
Abstract
Background:
Attention is an essential cognitive ability that is necessary in other cognitive processes. Only few studies have focused on decline in specific functions of attention in older adults with cognitive decline. No research explores the difference in the proactive and reactive mode of control between the healthy control (HC) and older adults with subjective cognitive decline (SCD).
Objective:
The current work investigated whether there was any decline in alerting, orienting, and executive control in SCD. Particularly, the present study further explored the impairment of the proactive and reactive control in SCD.
Methods:
We recruited 25 HC and 26 SCD. All participants first finished a set of neuropsychological assessments. They then completed an Attention Network Test for measuring the alerting, orienting, and executive control, the List-wide and the Item-specific Proportion Congruency Effect task for measuring the proactive and reactive mode of control, respectively.
Results:
No difference was found in alerting, orienting, and executive control measured by the ANT between SCD and HC. The results also indicated no difference in the reactive control between SCD and HC. However, older adults with SCD performed worse in the proactive control as compared to HC.
Conclusion:
Older adults with SCD showed an impairment in the proactive control. The current findings help us better understand objective decline in cognitive domains other than memory and shed light on early assessment and prevention of AD.
Keywords
INTRODUCTION
Attentional control, or executive control, plays a crucial role in our goal-directed behavior. It is responsible for the regulation of cognitive processes involved in goal maintaining and updating, in switching focus of attention, in enhancing attention to the relevant information and inhibiting irrelevant information and automatic response tendencies. Attentional control declines with normal aging [1 –3], resulting in decreased ability to pursue and achieve daily life goals in older adults.
Changes in attentional control have been investigated in older adults with normal cognition. However, very few studies have explored attentional control in older adults with subjective cognitive decline (SCD). SCD is a risk factor for Alzheimer’s disease (AD) [4]. AD, as a major cause of dementia, endangers health and life quality of the elderly. Individuals with SCD often subjectively experience declines in memory, though they perform normally at objective neuropsychologic examinations. A large number of studies indicate impairment of episodic memory in SCD [5 –8]. In addition, recent research found declines in several domains of cognition other than memory in SCD [9 –11]. More importantly, some researchers proposed that memory impairment might be due to a decline in attentional control [12, 13]. Thus, investigating attentional control would be important in diagnosis and prevention of SCD.
Previous studies have obtained inconsistent results on whether or not individuals with SCD show any decline in attentional control. Some results indicate no difference between healthy controls and SCD [14]. Others show worse performance in inhibition and alerting in SCD as compared to healthy controls [12, 15]. The mixed findings in previous research might be due to different measures of attention function. There are two types of measures. One is self-reported attention test scores, the other includes reaction time, accuracy rate, and amplitude or latency of event-related potentials in experimental tasks. The self-reported tests suffer from the accuracy issue and are affected by social desirability, which makes it not an ideal choice when testing participants with cognitive decline.
Attentional control is a complex ability that consists of multiple processes. We adopted an attention network test (ANT) to measure three functions of attention: alerting, orienting, and conflict resolution [16]. Those three functions are relatively independent aspects of attention [17], with each activating separate brain networks [16, 18]. This paradigm is often used to explore attentional changes in normal aging. Older adults with normal cognition show worse alerting in ANT compared to younger adults [13, 19]. With cognitive decline, individuals with SCD also performed worse in alerting relative to healthy controls [15]. There is evidence for that normal aging and cognitive decline affect only alerting function.
According to a recent theory on cognitive decline [20], conflict-monitoring and control processes decrease with the development of cognitive decline. This theory would predict worse conflict resolution in SCD than in healthy controls. The results of ANT provide no evidence for the decline of conflict resolution, which may be because the ANT only requires reactive control. Since there is equal opportunity for incongruent and congruent trials to be presented in ANT, individuals have to set stimulus-driven, reactive mode of control in motion to resolve unanticipated conflict. When the conflict can be expected, individuals adopt proactive mode of control [21]. Conflict-monitoring and control is dependent more on proactive than reactive control. By proactive control, people are able to actively maintain attention-guiding rules and prospectively anticipate the forthcoming conflict. SCD may be worse in proactive control as compared to healthy controls.
The present study thus was to explore changes in attentional control in SCD using an ANT and modified versions of Stroop tasks, the proportion Stroop tasks [22]. We attempted to achieve two goals. The first one was to replicate the previous findings of no impairment in conflict resolution tested by the ANT in SCD. The second one was to find decline of proactive control in SCD by the proportion Stroop tasks.
METHODS
Participants
Fifty-one participants were community-dwelling older adults aged 60 years and above who were recruited via word of mouth from a community in Baicheng, Jilin Province. Sample size was determined both based on previous research [15] and by estimation using G*power [23]. Esmaeili et al. [15] reported a significant difference in alerting between SCD group and healthy controls with 17 SCD and 15 healthy controls. The power analysis showed that, a minimum sample size of 24 was required to detect a medium effect (f = 0.25) for α= 0.5 and 1 –β= 0.95 for a 2 groups and 8 within-subject conditions. In the List-wide and the Item-specific Proportion Congruency Effect (PCE) tasks, a minimum sample size of 36 was required to detect a medium effect (f = 0.25) for α= 0.5 and 1 –β= 0.95 for a 2 groups and 4 within-subject conditions. All participants reported to have normal or corrected-to-normal vision, and with normal color vision. Data on demographics, cognitive function assessments, the ANT performance, and the list-wide and item-specific PCE were collected for each participant. The current study was approved by Research Ethics Committee of the Department of Psychology, Renmin University of China (22-010). All participants signed written informed consent. We initially contacted 85 older adults to invite them to participate in the current study. Fifty-six people enrolled and were screened. However, 5 participants quit due to personal reasons.
Age range of participants was 60–80 years. The inclusion criteria specific for SCD included 1) normal cognitive function as evidenced by the Montreal Cognitive Assessment (MoCA≥26) [24]. The score of MoCA was adjusted by adding 1 point to the total score for those participants whose education level was lower than 12 years; 2) subjective memory complaints yet preserved autonomy in daily activities assessed by Chinese version of the Subjective Cognitive Decline- Questionnaire (SCD-Q≥5) [25] and the Functional Activities Questionnaire (FAQ≤9) [26], respectively. The inclusion criteria of healthy controls were similar to SCD: MoCA≥26 and FAQ≤9, except for one score, SCD-Q < 5. The exclusion criteria were: (a) known history of mental disease and other illness (e.g., major depressive disorder, substance use, traumatic brain injury, or neurodegenerative disease); (b) inability to take neuropsychological assessments; (c) severe loss of vision, hearing, or communicative ability. There were 26 SCD and 25 healthy controls (HC).
Measurements
Neuropsychological assessment
Neuropsychological tests were administrated by a master student majoring in psychology. In general cognitive function, Chinese MoCA was scored [24]. Subjective complaints of memory decline was assessed by Chinese version of SCD-Q [25]. Memory function was assessed in episodic memory evaluated by the Auditory Verbal Learning Test-HuaShan version (AVLT-H) [27, 28] and in working memory assessed by the Digital Span Test (DST), including the Digit Span Forward Test (DSFT) and Digit Span Backward Test (DSBT) [29, 30]. Executive function and visuospatial ability were assessed by the Trail Making Test-B (TMT-B) [31, 32], the Verbal Fluency Test (VFT) [33], the Controlled Oral Word Association Test (COWAT) [34], the Clock Drawing Test (CDT) [35], and the Rey-Osterrieth Complex Figure Test (ROCFT) [36]. Language function was assessed by the Boston Naming Test (BNT) [37]. The processing speed was evaluated by the Symbol Digit Modalities Test (SDMT) [38]. Autonomy of activities in daily life was assessed by the FAQ [26]. The Chinese version of Hospital Anxiety and Depression Scale (HADS) [39] and the Positive and Negative Affect Scale (PANAS) [40] were used to evaluate anxiety and depression symptoms and emotional state.
The ANT
The ANT combined the precuring paradigm and the Flanker task (see Fig. 1) [18]. Participants pressed two keys to respond to the direction of a target arrow. The target arrow either pointed to a the same direction (the congruent condition) or a different direction (the incongruent condition) from the distractor arrows. Alerting, orienting, and executive control functions are measured by differences in reaction times (RT) between conditions. Alerting is the RT difference between no cue and the double cue conditions (Alerting = RTNo cue –RTDouble cue). Orienting is the RT difference between the center cue and the spatial cue conditions (Orienting = RTCenter cue –RTSpatial cue). Executive control is the RT difference between the incongruent and congruent conditions (Executive control = RTIncongruent –RTCongruent).
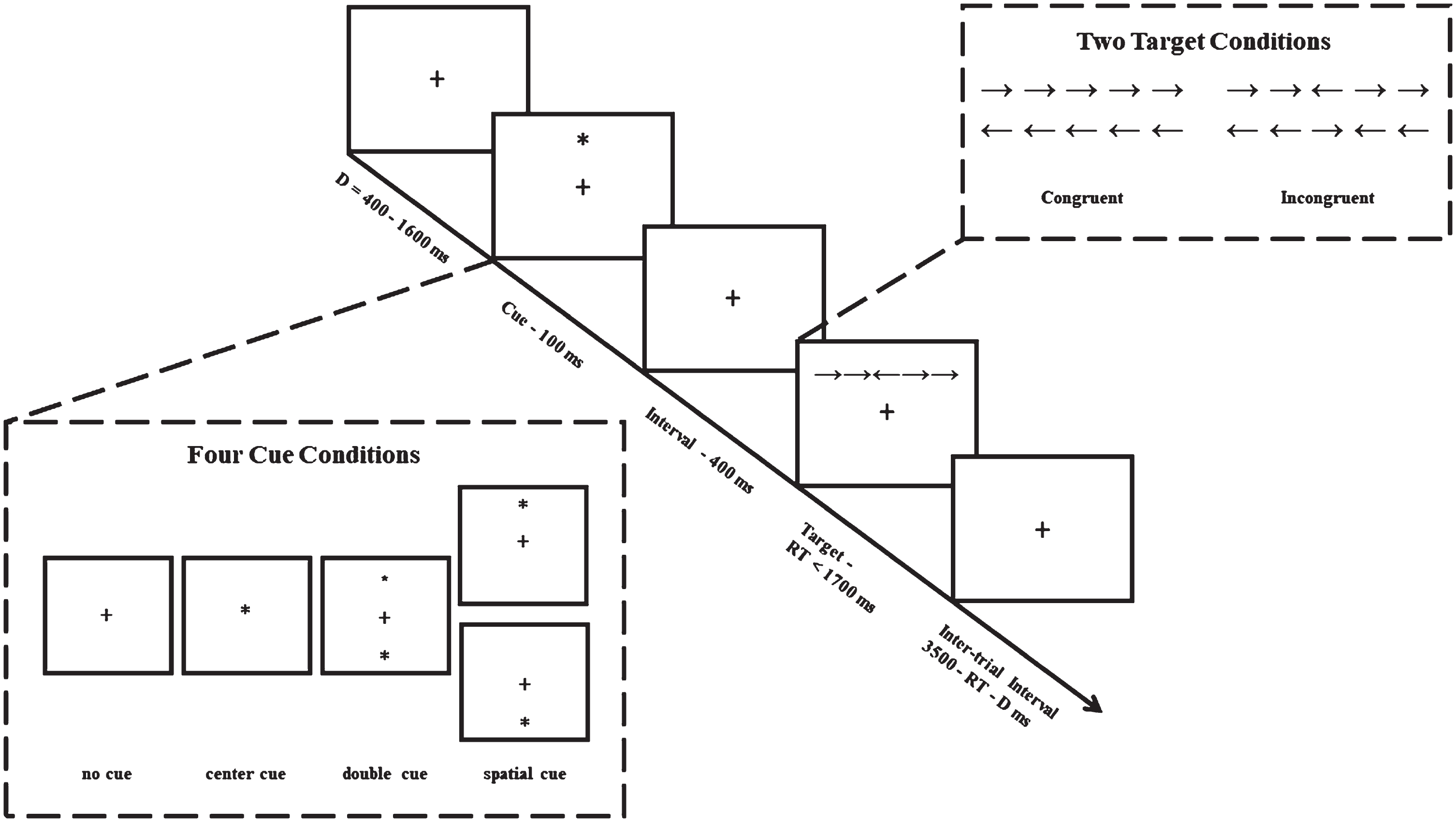
Attention Network Test [18]. The four types of cues (i.e., no cue, center cue, double cue, and spatial cue) were shown in the rectangle on the left. Two target conditions (congruent versus incongruent) were shown in the rectangle on the right.
On each trial, participants first saw a fixation randomly presented for 400–1600 ms, and then a cue (in the spatial cue and the central cue conditions) or two cues (in the double cue condition) for 100 ms followed by a 400 ms fixation. After the fixation disappeared, there was the target display remaining on the screen. Participants had to press the response key within 1700 ms. The fixation of the next trial was then presented after the response display. The duration of this display was intertrial interval, which was determined by subtracting the duration of the prior trial from 3500 ms to balance the duration of each trial. There were 192 trials divided in three blocks. Each participant could have a self-paced break after finishing a block. There was a practice block before the real experiment. It took about 20 min to complete the entire experiment.
We used a 4 (cue type: no cue, center cue, double cue, and spatial cue) x 2 (congruency: congruent versus incongruent) x 2 (group: SCD versus HC) mixed design, where cue type and congruency were within-subject variables and group was a between-subject variable.
In the final analyses, inaccurate responses and responses with reaction time longer than 1700 ms or shorter than 200 ms were deleted. Thirty hundred and sixteen trials (3.23%) were excluded from the final analyses, which were due to inaccurate responses.
The List-wide PCE Task
We adopted the same list-wide and item-specific PCE tasks used in [41]. The list-wide PCE task was a modified Stroop task. Four color words, “RED” (“ ” in Chinese), “BLUE” (“
” in Chinese), “BLUE” (“ ”), “GREEN” (“
”), “GREEN” (“ ”), and “YELLOW”(“
”), and “YELLOW”(“ ”), were selected as stimuli. In the congruency condition, each word was presented in its corresponding color. In the incongruency condition, “RED” was only presented in blue and “BLUE” was only presented in red; similarly, “GREEN” was only presented in yellow and “YELLOW” was only presented in green. There were two blocks in the task: the MC and MI blocks. In the MC block, majority of the trials (75%, 72 trials) were congruent. The proportions were reversed in the MI block.
”), were selected as stimuli. In the congruency condition, each word was presented in its corresponding color. In the incongruency condition, “RED” was only presented in blue and “BLUE” was only presented in red; similarly, “GREEN” was only presented in yellow and “YELLOW” was only presented in green. There were two blocks in the task: the MC and MI blocks. In the MC block, majority of the trials (75%, 72 trials) were congruent. The proportions were reversed in the MI block.
On each trial, a fixation appeared and remained on the screen for 250 ms. There was then a 250 ms interstimulus interval that was followed by the target display. The target remained on the screen for 2000 ms. There then were a 300 ms blank screen and a 500 ms feedback for correct, incorrect, and no response. Participants pressed one of the four keys to respond: H key for red word, J key for blue word, K key for green word, and L key for yellow word. Those keys were labelled by small color patch. Each participant had to complete 16 practice trials before entering the real experiment. The order of the MC and MI block was counterbalanced between participants. There were 192 trials in total. Participants had a self-paced break after finishing one block. It took about 11 minutes to complete the experiment.
It was 2 (Block: MC versus MI) x 2 (congruency: congruent versus incongruent) x 2 (group: SCD versus HC) mixed design, where block and congruency were within-subject variables and group was a between-subject variable.
The Item-specific PCE task
The color words in the item-specific PCE task were the same as in the list-wide PCE task. In addition, we used four pseudowords presented in those same colors to control the effect of contingency learning [42, 43]. In the Stroop block, “RED” and “BLUE” were predefined as the MC items, and “GREEN” and “YELLOW” were the MI items. A 48-trial MC set consisted of 32 trials (75%) of red “RED” and blue “BLUE”, and 16 trials (25%) of blue “RED” and red “BLUE”. A 48-trial MI set involved 32 trials of yellow “GREEN” and green “YELLOW”, and 16 trials of green “GREEN” and yellow “YELLOW”. Items from the MC and MI sets were intermixed in one 96-trial block. The probability of congruent/incongruent trials was fixed at 50% in the block. There were 96 trials in the pseudowords block.
Participants had to finish two blocks. One was color words and the other was pseudowords. The trial procedure was the same as in the list-wide PCE task. It took approximately 11 min to finish this task.
It was 2 (Item: MC versus MI) x 2 (congruency: congruent versus incongruent) x 2 (group: SCD versus HC) mixed design, where item and congruency were within-subject variables and group was a between-subject variable.
In both the list-wide and the item-specific PEC tasks, participants whose accuracy rate was lower than 75% were not included in the final analyses [44]. No participant was excluded.
The study procedure
Each participant signed an informed consent form and was informed the goal of the current study. The researcher then collected the demographic and neuropsychological data. After that, participants successively complete the ANT, the list-wide PCE task, and the item-specific PCE task. There was a 10-min break between tasks.
RESULTS
Table 1 shows demographic data and mean scores of each neuropsychological assessment for two groups. There was no significant difference in age and gender proportion in HC and SCD. However, the level of education was higher in HC than in SCD, and depression score was lower in HC than in SCD. Those results were similar to previous research [45 –48]. In daily activity and cognitive domains, HC did better in functional activities and the AVLT-H (recognition) as compared to SCD [28]. No significant differences in other cognitive abilities were found.
Demographic Characteristics and Cognitive Status of the HC and SCD
Demographic Characteristics and Cognitive Status of the HC and SCD
Values are expressed as mean and standard deviation with the exception of those denoting percentage and number of individuals for gender. * p < 0.05. SD, standard deviation; HC, healthy control; SCD, subjective memory decline; MoCA, Montreal Cognitive Assessment; SCD-Q, Subjective Cognitive Decline-Questionnaire; FAQ, Functional Activities Questionnaire; AVLT-H, Auditory Verbal Learning Test-HuaShan version; HADS, Hospital Anxiety and Depression Scale; PANAS, Positive and Negative Affect Schedule; PA, positive affect; NA, negative affect; DSFT, Digit Span Forward Test; DSBT, Digit Span Backward Test; TMT-B, Trail Making Test-B; VFT, Verbal Fluency Test; COWAT, Controlled Oral Word Association Test; CDT, Clock Drawing Test; ROCFT, Rey-Osterrieth Complex Figure Test; BNT, Boston Naming Test; SDMT, Symbol Digit Modalities Test.
Results of the ANT: No difference between SCD and HC in altering, orienting, and executive control
We first conducted a 4 (Cue: no cue, the central cue, the double cue, and the spatial cue)×2 (Congruency: congruent versus incongruent)×2 (Group: the HC versus the SCD) repeated-measures analysis of variance (ANOVA) for mean reaction times of each condition. Then, independent sample t-tests were conducted for the alerting, orienting, and executive control scores. The post hoc power analysis revealed that, given sample size of 51, the power to detect medium effect size (f = 0.25) in this design was≥0.99.
Mean reaction times and standard deviations in each condition for the two groups are shown in Table 2. The results of the repeated-measures ANOVA showed a significant main effect of congruency (F(1, 49) = 316.92, p < 0.05, η p 2 = 0.87) and a significant main effect of cue (F(2.35, 115.23) = 40.14, p < 0.05, η p 2 = 0.45). The main effect of group failed to reach the significance level (F(1, 49) = 0.4, p = 0.53, η p 2 = 0.01). The interactions of group×cue was significant (F(3, 47) = 3.16, p < 0.05, η p 2 = 0.06). The other interactions were not significant: group×congruency, F(1, 49) = 0.16, p = 0.69, η p 2 = 0.00; cue×congruency, F(2.47, 120.96) = 2.58, p = 0.07, η p 2 = 0.05; the 3-way interaction, F(3, 47) = 0.49, p = 0.69, η p 2 = 0.01.
Mean Reaction Times (ms) and Standard Deviations (in the parentheses) in Each Condition for the HC and SCD in the ANT
The results of t-tests for scores of alerting, orienting, and executive control revealed no significant differences in alerting (t = 1.26, p = 0.21, Cohen’s d = 0.35), orienting (t = 1.28, p = 0.21, Cohen’s d = 0.36), and executive control (t = 0.43, p = 0.67, Cohen’s d = 0.12) scores between the HC and SCD. The results showed that SCD performed the same as the HC in alerting, orienting and executive control. After controlling depression and education level [47, 49], the results remained the same.
Result summary for the ANT
The omnibus ANOVA showed a significant congruency effect for both SCD and HC groups, indicating that both groups responded faster for the congruent targets than the incongruent ones. As for three functions of attention: alerting, orienting, and executive control, there was no group difference in RTs.
Table 3 shows mean reaction times in each condition for the two groups. The 2 (Block: MC versus MI) ×2 (congruency: congruent versus incongruent) ×2 (group: SCD versus HC) ANOVA revealed a significant main effect of congruency (F (1,49) = 98.5, p < 0.001, η p 2 = 0.67), which indicated a congruency effect. That is, responses in the congruent condition were faster than in the incongruent condition. The results also showed significant interactions. The interaction of congruency×group was significant (F(1,49) = 6.34, p < 0.05, η p 2 = 0.12). The block×group interaction reached the significance level (F(1,49) = 5.26, p < 0.05, η p 2 = 0.10). The block×congruency interaction was also significant (F(1,49) = 61.13, p < 0.001, η p 2 = 0.56). The main effects of group (F(1, 49) = 0.45, p = 0.50) and block (F(1, 49) = 2.32, p = 0.14, η p 2 = 0.05) failed to reach the significance level.
Mean Reaction Times (ms) and the Standard Deviation (in the parentheses) in Each Block and Congruency Condition of Stroop for the HC and SCD in the List-wide PCE task
Mean Reaction Times (ms) and the Standard Deviation (in the parentheses) in Each Block and Congruency Condition of Stroop for the HC and SCD in the List-wide PCE task
Most importantly, we found a significant 3-way interaction (F(1,49) = 4.14, p < 0.05, η p 2 = 0.08). The simple effect analysis showed a significant block×congruency interaction for both the HC (F(1,24) = 36.6, p < 0.01, η p 2 = 0.60) and the SCD (F(1,25) = 24, p < 0.01, η p 2 = 0.49).
The list-wide PCE refers to smaller congruency effects in a list with mostly incongruent (MI list) trials than a list with mostly congruent (MC list) trials [50]. We calculated PCE for each participant in the two groups then conducted an independent sample t-test on PCE. The results indicated a significantly larger PCE for the HC compared to the SCD (t = 2.02, p < 0.05, Cohen’s d = 0.57).
Result summary for the List-wide PCE
We found a larger List-wide PCE for the HC (76.43 ms) than for SCD (45.47 ms). A larger PCE indicates a better proactive control. Those results indicated that the HC had better proactive control as compared to SCD.
Results for the Item-specific PCE task: No decline in the reactive mode of control in SCD
In both the List-wide and the Item-specific Proportion Congruency Effect (PCE) tasks, post hoc power analysis revealed that, given sample size of 51, the power to detect medium effect size (f = 0.25) in the design was≥0.99. Table 4 shows mean reaction times in each condition of the Stroop Block for the two groups in the Item-specific PCE task. The ANOVA revealed a significant main effect of congruency (F(1,49) = 19.56, p < 0.001, η p 2 = 0.29), which indicated a congruency effect. The results also showed a significant interaction of block and congruency (F(1,49) = 4.58, p < 0.05, η p 2 = 0.09). However, the other 2-way interactions failed to reach the significance level: congruency×group interaction, F(1, 49) = 2.41, p = 0.13, η p 2 = 0.05; block×group interaction, F(1, 49) = 0.75, p = 0.39, η p 2 = 0.02. The main effects of group and block failed to reach the significance level, group: F(1, 49) = 2.33, p = 0.13, η p 2 = 0.05 and block: F(1, 49) = 1.78, p = 0.19, η p 2 = 0.04; The 3-way interaction was also not significant (F(1, 49) = 0.68, p = 0.41, η p 2 = 0.01).
Mean Reaction Times (ms) and the Standard Deviation (in parenthesis) in Each Condition of the Stroop Block for the HC and SCD in the Item-specific PCE task
The item-specific PCE is the smaller congruency effect for stimulus pairs with more incongruent items (MI items) compared to pairs with more congruent items (MC items) [51]. We calculated the item-specific PCE for each participant in the two groups then conducted an independent sample t-test on PCE. The results showed no significant difference between the HC and the SCD (t = 0.83, p = 0.41, Cohen’s d = 0.23).
Results summary for the Item-specific PCE
The item-specific PCEs were statistically similar for the HC (12.63 ms) and SCD (29.90 ms). The item-specific PCE reflects the reactive control. Our results indicated that there was no impairment in the reactive control for SCD.
We also conducted ANOVAs for mean accuracy rates of each task. The results are shown in the Supplementary Material.
DISCUSSION
It is poorly understood how attentional functions change with cognitive decline. Jessen and colleagues [52] argued that it was more important to assess attentional functions in SCD other than memory, which was essential in developing scientific assessment tools for SCD. Impairments in attention was obvious in patients from early to late stage of AD [13 , 54]. However, very few studies have focused on decline in specific functions of attention in older adults with cognitive decline. The current work focused on exploring the changes of attentional functions in SCD. We first used the ANT paradigm to test alerting, orienting, and executive control functions in older adults with normal cognition and SCD. The results showed no difference in those three functions between HC and SCD. Since the ANT only reflects one type of attentional control in conflict resolution, we then adopted the list-wide and the item-specific PCE to investigate the changes of the reactive control and the proactive control in SCD. We replicated the results in the ANT. That is, there was no difference in the reactive control between HC and SCD. More importantly, we found better proactive control in HC than in SCD.
No evidence for impairment of attentional alerting, orienting, and executive control in SCD
Researchers used differential tasks and paradigms to investigate the changes of attentional functions in older adults with cognitive decline [12 , 56], which might cause problems in comparison between research. One benefit of the ANT is that to test three attentional functions in the same task. Our findings indicated no difference in alerting, orienting, and executive control between HC and SCD. The present results were not consistent with Esmaeili et al. [15] who found worse performance in alerting in SCD than in HC.
There is evidence for culture-related differences in attention. Some research revealed that Chinese adults respond faster in alerting relative to Western adults [57]. In addition, researchers found no difference in alerting for Chinese older adults with MCI and normal cognition [58, 59]. Logically, no difference should be found between SCD and HC, either. Another reason for the inconsistency between Esmaeili et al.’s and our results might lie in the differences in inclusion/exclusion criterion of SCD. Esmaeili et al. used two questions (i.e., “Do you feel like your memory is becoming worse?” and “Did that worry you?”) to recruit SCD, whereas the present study used a set of neuropsychological questionnaires. Participants with SCD in Esmaeili et al.’s study showed no difference in all cognitive domains as compared to HC. However, older adults with SCD in our study performed worse in episodic memory than HC. Individual differences in SCD samples may result in difference in alerting between the present study and Esmaeili’s study. Furthermore, McDonough et al. [13] found that normal aging was related to the impairment of alerting tested in the ANT and that there was no correlation between decline of alerting and the development of AD.
Except for alerting, our results also showed no difference in orienting and executive control between HC and SCD. Both groups benefited equally from the spatial cues, which replicated the previous findings [19, 59] Orienting in attention does not decline with normal aging. Older adults with normal cognition performed as well as younger adults in ANT-orienting index [19 , 61]. For executive control, McDonough et al. [13] found strong relation between impairment of executive control and early stage of AD. Cromarty et al. [62] also reported significant impairment in executive control in AD. However, the current work and Esmaeili et al. failed to provide evidence for the decline of executive control in SCD. The inconsistency may be due to different tasks used to measure executive control.
Decline of the proactive mode of control in SCD
The most important finding of our research is the worse proactive control in SCD than in HC. According to Braver et al. [21], individuals rely on dual mechanisms of attentional control: the proactive and the reactive mode of control. The former is goal-directed and the latter is stimulus-driven. A majority of tasks used in the previous research test the reactive mode of control. Recent studies have examined the proactive and the reactive mode of control in normal aging [2, 3]. However, as far as we know, no research has explored the dual mechanisms of attentional control in SCD.
We adopted the list-wide and the item-specific PCE paradigm to test the proactive control and the reactive control, respectively. The results of the present study revealed a larger List-wide PCE in HC than in SCD, which demonstrated better proactive control in HC as compared to SCD. However, the difference in the magnitude of Item-specific PCE was not significant. In other words, we found no difference in the reactive control between SCD and HC. Older adults with SCD showed worse proactive control than HC, but they performed the same in the reactive control. Our results were consistent with Braver et al. [63]. They also found worse proactive control in older adults on early stage dementia of the Alzheimer’s type (DAT) relative to HC and similar performance in the reactive control. The proactive control requires individuals continuously activate information on specific goals, which consumes more cognitive resources than does the reactive control. Older adults with SCD either do not have enough cognitive resources or do not have the same ability to recruit cognitive resources due to general decline in cognition, resulting in worse proactive control. The reactive control is stimulus-driven and does not require extra resource. Older adults with SCD show no impairment in the reactive control.
SCD individuals experience more conflicts between perceived representation and reality and form the belief of cognitive decline. They then make more efforts to make themselves perform normally [20]. Hyperactivation in the PFC may be related to the extra efforts in SCD. As mentioned by Mizuno [20], such compensatory hyperactivation may lead to neuronal death [64], further resulting in decline of core cognitive structure. This also explains why SCD individuals are more likely to develop into MCI and even into AD than HC.
There were some limitations in the present study. Firstly, older adults in the present study had to finish all the neuropsychological tests and then completed three tasks. Each participant spent almost two hours to finish the entire study. Many participants might feel tired during the experiment, which may result in the fatigue effect. Secondly, all three tasks for testing attentional function measured reaction times and accuracy. Older adults’ response was easily affected by speed-accuracy tradeoff. After finishing the experiment, some of our participants reported that they tried their best to do well so that they could get a higher score. They preferred accuracy more than speed. Thirdly, we used a cross sectional design. The further research should consider longitudinal designs. Finally, the sample size was not large enough, because many people quit the study due to too many tests.
Future directions
Future work should adopt tasks other than the list-wide and item-specific PCE paradigm to examine the proactive and reactive control in SCD and MCI. For example, the AX-continuous performance test (the AX-CPT) can be used [65]. The AX-CPT is a simpler task than the list-wide and item-specific PCE and is better suitable for older adults with lower cognition. Since speed-accuracy tradeoff has significant effect on results, further research should choose tasks focus on accuracy only. The antisaccade task with accuracy measure is free from the influence of speed-accuracy tradeoff. This task is highly reliable (with effect size around 0.90) in measuring individual differences in cognitive control [66]. Future work can also combine behavioral and neurocognitive indices to explore neural mechanisms of attention changes in SCD.
Conclusion
More than one cognitive domain other than memory declines in SCD. When testing with the ANT, SCD individuals perform as well as HC in alerting, orienting, and executive control. However, older adults with SCD show an impairment in the proactive control. Our findings shed light on developing scientific and objective assessment tools.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all the participants and their families who gave their time and energy to support these three reported experiments.
FUNDING
This work is supported by the Fundamental Research Funds for the Central Universities, and the Research Funds of Renmin University of China (Grant number: 19XNB033).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.