
Abstract
Background:
Subjective memory complaints (SMC) are commonly studied in older adults and have been identified as potentially prodromal to dementia and Alzheimer’s disease. Studies among younger adults from South America are lacking.
Objective:
To estimate the prevalence of SMC and the factors associated with it among Maule Cohort (MAUCO) participants.
Methods:
We performed a cross-sectional analysis to estimate the prevalence of SMC and investigated its associated factors from MAUCO baseline data (N = 6,687). Within groups defined by age (38–59, 60–74) and global cognition (Mini-Mental State Examination: ≥26, 25-22, ≤21), multinomial logistic regression models evaluated risk factors for SMC (Yes, Sometimes, No).
Results:
Overall, SMC prevalence was 16.4%; 15.9% (95% CI 14.9–16.9%) among younger and 17.6% (15.8–19.4%) among older participants. Female sex, comorbidities, and bad/fair self-reported health status (SRHS) were generally associated with higher odds of SMC.
Conclusion:
Overall prevalence of SMC was 16%. Different factors were associated with the odds of SMC depending on age and global cognitive status. Future SMC studies should include sex-specific assessments, evaluate SRHS as a moderator of SMC reporting, and the influence of the SARS-CoV-2 pandemic on SMC reporting.
INTRODUCTION
Subjective memory complaints (SMC), defined as the subjective awareness of memory loss [1, 2], are common in later life and have been associated with increased risk of cognitive impairment and dementia [3–7], and it has been suggested that SMC is a prodrome of dementia [5, 9]. In addition to the association with cognitive decline, later-life SMC is also reported to be associated with the risk of falls as well as impaired activities of daily living [10]. Further, with the arrival of the SARS-Cov-2 pandemic, an increase in SMC is expected. It has been established that more than 50% of patients with severe COVID-19 experience persistent neurological symptoms (“Long-Covid”), where subjective cognitive complaints (e.g., attention and memory) are central [11, 12]. The prevalence of late-life SMC is estimated to be between 25–50% globally, although data from South America are limited [8, 13–16].
Several risk factors have been associated with later-life SMC, and many of these are also associated with cognitive impairment and dementia. These include demographic factors like sex [1, 17], age [14, 18], education [14, 17], and smoking status [17]. Numerous health conditions are also reported to be associated with SMC, such as diabetes [14, 17], pain [14], impaired vision and hearing [14], stroke [14], cardiovascular or respiratory disease [14], chronic constipation [14], arthritis [14], sleep problems [18], polypharmacy [14], and multimorbidity [13]. Many studies have reported that SMC is associated with depression or depressive symptoms [2, 19–21], anxiety [2, 22], and psychological distress [17].
Additionally, poor self-perceived health has also been associated with SMC [14].
While SMC has been heavily studied in older adults, literature regarding risk factors for SMC among younger adult populations is scarce. Among Australian research volunteers ages 45 to 64, psychological distress and some cardiovascular factors were associated with higher odds of SMC [17].
The Maule Cohort (MAUCO) [23] is a Chilean population-based study of middle-aged and older adults (N = 8762 by December 2020). In the current study, using data collected prior to the SARS-Cov-2 pandemic, we estimated the baseline prevalence of SMC among MAUCO participants presumed to be free from dementia within two age groups: 38–59, and 60–74 years old. Patients were presumed to be free from dementia if they reported not having received a dementia diagnosis. Additionally, we aimed to estimate the association of potential risk factors with reports of SMC in both age groups.
METHODS
Participants
The present study is a cross-sectional analysis of the baseline evaluation performed on the Maule Cohort (MAUCO) participants. MAUCO is a prospective cohort from Molina, Chile, designed to study the natural history of chronic diseases [23]. The cohort comprises Molina inhabitants, aged 38 to 74 years old at study entrance (“baseline”), between December 2014 and March 2019. Potential volunteers who were unable to give informed consent autonomously or who have a terminal illness were not eligible for the cohort. According to the 2017 census, Molina had a population of 45,976 inhabitants, with 19,468 in the recruiting ages [23]. Additional details about the cohort have been published previously [23, 24].
The study protocol was approved by Ethics Committees at Pontificia Universidad Católica de Chile (N° 14–141) and the Maule Regional Service of the Chilean Ministry of Health [23]. Informed consent was obtained from all participants in the Maule cohort.
Objective cognitive function
Objective measurement of memory and cognitive function was performed using Addenbrooke’s Cognitive Examination-Revised (ACE-R), adapted for the Chilean population [25]. ACE-R has been shown to have greater sensitivity and predictive value to detect dementia than the Mini-Mental State Examination (MMSE) [26]. ACE-R scoring ranges from 0 to 100, which is the maximum score [25]. However, the ACE-R also incorporates the MMSE, which comprises seven subsections— temporal orientation, spatial orientation, registration, attention, recall, language, and copying. Because the overall score from the ACE-R was missing for a large number of participants (N = 1,350), we focused on the MMSE as the primary measure of global cognition. The memory and fluency modules from the ACE-R were incorporated as secondary measures of objective cognitive function.
In the current study, we excluded participants who did not have data for more than 4 domain sections of the MMSE (n = 29); who declared knowing neither how to write nor read; or declared only knowing how to write or only knowing how to read (n = 618), leaving 8,105 participants for analysis. To facilitate analysis, MMSE score was operationalized as greater than 26, between 26 and 22, and 21 or less, corresponding to normal cognition, mild cognitive impairment, and possible dementia, respectively. The cut-off scores were selected based on what has been previously validated and used for the MMSE in the Chilean population [27, 28].
Finally, we excluded those participants that did not answer the question related with medication use, leaving a final sample for analysis of 6,687 participants.
Stratification by MMSE was performed to control for potential associations between SMC and the scores of the cognitive evaluations, as some research has reported [29].
Subjective memory complaint
SMC was determined by the question “Does your memory fail frequently, or do you forget events, even recent, or some appointments?”[30] Participants could answer with “yes,” “sometimes,” and “no.” These categories were retained for analysis, although only “yes” responses were considered to indicate SMC for prevalence calculations.
Risk factors
Risk factors selected for study and their operationalization in the analysis are described below. These factors were selected for study based on previous literature. Given the expected increases in SMC prevalence with older age, and the potential for age-group-specific risk factors, risk factor analyses were performed within age strata (38–59 and 60–74). The full set of risk factors was evaluated within each age group.
Demographic and behavioral
Demographic factors were age (continuous variable), sex (categorical variable, female/male), and education (≤8 years, 9 to 12 years, and more than 12 years). Smoking behavior was categorized as current, former, or never smoker.
Medical
Medical conditions, which were reported by the participant, were operationalized as present/absent unless otherwise indicated. The selected factors included self-reported health (Excellent, Very Good, Good, Fair, and Bad; Excellent/Very Good were collapsed for analysis); arthritis; hypothyroidism; diabetes; dyslipidemia; hypertension; and respiratory disease (considered present if any of the following were present: asthma, chronic obstructive pulmonary disease (COPD), emphysema, or other chronic respiratory diseases reported by the participant). Depression, diabetes, hypertension, and dyslipidemia were considered present if the participant reported having been diagnosed or was currently using pharmacotherapy for any of these conditions. Furthermore, body mass index (BMI; dichotomized at ≥30 kg/m2) was calculated from the weight and height measurements taken at the interview.
In addition to individual health conditions, we considered multimorbidity, which was operationalized as the number of the following conditions present (total possible score from 0 to 21 comorbidities): diabetes, hypertension, myocardial infarction, stroke, heart failure, other chronic cardiac conditions, chronic kidney disease, other chronic renal conditions, arthritis, intestinal inflammation, other chronic digestive diseases, hypothyroidism, COPD, asthma, emphysema, other chronic respiratory conditions, Parkinson’s disease, other chronic neurological diseases, cancer, and depression. In the case of those conditions that fall under the “other” category, the presence of any number of conditions in that category, only adds 1 to the multimorbidity score.
Medication use
Polypharmacy was defined as the concomitant use of 5 or more medications [31, 32]. Medications were counted as individual active ingredients, thus if a participant was using a medication with two active ingredients, it would add two to their total medications. Also, indicator variables were created to register the use of benzodiazepines, antihypertensives, antidepressants, and lipid-lowering medications (yes/no) as they have been previously associated with memory [33–36].
Statistical analysis
SMC category prevalence (Yes, Sometimes, No) was estimated by age group, MMSE stratum, sex, and overall. Descriptive group comparisons were performed using chi-square or analysis of variance (ANOVA).
To determine factors associated with SMC response, we fit multinomial logistic regression models to the data, with ‘No SMC’ as the reference group. First, we fit a model with all the variables including a variable for age group (38–59 or 60–74), a categorical variable for the MMSE score (<26, 26 to ≤21, and <21), and an interaction term between both. Then, using an exploratory modeling framework (that is, to identify patterns and generate hypotheses rather than focus on hypothesis testing [37]), we fit multinomial regression models including all the covariates (full model) for each age and MMSE score category stratum, and then a modified backward variable selection and AIC were used to select the model with the best fit. In addition to the factors associated with SMC, participant scores on the ACE-R memory and fluency sections were included as control variables to account for within-stratum cognitive heterogeneity. Only complete cases were included in the regression analysis; 44 participants were dropped for incomplete data.
As a sensitivity analysis, taking into consideration the robust association between depression and SMC and their potential biological link, and as depression has been described as reducing patients’ cognitive resources, the described regression analysis was repeated on a restricted cohort, excluding those participants with self-reported depression. All analyses were conducted using SAS 9.4®.
RESULTS
Sample characteristics
There were 4,962 MAUCO participants aged 38–59 and 1,725 aged 60–74 years included in this study; most participants were female (56%), with ≤8 or 9–12 years of education (44% and 43%, respectively), and reported fair health (46%) (Table 1).
For both age groups, the most common response to the memory complaint question was “Sometimes”, which accounted for 49% of the 38–59 group, and 55% of the 60–74 group. Prevalence of endorsed SMC (Response = “Yes”) was about 16% among all participants included in the analysis and was slightly lower in the 38–59 (15.9% : 95% CI 14.9–16.9%) versus the 60–74 years group (17.6% : 95% CI 15.8–19.4%) (Table 1). Denial of SMC (Response = “No”) was significantly higher among the younger versus the older group (34.9% : 95% CI 33.6–36.3% versus 26.9% : 95% CI 24.8–29.0%) SMC endorsement was significantly higher among people with fewer years of schooling, and in those who reported fair or bad health (Table 1).
MAUCO prevalence of SMC stratified by age and SMC status. Numbers are %, or mean±SD
aSelf-reported diagnosis, or using a treatment for the condition; b2,065 missing values; cMaximum score = 30; dMaximum score = 26; emaximum score = 7, list words starting with letter “P”; fMaximum Score = 7, list animals. p-values are for comparison between SMC by age group using t test or χ2 as needed. †p-value <0.05; ‡p-value <0.0001.
When evaluating the prevalence of SMC by sex, we observed that SMC was commonly reported by women, regardless of age group (21.2% and 21.1% for young and older women) (Table 1 and Fig. 1). For male participants, SMC prevalence was higher among the older participants (8.9% and 13.6% for younger and older men) but was strikingly lower than the reported prevalence among women (Table 1 and Fig. 1). Denial of SMC was also most common among male participants, accounting for 47.2% of men in the younger group and 35.7% in the older group. Only 25.7% of women in the younger group and 19.4% in the older group denied SMC.
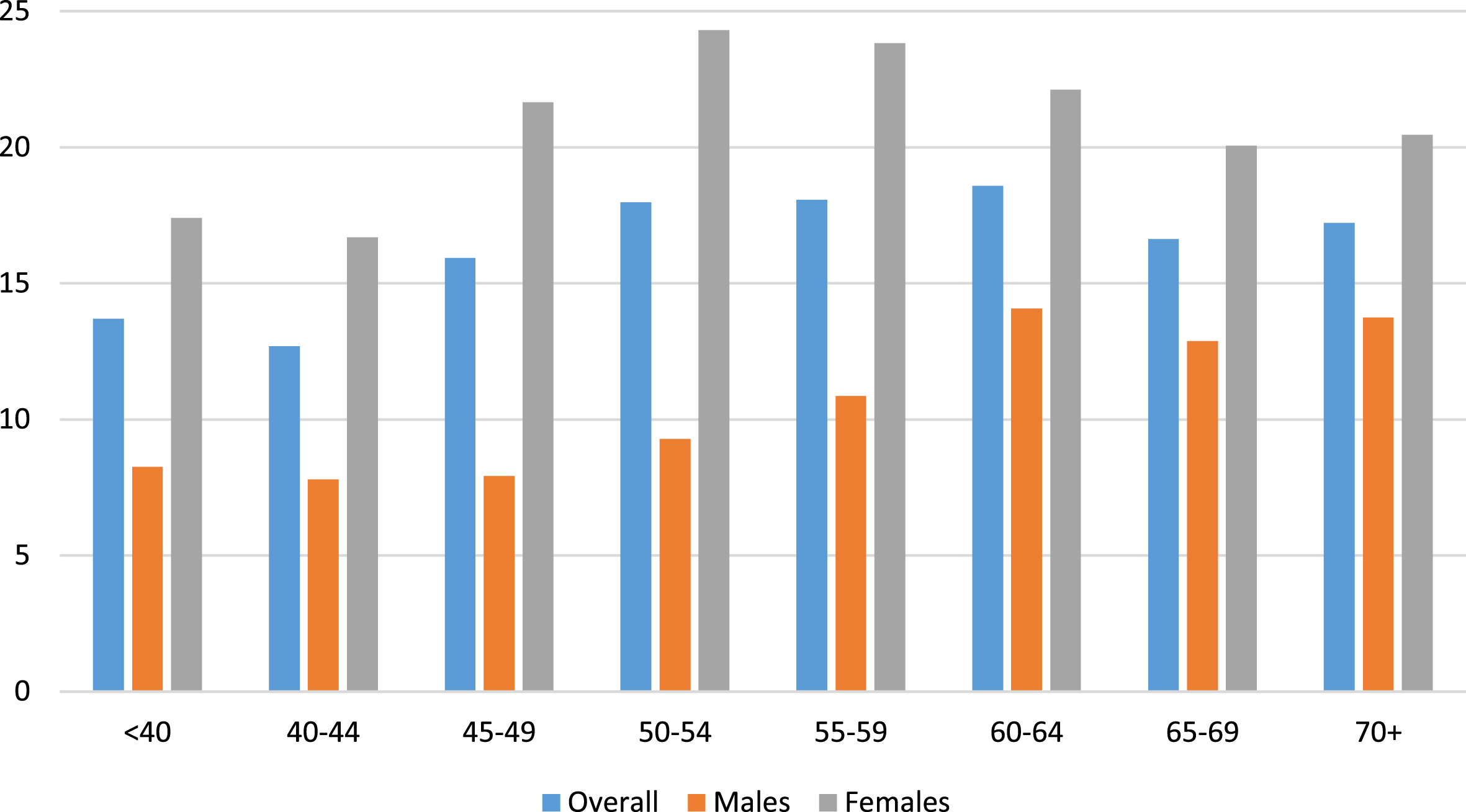
Prevalence of SMC by age and sex.
Objective global cognitive function (i.e., MMSE performance) was more strongly associated with SMC responses in the older versus the younger participants (Table 1). SMC endorsement among those with an MMSE score >26 was 13.7% among the younger participants and 13.3% among the older participants, while reported prevalence among those with an MMSE score ≤21 was 22.5% in the younger group and 28.5% in the older group. Among those who denied SMC, 30.5% of the younger participants had MMSE ≤21, while 19.5% of the older participants who denied SMC had MMSE ≤21. Cognitive evaluation scores, MMSE, as well as the individual modules for semantic fluency and memory of the ACE-R, were significantly worse among those endorsing SMC, regardless of the age group (Table 1); however, phonemic fluency was significantly worse only among the older participants.
Some characteristics of participants who reported SMC were also different within age groups. Among those 38–59 years old, participants who reported SMC were more likely to use antidepressants, but this was not the case among the older group. The univariate analysis showed higher odds of SMC among those younger than 60 and with diabetes, hypertension, history of cancer, depression, and hypothyroidism, while in the older group the associations with diabetes and hypothyroidism were not observed (Supplementary Table 1). Furthermore, the use of antidepressants appeared to be significantly related to higher odds of SMC only among the younger participants, while having depression was associated with higher odds of SMC in both groups (Supplementary Table 1).
Factors associated with SMC
The results from the not-stratified adjusted multinomial regression analysis showed that older participants compared with the younger participants with normal cognition have higher odds of SMC. Furthermore, it showed that having a bad self-reported health status, depression, a higher number of comorbidities, and a greater number of missing teeth increases the odds of SMC, while being a male, having more years of education, a higher score in the memory components of ACE-R, diabetes, and hypertension significantly decreased the odds of SMC (Fig. 2).
The results from the stratified adjusted multinomial regression analysis are shown below.
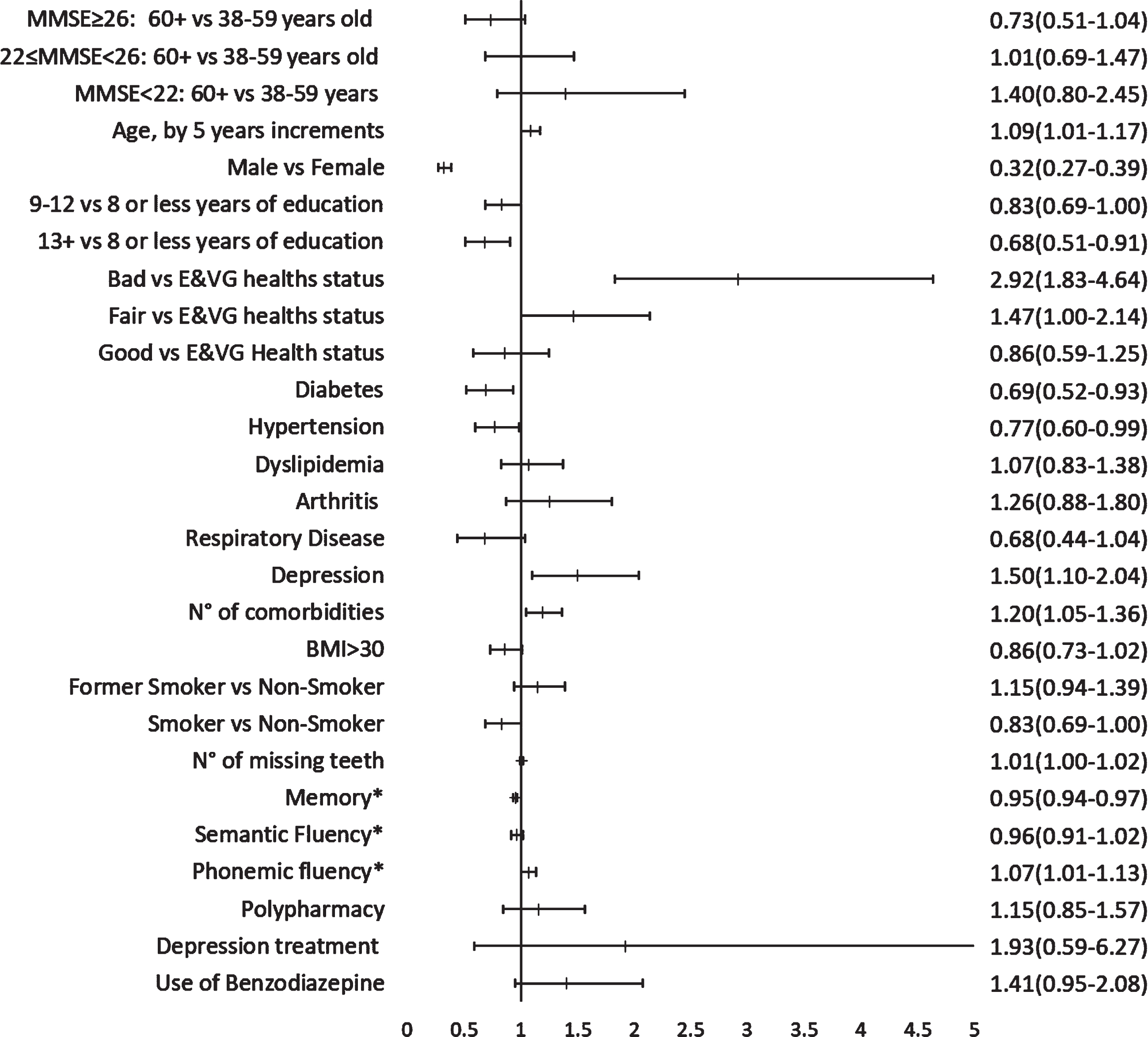
Non-stratified multinomial regression analysis for SMC. Yes versus No. N = 6,499. E&VG, Excellent and Very good; *This corresponds to components from the ACE-R.
Younger participants (<60 years old)
Among the participants with high MMSE (>26) scores (n = 3,313), age, sex, self-reported health status (SHRS), depression, and number of comorbidities were most strongly associated with odds of SMC reporting. Among those with MMSE scores 22–25 (n = 1,327), sex, self-reported health status (SRHS), number of missing teeth, and use of benzodiazepines were most strongly associated. For those with MMSE scores ≤21 (n = 293), only sex was strongly associated with odds of SMC. We note that male sex was strongly associated with decreased odds of endorsing SMC, across all three strata (Fig. 3A, C, E).
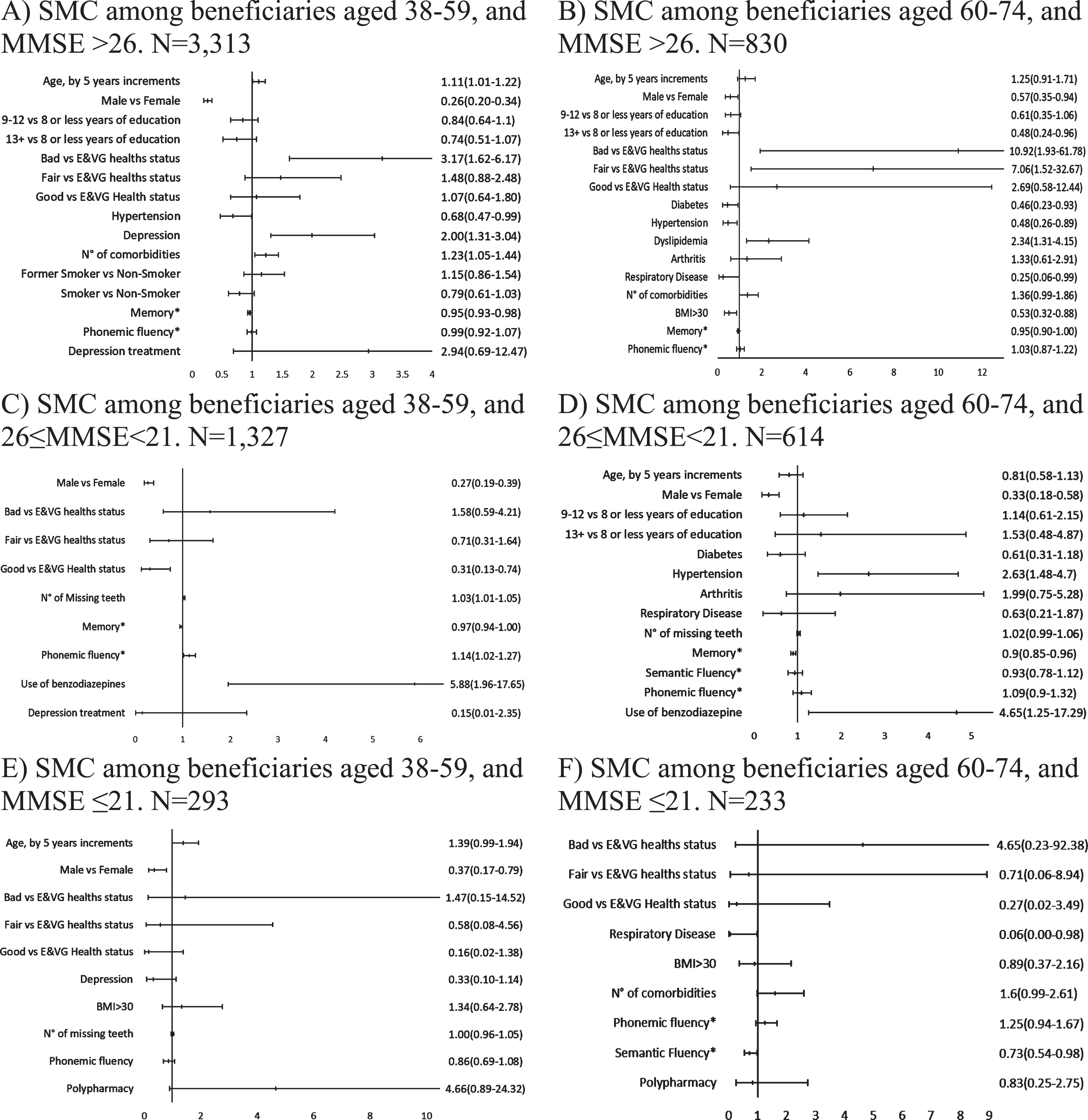
Results from the stratified multinomial regression analysis to determine factors associated with SMC Yes versus No for the different strata. E&VG, Excellent and Very good; *This corresponds to components from the ACE-R.
Older participants (60 and older)
Among the participants with high MMSE (>26) scores (n = 830), sex, and SRHS were again strongly associated with odds of SMC (Fig. 3B). Dyslipidemia was also associated with higher odds of SMC reporting, but depression was notably absent. Among those with MMSE scores 22–25 (n = 614), sex was again most strongly associated (Fig. 3D). For those with MMSE scores ≤21 (n = 233), only respiratory disease and a higher score in the semantic fluency component of the ACE-R were associated with the odds of SMC. In this case, sex was absent (Fig. 3F).
The sensitivity analysis on the restricted cohort (participants with depression were excluded, N = 616) performed provided very similar results, showing that the associations observed were the same regardless of the depression status of participants (Supplementary Table 2).
DISCUSSION
Prevalence of SMC
SMC was common in both younger and older MAUCO participants; however, the observed prevalences were lower than what has been previously reported. In a review by Jonker et al., the prevalence of SMC in cross-sectional studies varied from 22% to 56% [8]. However, this review included only one study that included participants younger than 65; this study showed the lowest prevalence of SMC (22%) [8, 38]. The SMC prevalence observed among those younger than 65 in that study population was about 16%, very similar to what was observed in MAUCO for the younger participants [38]. However, the SMC prevalence in the USA for those younger than 65 years old is about 11%, and close to 12% for those 65 and older, much lower than the observed prevalence in MAUCO.
Some potential explanations for the lower observed prevalence in this study could be the fact that Molina is a semi-rural county (20% of its population lives in rural areas [39]), with lower education, and a lower prevalence of depression (national prevalence of depression in Chile is 15.8% according to the last National Health Survey [40], while the sample studied has a prevalence of 8.5%), both factors previously associated with reporting SMC [14, 41]. These same factors could be influencing the big difference in the prevalence of SMC between MAUCO participants and US populations. For example, the US prevalence of depression is close to 5% [42], much lower than the prevalence observed in the MAUCO and Chilean populations. Another key feature is that MAUCO also included “sometimes” as a possible response, which may better capture a participant’s assessment of their memory function. Of note, the sex-specific differences in SMC reporting in this study require further study. In the present study, as in previous ones, female participants were most likely to report SMC, independent of age and cognitive status: by about 273–388% for those 38–59 and 75–305% for those 60–74 [1, 14]. Even after controlling for SHRS, comorbidities, education, cognitive status and age, men were significantly less likely to endorse SMC. Thus, our study may underestimate the true burden of SMC in this population. Nevertheless, whether this difference is based on self-perception of participants or a real difference in the prevalence of SMC, it is important to study the potential reasons for this difference, as this may be part of the etiology of SMC and later dementia.
Factors associated with SMC
Previous research showed that having a bad or poor SRHS increases the risk of SMC [14], and our results were largely in agreement. Indeed, our results suggest that SRHS may be an important factor to account for when assessing SMC. Previous researchers report an association between a diagnosis of depression and an increased risk of SMC, independent of the age group [3, 22]. However, our analysis only found an association between depression and increase risk of SMC among the younger adults with possible dementia. Similarly, while we observed associations between dyslipidemia and elevated BMI and higher odds of SMC [14, 17], these associations were restricted to certain subgroups. This may reflect that risk factors are in fact subgroup or disease-stage specific, or it may be due to variability and sample size limitations.
Our result showed that diabetes was statistically significantly associated with lower odds of SMC only among the older adults with normal cognition or mild cognitive impairment; however, in this case the association was in the opposite direction of what was expected (if diabetes contributes to cerebral small vessel disease, for example), as it showed to be a protective factor against SMC. However, this is only a somewhat unexpected finding that may need more research, as previous studies have either also reported diabetes associates with reduced odds of SMC or found no association between diabetes and SMC [43, 44].
Regarding medication use, we noted that use of benzodiazepines was retained only in the models for the strata with MMSE score between 22 and 26, and in both cases, it was a significant factor increasing the odds of SMC. Also, even though polypharmacy was present in the models for both strata with potential dementia, it was not statistically significant.
Up to our knowledge, polypharmacy has only been considered as a risk factor for SMC in one previous study, where it was defined as the number of medications participants were using, and was associated with SMC [14]. In this case, it is important to consider that the definitions used for polypharmacy are different, and then, comparing the results from Pedro et al. with the current results may not be appropriate. Thus, further analysis of the potential association of medication use and SMC is needed. Although further research on this field is needed, we can hypothesize that the effects of medications are observed once there is already some level of cognitive decline.
Thus, research on SMC should include analyses of the evolution of the cognitive function over time taking into consideration potential risk and protective factors. Furthermore, the results presented here are a good baseline for future research comparing MAUCO participants’ cognitive status before and after SARS-COV-2 infection.
Strengths and limitations
This study has several strengths. First, MAUCO is a large, well-characterized population-based cohort. Most studies analyzing the prevalence of SMC have been done in older populations or particularly selected populations, such as memory clinic patients [3, 45]. The MAUCO sample representativeness regarding Molina was previously evaluated with positive results [46]. Even though the study cannot be generalized to every population, we believe it could be generalizable to other semi-rural communities in Chile and other areas in South America. Another strength of the present study is that it encompasses a large number of participants from ages 38 to 74, which would allow generalizability of the results to younger people living in semi-rural environments.
On the other hand, the possibility of information bias is a potential limitation. Chile does not have a centralized system to register and analyze patient’s medications and diagnoses, which makes this information subject to recall bias. Another limitation is that SMC was evaluated with only one question, not with a standardized method, such as the Memory Complaint Questionnaire [45]. This could be associated with some validity issues, and we observed some evidence that male and female participants responded to the question differently. However, previous studies have also shown that SMC reporting is different by sex when using the Everyday Cognition Scale, so we do not believe this measurement issue is specific to MAUCO. Finally, the present analysis, although informative, does not have enough information on anxiety, and other psychiatric disorders and symptoms associated with SMC, especially in younger populations [47]. Thus, future analysis should consider these variables in addition to what has been used here and the literature.
Footnotes
ACKNOWLEDGMENTS
We are grateful to the MAUCO team and participants for their time and assistance.
FUNDING
The development and management of MAUCO are supported by funding provided by the Chilean government through the National Commission for Scientific & Technological Research (CONICYT) for Research Centers in Priority Areas (FONDAP) [grant number 15130011], and from FONDECYT Project [grant number 1170395]. Furthermore, additional funds come from the Faculty of Medicine and the Vicerectoría de Investigación of Pontificia Universidad Católica de Chile. Dr. Abner is supported by National Institute on Aging P30AG072946. However, the sponsors had no role in the writing process of the present manuscript.
CONFLICT OF INTEREST
Erin L. Abner is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review. All other authors have no conflict of interest to report.