
Abstract
Background:
Virgin coconut oil (VCO) is a potential therapeutic approach to improve cognition in Alzheimer’s disease (AD) due to its properties as a ketogenic agent and antioxidative characteristics.
Objective:
This study aimed to investigate the effect of VCO on cognition in people with AD and to determine the impact of apolipoprotein E (APOE) ɛ4 genotype on cognitive outcomes.
Methods:
Participants of this double-blind placebo-controlled trial (SLCTR/2015/018, 15.09.2015) were 120 Sri Lankan individuals with mild-to-moderate AD (MMSE = 15-25), aged > 65 years, and they were randomly allocated to treatment or control groups. The treatment group was given 30 mL/day of VCO orally and the control group, received similar amount of canola oil, for 24 weeks. The Mini-Mental Sate Examination (MMSE) and Clock drawing test were performed to assess cognition at baseline and at the end of the intervention. Blood samples were collected and analyzed for lipid profile and glycated hemoglobin (HbA1 C) levels.∥
Results:
There were no significant difference in cognitive scores, lipid profile, and HbA1 C levels between VCO and control groups post-intervention. The MMSE scores, however, improved among APOE ɛ4 carriers who had VCO, compared to non-carriers (2.37, p = 0.021). APOE ɛ4 status did not influence the cognitive scores in the control group. The attrition rate was 30%.∥
Conclusion:
Overall, VCO did not improve cognition in individuals with mild-to-moderate AD following a 24-week intervention, compared to canola oil. However, it improved the MMSE scores in APOE ɛ4 carriers. Besides, VCO did not compromise lipid profile and HbA1 C levels and is thus safe to consume.
INTRODUCTION
Late-onset Alzheimer’s disease (AD) emerges in older adults and is thought to be caused by complex interactions of genetics and environmental factors that provoke neuronal hypometabolism [1]. Induction of ketosis via diet during glucose deficit is an intervention recognized for its potential in providing symptomatic and disease-modifying effects in AD [2–4]. Increased ketone bodies substitute for glucose as an alternative energy source for neurons with compromised glucose metabolism in AD as a result of disruptions in the glucose transporter enzymes and several Krebs cycle enzymes [5–7]. Medium chain fatty acids (MCFA) effectively generate ketone bodies during metabolism. MCFA are absorbed mainly as free fatty acids and transported to the liver directly through the portal venous system. They then undergo rapid beta-oxidation to produce ketone bodies (acetoacetate, 3-beta-hydroxybutyrate, and acetone) in the liver mitochondria [8–11]. Since the major portion of the absorbed MCFA does not directly enter the systemic circulation, they are less prone to deposit in the arterial walls and adipose tissue, thereby not contributing to atherosclerosis [12, 13]. Evidence shows that atherosclerosis induced cerebral hypoperfusion contributes to the clinical and pathological manifestations of AD [14]. Moreover, other related cardiometabolic risk factors such as hyperlipidemia, hypertension, obesity, and insulin resistance are also risk factors for AD [15, 16]. Therefore, induction of ketosis via MCFA would potentially be a safe treatment approach for AD that would not elevate other risk factors.
Coconut is an excellent source of MCFA due to its unique fatty acid composition serving as a substrate for the generation of ketone bodies that can substitute glucose in the AD brain, in which the glucose metabolism is impaired. Coconut oil primarily consists of approximately 92% saturated fatty acids (SFA), out of which nearly 63% is MCFA [17]. This makes coconut oil a good source of ketones. In addition, the antioxidant properties of virgin coconut oil (VCO) due to its high polyphenolics content make it a functional food beneficial against oxidative stress and related chronic diseases such as cardiovascular disease and neurodegenerative disorders [18–20]. The production of VCO using extraction under cold conditions makes it a rich source of antioxidants, mainly polyphenolics, compared to refined, bleached, and deodorized (RBD) coconut oil made with copra [21, 22]. The major phenolic acids detected in VCO are ferulic acid and p-coumaric acid, which are capable of attenuating the oxidative stress associated with AD and combating inflammation [23]. Moreover, in rat models, the polyphenolic fraction of VCO has showed more inhibitory effect on microsomal lipid peroxidation compared to that of copra oil [22, 24]. Thus, VCO supplementation is recognized as a potential therapeutic dietary approach to combat AD and associated cardiometabolic risk factors, due to its excellent ketogenic and antioxidative properties [25–27].
Anecdotal reports from Dr. Mary Newport suggested that addition of extra-VCO into the diet of her husband, who had AD, improved his cognition and interaction with family [28, 29]. In addition, a semi-synthetic preparation of fractionated triglycerides, predominantly caprylic acid derived from coconut oil and named “Axona®”, has shown some beneficial effects in individuals with AD [7, 31]. Development of dietary remedies with VCO in terms of a nutritional supplement or a medical food is an emerging industrial approach. Although these findings triggered more attention towards investigating VCO as a therapeutic approach in the treatment of AD, this research is still at its infancy and the published systematic clinical trials on the use of VCO in AD is limited. Determination of the effects of genetic risk factors such as presence of apolipoprotein E (APOE) ɛ4 allele is crucial to the development of successful personalized therapeutic strategies for optimal benefits [32]. There is controversy with regard to the effects of coconut oil in particular on serum lipids, where controlled trials comparing coconut oil and polyunsaturated oils have suggested that coconut oil tends to raise plasma low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and total cholesterol (TC) [33]. However, there have been several studies with VCO demonstrating it does not increase LDL-C [34–36]. A controlled trial comparing intake of extra VCO, extra virgin olive oil, and butter found that the effect of extra VCO on LDL-C was more comparable to that of extra virgin olive oil [34].
The objectives of this research were to investigate the effects of VCO on cognition in individuals with mild-to-moderate AD (VCO-AD Study) and to investigate the association of APOE genotype on the changes in cognition. In addition, the effect of VCO on lipid profiles and HbA1 C levels was also determined.
MATERIALS AND METHODS
Study design
The VCO-AD study is a double-blind randomized placebo-controlled trial. Study protocol is shown in Fig. 1. Ethical approval was obtained from the Ethics Review Committee of the Faculty of Medicine, University of Kelaniya, Sri Lanka, and this research has been registered at the Sri Lanka Clinical Trials Registry (Reg. no. SLCTR-2015-018, Reg. date 15 September 2015).
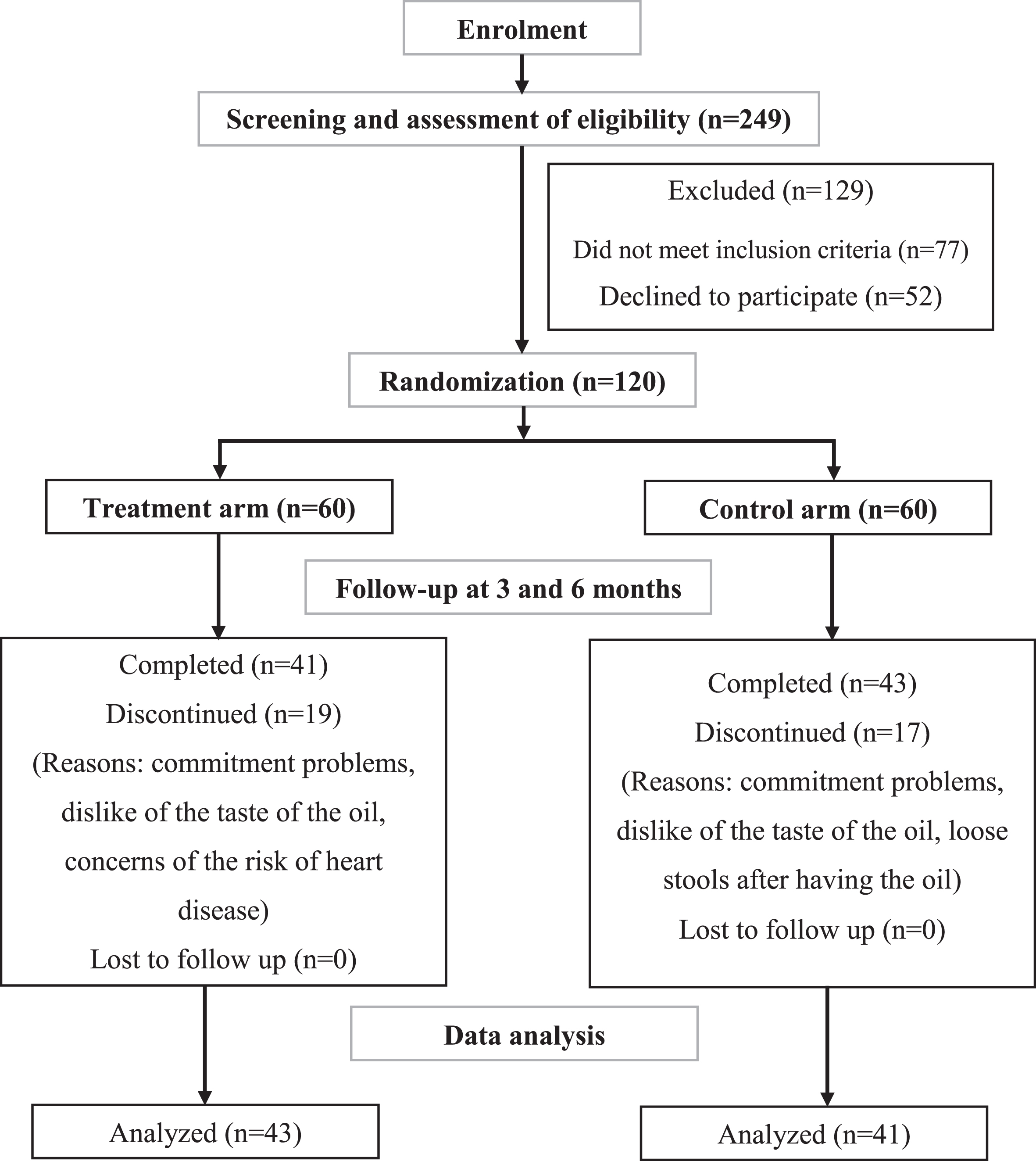
Flow diagram of the double-blind randomized placebo controlled trial to investigate the effect of consumption of 30 mL/day of VCO for 24 weeks on the cognition of individuals with mild-to-moderate AD (VCO-AD Study).
Participants
The study population was Sri Lankan older adults including males and females with mild-to-moderate AD, who were 65 years or older. Participants were recruited from the Psychiatry Clinics of North Colombo Teaching Hospital, Ragama and Lanka Alzheimer’s Foundation, Colombo 10 (residents of Colombo and Gampaha districts, Sri Lanka). Both participants and their next of kin caregivers provided informed consent prior to be enrolled into the study. The diagnosis of probable AD was made by clinicians based on the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS/ADRDA) criteria [37]. The Mini-Mental State Examination (MMSE) [38] was conducted and those with a MMSE score between 15 and 25 were selected. A total of 120 participants were recruited [males: n = 42 (35%), females: n = 78 (65%)], and randomly allocated to each of the treatment and control (placebo) groups (n = 60 for each group). Allocation concealment was maintained throughout the study.
Participants with a history of Parkinson’s disease, head injury, stroke or radiological evidence of vascular cognitive impairment, untreated diabetes or thyroid disorder and probable Korsakov’s syndrome or other known cause of dementia were excluded. Moreover, participants with significant depressive or psychotic disorders and those who were currently participating in other similar types of trials or had a habit of consuming VCO were also excluded.
Intervention
The treatment group was administered a total of 30 mL/day of VCO orally in liquid form of the oil and the control group had the same amount of canola oil as placebo. The oil was given to the participant by the caregiver in two 15 mL doses, one in the morning and one in the evening with a meal or before a meal for 24 weeks.
Data collection tools and measurements
The MMSE and executive clock drawing task (CLOX) [39] were performed to assess the cognition of the participants on the date of recruitment (baseline) and at the end of the intervention (after 24 weeks) by a blinded rater. Information was collected on socio-demographic and lifestyle characteristics, physical activity level and medical history for chronic disorders and family history for AD. The retrospective information collected from participants was verified for accuracy by the participant’s next of kin caregiver. The nutritional status of the participants was assessed using the Mini Nutritional Assessment tool (MNA) [40]. Anthropometric measurements of height, weight, mid-upper arm circumference (MUAC), and calf circumference were measured following the World Health Organization’s (WHO) standard procedures [41].
Dietary data was collected using an interviewer administered 24-h recall and a self-administered 5-day diet diary. A 24-h recall was taken with the support of the next of kin caregiver at baseline and the information was used to identify the usual dietary energy and nutrient intake. With the aim of maintaining the same usual dietary energy and fat intake of the participants during the intervention period, they were advised to cut down a similar amount of fat to the treatment therapy from their diet (30 mL/day), while not making any drastic changes to their usual dietary pattern. A self-administered 5-day diet diary with the support of the next of kin caregiver was collected during the 10th and the 12th week after initiating the intervention (mid-point). Information collected on the 5-day diet diaries was used to assess the dietary energy and nutrient intake of participants during the intervention.
Blood samples were collected following the standard WHO guidelines for drawing blood [42]. A total of 5 mL of blood was collected after a 12-h fast for lipid and glucose measurements at baseline, mid-point, and post intervention. Fasting lipid profile [TC, triglycerides (TG), HDL-C, LDL-C, very low-density lipoprotein cholesterol (VLDL-C), and total cholesterol/HDL-C ratio] was measured by the Siemens Dimension® EXLtrademark analyzer and fasting glycated hemoglobin (HbA1 C) level was measured using the standard High-Performance Liquid Chromatography (HPLC) method at baseline and post intervention. Fasting lipid profiles were also measured in the blood samples taken at the mid-point (12th week) to verify if there were any adverse changes which could indicate VCO (or canola oil) intake was unsafe for the participant to continue the intervention. In addition, full blood count, liver function tests, urine full report, blood urea level, serum electrolytes, serum creatinine level, thyroid stimulating hormone level, and blood picture were taken at baseline to determine the presence of any other potential diseases or risk factors. Lipid profile, HbA1 C levels as well as all other blood investigations were performed at the accredited laboratory of Hemas Hospital, Wattala, Sri Lanka. APOE genotype was determined using standard polymerase chain reaction and restriction enzyme digest techniques at the accredited laboratory of Genetec Molecular Diagnostics and School of Gene Technology, Sri Lanka. Amplification refractory mutation system- polymerase chain reaction (ARMS-PCR) techniques were performed for APOE haplotypes; ɛ4, ɛ3, and ɛ2 on blood samples [43].
Data analysis
Information on the 24-h recall and 5-day diet diaries were analyzed using a modified version of the “Foodbase 2000” software (The Institute of Brain Chemistry and Human Nutrition, UK) with nutrient compositions of Sri Lankan dishes [44].
Statistical analyses were performed using the Statistical Package for the Social Sciences version 27.0 (SPSS Inc, Chicago, Illinois, USA). The analyses were adjusted for confounders such as severity of disease and co-morbidities. The data was not normally distributed and the significant differences between treatment and control groups were compared using Chi-square test and Mann-Whitney U test, while, within group variations were compared using Wilcoxon signed rank test.
RESULTS
Out of 120, 43 participants in the treatment group (males: 11, female: 32) and 41 in the control group (males: 18, females: 23) completed the study. The dropout rate was 30%, which included 28% from the treatment group and 32% from the control group. There was no significant difference in attrition rate between the groups. The reasons for dropout in both groups were AD individuals’ or their family members’ commitment problems (treatment group: 10, control group: 11), mobility difficulty and frailty impacting on clinic visits (treatment group: 1, control group: 0), concerns related to the risk of coronary heart disease (treatment group: 0, control group: 1), disliking the taste of the oils (treatment group: 3, control group: 7) and loose stools after having VCO (treatment group: 3, control group: 0). The mean age (± SD) of the participants was 74 ± 7 years and the age at onset of AD was 72 ± 6 years. The majority were retired at the time of the assessment with an average monthly income (± SD) of 55,136 ± 88,395 LKR suggestive of a middle-income group in Sri Lanka. The socio-demographic and lifestyle characteristics of the participants are shown in Table 1.
Socio-demographic and lifestyle characteristics
LKR, Sri Lankan rupees (1 LKR is equivalent to 0.0034 US dollars).
Nutritional status and physical activity level
#Chi-square test, significant level of 5%. BMI, body mass index; MET, metabolic equivalents; MNA, Mini Nutritional Assessment; MUAC, mid upper arm circumference.
Nutritional status, physical activity level, and medical history
Based on the BMI scores, the majority of the participants were overweight or obese according to the Asian-Pacific cut-off points for BMI, and based on the MNA scores, the majority had normal nutritional status. Most of the participants were sedentary (< 600 Metabolic equivalents; MET). There was no significant difference in the nutritional status and physical activity level between the treatment and the control group (Table 2).
Participants diagnosed with chronic diseases included those with hearing impairment (13.1%), visual impairment (36.9%), ischemic heart disease (15.5%), hypertension (41.7%), diabetes (29.8%), hypercholesterolemia (34.5%), peptic/gastric ulcers (2.4%), respiratory disease (3.6%), and depression (7.1%). These disease conditions were all in clinically well managed stages with or without medication. Thus, the participants at entry into the study were relatively healthy with normal clinical parameters for full blood count, liver profile, serum electrolytes, serum creatinine, blood urea, thyroid stimulating hormones and urine full report and there were no significant differences between treatment and control groups.
Dietary intake of energy and nutrients
There was no difference of pre-intervention as well as during the intervention (diet + oil supplement) dietary intake between the treatment and the control groups, except that in the treatment group, the saturated fat intake during the intervention was higher compared to the control group (Table 3).
Pre- and during the intervention dietary intake of energy, macro- and micro-nutrients
†Mann-Whitney U test, significant level of 5%, *p < 0.05.
Both pre- and during the intervention, the mean energy and protein intake of the participants was lower than their Recommended Dietary Allowance (RDA) [45]. Percentage calories derived from carbohydrate, protein and fat in the diet were at the recommended levels. However, the amount of saturated fat intake was higher than the recommendation [46]. Prior to the intervention, only 21% and 42% of the participants in treatment group and 10% and 32% in the control group met the RDA for energy and protein, respectively. During the intervention, only 21% and 30% of the participants in the treatment group and 23% and 34% in the control group met the RDA for energy and protein intake, respectively. Energy and fat intake (diet + oil supplement) of the treatment (energy: p = 0.001, fat: p = < 0.001) and control (energy: p = < 0.001, fat: p = < 0.001) groups during the intervention was significantly higher than the pre-intervention intake, due to the oil supplementation.
APOE genotypes and family history for AD
Among the participants in the treatment and the control groups, 48.8% and 65.9% respectively, had an APOE ɛ4 allele, and there was no significant difference between the groups (p = 0.115) (Fig. 2). Most prominent genotype was ɛ3/ɛ4. The majority of both the treatment and the control groups (77.4%) did not have a family history for AD.

APOE genotypes in the treatment and the control groups. APOE ɛ4 (+), presence of APOE ɛ4 allele; APOE ɛ4 (–), absence of APOE ɛ4 allele.
Change in cognitive scores, lipid profile, and HbA1 C levels
Cognitive scores, lipid profile and HbA1 C levels during the intervention (Change = post-intervention result –baseline result) did not significantly differ between treatments; VCO and control (canola oil) groups (Table 4).
Change in cognitive scores, lipid profile and HbA1 C levels by VCO and canola oil
†Mann-Whitney U test, significant level of 5%; ‡Wilcoxon signed rank test, significant level of 5%; *p< 0.05. CLOX, Clock Drawing Task; HbA1 C, glycated hemoglobin level; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; MMSE, Mini Mental State Examination; SD, standard deviation; TG, triglycerides; TC, total cholesterol; TC/HDL-C, total cholesterol/ high density lipoprotein cholesterol ratio; VLDL-C, very low-density lipoprotein cholesterol.
Among the participants who were taking VCO, post-intervention TC (–6.7 mg/dL, p = 0.005), LDL-C (–10.4 mg/dL, p = 0.001), and TC/HDL-C ratio (–0.4, p = 0.001) decreased significantly, while HDL-C level (2.2 mg/dL, p = 0.011) increased significantly compared to the baseline (Table 4). Among the participants who were taking canola oil, post-intervention TC (–5.5 mg/dL, p = 0.020), LDL-C (–5.9 mg/dL, p = 0.028), TC/HDL-C ratio (–0.2, p = 0.009), and HbA1 C level (–0.1 mg/dL, p = 0.040) decreased significantly and HDL-C level (1.3 mg/dL, p = 0.040) increased significantly, compared to the baseline.
Among the participants who were taking VCO, the MMSE score was significantly increased in APOE ɛ4 carriers (2.37, p = 0.021) compared to non-carriers (Table 5). This difference was mainly due to the decline in the MMSE score of APOE ɛ4 non-carriers in the VCO group. Among the participants who were taking canola oil, there were no significant difference in the MMSE scores between APOE ɛ4 carriers and non-carriers. However, when comparing irrespective of APOE ɛ4 status there was no significant difference observed between the treatment and control group in the MMSE or other cognitive parameters at the end of the trial. There was also no significant difference in the lipid profile and HbA1 C levels between the treatment and control groups.
APOE ɛ4 status and change in cognitive scores, lipid profile and HbA1 C levels by VCO and canola oil
†Mann-Whitney U test, significant level of 5%; *p < 0.05. MMSE, Mini-Mental State Examination; CLOX, Clock Drawing Test; HbA1 C, glycated hemoglobin level; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; TG, triglycerides; TC, total cholesterol; TC/HDL-C, total cholesterol/ high density lipoprotein cholesterol ratio; VLDL-C, very low-density lipoprotein cholesterol; SD, standard deviation.
DISCUSSION
This double-blind randomized placebo-controlled trial investigated for the first time the effect of VCO on the cognition of individuals with mild-to-moderate AD. Oral administration of 30 mL of VCO daily for 24 weeks did not change the MMSE and CLOX scores of individuals with mild-to-moderate AD compared to administration of canola oil. The MMSE scores, however, did improve in the APOE ɛ4 group compared to the non APOE ɛ4 group in the VCO treated group.
These findings differ from the study which reported that adjunctive oral administration of extra-VCO (20 g/day) positively influenced the cognitive performance of individuals with AD when administered for 6 weeks [35]. However, the sample size of the Gandotra et al., was 31 individuals with moderate-to-severe AD and comparisons were made on the basis of ADAS-Cog measures at baseline, 2, 4, and 6 weeks. Another study demonstrated improvement in the cognitive status of individuals with AD measured by the Mini-Examination Cognitive of Lobo after a dose of 40 ml/day of extra-VCO for 3 weeks alongside a Mediterranean diet [47].
The MMSE scores of APOE ɛ4 carriers in our study improved when treated with VCO. In contrast, the MMSE score in the APOE ɛ4 non-carriers declined. The literature in this context is inconsistent. A study on multidomain intervention (diet, exercise, cognitive training, and vascular risk management) to prevent dementia has also concluded that the benefits are more pronounced in APOE ɛ4 carriers [48]. APOE ɛ4 carriers have also benefitted more from an exercise intervention to preserve cognitive performance of individuals with AD [49] and from an acute high-fat feeding therapy (50% total fat, 25% saturated fat, glycemic index > 70) with cognitively impaired adults [50]. Contrary to these findings, Reger and colleagues have shown an improvement in ADAS-Cog test scores and paragraph recall only in individuals who were APOE ɛ4 non-carriers, although production of ketone bodies (beta-hydroxylbutyrate) after MCT supplementation was higher among the individuals with AD who carried the APOE ɛ4 allele [7]. This demonstrates that even though ketone production was higher in APOE ɛ4 carriers, APOE ɛ4 non-carriers may have utilized the ketones more efficiently. In another study, ADAS-Cog test scores were also improved by a ketogenic agent (AC-1202) only in individuals with AD who are APOE ɛ4 non-carriers [51]. APOE ɛ4 carriers were also identified to be resistant to drug therapies to improve cognition in AD [52–54]. It is also interesting to note that in our study the control group had more APOE ɛ4 non-carriers compared to the treatment group. It is unlikely though this difference alone could have accounted for a lack of difference in the control group. Overall, the exact mechanisms of the interplay between APOE ɛ4 status, ketones, and cognition in AD are not clear.
However, it is heartening that this intervention with VCO did not significantly change the TC, TG, HDL-C, LDL-C, VLDL-C, TC/HDL-C ratio, and HbA1 C levels of the individuals with mild-moderate level AD compared to canola oil. Supplementation with both VCO and canola oil did not compromise lipid parameters and thus, VCO is safe to consume in terms of the elevation of serum cholesterol levels in older adults with mild-to-moderate AD.
Considerable debate surrounds the effect of coconut oil on LDL-C. Coconut oil is predominantly saturated fat (approximately 90%) and saturated fats are known for increasing blood LDL-C level. A recent meta-analysis of controlled trials looking at the effect of coconut oil or VCO compared to polyunsaturated or monounsaturated oils (non-tropical vegetable oils such as sunflower oil, canola oil, corn oil, and virgin olive oil) cautioned against the use of coconut oil [33]. The authors did not attempt to separate out trials where VCO was fed from those where coconut oil was used. If one looks at VCO, our study is the second study where VCO has been shown to lower LDL-C while raising HDL-C, though the differences between VCO and canola oil groups failed to reach significance. In a previous controlled trial comparing effects of feeding VCO to butter and olive oil, LDL-C levels after VCO were comparable to olive oil but significantly lower than with butter [34]. These findings suggest that the effect of consuming VCO on plasma lipids may differ from that due to copra derived coconut oil.
Several other studies have also shown that dietary supplementation with coconut oil does not cause hyperlipidemia. In one study in obese women, feeding coconut oil raised the plasma HDL-C levels and lowered the TC:HDL-C ratio. In another study, consumption of 30 mL of VCO for 8 weeks showed a significant increase of HDL-C levels (5.72 mg/dL) of healthy Thai adults compared to controls (2% carboxymethylcellulose solution) with no changes in TC and LDL-C levels [55]. Compared to copra oil/ RBD coconut oil, VCO has also demonstrated more favorable effects on blood cholesterol levels and LDL-C oxidation with decrease of TC, TG, LDL-C, VLDL-C, and increase of HDL-C levels in Sprague-Dawley rats fed with oils for 45 days [22]. One possible explanation is that VCO is richer in antioxidants and thus exerts a positive effect on plasma lipids. In the same study, polyphenol fraction from the oils were isolated and in vitro LDL-C oxidation was assessed. The results showed that the polyphenol fraction of VCO prevented in vitro LDL-C oxidation with reduced carbonyl formation.
There were no significant differences in the socio-demographic and lifestyle factors, dietary intake, nutritional status, and physical activity level between the groups. Thus, the randomization had minimal impact from confounding factors. Nearly 60% of the participants were sedentary, while others were moderately active. MNA shows that 30% of the participants were at risk of malnutrition, while nearly 10% were underweight (BMI, less than 19 Kg/m-2) and MUAC was lower than 22 cm. Comparatively similar evidence on malnutrition was reported by another research from the Galle district of Sri Lanka, in which, nearly 31% of the elders were malnourished or at risk of malnutrition [56].
In the current study, the fat intake was significantly higher than in the participant’s usual diet (27 g) due to the oil supplementation, with no change in protein and carbohydrate intake. Even though this accounted for nearly a 14% increase in energy intake, the energy and protein intake remained lower than the RDA and only 22% and 34% of the participants met the RDA for energy and protein, respectively. Administration of 30 mL/day of VCO for 24 weeks, alongside the daily diet of low calorie, low protein, and high saturated fat, resulted in no adverse side effects in terms of blood lipid profile on individuals with mild-to-moderate AD. Thus, incorporating a reasonable quantity of VCO daily as a main dietary oil seems to be a safe practice.
Limitations
The drop-out rate was 30% with no significant differential attrition between groups. Due to the sample size reduction, the statistical power achieved was 80% (for the outcome of cognitive assessment score-MMSE). Furthermore, the study endpoint was an improvement in the MMSE and/or in CLOX scores which are non-specific cognitive outcomes and may not reflect improvements in specific cognitive domains including short term memory. A more extensive cognitive battery such as The Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) may have been useful to detect subtle changes but would not have been feasible to use given the lack of a cultural and linguistically adapted version in the Sinhalese and Tamil languages. Changes in behavioral and psychological symptoms of dementia and carer reports were not assessed. The energy and fat intake in the background diet was higher than the habitual diet (mainly due to the calories and fat from the treatment and control oil samples). These changes may have influenced overall nutrition/ health of the subjects and thus, the intervention results.
Future directions
A higher sample size as well as periodical assessment of plasma ketone levels throughout the intervention are useful to validate this relationship. Moreover, research should be conducted with a defined diet that matches the usual calorie intake of the subjects, to exclude any effects on memory and cognition due the changes in diet. In addition, research can be conducted to identify the optimal ketogenic diet ratios to generate a higher ketogenic effect during the VCO therapy that will amplify the benefits. Studies on VCO can also be conducted to identify the most effective MCFA and specific antioxidants in VCO which can be extracted and concentrated to develop therapeutic products such as medical food or supplements that are beneficial. Furthermore, the role of ketones in the treatment of more advanced dementia is not known and those with advanced dementia particularly may benefit from more ketones from their diet as glucose utilization becomes increasingly impaired with advanced AD.
Conclusion
Supplementation with oral VCO for 24 weeks did not result in improvement in the MMSE and CLOX scores in people with mild-to-moderate AD compared to canola oil. An improvement in the MMSE score was noted in the APOE ɛ4 carriers but its interpretation is unclear. Supplementation with VCO and canola oil did not compromise lipid parameters and is thus safe for consumption.
Footnotes
ACKNOWLEDGMENTS
The authors acknowledge the study participants and their carers who participated voluntarily without any remuneration. We also thank the Lanka Alzheimer’s Foundation, Sri Lanka for being a principal site for recruitment and conduct of the study.
FUNDING
The study was funded by the Coconut Research Institute, Sri Lanka, through a competitive grant.
CONFLICT OF INTEREST
Professor Ralph Martins is an Editorial Board Member of this journal but was not involved in the peer-review process, nor had access to any information regarding its peer-review. All other authors declare that there are no conflicts of interest to report. None of the authors are employed nor remunerated by the funding institute.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.