
Abstract
Background:
Studies have reported the associations between inflammation, brain volume, and cognition separately. It is reasonable to assume peripheral inflammation may contribute to cognitive decline through brain volume atrophy.
Objective:
To examine the associations between peripheral inflammation, brain volume, and cognition among adults, and to investigate whether brain volume atrophy mediates the inflammation-cognition relationship
Methods:
We retrieved 20,381 participants with available data on peripheral inflammation, brain volume, and cognition from the UK Biobank cohort. Cognitive function was assessed by performance on cognitive tasks probing various cognitive domains. Brain volumes were measured by magnetic resonance imaging (MRI). Multivariable linear models were used to investigate the associations between three peripheral inflammatory indexes (C-reactive protein, systemic immune-inflammatory index, neutrophil-to-lymphocyte ratio), brain volume, and cognition. Mediation analyses were conducted to assess the potential mediating effect of brain volume atrophy. All results were corrected for multiple comparisons using the false-discovery rate (FDR).
Results:
Peripheral inflammation was inversely associated with grey matter volume (GMV), white matter volume (WMV), and cognition after adjusting for potential covariates. For instance, CRP was associated with the GMV of left parahippocampal gyrus (β= –0.05, 95% confidence interval [CI]: –0.06 to –0.04, pFDR =1.07×10-16) and general cognitive factor (β= –0.03, 95% CI: –0. –0.04 to –0.01, pFDR = 0.001). Brain volume atrophy mediated the inflammation-cognitive decline relationship, accounting for 15–29% of the overall impact.
Conclusion:
In this cohort study, peripheral inflammation was associated with brain volume atrophy and cognitive decline. Brain atrophy may mediate the inflammation-cognitive decline relationship.
INTRODUCTION
Cognition is a normal mental process for knowledge acquiring, understanding, and reasoning. Cognition decline disturbs normal life and may potentially lead to dementia disorder after a period of subtle cognition change, posing a burgeoning public health challenge globally [1]. Early management of cognitive decline risk factors is pivotal for preserving cognitive health, attenuating cognitive impairment and dementia progression, and thus holds significance for public health.
Current studies have established a link between peripheral inflammatory biomarkers and cognitive function, such as interleukin-6 and C-reactive protein (CRP) [2, 3]. Integrated inflammatory indexes such as systemic immune-inflammatory index (SII) and neutrophil-to-lymphocyte ratio (NLR) which take into account both overall immune status and systemic inflammation, have been extensively used to predict various clinical outcomes [4, 5]. More recently, SII and NLR have also been reported to have a predictive value in the cognitive outcomes of patients with specific diseases [6]. However, the associations of integrated inflammatory indexes with cognitive decline in various cognition domains in the general population remain unclear.
Advancements in neuroimaging have enabled the identification of neurodegenerative processes with heightened sensitivity [7]. A few studies have reported that brain volume reduction such as atrophy in grey matter volume (GMV) was associated with cognition impairment [8, 9]. Moreover, inflammation could affect the brain structure and further leading cognitive impairment [10, 11]. For example, Conole et al. found a mediation effect of brain structure on the association between the DNA methylation signature of CRP and cognitive ability [10]. We thus hypothesized that brain volume atrophy would have a mediation effect on the inverse associations between peripheral inflammation and cognitive decline, which may help explain the pathway of peripheral inflammation on cognition. However, there remains a lack of consensus regarding this hypothesis, and its potential mediating effect on the general population has yet to be accurately quantified and studied in population-based cohorts.
We conducted this study with the aim to investigate the association between peripheral inflammation, brain volume, and cognition among individuals without neurological conditions in the UK Biobank (UKB) cohort and explore whether brain volume atrophy mediates the effect of peripheral inflammation on cognitive function (elevated level of peripheral inflammation ⟶ brain volume atrophy ⟶ cognitive decline).
METHODS
Study participants
Our analysis was based on UKB, a natural population-based, prospective cohort of over 500,000 adults aged 40–69 years. The participants were recruited from 23 assessment centers, and the baseline survey was conducted between 2006 and 2010. The study protocol of UKB can be found elsewhere [12]. The UKB dataset is a comprehensive collection of genetic, health, and lifestyle information about individuals in the UK, including demographic information, self-reported health behaviors, biological measures, results of clinical exams, and genome-wide genotyping data. The data was collected by touch-screen questionnaires, physical and functional measures, biological examination, and so on. The full UKB dataset is supplemented with various clinical outcomes by linking with electronic health records.
Among participants who had their peripheral inflammation examined at baseline, we excluded those with acute infection (CRP > 10 mg/L) and self-reported neurological conditions, including dementia (Alzheimer’s disease, Vascular dementia, and Other dementia), and other neurological conditions (multiple sclerosis, cognitive impairment, Parkinson’s disease, neurological injury and trauma, chronic degenerative neurological problems, and head injury), as well as participants with missing data of important covariates. This study ultimately involved 20,381 participants with cognitive function, peripheral inflammation, and brain volume assessed for main analysis (Fig. 1).
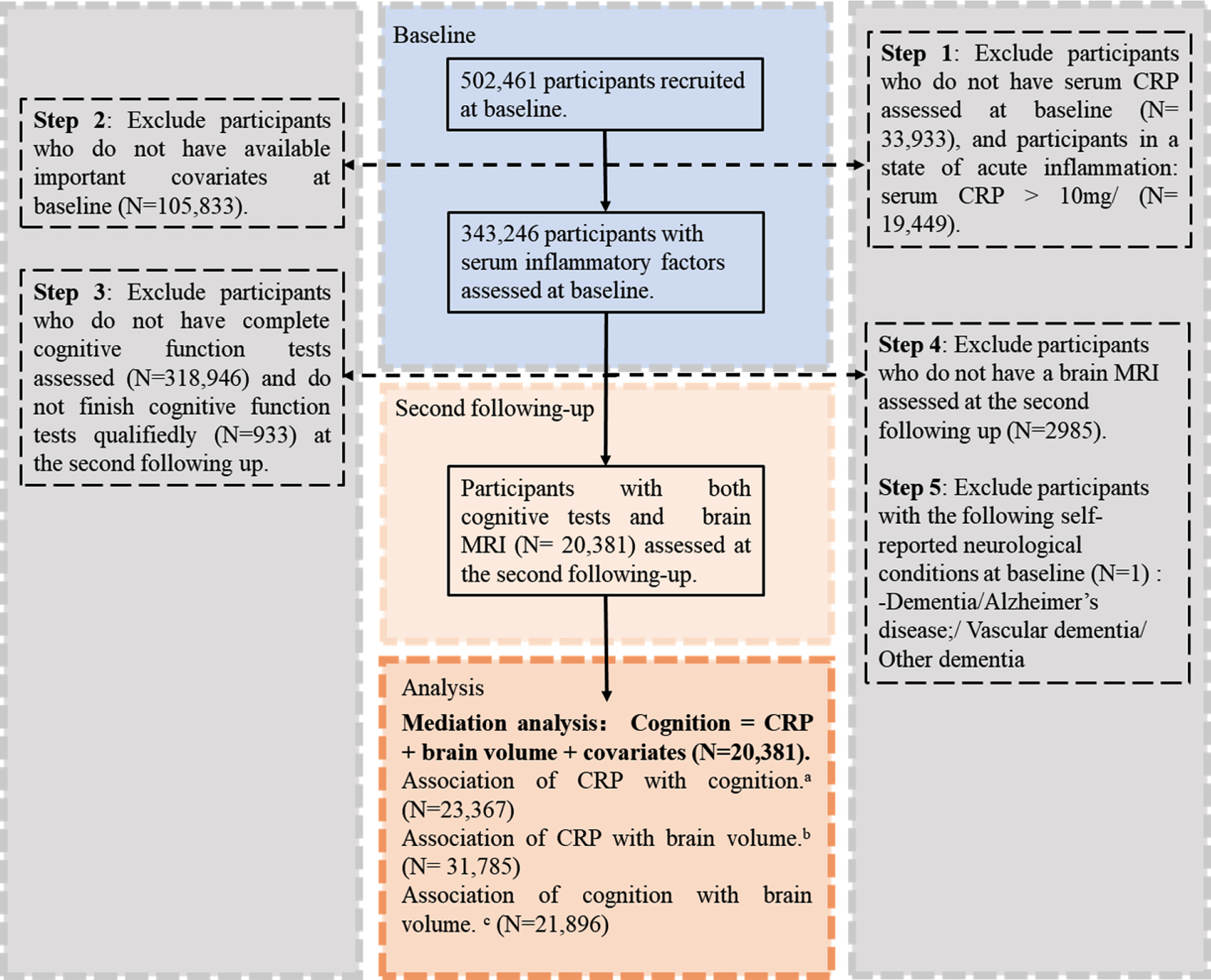
Flowchart Depicting the Population Selection Process for Analyses from the UKB (taking CRP as an example of the inflammatory index). The superscript “a” denotes the study subjects with complete data on CRP and cognition, CRP and brain volume, and cognition and brain volume respectively.
All participants provided electronic informed consent and UKB received ethical approval from the North West Multi-center Research Ethics Committee covering the whole of the UK.
Inflammatory indexes
UKB has embarked on a project to measure a variety of biochemical markers in available biological samples collected at baseline (2006–2010). The assay of peripheral blood samples was conducted by a Beckman Coulter LH750 Hematology Analyzer within 24 h of collection at UKB central laboratory. Specifically, peripheral CRP levels (mg/L) were measured using the Immunoturbidimetric-high sensitivity system on Beckman Coulter AU5800 analytical platform. Neutrophil counts (N, cells/mm3) and lymphocyte counts (L, cells/mm3) were calculated using differential absolute quantities. Platelet counts (P, cells/mm3) were obtained directly using complete blood count.
Based on peripheral blood cell counts, two systemic inflammation indexes were calculated. The NLR was defined as NLR = N/L. The SII was calculated as SII = (P×N)/L. Due to the non-normal distribution of CRP, NLR, and SII values, log-transformed values were used in analyses. NLR and SII values > 99.73% or<0.27% after log transformation was considered extreme and were removed.
Cognitive function measurement
Six cognitive tests (Numeric Memory Test, Fluid Intelligence Test, Symbol digit substitution test, Trail Making Test B, Matrix Pattern Completion, Tower Rearranging Test) were included in this analysis, involving measurements of various cognitive domains: working memory, verbal and numerical reasoning, processing speed, executive function, and non-verbal reasoning. Psychometric properties, reliability, and validity of cognitive tests in UKB have been mentioned in detail elsewhere [13]. Participants underwent cognitive tests through a fully-automated touchscreen assessment which was designed to be administered unsupervised [13, 14]. The raw data of cognition tests were normalized and reversed, where required, and converted to Z-scores as described previously [15, 16]. Eventually, cognitive scores were positively correlated with each other with a higher cognitive score indicating a better cognition performance. Full details of each cognition test are provided in Supplementary Methods 1.
Principal components analysis was used to identify patterns and reduce the dimensionality of cognitive data while capturing the most important variations in the information contained in multiple cognitive tests and summarizing the original data into a new set of variables called principal components [17]. The general factor of cognition in this study, represented by the first principal component, is a measure of general cognitive performance and accounts for 45.68% of the variation in the above cognitive scores.
Brain image data
We used structural MRI data of the brain from the UKB dataset. All brain MRI data were acquired on a standard Siemens Skyra 3T scanner with a 32-channel RF receiver head coil, with the imaging matrix tilted down 16 degrees along the AC-PC line [18, 19]. GMV, white matter volume (WMV), and subcortical volumes were processed by the UKB team and made available to approved researchers as imaging-derived phenotypes [18]. We included pre-processed data of imaging-derived phenotypes of brain structure, including total GMV, total WMV, and regional GMV of 98 cortices (49 in each hemisphere), 12 subcortices (thalamus, caudate, putamen, pallidum, hippocampus, and amygdala in each hemisphere), 28 cerebellum regions and brain stem in mm3. To present the volume of cortical grey matter more concisely, we combined the GMV of 98 cortical structures into 76 regions (38 in each hemisphere) on the basis of parcellations from the Harvard–Oxford cortical and subcortical atlases.
Covariates
Covariates were chosen based on the availability of variables and potential confounders known to affect inflammation, brain volume, and cognition. Sociodemographic factors (age, sex, ethnicity, and Townsend deprivation index), and information on lifestyle factors (smoking status, body mass index (BMI), alcohol intake, physical activities, and HbA1c) at baseline were extracted. Full details of each covariate are provided in the Supplementary Methods 2.
Statistical analysis
To examine whether brain volume mediates the effect of inflammation on cognition, a two-stage analytic approach was used in our study. In the first stage, the associations between the inflammatory indexes, regional brain volume, and general cognitive function were examined using multivariable linear regression models adjusting for potential covariates: linear regression coefficients (β) and robust standard errors (SE) were reported for all models. In the second stage, we conducted mediation analyses to test the mediation effect of brain volume, quantifying indirect associations acting through brain volume as a mediating variable, the direct associations not mediated by brain volume, and their bootstrapped standard errors (Fig. 2).
Both single and multiple mediation analyses in this study obeyed two basic assumptions: 1) inflammatory indexes are significantly associated with brain volume, and 2) brain volumes are significantly associated with cognitive function. In the mediation analysis, we specified regression models (package “burceR” in R) to assess the potential mediation effect of brain volume atrophy (M) on the pathway “inflammation (X) ⟶ cognitive decline (Y)”:
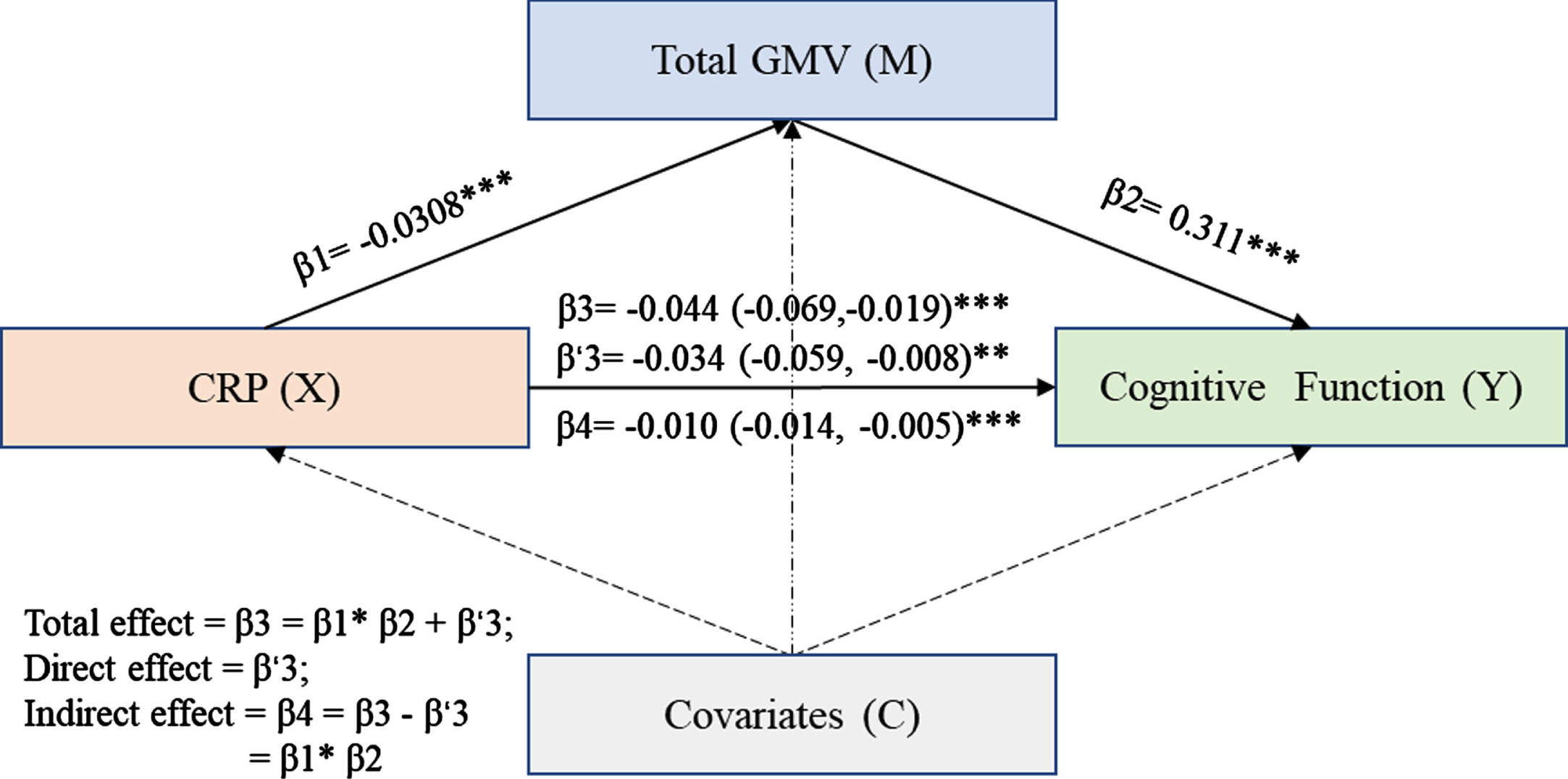
Brain Structure Mediated the Association of Inflammation with Cognition Decline (CRP⟶Total GMV⟶Cognitive Function as an example). The association between CRP and cognitive function (β3, p < 0.001) was significantly, and partially mediated by GMV (β4, p < 0.001). Analysis was adjusted for age, sex, ethnicity, alcohol consumption, physical activity, smoking, BMI, HbA1c, and deprivation index. GMV, grey matter volume; CRP, C-reactive protein; NLR, neutrophil to lymphocyte; SII, systemic immune-inflammatory index.
where Mi indexes the regional brain volume, X represents levels of inflammatory indexes, and C represents covariates included in model. In multiple-mediators model, brain volume including total GMV and total WMV entered parallelly as multi-mediators. To further explore the mediation effect of brain volume, we define “cognitive function related-regions” according to associations between regional brain volume and cognitive function as well as previous studies. These regions contained the frontal pole, insular cortex, and amygdala. We calculated the direct effect and indirect effect with a bootstrap procedure (1,000 replications). Proportions of the indirect effect of brain volume atrophy on associations between elevated inflammation and cognitive decline attributable were evaluated. We adopted the Benjamini–Hochberg false discovery rate (FDR) correction to address multiple comparison issues.
During the analysis process, we conducted a preliminary standardization of cognitive scores (Ys) and brain volumes (Ms). Additionally, we identified and removed outliers in brain volume (Ms) with values above 99.73% and below 0.27%. All statistical analyses were conducted in R software (version: 4.1.2). p values (two-tailed) smaller than 0.05 were considered statistically significant.
Sensitivity analysis
Additional sensitivity analyses were performed to examine the robustness of our results: 1) we estimated whether the mediation effect of GMV varied according to different cognitive domains. The mediation analyses were repeated in the single cognitive domain, which showed a significant association with inflammation in this study; 2) to examine whether the hypothesized mediation was modified by sex, age, and the use of anti-inflammatory drugs, moderated mediation analyses were conducted with sex, age, the use of anti-inflammatory drugs as moderators; 3) further adjustment for follow-up interval as a potential confounder; 4) further adjustment for education as a potential confounder and stratification analysis for modification effect of education on the association between brain volume and cognition; and 5) excluding the participants with other neurological conditions (multiple sclerosis, cognitive impairment, Parkinson’s disease, neurological injury and trauma, chronic degenerative neurological problems, and head injury).
RESULTS
Descriptive results
Of 20,381 participants with complete data on inflammatory indexes, cognitive tests, and brain volume, 10,384 (50.95%) were male, and the mean (SD) age was 54.27 (7.45) years (Supplementary Table 1). 97.34% of participants were white, and their mean (SD) BMI was 26.34 (4.02). The sample used here was more often moderate alcohol drinkers (54.98%), never-smokers (61.78%), and moderate physical activity (43.12%).
Association between Inflammation and GMV and WMV
Higher circulating inflammatory indexes (CRP, SII, and NLR) were in strong association with greater atrophy in GMV and WMV (Supplementary Table 2 and Supplementary Figures 2–9). Specifically, CRP was significantly associated with atrophy in WMV (β= –0.04, 95% CI: –0.05 to –0.03, pFDR = 2.15 × 10-9) and 108 regional GMVs, which were mainly distributed in the cerebellum, temporal, and frontal lobes. For example, higher CRP levels were associated with GMV atrophy of the frontal pole (Left: β= –0.02, 95% CI: –0.03 to –0.01, pFDR = 9.62 × 10-5), inferior temporal gyrus (Left: β= –0.04, 95% CI: –0.05 to –0.03, pFDR = 8.64 × 10-9), and lobules X in the cerebellum (Left: β= –0.03, 95% CI: –0.04 to –0.02, pFDR = 2.59 × 10-6).
The results suggest that SII was associated with atrophy in WMV and 56 regional GMVs which were mainly distributed in the temporal, frontal, and occipital lobes. We observed significant associations of NLR with atrophy in 47 regional GMVs, which were mainly located in the frontal, occipital lobes, and cerebellum. These findings remain significant after adjusting for age, sex, ethnicity, alcohol intake, smoke status, BMI, physical activity, HbA1c, and deprivation index and correction for multiple testing.
Association of GMV and WMV with cognitive function
WMV and nearly all regional GMVs were in significant positive associations with cognitive function after correction for multiple testing (Supplementary Table 3), among which, the frontal pole (Left: β= 0.13, 95% CI: 0.12 to 0.15, pFDR = 1.82 × 10-75; Right: β= 0.14, 95% CI: 0.13 to 0.16, pFDR = 1.11 × 10-87), amygdala (Left: β= 0.13, 95% CI: 0.12 to 0.14, pFDR = 6.75 × 10-75; Right: β= 0.14, 95% CI: 0.13 to 0.16, pFDR = 1.81 × 10-90) and insular cortex (Left: β= 0.14, 95% CI: 0.13 to 0.15, pFDR = 1.94 × 10-90; Right: β= 0.14, 95% CI: 0.13 to 0.15, pFDR = 6.70 × 10-90) had the greatest associations seen for cognitive function. Therefore, we selected these regional GMVs as cognition-associated regions for the exploration of mediation analysis.
Mediation effect of GMV and WMV on the association between inflammatory indexes and cognitive function
On account of the fact that a higher level of inflammation was associated with poorer cognitive function both here (Supplementary Figure 1) and previously [2], we conducted single and multiple mediation analyses to quantify the level to which brain volume atrophy contributed to the general cognition decline associated with inflammation. The indirect effect of total GMV (β= –0.010, 95% boot CI: –0.014 to –0.005, p < 0.001) and WMV (β= –0.008, 95% boot CI: –0.012 to –0.005, p < 0.001) were statistically significant, which accounted for 22.7% and 18.2% of the total effect of CRP on general cognitive function respectively (Table 1 and Fig. 2). Similarly, GMV and WMV significantly mediated the association of SII and NLR with general cognition function in single mediation analysis. The total GMV of cognitive function-related regions significantly mediated the association of CRP with general cognitive function (β= –0.007, 95 % boot CI: –0.011 to –0.003, p < 0.001, mediation proportion: 16.3%) and association of SII with general cognitive function (β= –0.011, 95 % boot CI: –0.019 to –0.004, p < 0.01, mediation proportion: 16.9%).
Single-Mediator Models: Adjusted Direct Effect, Indirect Effect, Total Effect, and the Proportion of Mediation of brain volume for the Associations Between CRP and Cognitive Function
Analysis was adjusted for age, sex, ethnicity, alcohol consumption, physical activity, smoking, BMI, HbA1c, and deprivation index. *p < 0.05; **p < 0.01; ***p < 0.001.
In the multiple mediator models (Table 2 and Supplementary Figure 10), brain volume (total volume of grey matter and white matter) significantly mediated the association between CRP and general cognitive function (β= –0.009, mediation proportion: 20.9%). GMV showed a larger contribution to mediated effects than WMV in both single and multiple mediator models, which suggests GMW atrophy is more vulnerable to poor cognitive function related to inflammation.
Multiple Mediator Models (GMV and WMV): Adjusted Direct Effect, Mediation Effect, Total Effect, and the Proportion of Mediation for the Associations between CRP and Cognitive Function
Analysis was adjusted for age, sex, ethnicity, alcohol consumption, physical activity, smoking, BMI, HbA1c, and deprivation index. *p < 0.05; **p < 0.01; ***p < 0.001.
Sensitivity analyses
Sensitivity analysis revealed the mediation effect of GWV on statistically significant associations between inflammatory indexes and scores of single cognitive function tasks (Supplementary Table 4). Significant mediation effect appeared in the cognitive score of Numeric Memory Test, Fluid Intelligence Test, Matrix Pattern Completion, and Trail Making Test B, with a slightly larger mediation proportion for the association between CRP and Matrix Pattern Completion (β= –0.005, 95 % boot CI: –0.007 to –0.003, p < 0.001, mediation proportion 29.4%). Besides, the results of the moderated mediation analyses (Supplementary Table 5) showed that the interaction term CRP×anti-inflammatory drug use (β= 0.002, 95% boot CI: –0.006 to 0.010), CRP×age (β= 0.001, 95% boot CI: –0.040 to 0.042) were insignificant and interaction term CRP×sex (β= 0.008, 95% boot CI: 0.000 to 0.016) was slightly significant. Estimates for moderated mediation suggested that the mediation effect of GMV was independent of anti-inflammatory drug use and age. To further explore the modification effect of sex, the conditional indirect effect of CRP on cognitive function via GMW atrophy was estimated in both females and males. The significant mediated effect of GMV was slightly higher in males (β= –0.014, 95% boot CI: –0.020 to –0.008, p < 0.001) than in females (β= –0.006, 95% boot CI: –0.011 to –0.001, p < 0.001). The associations in sensitivity analyses including follow-up interval remain significant and similar to the main analysis (Supplementary Table 6). The results of model including education were significant (Supplementary Table 7). The association between brain volume and cognitive function was significant in participants in all education subgroups (Supplementary Table 8). The results after excluding participants with other neurological conditions were similar to results from main models (Supplementary Table 9).
DISCUSSION
Based on the large population-based UKB cohort, we found associations for peripheral inflammation across multiple outcomes including brain volume and cognition with adjustment for various covariates. Our results revealed that CRP exhibited robust and negative associations with cognitive function and brain volume, whereas the associations of SII and NLR with these outcomes were comparatively weaker. Elevated peripheral inflammation was also associated with brain volume atrophy, consequently resulting in a subsequent cognitive decline. Taken together, our findings showed that even minor increases in peripheral inflammation may have a significant impact on cognitive decline among midlife adults, and supported the role of brain volume atrophy in mediating cognitive decline attributed to elevated peripheral inflammation.
The role of inflammation in mechanisms for cognitive decline and brain atrophy
Consistent with previous studies of inflammation and cognition [2, 20], we also found that peripheral inflammation was linked to cognitive decline (Supplementary Figure 1), which indicates that inflammation is an important biological pathway underlying cognitive decline. Biological mechanisms such as epigenetic modifications, cellular senescence, metabolic dysfunction, aberrant autophagy, inflammation, vascular dysfunction and loss of blood-brain barrier integrity, and lipid dysregulation are distinguishingly involved in cognitive decline [21]. Among these, inflammation has been shown to interact with multiple biological processes [21] and further plays a role in accelerating neurodegenerative and cognitive decline.
The potential mechanisms underlying the adverse impact of inflammation on brain volume may be elucidated as follows. Elevated peripheral inflammation may penetrate the cerebral regions, eliciting a neuroinflammatory response that can instigate cellular necrosis, apoptosis, and synapse loss within these areas [22]. Furthermore, increased interaction of ischemic brain endothelium with inflammatory cells may lead to the dysfunction of the cerebral microvasculature and disruption of the blood-brain barrier, resulting in regional cerebral blood flow reduction [23, 24]. Moreover, neuroinflammation induced oxidative stress in the brain, which also subsequently exacerbated cellular death. [25]. Ultimately, this sequence of events may culminate in brain volume atrophy.
Peripheral inflammation-induced atrophy of regional brain volumes and its impact on cognitive functioning
In this study, we investigate the associations of inflammatory indexes with brain volume at a more granular level. In line with the findings of some previous studies [26, 27], we found that peripheral inflammation associated with a reduction of brain volume in nearly all brain regions. Nevertheless, the association between inflammation and regional GMV remains unclear due to inconsistent findings in the literature. For example, a prior study indicated that genetically predicted circulating biomarkers of immunity and inflammation are not correlated with hippocampal volume, further contributing to the ambiguity of this association [28].
Specifically, we observed that individuals with elevated CRP levels exhibited a notably higher degree of GMV atrophy in temporal fusiform cortex and the parahippocampal gyrus in comparison to other brain regions. The temporal fusiform cortex region, known as the occipitotemporal gyrus, located at the junction of the temporal and occipital lobes on the basal surface of the brain, is a critical brain structure for processing high-level visual information [29, 30]. The parahippocampal gyrus region, located at the junction between brain regions has been identified as being essential to memory formation and high-level visual processing [31]. In addition, notable atrophy in GMV was also found in the frontal pole, occipital pole, precentral gyrus, and postcentral gyrus. These identified regions are characterized by extensive interconnectivity with numerous other brain regions and are recognized for their notable involvement in various cognitive processes such as learning, problem-solving, decision-making, visual-cognitive abilities, and verbal working memory [32–34]. Previous research has established that synaptic loss and neural cell death are two basic biological mechanisms that have been linked to the association between brain atrophy and cognitive decline [35]. GMV atrophy in these brain regions attributed to elevated peripheral inflammation may potentially explain the association between inflammation and cognitive decline.
Brain atrophy as a mediator in the pathway from inflammation to cognitive decline
The findings from mediation analyses supported the role of brain volume atrophy in mediating cognitive decline attributed to elevated peripheral inflammation. These results remained robust after adjusting for potential confounders. Whereas numerous studies have investigated associations between inflammatory markers and reduced brain volume [27, 36], there has been a relative paucity of investigations that have examined the potential simultaneous associations between inflammation, brain volume, and cognitive decline. Conole et al. found a mediation effect of brain volume on the association between the DNA methylation signature of CRP and cognitive ability after adjusting for sex and age in the Lothian Birth Cohort 1936 [10]. Wersching et al. also found that CRP is associated with cerebral microstructural disintegration that predominantly affects frontal pathways and corresponding executive function [11]. However, no significant mediating effect of brain volume atrophy on the association between inflammation index in peripheral blood and cognitive decline was observed in the previous studies. By investigating cognitive decline across various cognitive domains and brain volume at a more granular level as well as utilizing a larger middle-aged sample, our study expands upon the findings of previous research.
The proportion of the mediating effect of GMV on inflammation-related cognitive decline was particularly noteworthy in the realm of non-verbal reasoning as evaluated by Matrix Pattern Completion. Non-verbal reasoning is the cognitive ability to examine and resolve problems using visual and spatial information, as opposed to linguistic or verbal means. The cognitive domain encompassing reasoning, logical thinking, and problem-solving, is underpinned by the activation of a network of frontal and parietal brain regions, notably the dorsolateral prefrontal cortex (DLPFC), superior parietal lobule, and intraparietal cortices [37, 38]. The observed disproportionate impact of inflammation on brain volume demonstrated in this study and prior research, may contribute to elucidating the differential mediating effect of GMV on the associations between inflammation and cognition.
Predictive effect of SII and NLR in cognitive decline and brain atrophy
In addition to CRP, both SII and NLR demonstrate negative associations with cognition and various regional brain volume in our study, underscoring their utility as reliable inflammatory predictors of brain volume atrophy and cognitive decline, which align with prior research [6, 39].
SII and NLR are composite measures of a series of inflammatory cells (such as platelets, neutrophils, and lymphocytes) to assess the balance between systemic inflammation and immune response [4]. Neutrophils involve in the immune response through various mechanisms, and their interactions with the neurovascular unit lead to endothelial dysfunction and subsequent disruptions in the blood-brain barrier and cerebral immune [40, 41]. Platelets play a role in regulating endothelial permeability and the recruitment of neutrophils and macrophages [42]. Lymphocytes are essential for immunological surveillance and defense, and their decline may indicate cellular immune injury [43]. Therefore, SII and NLR are comprehensive biomarkers for inflammation burden and process that merit further investigation in relation to brain volume and cognition.
Gender disparities in the mediating role of GMV atrophy
Sex exerts moderation over the mediating effect of GMV atrophy, as the results showed a more pronounced impact of inflammation on cognitive decline in males. Conclusions regarding sex differences in inflammatory response and cognition have not been consistent across studies. The possible mechanisms are as follows. Firstly, the peripheral immune cells, that participate in neuroinflammatory processes display notable sexual dimorphism, potentially due to differences in sex hormone receptors and peripheral steroid hormone levels [44, 45]. sex hormones, including estrogen and testosterone, have a major biological basis for cognitive decline [46], thus sex hormones fluctuations could influence inflammatory activity, potentially impacting brain volume and cognition. Furthermore, immune cells in the brain, such as microglia, a primary immune effector that respond to injury and infection and promotes inflammation resolution, exhibited sex difference in activity, number, and regulation [47].
Additionally, lifestyle factors such as smoking and alcohol intake could account for the sex differences, while healthier lifestyle was often associated with better cognition [48]. For example, a higher proportion of males reported being current or former smokers (male: 41.01%; female: 35.53%) in our study. Further research is needed to fully understand the mechanisms underlying these sex differences.
Strengths and limitations
The present study possessed several strengths. First, the study used data from the UK Biobank, a contemporary population-based cohort with extensive demographic, cognitive, inflammation, and brain imaging data. The exclusion of individuals with neurological conditions has been carefully implemented to reduce the risk of reverse causality. Furthermore, we have adjusted several variables in analyses to mitigate the confounding effects of covariates. A series of sensitivity analyses were also conducted to ensure the robustness of the findings. However, it is worth noting that there exist other potential covariates were not considered in our models. One limitation of the study is that the assessment of lifestyle factors relied on self-reported data, which may result in reporting biases. Another limitation is that peripheral inflammatory biomarkers were adopted instead of measurements from cerebrospinal fluid. Although the latter reflects the neuroinflammation more directly, it is impractical to collect in a large-scale population-based study. Despite excluding CRP > 10 mg/L and outliers, inflammation indexes measured at baseline still pose challenges in accurately representing an overall level of inflammation during the follow-up interval.
Conclusion
In conclusion, our findings support the hypothesis that elevated levels of peripheral inflammatory indexes were associated with cognitive decline via GMV and WMV atrophy. The results emphasized that inflammation is a vital risk factor for cognitive decline. Due to the absence of any proven treatment for forestalling or delaying dementia or mild cognitive impairment, and the notable side effects of existing pharmaceutical interventions, the systematic monitoring of peripheral inflammation and mitigation of excessive inflammatory burden are crucial for optimizing cognitive outcomes in the midlife individuals.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful to the UK Biobank participants who took part in this study and the UK Biobank research team members who collected, entered, and checked the data used in this article. This research has been conducted using the UK Biobank Resource under the project number of 69550.
FUNDING
This work was supported, in whole or in part, by the Bill & Melinda Gates Foundation [Grant Number: INV-016826]. Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data analyzed in this study are not publicly available as it contains data that could compromise participant consent and confidentiality, but can be requested via a data access request to the UK Biobank.