
Abstract
Background:
Hypertension has been identified as a risk factor of dementia, but most randomized trials did not show efficacy in reducing the risk of dementia. Midlife hypertension may be a target for intervention, but it is infeasible to conduct a trial initiating antihypertensive medication from midlife till dementia occurs late life.
Objective:
We aimed to emulate a target trial to estimate the effectiveness of initiating antihypertensive medication from midlife on reducing incident dementia using observational data.
Methods:
The Health and Retirement Study from 1996 to 2018 was used to emulate a target trial among non-institutional dementia-free subjects aged 45 to 65 years. Dementia status was determined using algorithm based on cognitive tests. Individuals were assigned to initiating antihypertensive medication or not, based on the self-reported use of antihypertensive medication at baseline in 1996. Observational analog of intention-to-treat and per-protocol effects were conducted. Pooled logistic regression models with inverse-probability of treatment and censoring weighting using logistic regression models were applied, and risk ratios (RRs) were calculated, with 200 bootstrapping conducted for the 95% confidence intervals (CIs).
Results:
A total of 2,375 subjects were included in the analysis. After 22 years of follow-up, initiating antihypertensive medication reduced incident dementia by 22% (RR = 0.78, 95% CI: 0.63, 0.99). No significant reduction of incident dementia was observed with sustained use of antihypertensive medication.
Conclusion:
Initiating antihypertensive medication from midlife may be beneficial for reducing incident dementia in late life. Future studies are warranted to estimate the effectiveness using large samples with improved clinical measurements.
Keywords
INTRODUCTION
Midlife hypertension has been identified as one of the most important modifiable risk factors of dementia [1]. Evidence from prospective cohort studies has indicated that high blood pressure in midlife is associated with a higher risk of cognitive decline and dementia [2–5]. It is therefore hypothesized that reducing blood pressure in midlife may prevent incident dementia in populations entering late life. Although findings from observational studies showed that use of antihypertensive medication, the major approach to reducing blood pressure, is associated with a lower risk of dementia [6], such treatment effect has been rarely demostrated in randomized controlled trials (RCTs), which would provide a higher level of evidence by design and principle. In a recently published systematic review and meta-analysis [7], although it concluded that antihypertensive medication use is significantly associated with a lower risk of incident dementia, only one out of twelve RCTs showed significant results [8], while none of the other RCTs showed a significant reduction in risk of dementia from antihypertensive medication use [9–14].
Efforts have been made to explain the gap in contradictory findings between RCTs and observational studies. One of the potential explanations is that while high blood pressure in midlife is associated with a higher risk of dementia, high blood pressure in late life does not predict the risk of dementia well, as is documented in the existing literature [15–20]. Cohort studies have found that antihypertensive medication is associated with a lower risk of incident dementia among older adults. However, there is potential for confounding due to the possibility that antihypertensive medication was initiated in earlier stages of life. In addition, in observational studies, other factors that affect medication use and dementia risk may not be fully adjusted in the analysis. Therefore, initiating systolic blood pressure in late life may not lead to a lower risk of dementia. However, except for the SPRINT-MIND trial (Systolic Blood Pressure Intervention Trial - Memory and Cognition in Decreased Hypertension), which includes participants 50 years or older, all existing RCTs of antihypertensive medication on incident dementia are based on older adults. Thus, since midlife high blood pressure is more predictive of incident dementia, the target for intervention should be on blood pressure in midlife.
Ideally, an RCT should be conducted to estimate the long-term effectiveness of antihypertensive medication use in midlife on the prevention of dementia in late life. However, it would not be feasible, if not impossible in practice to enroll participants in midlife into a trial that lasts for decades. Moreover, given the huge burden of public health brought by dementia, it is not appropriate to spend decades for the results of a potential trial with numerous decision to be made during this long period of time. Given the fact that no existing trial started an intervention of antihypertensive medication use from midlife, evidence from such RCTs is unlikely to emerge in near future. Under such circumstances, the optimal way to draw a causal conclusion on the effect of antihypertensive medication use for preventing incident dementia in late life is to emulate a target trial with existing observational studies, in which causal questions are specified, and observational data is analyzed like RCTs.
Therefore, we aimed to use a prospective cohort study to emulate a target trial and estimate the effectiveness of initiation and sustained use of antihypertensive medication from midlife among hypertensive patients on preventing incident dementia in late life.
MATERIALS AND METHODS
Target trial emulation
Target trial emulation is a method for designing and analyzing observational data to simulate the condition of an RCT, when an RCT is not feasible or ethical. The process of a target trial emulation includes two steps. The first step is to pose a causal question, and specify necessary elements for causal estimation, including eligibility criteria, treatment strategies and assignment, outcomes of interest, the start and end of follow-up, causal contrasts, and analysis plan. The second step is to emulate the components of that protocol using observational data [21, 22]. In the target trial emulation, appropriate methods need to be applied to ensure conditional exchangeability, and correct specification of the time-zero point. The validity of target trial emulation has been confirmed through the recovery of estimates from existing RCTs [23, 24].
Study population
To emulate the target trial, we used data from the Health and Retirement Study (HRS) [25]. The HRS is a nationally representative, longitudinal study of adults who are 51 years or older and their spouses starting from 1992 [26]. Participants have completed questionnaires every two years. The Wave 3 (1996) of HRS was set as the baseline of our study, and we used the data from Wave 3 (1996) to Wave 14 (2018) for analysis. All study participants provided informed written consent, and participants were de-identified in the dataset for statistical analysis.
Information on antihyertensive medication use was obtained via self-report, with the question “In order to lower your blood pressure, are you now taking any medication” among participants who claimed to have hypertension by answering “Yes” to the question “Has a doctor ever told you that you have high blood pressure or hypertension”.
Dementia status for HRS participants at each wave was determined using Langa-Weir Classification of Cognitive Function [27], based on a 27-point scale that included tests of immediate and delayed word recall, a serial sevens subtraction test for working memory, and a counting backwards test for processing speed. Cognitive status was categorized as “demented” with a score between 0 and 6. The status of “demented” was considered having dementia. The Langa-Weir Classification of Cognitive Function was validated against neuropsychiatric interview in the Aging, Demographics and Memory Study, and demonstrated an accuracy of 87% (95% CI: 83%, 91%) in the classification of dementia and has been widely used in prior research [28].
In addition to the key variables for the emulated target trial, additional variables were collected in the HRS through questionnaire and were included as covariates in our regression analysis, including age (in years), sex (men, women), race (White/Caucasian, Black/African American, other), education (below high school, high school graduate or equivalent, at least some college), smoking status (never, former, current), physical activity (≥3 vigorous physical activity per week or not), depressive symptoms (yes/no, based on having at least 4 self-reported depressive symptoms or not), body mass index (kg/m2), prevalent diabetes (yes/no), heart disease (yes/no), and stroke (yes/no).
Target trial design and specification
The design of the target trial and its emulation were described below and in Table 1.
Specifying the emulated target trial for midlife adults using observational data
Eligibility criteria
Non-institutional living individuals who are 45 to 65 years old with hypertension and normal cognition, free of cancer, as well as no use antihypertensive medication use in the previous 2 years.
Treatment strategies and assignments
Individuals included in the target trial are randomly assigned to one of the strategies, including initiating and not initiating antihypertensive medication.
Outcome of interest
The outcome of the target trial is incident dementia during 22 years of follow-up.
Start and end of follow-up
Each individual included in the target trial is followed when the individual meets the eligibility criteria, and all of the participants are followed until the occurrence of incident dementia, death, or the end of follow-up, whichever occurs first.
Causal contrast of interest
Intention-to-treat effect and per-protocol effect.
Analysis plan
Intention-to-treat analysis. We will fit pooled logistic regression models to predict the cumulative 22-year risk of dementia in both intervention group and control group.
Per-protocol analysis. Individuals will be artificially censored if they deviate from their assigned strategy of intervention. Specifically, individuals who are assigned to sustained antihypertensive medication use will be censored if they deviate from antihypertensive medication use at the next wave, and individuals who are assigned to not initiating antihypertensive medication use will be censored if they initiate antihypertensive medication use at the next wave. We will fit the pooled logistic regression model weighted with stablized time-varying inverse-probability of censoring weights (IPCW) based on covariates.
Emulation of target trial
Eligibility criteria
We included noninstitutional individuals aged 45 to 65 years old who reported having hypertension in the HRS cohort, who were cognitively normal at the baseline (1996), and who did not use antihypertensive medication two years prior to baseline. We also excluded participants living in nursing home, and those who had missing important demographic information, including race and education levels, as well as participants with cancer, which may affect survival of participants. We additionally excluded participants without complete sets of covariates for analysis.
Treatment strategies and assignment
Those who newly used antihypertensive medication at baseline were considered as being in the intervention group, and those who never used antihypertensive medication were at baseline considered as being in the control group. The assignment of treatment strategies was randomized by adjusted for baseline covariates.
Outcome of interest
The outcome of the emulated target trial was incident dementia based on Langa-Weir Classification of Cognitive Function in the HRS during 22 years of follow-up.
Start and end of follow-up
The start of follow-up for each individual was 1996. We followed participants forward in time until a diagnosis of dementia, death, drop-out, or the end of follow-up (Wave 14 (2018)), whichever occurred first.
Causal contrast of interest
Observational analog of intention-to-treat and per-protocol effect.
Analysis plan
Observational analog of intention-to-treat analysis. We fit the pooled logistic regression model weighted with stablized inverse-probability of treatment weights (IPTW) and IPCW based on the joint distribution of baseline covariates, including baseline age, sex, race, education, body mass index, smoking, physical activity depressive symptoms, prevalent hypertension, and prevalent diabetes to calculate the cumulative incidence of dementia in the intervention group and control group, respectively [29].
Observational analog of per-protocol analysis. Individuals were artificially censored if they deviated from their assigned strategy of intervention. Specifically, individuals assigned to initiation and sustained antihypertensive medication use were censored if they deviated from antihypertensive medication use at the next wave, and individuals who were assigned to not initiating antihypertensive medication use were censored if they initiated antihypertensive medication use at the next wave. To account for attrition due to loss to follow-up, time-varying stablized inverse-probability of censoring weights were created based on time-fixed variables at baseline (baseline age, sex, race, education) and time-varying covariates (smoking, physical activity, body mass index, depressive symptoms, hypertension, diabetes, heart disease, stroke, cancer) at each wave. We fit the pooled logistic regression model weighted with stablized inverse-probability of treatment baseline covariates and stablized time-varying inverse-probability censoring weights to calculate the cumulative incidence of dementia in the intervention group and control group, respectively. Death was considered a censoring event in the analysis [30], which assumed death was independent of risk factors for dementia.
Statistical analysis
Descriptive analysis was conducted using T-test and Chi-square test for baseline characteristics by assigned groups (initiators versus noninitiators) in the emulated target trial. The results of effectiveness were analyzed at every two years during follow-up. The estimated risk ratios (RRs) were calculated based on the cumulative incidence of dementia estimated by pooled logistic regression models with the steps above. The 95% confidence intervals (CIs) were obtained through percentile-based bootstrapping with 200 resamples. The results were considered statistically significant if the 95% confidence interval did not include 1.
For sensitivity analysis, we conducted a target trial with the same procedures as above and used the composite outcome of dementia and death, and evaluate whether the results differed from the primary analysis.
All analysis was conducted using SAS 9.4 (SAS Institute, Cary, NC).
RESULTS
A total of 2,375 subjects were included in the emulated target trial after applying all inclusion and exclusion criteria (Supplementary Figure 1), with 1,882 initiators and 493 noninitiators. The baseline characteristics of the participants in the emulated target trial were shown in Table 2. The initiators had a higher proportion of female participants, higher prevalence of diabetes, heart disease, and stroke. With application of IPTW and IPCW, the variables were balanced between two groups in the emulated target trial.
Baseline characteristics of participants in the emulated target trial in HRSa
aThe bold parts indicated statistically significant differences between groups.
In the emulated target trial, during 22-year (mean: 14.1±7.5) follow-up period, a total of 309 (13.0%) dementia cases occurred. With adjustment for all covariates and weighted by IPTW and IPCW, by the end of 22-year follow-up, the risk of incident dementia was 23.0% and 29.4% among initiators and non-initiators, respectively. The initiation of antihypertensive medication showed a significant effect in reducing incident dementia after 18 years of follow-up (RR = 0.70, 95% CI: 0.51, 1.00). At the end of the follow-up period, initiating antihypertensive medication was found to reduce the risk of incident dementia by 22% (RR = 0.78, 95% CI: 0.63, 0.99) (Fig. 1, Table 3).
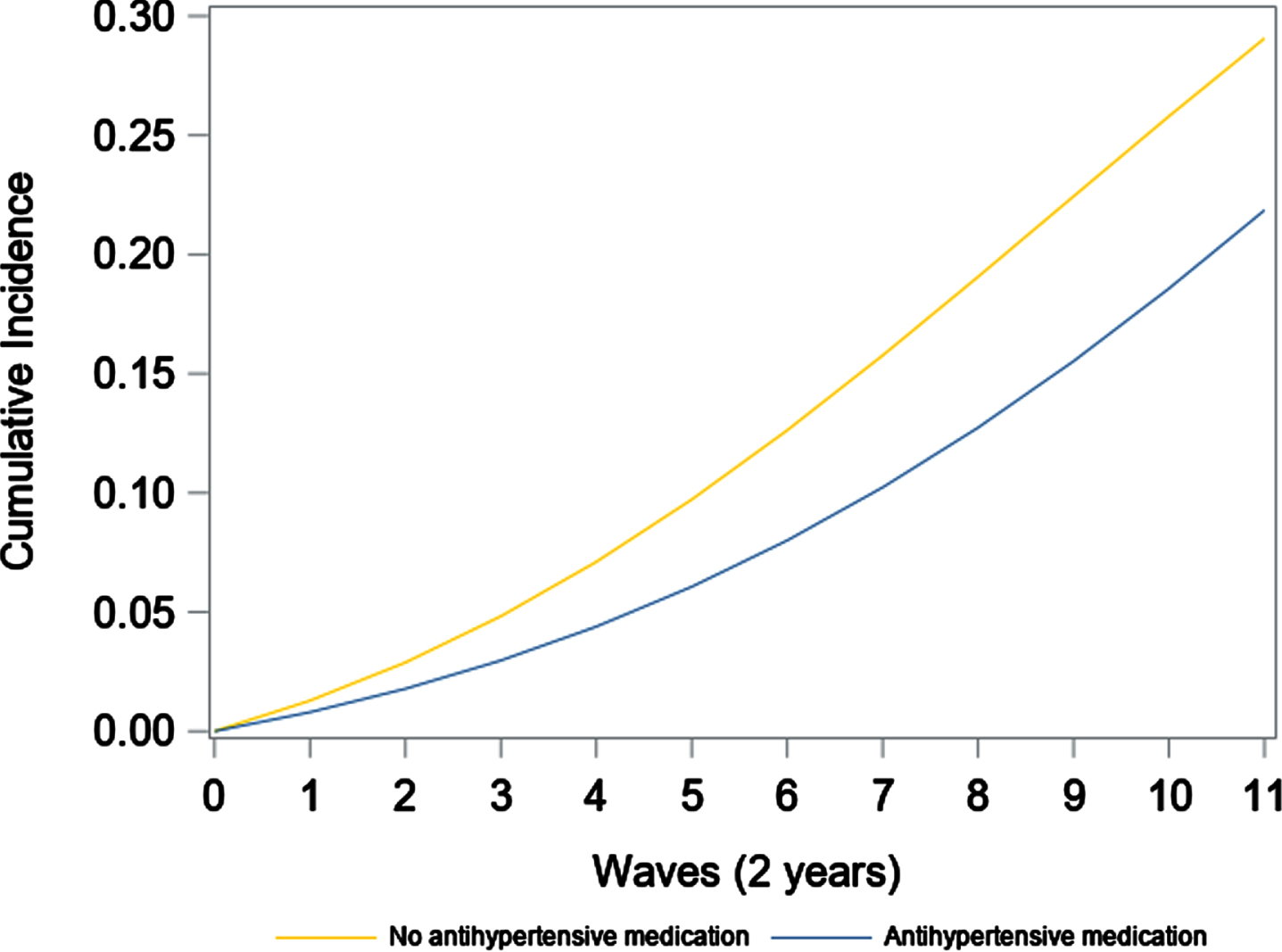
Estimated cumulative incidence of dementia among participants who initiated antihypertensive medication and not initiated antihypertensive medication in the emulated target trial using pooled logistic regression models. The models were weighted for inverse-probability treatment weight and inverse-probability censoring weight based on baseline covariates, including age, sex, race, education, smoking status, physical activity, depressive symptoms, body mass index, prevalent diabetes, heart disease, and stroke.
The estimated risk ratios of initiating antihypertensive medication from midlife on incident dementia during 22 years of follow-upa
a95% confidence intervals were calculated with 200 sets of bootstrapping. The bold parts indicated statistically significant differences between groups.
After censoring participants as they deviated from the initial assignment of treatment at baseline, the estimated cumulative incidence of dementia estimated by pooled logistic regression models with IPTW and IPCW by the end of 22-year follow-up was 22.3% and 28.3% among sustained use of antihypertensive medication and persistent non-initiators, respectively. However, no significant effect was shown with adherence to antihypertensive medication on reducing incident dementia (Fig. 2, Table 4).
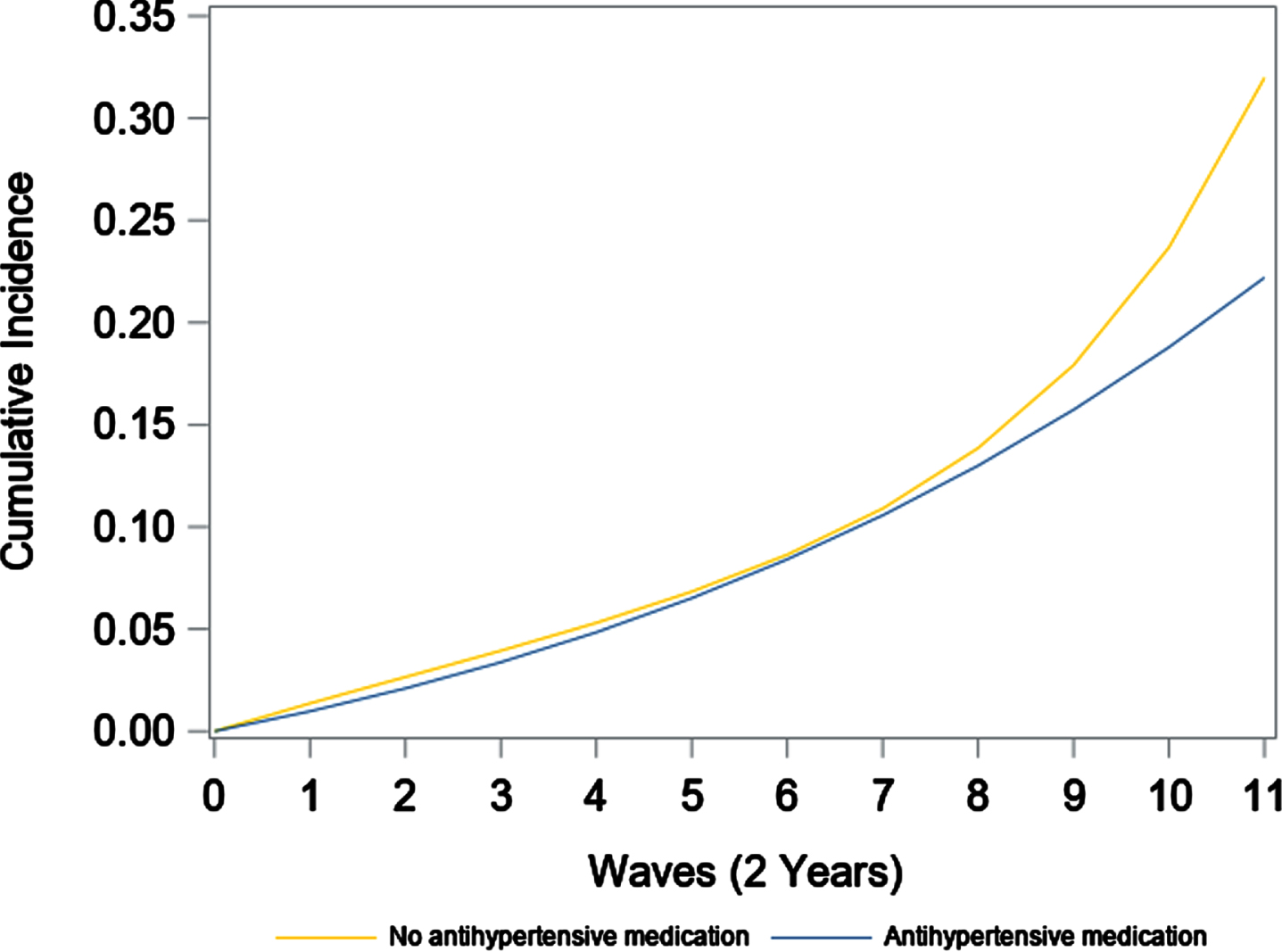
Estimated cumulative incidence of dementia among participants who had sustained use of antihypertensive medication and those who never initiated antihypertensive medication in the emulated target trial using pooled logistic regression models. The models were weighted for inverse-probability treatment weight (base on baseline covariates) and inverse-probability censoring weight (based on baseline covariates (including age, sex, race, education, body mass index, smoking, depressive symptoms, physical activity, prevalent diabetes, heart disease, stroke) and time-varying covariates (smoking status, physical activity, depressive symptoms, body mass index, prevalent diabetes, heart disease, and stroke)).
The estimated risk ratios of sustained use of antihypertensive medication initiated from midlife on incident dementia during 22 years of follow-upa
a95% confidence intervals were calculated with 200 sets of bootstrapping. The bold parts indicated statistically significant differences between groups.
For sensitivity, initiating antihypertensive medication use reduced the risk of dementia and death after 22 years of follow-up (RR = 0.90, 95% CI: 0.83, 0.97) (Supplementary Figure 2, Supplementary Table 1), and no significant reduction was found for sustained antihypertensive medication use on dementia and death (Supplementary Figure 3, Supplementary Table 2).
DISCUSSION
In an emulated target trial of antihypertensive medication use on reducing incident dementia starting from midlife, using the new-user design and application of IPTW and IPCW, we found that individuals with hypertension those who initiated antihypertensive medication use had a lower risk of dementia compared with those who did not, while we did not find effectiveness for sustained antihypertensive medication use on reduction of incident dementia.
In addition to multiple RCTs, previous efforts have been taken to draw a causal relationship between initiation of antihypertensive medication use and incident dementia using emulated target trials. Using the Rotterdam Study, Rojas-Saunero et al. studied the effects of hypothetical interventions on systolic blood pressure to reduce dementia with 15 years of follow-up [31]. The study defined multiple strategies for blood pressure reduction, including maintaining systolic blood pressure below 120 mmHg, and maintaining systolic blood pressure below 140 mmHg. However, compared to the natural course, blood pressure reduction did not achieve a reduction of incident dementia. There are several reasons that may explain the null results. First of all, consistency is an important issue, since the cause for different levels of blood pressure reduction is unknown, and a lower blood pressure may be achieved due to pathological (but unmeasured) reasons, such as hypotension. Improvement of lifestyle factors (e.g., physical activity, healthy diet) also reduces blood pressure levels. Therefore, there could be different multiple versions of treatment in the same group of people with the same level of blood pressure reduction. In the presence of multiple versions of treatments in the same group, there could be unmeasured confounders between the treated blood pressure during follow-up and incident dementia, and when the follow-up dementia is controlled, then the unmeasured confounder can bias the relationship between blood pressure reduction and incident dementia, which is known as collider bias [32, 33]. Also, all the participants included in the analysis were 65 years or older, and as is indicated in the literature, high blood pressure in late life may not be predictive of incident dementia, and late treatment of blood pressure may have missed the optimal time for prevention of dementia [15, 16]. In addition, residual confounding may still exist after adjustment for all covariates. Given these potential reasons, we selected midlife individuals younger than 65 years as the start of intervention for antihypertensive medication, and we specified the means of intervention at baseline instead of blood pressure change during follow-up time. Based on an emulated target trial using a cohort study design, our results suggested a causal relationship between early initiation of antihypertensive medication use and a reduction of incident dementia.
The different findings between observational studies and RCTs could be attributed to different features of their study designs for prevention of Alzheimer’s disease and related dementias, such as the eligibility criteria and sample composition, length of follow-up time, and treatment conditions [34]. The participants included in an RCT are highly selective, while there are few restrictions on observational studies. Also, due to the feasibility, the length of intervention in an RCT is usually shorter than 5 years, while it is common for observational studies to last for decades. In addition, treatment arms are randomly assigned to different groups, while the exposure in observational studies may be related to intrinsic characteristics of the groups of populations, which may remain after adjustment for covariates. All these differences do not only form the different definitions of the study designs, but also the different results and their interpretations. Taking the advantage of the large sample size and a long follow-up period of a cohort study, as well as methods of causal inference, we were able to estimate the effect of long-term intervention without the issue of limited feasibility. Admittedly, while the emulated target trial is a compromised way of conducting a real RCT, it does suggest a causal relationship, which answers a question of “Will the risk of dementia in late life be reduced if individuals with hypertension start to take antihypertensive medication from midlife” that can hardly be answered in an actual trial.
Different from the results of initiating antihypertensive medication on reducing the risk of incident dementia, our study did not show effectiveness for adhering to antihypertensive medication use on reduction of incident dementia. The different results between point and sustained effectiveness may suggest that the importance of antihypertensive medication in midlife, while use of antihypertensive medication in a later phase may not be as important as that in midlife. This is consistent with results from previous observational studies and RCTs. However, it did not necessarily mean there was no effectiveness of adherence to antihypertensive medication use on dementia, since the sample size may not be large enough to observe per-protocol effect, which can be reflected from the wide confidence intervals. This calls for future studies to estimate the effectiveness using large clinical datasets.
Our study has important clinical and public health significance. Using the causal inference methods, we were able to provide a causal relationship between antihypertensive medication use from midlife and prevention of incident dementia. This is consistent with our hypothesis that intervention on blood pressure reduction in midlife, instead of in late life, may be an effective way to prevent incident dementia. This also emphasizes the importance of midlife blood pressure in predicting a high risk of incident dementia in late life, as well as an early intervention on high blood pressure to prevent dementia. As is reflected in the effect sizes of these two emulated target trials, initiating antihypertensive medication use at an earlier stage of life could achieve much greater risk reduction on incident dementia. Also, with the use of antihypertensive medication, both cardiovascular and cognitive health will be improved among hypertensive patients, which may potentially increase the motivation of early initiation of antihypertensive medication and healthy lifestyle.
Limitations
Our study is subject to several limitations. First, the information on hypertension and antihypertensive medication use is based on self-report, which may suffer from misclassification. The specific pharmacological classes of antihypertensive medication were unknown, and literature has shown that different classes of antihypertensive medication showed different relationships with incident dementia, for example calcium channel blockers and angiotensin II receptor blockers are associated with lower risk of dementia [35]. Also, the algorithm of dementia is not the actual formal diagnosis of dementia, and the exams were not conducted in person and the cognitive assessment was not comprehensive. Furthermore, there are several variables related to incident dementia but not included in (or some waves of) the HRS, such as dietary intake, blood pressure, and biomarkers, which may lead to unmeasured confounding. In addition, the sample size of this study may not be large enough to detect effects in per-protocol analysis in different subgroups, such as those defined by sex and APOE ɛ4 carrier status (which was only available for a subsample of HRS). Future studies with larger sample sizes are needed to estimate the effects of antihypertensive medication initiation in these subgroups.
Despite these limitations, we used the new-user design and adequately adjusted for covariates available in the HRS, which could form the causal relationship between initiating antihypertensive medication use and prevention of incident dementia. Future studies are expected to take advantage of large sample size with accurate and detailed information of antihypertensive medication use and diagnosis of dementia to study the effectiveness of antihypertensive medication on reduction of incident dementia.
Conclusion
In conclusion, initiating antihypertensive medication from midlife may be beneficial for reducing incident dementia in late life. Future studies are warranted to estimate the effectiveness using large sample with accurate measurement of antihypertensive medication use and dementia diagnosis.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledments to report.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The HRS (Health and Retirement Study) is sponsored by the National Institute on Aging (grant number NIA U01AG009740) and is conducted by the University of Michigan.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.