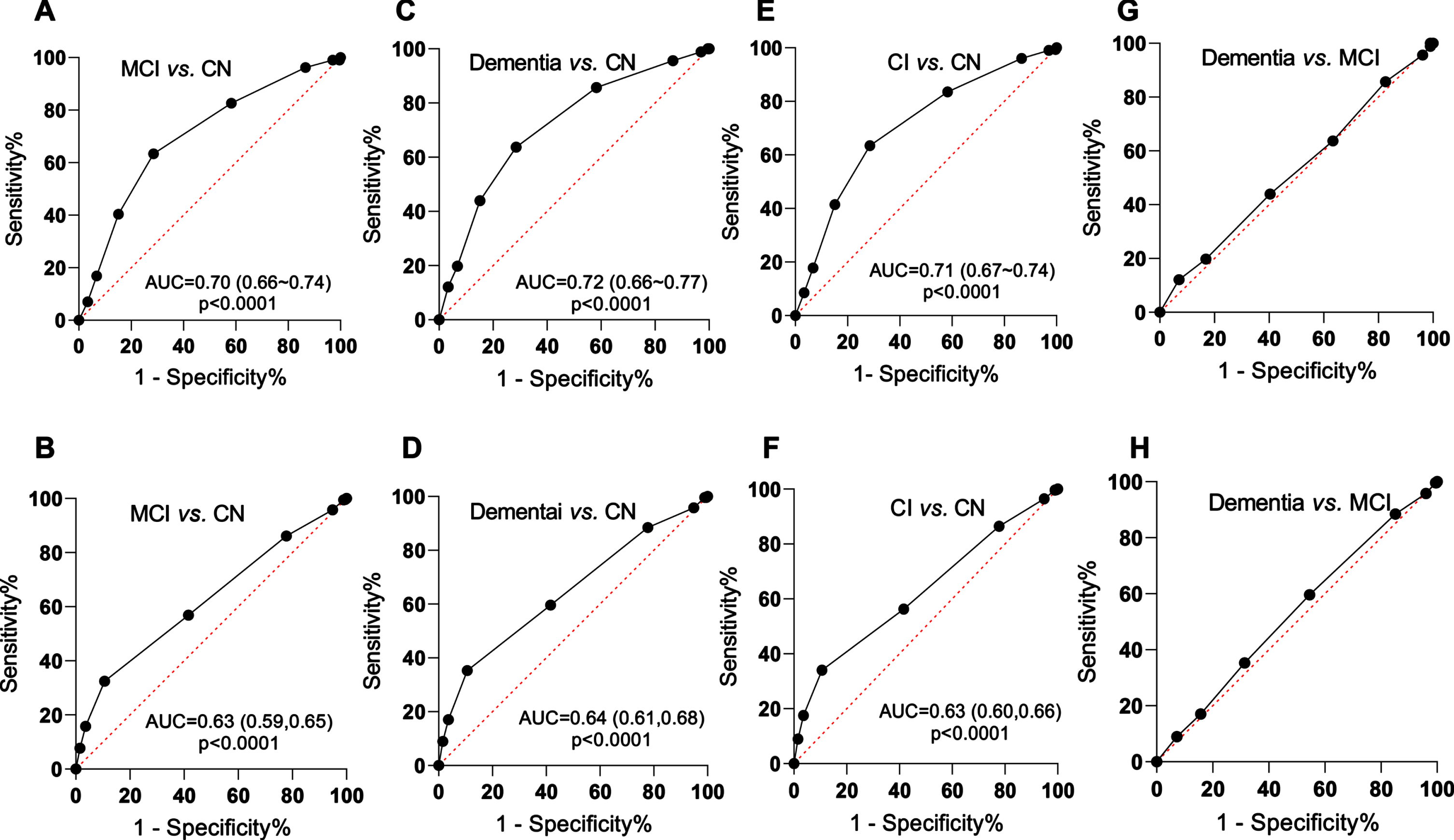
Discrimination performance of odor threshold score. Odor threshold score could distinguish MCI (A, B), dementia (C, D), CI (E, F) from CN in both Discovery cohort (above) and Validation cohort (below). G, H) Odor threshold score could not distinguish dementia from MCI (p > 0.05). MCI, mild cognitive impairment; CI, cognitive impairment; CN, cognitive normal.
Youden’s indices, which can be used to determine an optimal cut-off value of OTS for the best discrimination using their highest value, i.e., the maximum of the sum of sensitivity and specificity. The cut-off value 3 or 4 was comparable in Discovery cohort, and 3 was the best in Validation cohort (Table 3). When cut-off was set at 3, the diagnostic accuracy in two cohorts was 73.3% and 69.5%, respectively (Table 4). These data suggest that an optimal cut-off value 3 (OTS = 0/1/2 was diagnosed as CI) may be used for screening.
Sensitivity and specificity of the olfactory threshold scores for discrimination analyzed by ROC
ROC, operating characteristic curves.
Diagnostic accuracy of cognitive impairment for screening in two cohorts
Diagnostic accuracy = (the number of true positives + the number of true negatives)/total number of subjects.
DISCUSSION
Olfactory dysfunction is a common and early symptom of many neurodegenerative diseases, particularly of AD [18]. Studies show that olfactory impairment tested by odor detection threshold, odor discrimination, and odor identification has clinical application as an early diagnostic biomarker for MCI and AD [9 , 20]. Identification and discrimination were achieved through an interaction with cognitive functions that recall and relate to semantic memory, verbal memory, and executive function [9 , 21]. However, odor detection threshold test was more associated with basic sensory perception processes, more convenient and likely to screen in large number population [11, 21]. In our current study, we analyzed the association between olfactory function detected by odor detection threshold with cognitive performance. We found that measuring OTS could effectively distinguish cognitive impaired (MCI and dementia) from the normal cognition populations, and cut-off value 3 showed the highest validity for the screening.
The shared and connected projections of brain-olfactory structures are the basis for the correlation between olfaction and cognition [22, 23]. Olfactory receptors are located in the olfactory epithelium in the nasal cavity consisted of supporting cells, olfactory cells, and base cells. The axons of olfactory cells form olfactory nerves projecting to the olfactory bulb. Then, mitral cells in olfactory bulb project to piriform cortex, which form triples with the amygdala (CoA) and the lateral entorhinal cortex (EC), respectively [24]. EC and CoA are also bidirectionally connected with olfactory bulb and hippocampus. These brain regions are particularly susceptible to aging and neurodegeneration, with aging being the major risk factor for cognitive, and as well as odor function [25, 26]. Odor detection threshold, odor discrimination, and odor identification domains decreased with aging, while odor detection threshold in particular was much greater compared to the other two [11]. In both of our cohorts, age was associated with the decreased olfaction and cognitive. In addition, APOE ɛ4, the highest genetic risk factor for sporadic AD and cognitive impairment [6], is also associated with decreased olfactory function [27]. Compared with APOE ɛ4 non-carriers, the ɛ4 carriers had worse olfactory function, consistent with previous studies [27, 28]. Olfactory dysfunction is a predictor and a diagnostic marker of AD, partly for the spatial and temporal patterns of pathological progression in neurodegenerative diseases [18]. Brain regions associated with olfactory function are impaired earlier than that associated with cognition. Neurofibrillary tangles in the olfactory bulb are among the earliest pathologic features of AD, which are also seen in the projection pathways from the olfactory bulb to secondary olfactory brain regions, including the piriform and medial temporal cortex, orbitofrontal cortex, and other limbic regions [18, 29]. Tau pathology occurs earlier in olfactory-pathways than in the brain regions associated with cognitive function, in which the spread of hippocampal Tau pathology is originated from EC [30].
According to several cross-sectional and longitudinal studies, impaired olfaction is believed to be associated with incident MCI/AD or cognitive decline [8 , 31]. In T2DM patients, the alteration of olfactory network appears before clinically measurable cognitive decrements, bridging the gap between the central olfactory system and cognitive decline [32]. A LIFE-Adult-Study based on 6,783 participants had found that better olfactory performance was associated with better cognitive performance [10]. Cognitive assessments comprised tests from 5 different tests and the “Sniffin’ Sticks Screening 12” test have been used to measure olfactory identification performance. However, the ability to discriminate individuals with or without cognitive impairment was limited (AUC = 0.55 to 0.62). A small sample study in 195 elderly people was aimed to find the optimal cut-off scores for screening MCI and dementia [9], and an odor threshold with a cut-off point of 2 showed high validity for distinguish AD from MCI (AUC = 0.72). Longitudinal studies in nationalities and ethnicities gave further proof that olfactory impairment is associated with incident MCI and progression from MCI to AD [8 , 34]. They suggest that olfactory tests have potential for screening MCI or MCI that is likely to progress. Of note is that none of the included studies used for follow-up was odor detection threshold, and whether it could predict progression to MCI/AD requires further evaluation.
We previously reported that odor deficit was strongly associated with cognitive impairment in T2DM patients [6, 15]. To broaden the applicability of these findings, we tested in an approximate to real-world population to provide prospective guidance for screening. To the best of our knowledge, this is the largest sample sizes to test OTS and MMSE score in two independent and heterogeneous cohorts. We established reference data based on a large and representative population, which may be used for rapidly detection of persons with cognitive impairment. The test costs short time (only 1-2 minutes), easy to operate, no need for administration or interpretation by trained personnel, inexpensive and noninvasive. Nonetheless, single OTS is not sufficient to discriminate the degree of cognition impairment, suggesting that combination with other biomarkers for diagnosis of MCI or AD is necessary.
Other limitations of the current study are as follows: Firstly, odor identification (I) or discrimination (D) detection was not applied to assess olfaction in two cohorts for odor threshold (T). Therefore, the data can only partially reflect the olfactory functional domain, and it remains to be determined whether “TDI score” [11] would improve the discriminatory performance. Secondly, the diagnosis of dementia lacks brain imaging or pathology, which might also partly interpret the biased results.
Conclusions
We demonstrated a consistent association between olfactory function and cognitive performance, and the odor threshold test may be used as a tool for screening cognitive impairment in the elderly. Further longitudinal study will confirm that whether the test is suitable to predict the risk of cognitive decline.
Footnotes
ACKNOWLEDGMENTS
We thank all the people who contributed to this program.
FUNDING
This study was supported in parts by the Natural Science Foundation of China (91949205, 31730035, 81721005), the National Key R&D Program of China (2016YFC1305800), the Fundamental Research Funds for the Central Universities (YCJJ202203019), the Hubei Province scientific research project (WJ2021M041), the Wuhan Health Science Foundation (WX20Q04), the Guangdong Provincial Key S&T Program (018B030336001). The funders neither played a role in the study design, conduct, data collection, analysis, interpretation, nor participated in the preparation, review, approval of the manuscript.
CONFLICT OF INTEREST
Jian-Zhi Wang is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.