
Abstract
Background:
Primary progressive aphasia (PPA) is a neurodegenerative syndrome characterized by speech and/or language impairment with relatively spared cognition. Research investigating behavioral speech-language intervention and methods for cognitive-linguistic assessment in PPA has predominantly centered around monolingual speakers. This gap hinders the widespread adoption of evidence-based approaches and exacerbates the inequities faced by culturally and linguistically diverse populations living with PPA.
Objective:
This scoping review synthesizes the current evidence for assessment and treatment practices in bilingual PPA as well as the operationalization of bilingualism in PPA.
Methods:
Arksey & O’Malley’s scoping review methodology was utilized. Information was extracted from each study and entered into a data-charting template designed to capture information regarding operationalization of bilingualism in PPA and assessment and treatment practices.
Results:
Of the 16 identified studies, 14 reported the results of assessments conducted in both languages. Three studies reported positive naming treatment outcomes. Thirteen studies included English-speaking participants, revealing linguistic bias. Most studies reported age of acquisition, proficiency, and patterns of language use rather than providing an operational definition for bilingualism.
Conclusions:
Neither formal assessment measures nor clear guidelines for assessment of bilingual PPA currently exist; however, language-specific measures are emerging. Speech-language intervention in bilingual PPA has been relatively unexplored, representing a significant gap in the literature. In order to improve diagnostic and treatment options for bilingual PPA, targeted efforts to increase representation of bilinguals from various sociocultural contexts, as well as those who speak a variety of language pairs, is necessary.
Keywords
INTRODUCTION
Primary progressive aphasia (PPA) is a progressive syndrome caused by neurodegenerative disease, wherein the first and most salient symptom is speech and/or language impairment in the presence of relatively spared cognition [1–3]. In later stages of progression, global dementia presentation emerges and changes in memory, motoric function, and personality may appear. Consensus criteria [3] delineate three clinical variants, consisting of the semantic (svPPA), logopenic (lvPPA), and nonfluent/agrammatic (nfvPPA) variants; however, estimates indicate that 10–40% [4–7] of PPA cases present with features consistent with more than one variant. Each variant is characterized by a distinct profile of speech-language deficits and associated pattern of brain atrophy. Individuals with svPPA present with anomia and single-word comprehension deficits yet with fluent speech [3]. Atrophy in this variant is observed bilaterally in the anterior temporal lobes, although to a greater extent in the left hemisphere when individuals present with prominent aphasia [8]. Individuals with lvPPA present with anomia and repetition deficits due to impaired phonological processing [3]. Atrophy in lvPPA is observed in left temporoparietal cortex [9]. Individuals with nfvPPA present with apraxia of speech and/or agrammatism [3, 10–12]. Atrophy in nfvPPA is observed in left inferior frontal cortex and insula [10]. When individuals present with apraxia in the absence of notable linguistic impairment, the term primary progressive apraxia of speech [11–13] has been proposed to describe this phenotype.
Although there is currently no cure for this devastating condition, an increasing body of literature indicates that behavioral speech-language intervention results in improved communication [14–18]. A major limitation of this previous work is that the overwhelming majority of existing research has been conducted in monolingual speakers, despite estimates indicating that over half of the world’s population speaks more than one language [19, 20]. The lack of representation of bilingual speakers in PPA research extends beyond intervention studies as methods for cognitive-linguistic assessment in PPA have also focused predominantly on monolingual speakers [21–23]. As such, speech-language pathologists, who often administer cognitive-linguistic assessments and speech-language interventions to individuals with PPA, are faced with particular challenges when working with individuals who speak more than one language [24, 25]. The inability to provide evidence-based services to bilingual groups represents an inequity for culturally and linguistically diverse populations. In order to address this gap in the field additional work is needed addressing assessment and intervention practices developed for bilingual speakers with PPA in distinct sociocultural contexts.
When assessing and treating bilingual individuals with PPA, it is crucial to ensure equity, which means providing fair, unbiased, and just care that meets the unique needs of bilingual individuals [26, 27]. To provide equitable services that address the needs of bilingual patients, clinicians must embrace cultural humility, acknowledging and respecting the diverse cultural backgrounds, beliefs, and values that shape these individuals [27, 28]. To champion equity consistently, there’s a pressing need for clinician training on the nuances of bilingualism, more research focused on bilingual PPA, and collaboration with bilingual communities [29]. Conversely, inequities manifest in the absence of valid and reliable bilingual assessments developed for bilingual speakers, over-reliance on monolingual standards, inadequate clinician training, neglect of one of the patient’s languages, and limited accessibility to evidence-based intervention, all of which can compromise the quality of care bilingual individuals with PPA receive.
In this scoping review, we reviewed and synthesized the literature addressing cognitive-linguistic assessment and speech-language intervention practices in bilingual speakers with PPA. Given that there is a great deal of variability in current definitions and methods for characterizing bilingual speakers [30, 31], an additional aim of the current review was to synthesize definitions and characterizations of bilingualism within studies examining cognitive-communication assessment and speech-language interventions in PPA.
In the current scoping review, we sought to synthesize the existing evidence pertaining to three specific questions: Within studies that have examined assessment (question 2) or intervention (question 3) in bilingual PPA, what are the measures, instruments, and definitions used to characterize bilingualism in PPA? What are the current cognitive-communication assessment practices being utilized with bilingual speakers with PPA? What are the current evidence-based behavioral speech-language intervention practices that are utilized with bilingual speakers with PPA?
METHODS
Design
The methodology for conducting scoping reviews as described by Arksey & O’Malley (2005) [32] was utilized. This approach is beneficial when seeking to clarify definitions and conceptual boundaries of topics, especially when there is not a large number of studies conducted in a particular area of investigation. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist is a widely recognized tool designed to enhance the transparency and rigor of scoping reviews. It outlines key items that researchers should report when conducting and publishing scoping reviews, ensuring that the review process is comprehensive. The checklist [33] was completed by the first author in order to ensure comprehensive reporting throughout the review and adherence to established reporting standards (see the Supplementary Material for checklist).
Identifying and selecting relevant studies
A comprehensive search was conducted in October 2021 for peer-reviewed original research studies that report the inclusion of bilingual or multilingual individuals with PPA. Using the same search parameters, the search was conducted for a second time in February 2023 to ensure any additional published papers were reported. These searches were not restricted on the basis of the language the articles were written in. Four databases were used to identify potential sources: PubMed, Web of Science, Science Direct, and Google Scholar with an unlimited start date up until October 2021, and the secondary search included a range from October 2021 through February 2023. For each database, particular conventions were utilized with the use of multiple search fields and filters that were customized for each database. The search terms that were used were developed in consultation with a research librarian and were piloted before conducting the final search. Table 1 indicates the search terms used for each database. Elements of the search related to either the speaker status of the group or diagnostic terminology were combined within each domain using the OR operator and search domains were combined via the AND operator. Search terms were modified depending upon the constraints of the individual database.
Search Terms Utilized by Database
References were retrieved and stored in Mendeley and the automatic de-duplication feature was used to remove duplicated references. The unique references were then added to Covidence for screening. All articles were screened via title and abstract by two authors (S.M.G. and C.A.W.R.). Following the title and abstract screening, full texts were reviewed by the same two authors and any inconsistencies were discussed and resolved. Figure 1 displays a PRISMA flow chart indicating the results of study identification, screening, eligibility, and inclusion.
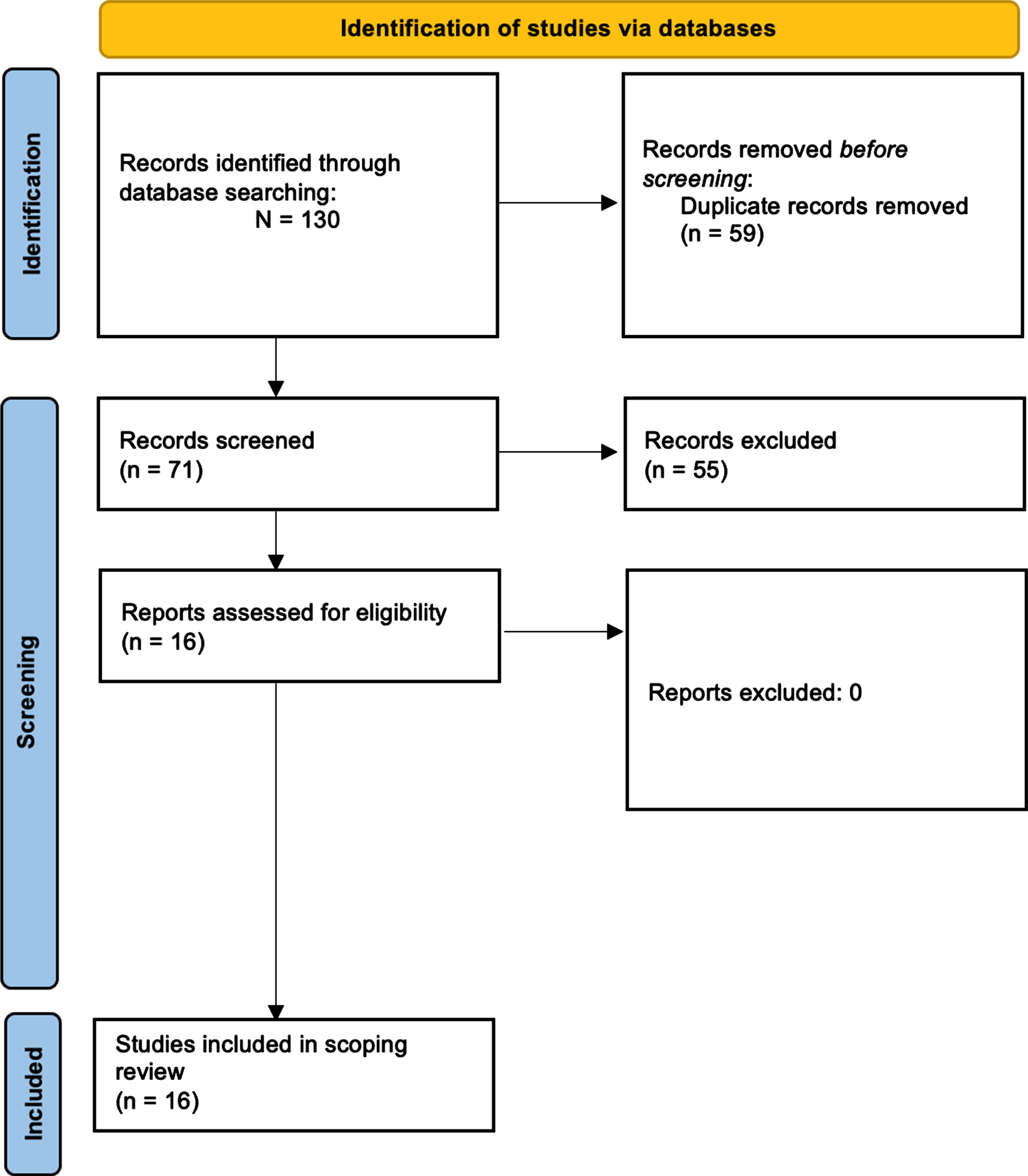
PRISMA flow diagram [34] demonstrating the study selection process for the current scoping review.
Eligibility criteria
The following inclusion criteria were utilized: Publication is a research article. Article reports an original research study. Participants included in the study are bilingual or multilingual. Participants included in the study have a diagnosis of PPA/PPAOS. Study investigates behavioral treatment for communication (in isolation or with other, non-behavioral intervention) -OR- investigates results of behavioral assessment battery (may be embedded within a case report/case study/single-subject experimental design; may be administered in one or more languages). Data reported in study demonstrate effects of treatment on communication -OR- effects/results of behavioral assessment battery. Article or abstract was written in English or Spanish.
Charting the data
From each study, information was extracted and entered in a data-charting template that was developed by the first author for the purpose of the current scoping review. These data included participant characteristics, methodological details of the study, assessment details, and intervention details (Table 2). A subset of the studies (13%; n = 2) were double-rated (between N.M.C. and S.K.M.K.) for all extracted information, reaching 89% consistency.
Data items extracted from selected studies
RESULTS
Study and participant characteristics
As is reported in the PRISMA flowchart (Fig. 1), 130 records were identified with 71 articles entering the screening stage and 16 full-text articles met inclusion criteria. Of the 16 articles that met inclusion criteria, only three studies had a primary focus on speech-language interventions utilized with bilingual speakers with PPA and the remaining articles investigated cognitive-linguistic assessment of bilingual PPA. Papers that met inclusion criteria were published between 2008 and 2023. The Supplementary Material includes a spreadsheet generated via Covidence indicating one reason that each abstract/article was excluded from the review.
In aggregate, studies reported on 56 bilingual individuals with PPA (n = 34 males), with 12 studies including a single participant. A total of 6 studies took place in the United States of America, with the remaining studies distributed across the United Kingdom (2), Spain (2), Greece (2), and single studies were reported from Norway, Italy, India, and Israel. Of the 16 total studies, ten reported the use of diagnostic criteria. Nine studies reported to use the consensus criteria proposed in Gorno-Tempini et al. [3], whereas two independent studies [35, 36] reported the respective use of the criteria in Weintraub et al. [37] and Mesulam [38]. There was a roughly equivalent representation of individuals with lvPPA (24) and svPPA (23; for the purposes of this review those with semantic dementia or right temporal FTD were included as svPPA), and far fewer individuals with either nfvPPA (5) or unspecified (4). Terminology defining PPA has evolved since the first descriptions of the syndrome. With respect to svPPA, some suggest that semantic dementia may be considered within the same realm as svPPA in the presence of object recognition impairments [39], and only one study in the review referenced inclusion of semantic dementia, though the criteria cited was that of svPPA [40]. In addition, in the current review, only one individual with right temporal FTD was included as their initial diagnosis was svPPA and with progression their diagnosis was considered most consistent with right temporal FTD [41]. On average, participants were 66.11 years old (range = 56–76; SD = 5.73) with an average symptom duration of 4.20 years (range = 1–10; SD = 2.72). For further summary data, please reference Fig. 2.
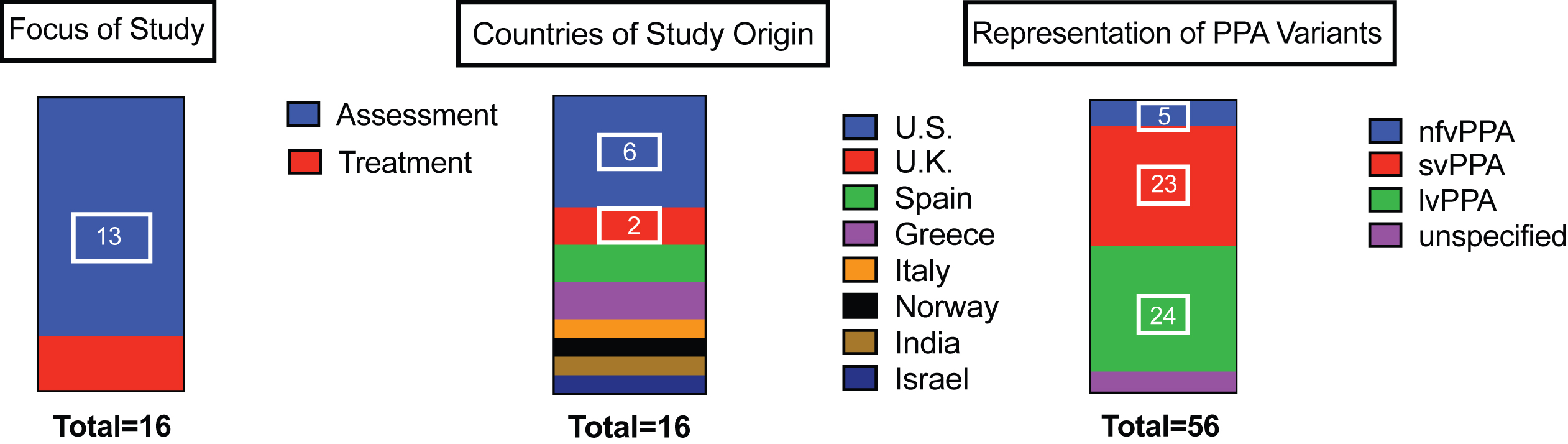
Summary data pertaining to foci, location, and distribution of participants by PPA variant.
Synthesis of results
Defining and characterizing bilingualism in the context of PPA
A summary of the definitions of bilingualism as well as subjective and objective measures reported in the reviewed studies are reported in Table 3. Of the 16 articles, 4 provided a definition of bilingualism [35, 42–44]. Three of the four studies cited Grosjean 1994, 1998, 2010 [19, 46], and a single study cited either Alladi et al. 2017 [47] or Fabbro 2001 [48] 2001. In general, these definitions described bilingualism or multilingualism as the regular/frequent use of more than one language, though different levels of specificity were used with describing specific aspects of defining bilingualism (see Table 3). The same four articles that provided a definition of bilingualism also indicated the use of a subjective measure (questionnaire) which was administered to the individual with PPA and there was variability in the specific questionnaire that was used [35, 42–44]. Although several studies did not report the use of a specific subjective measure, all studies reported variables characterizing some aspect of the bilingual experience. The specific subjective measures that were reported included the history of bilingualism portion of the Bilingual Aphasia Test [49], the Language Experience and Proficiency Questionnaire [50], the Language Use Questionnaire [51], and an in-house developed tool. The most frequent characteristics reported included proficiency (87.5%), language use (93.75%), and age of acquisition (87.5%). Only one paper [41] indicated the use of an objective measure which was intended to capture language dominance (see Gollan et al., for more detail [52, 53]).
Definitions, Measures, and Instruments Used to Characterize Bilingual Speakers with PPA
Assessment practices in bilingual speakers with PPA
A summary of the reported assessments used in each language of bilingual speakers with PPA is provided in Tables 4–6. All 16 studies included some form of cognitive-linguistic assessment for bilingual individuals with PPA. Two studies assessed individuals in only one language and the remaining fourteen studies assessed individuals in both languages. Beyond description of standardization, four studies overtly described psychometric properties relevant to the assessment of bilingual populations. Karpathiou et al. (2018) [42] described that the MMSE and Addenbrooke’s Cognitive Examination-Revised have been validated in Greek. Lind et al. (2008) [43] described that the Rowland Universal Dementia Assessment Scale is specifically designed to assess cognitive impairment in culturally and linguistically diverse populations with an established cut-off to indicate cognitive impairment. Calabria [62] and Tee [63] described that normative data were available for the tasks/tests utilized in each of their respective studies.
Summary of Cognitive Assessments and Informal Cognitive Tasks Used in the Assessment of Bilingual Speakers with PPA
Summary of Speech-Language Assessments Used in the Assessment of Bilingual Speakers with PPA
Two studies reported testing bilingual speakers in one language [44, 62]. In Calabria et al. [62], although the participant was assessed in one language (Spanish), instructions were provided in the participant’s other language (Catalan) due to the participant’s preference for that language and the authors indicated that Spanish instruction was used for those tests available in Spanish. In de Leon et al. [44], historical data were utilized wherein participants were tested in English if they had adequate proficiency and did not require an interpreter/translator.
Only two studies used measures that were developed specifically for use in PPA: the Progressive Aphasia Severity Scale [98] and the Chinese language Assessment for PPA test [63]. Four studies used the same measure specifically designed for bilingual speakers, the Bilingual Aphasia Test [49]; however, this measure was not originally designed for use with individuals with neurodegenerative disorders. In addition, several informal measures were utilized across eleven studies (Table 6). These measures and tasks assessed several linguistic domains across twelve different languages. Eight of the eleven studies administered these tasks across languages.
Summary of Informal Language Tasks Used in the Assessment of Bilingual Speakers with PPA
*Note that these tasks are described as part of the Chinese language Assessment for PPA Project.
Treatment practices in bilingual speakers with PPA
A total of three studies investigated the effects of treatment in bilingual speakers with PPA. These studies reported on interventions for anomia in either logopenic variant only or logopenic and semantic variant PPA. We summarize each study below.
In Meyer et al. (2015) [59], a naming treatment was administered in English to a Norwegian-English bilingual speaker with lvPPA. Initially eight in-person sessions took place, which were followed by 11 months of home practice. With the exception of written naming accuracy, the participant demonstrated decline in both languages from pre- to post-treatment. More specifically, the participant demonstrated better written naming accuracy for trained versus untrained items in English. Despite the fact that treatment was only offered in English, evidence for cross-language transfer was observed in oral naming and naming-to-definition accuracy in Norwegian.
An additional case study examined the effects of Verb Network Strengthening Treatment provided in Hebrew to a English-Hebrew speaker with lvPPA [36]. Treatment was administered over a ten-week period, with sessions taking place twice per week. Results indicated significant improvement in the independent retrieval of thematic roles per verb in Hebrew; however, decline was observed in oral narrative production, with stability present for word production, sentence production, and written narratives (as assessed via performance on the WAB and REHAB). Maintenance effects could not be assessed as the participant did not agree to participant beyond the treatment period. This study provides preliminary evidence that VNeST may be a viable prophylactic treatment option for individuals who present with a similar cognitive-linguistic profile.
Finally, in the first group treatment study of bilingual PPA, Grasso et al. (2021) [41], evaluated the effects of lexical retrieval treatment in bilingual speakers with lv and svPPA. Both within and between language effects were observed and the participants in this study were treated in English and their other language (i.e., Spanish, Portuguese, Farsi, or French). The treatment was designed to capitalize upon residual linguistic knowledge, while concurrently encouraging self-cueing through embedded strategic training, which was administered twice per week over a ten-week period. Participants demonstrated significant improvement in naming of trained items at post-treatment, with maintenance observed during the follow-up period (up to one-year post-treatment). These direct treatment effects were evident in participants’ dominant and nondominant languages and cross-linguistic transfer for cognate items was observed in the majority of the cohort. Participants and their care partners also perceived qualitative improvements in strategy usage and confidence in communication. In sum, this group study indicates that dual-language speech and language intervention results in immediate and long-term improvements in naming accuracy in bilingual speakers with PPA.
DISCUSSION
The purpose of this review was to synthesize the current evidence pertaining to cognitive-communication assessment and speech-language treatment practices in bilingual speakers with PPA. An additional aim was to synthesize the definitions and measures used to characterize bilingualism in this population. Our findings, highlighting the mere 16 papers (n = 56 participants across studies) focused on the assessment and treatment of bilingual PPA, underscore a stark inequity in the available evidence base for clinical decision making in this underserved population. The lack of research investigating assessment and treatment in bilingual PPA not only overlooks a substantial portion of the global bilingual population but also raises concerns about the underrepresentation of cultural and linguistic diversity in the literature. Although the current literature investigating bilingual PPA is limited, notable patterns emerged from the existing studies included in the current review.
Characterizing and measuring bilingualism
The results of the current review indicate that each study collected subjective data comprising at least two characteristics of the bilingual experience from participants. Most frequently, studies reported on age of acquisition, proficiency, and language use. Despite characterizing the study participants’ language history, very few studies 1) provided an operational definition of bilingualism or 2) used an already established measure/questionnaire meant to evaluate bilingualism history. The lack of consistency in the use of operational definitions and established measures makes it challenging to conduct cross-study comparisons. As such, future studies of bilingual PPA should clearly state operational definitions of bilingualism. Sociocultural factors have been shown to influence how individuals’ self-rate their degree of bilingualism [136]. The inclusion of clear definitions may provide one common basis for cross-study comparisons particularly if studies are conducted in different bilingual populations that may present with differences in their approach to conducting self-ratings.
Several self-report measures are now freely available to characterize several components of the bilingual experience and are essential to the investigation of bilingual PPA. Systematic inclusion of self-report measures is a prerequisite to draw meaningful conclusions on the basis of bilingualism history. These measures include but are not limited to the Language History Questionnaire [137], Language Use Questionnaire (LUQ) [51], and Bilingual Language Profile (BLP) [138]. Several factors may influence the selection of such a measure and will depend on the purpose of the study. Nevertheless, when considering the selection of a measure for individuals presenting with progressive language impairment, it is crucial to consider comprehensibility and responses that allow for pre- and post-morbid ratings of language abilities. The LUQ is one such measure that queries both pre- and post-morbid ratings and provides detailed information regarding language use. Although the BLP does not specifically query pre- and post-morbid ratings, this measure has the possibility of being easily modified for the purpose of capturing pre- and post- morbid ratings. An additional benefit of the BLP is that it consists of quite comprehensible language, with a consistent response format. In sum, the inclusion of clear operational definitions and use of established measures that can provide a number of characteristics associated with the bilingual experience will facilitate the ability to conduct cross-language comparisons. At present, there is a lack of evidence regarding how particular bilingual factors including age of acquisition, proficiency, and language use patterns affect language decline due to heterogeneity surrounding the reporting of such measures. Consistency in reporting such measures is especially important in bilingual PPA as bilinguals represent a subgroup of an already relatively rare syndrome. Therefore, the ability to address broader basic and clinical questions in bilingual PPA and other neurodegenerative disorders will be facilitated by examining patterns across studies. Such cross-study comparisons will be greatly strengthened via the use of comparable measures used to characterize bilingualism coupled with the inclusion of operational definitions.
Assessment practices
The majority of studies administered cognitive-linguistic assessments across bilingual speakers’ languages. A greater number of cognitive assessments appeared to be utilized across studies in comparison to speech and language testing. This appears to be driven by availability of such measures across languages. Whereas several adapted versions of cognitive screeners and measures currently exist, adaptation of language measures requires expertise of the structural properties of a given language and how those properties compare to those of other languages. The development of such tools have begun to emerge for screening of language symptoms (Mini-Linguistic State Exam [139]). Nevertheless, assessments designed specifically to detect language-specific features that are vulnerable in PPA have yet to be systematically designed across languages. One example of such a measure is the CLAP [63], which has specifically been designed to assess the features of PPA that have been shown to be symptoms in Chinese speakers with PPA, as well as emerging measures to characterize motor speech symptoms in Spanish or Catalán [140, 141]. The lack of language-specific measures for PPA is a direct reflection of the lack of research documenting symptoms unique to different languages. This is a limitation not only for monolingual speakers of languages other than English, but also for bilingual speakers wherein symptoms may reflect a combination of language-specific features. Limitations in diagnosis do not only arise from the lack of language-specific measures, but also from the fact that some components of the current diagnostic criteria focus most heavily on symptoms/linguistic features that are more frequently observed in the English language.
Several studies developed informal language tasks to assess the participants in their study. This is likely due to the inability to rely on established languages measures. As such, future research should continue to document the manifestation of PPA in different languages, as this will aid in earlier and more accurate diagnosis. Nevertheless, the development of such measures should emphasize functional and efficient means of assessment that also allow for identification of an individual’s strengths [142].
The development of speech-language assessments for different languages represents a foundational step towards informing assessments for bilinguals with PPA. Generally speaking, it is recommended that bilingual speakers be assessed in both languages (at least in some linguistic domains) as the bilingual experience leads to distributed knowledge across languages [143, 144]. In addition, because most individuals become bilingual out of necessity, without evaluating both languages clinicians will only gain partial knowledge regarding an individual’s language abilities when testing in one language. This is supported by the finding that bilinguals with and without Alzheimer’s Dementia (AD) named some items on confrontation naming tasks in the nondominant language that they were unable to name in the dominant language [145]. In addition, it was observed that confrontation naming in the dominant language resulted in greater differences between bilingual AD patients and controls, relative to performance in the nondominant language [145]. This suggests that testing in both languages provides important information for diagnostic purposes and treatment planning. In the context of the United States, a study investigating age of onset in bilingual FTD found that assessing individuals in English only resulted in similar patterns of performance in both nfvPPA and svPPA on a comprehensive neuropsychological battery, suggesting that overall profiles of impairment may reflect the expected pattern when bilinguals are tested in English. Nevertheless, this study was limited in the available data regarding bilingualism history and how this may have influenced the results [146]. In addition, such a pattern may only hold true in languages that are typologically similar to English, because as previously described, current consensus criteria heavily focus on symptoms present in the English language.
Several open questions remain regarding assessment in bilingual PPA, including the basic characterization of cognitive-linguistic presentation in bilinguals PPA across sociocultural contexts, what the earliest and most sensitive markers of PPA are in bilingual speakers, and if a particular threshold of language use or proficiency may support single-language testing when conducting an evaluation [147]. In order to address the risk of over-diagnosis (driven by normal speech-language differences related to bilingualism) and under- or late-diagnosis (because clinicians assume that symptoms are actually normal speech-language differences attributed to bilingualism) of PPA in bilingual speakers, much work is needed to develop appropriate assessments that account for bilingualism and sociocultural factors.
Treatment practices
Only a few studies have investigated treatment outcomes in bilingual PPA. Interestingly, one study took place outside of the United States (i.e., Jerusalem) [36], and only one study included a sub-sample of Latinx/o/a/es [41], the largest group of bilingual speakers in the U.S. The outcomes of these studies indicate that speech-language intervention can result in significant improvements and cross-linguistic transfer effects with an advantage for cognates (in lv and svPPA). The paucity of research examining the effectiveness of intervention in bilingual PPA represents a significant gap in the literature, with no studies yet reporting outcomes in bilingual nfvPPA. In some cases, intervention approaches may largely require adaptation and optimization for those who speak more than one language as the linguistic system of a bilingual speaker is not representative of two monolingual systems in one. Nevertheless, the basic assumptions that current treatment approaches are based upon ranging from theoretical bases, acceptability of treatment, dosage decisions, amongst others have largely been tested or explored in homogenous populations [148]. Sociocultural factors may also influence the feasibility, acceptability, and adherence to particular treatment approaches and philosophies. As such, there is a need for designing intervention approaches for bilingual speakers, informed by lived experiences and with bilingualism considered at the start and the center of intervention design.
The current review highlights several open questions regarding treatment in bilingual PPA including 1) identifying the language that results in greatest within and between language effects, 2) how generalization effects may be maximized in bilingual PPA within and between languages, 3) if baseline characteristics predict treatment response, and, crucially, 4) how these effects may differ on the basis of bilingualism factors, language typology and sociocultural context. We note that although it is of theoretical and clinical importance to understand the bilingual factors that relate to greater within-language outcomes, from a life participation perspective, bilingual speakers often have a functional need to communicate in both languages. When a functional need exists to communicate in both languages, it is of critical importance that speech-language pathologists exhaust all avenues to provide intervention in both languages [149]. In some cases, this may require collaboration with/referral to other clinicians who speak the specific language pair of a given individual with PPA. Technological advances and collaborative models may also serve to facilitate broader access to bilingual services in PPA. As clinical researchers continue to study treatment effects in bilingual PPA, empirical evidence should be generated reporting the effects of collaborative models that could support development of different bilingual service delivery models.
Clinical implications and future directions
Linguistic bias has been documented in stroke-induced aphasia [150] and also holds true in the realm of aphasia caused by neurodegenerative disease. We observed that the majority of assessment and treatment studies reported English as one of the languages spoken by participants, with most studies being conducted in the U.S. As such, there is a need to increase representation of bilingual speakers from various sociocultural contexts, as well as those who speak a variety of language pairs. There is indeed evidence suggesting that the deficits that emerge may differ on the basis of the language(s) an individual speaks [63, 151–153]. Nevertheless, studies evaluating languages that are less typologically related are only beginning to emerge. In addition, it is unknown if cross-language transfer effects might be reduced in less typologically related languages relative to languages that are more closely related.
Common inclusion criteria in studies of primary progressive aphasia conducted in the United States, where the majority of studies were conducted in this review, include being a “native” English speaker, or having “high” English proficiency. First-hand, independent observations from our group also indicate that in other countries such as Spain and Mexico, individuals are often excluded from inclusion in PPA research if they do not speak the majority language(s) (e.g., German in Spain or Nahautl in Mexico). We strongly suspect that this is the case in many other countries and contexts as well. As such, many individuals who are bilingual are either excluded from the study of PPA or are included without characterization or query of their language history. It is important that researchers explore all avenues to include bilingual individuals in both research and clinical practice (e.g., collaborating with other researchers/clinicians who hold the relevant qualifications). When more lenient inclusionary criteria are adopted (with respect to language experience), it is important that the language history background of these passive (or potentially active) bilinguals are well-characterized to account for the unique attributes of the bilingual language system. Reporting these data in an open science framework will then allow for reviews and meta-analyses to be conducted with the indispensable factors needed to investigate bilingual PPA in its own right.
In the current review, articles considered for inclusion (at the screening stage) could have been written in several languages. One of our inclusion criteria included that abstracts or articles were available in English or Spanish. However, not a single study generated from our search was excluded due to the language it was written in. In the future, it will be important that researchers collaborate with those who speak a variety of languages to ensure representation in scoping and systematic reviews more broadly [154, 155].
Conclusion
The purpose of this scoping review was to synthesize the evidence regarding assessment and treatment practices in bilingual PPA, while also documenting the current definitions of bilingualism in PPA. Despite the fact that the majority of the world’s population is bilingual, studies documenting assessment methods and response to speech-language intervention are severely lacking. In order to maintain relevance in the healthcare marketplace, it is crucial that concerted efforts are made to develop sensitive assessment tools and effective treatment options that are culturally and linguistically tailored to bilingual speakers. The lack of appropriate assessments for bilingual PPA perpetuates delayed diagnosis and delayed access to intervention, when it is well established that early access to intervention and education is crucial for individuals living with PPA and their support networks. Individuals living with PPA and their families deserve equitable assessment and treatment options as this devastating condition impacts individuals who speak a variety of languages. The development of assessment and intervention options designed for bilingual PPA represents a crucial first step towards improving diagnosis and quality of life for individuals living with PPA.
Footnotes
ACKNOWLEDGMENTS
We thank Reagan Price for assistance with a secondary search and updating references.
FUNDING
This work was supported by the National Institute on Aging of the National Institute of Health R01AG080470 and the Alzheimer’s Association AACSF-22-972945. N.M.C. also received a scholarship from Hospital Clínic de Barcelona to complete her training in PPA assessment and intervention at UT Austin.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article and/or its supplementary material.