
Abstract
Background:
Degeneration of cholinergic basal forebrain (BF) neurons characterizes Alzheimer’s disease (AD). However, what role the BF plays in the dynamics of AD pathophysiology has not been investigated precisely.
Objective:
To investigate the baseline and longitudinal roles of BF along with core neuropathologies in AD.
Methods:
In this retrospective cohort study, we enrolled 113 subjects (38 amyloid [Aβ]-negative cognitively unimpaired, 6 Aβ-positive cognitively unimpaired, 39 with prodromal AD, and 30 with AD dementia) who performed brain MRI for BF volume and cortical thickness, 18F-florbetaben PET for Aβ, 18F-flortaucipir PET for tau, and detailed cognitive testing longitudinally. We investigated the baseline and longitudinal association of BF volume with Aβ and tau standardized uptake value ratio and cognition.
Results:
Cross-sectionally, lower BF volume was not independently associated with higher cortical Aβ, but it was associated with tau burden. Tau burden in the orbitofrontal, insular, lateral temporal, inferior temporo-occipital, and anterior cingulate cortices were associated with progressive BF atrophy. Lower BF volume was associated with faster Aβ accumulation, mainly in the prefrontal, anterior temporal, cingulate, and medial occipital cortices. BF volume was associated with progressive decline in language and memory functions regardless of baseline Aβ and tau burden.
Conclusions:
Tau deposition affected progressive BF atrophy, which in turn accelerated amyloid deposition, leading to a vicious cycle. Also, lower baseline BF volume independently predicted deterioration in cognitive function.
INTRODUCTION
Although amyloid plaques and neurofibrillary tangles are the two main neuropathological hallmarks of Alzheimer’s disease (AD), the selective and progressive loss of cholinergic neurons within the basal forebrain (BF) [1] characterises the early stages of AD and is associated with cognitive and functional decline [2, 3]. In AD, cortical and limbic cholinergic innervation is highly denervated [4], and cholinergic depletion has been shown to correlate with the severity of cognitive impairments in AD [5, 6]. The clinical improvement in patients with AD treated with acetylcholinesterase inhibitors [7] also indicates the importance of cholinergic dysfunction in AD [2, 3]. Therefore, degeneration of BF cholinergic neurons and cholinergic denervation of the cortical and limbic regions may play a crucial role in the pathogenesis of AD.
The cholinergic system of BF is closely related to AD pathology [2, 3]. Large amounts of neurofibrillary tangles are found in BF cholinergic neurons, even in the early stage of AD [8, 9], which may be followed by the degeneration of the cholinergic axons that it sends to the cerebral cortex [4]. Cross-sectional imaging studies have revealed that BF atrophy occurred in parallel with the development of tau pathology [10, 11]. A longitudinal study showed that tau pathology, as measured by a plasma biomarker, correlated with BF atrophy over time in cognitively intact older adults [12]. However, the longitudinal association between BF and tau has not been investigated in both directions using in vivo imaging biomarkers.
Amyloid-β (Aβ) pathology also has a close relationship with BF cholinergic system. Autopsy studies have reported a correlation between the loss of cholinergic axons and Aβ deposition in cognitively unimpaired subjects as well as in patients with AD [13, 14]. Experimentally, Aβ peptide modulates cholinergic neurotransmission and vice versa [15, 16]. Imaging analyses have also revealed that cross-sectionally, BF volume was associated with Aβ deposition in preclinical and prodromal AD [17]. Longitudinally, baseline amyloid positivity was associated with differentiated BF degeneration [18]. However, these studies have not considered the effect of Aβ and tau PET burden simultaneously.
Considering that BF atrophy predicted increased risk for conversion from mild cognitive impairment to dementia [19], we can assume that BF degeneration may accelerate the progression of AD independently or along with other AD-related pathologies. To figure out the role of BF cholinergic degeneration in AD pathological cascade, we investigated the association of BF volume with positron emission tomography (PET) measurements of Aβ and tau deposition as well as with cognitive dysfunction in the AD spectrum in both cross-sectional and longitudinal manners. In this study, we hypothesised that the BF volume is more closely related to tau burden than to Aβ burden when considering BF volume, tau burden, and Aβ burden simultaneously and that it plays an independent role in cognitive decline in AD.
METHOD
Participants
From January 2015 to September 2021, we made the dementia neuroimaging cohort which enrolled those who visited the memory disorder clinic of Gangnam Severance Hospital and healthy controls. At baseline, all subjects in the cohort completed brain magnetic resonance imaging (MRI), 18F-florbetaben (FBB) PET, 18F-flortaucipir (FTP) PET, and detailed neuropsychological tests within 6 months. Healthy controls and those who were positive in FBB PET underwent the same follow-up evaluations, with the mean intervals between the assessments of 2 to 3 years (Table 1). The two PET scans were performed at least 24 h apart to avoid being affected by the previous PET scan. Among them, we included 113 individuals and divided them into the 4 groups according to baseline Aβ positivity and detailed neuropsychological test; 30 patients with AD with dementia (DEM+), 39 patients with mild cognitive impairment due to AD (MCI+), 6 cognitive unimpaired and Aβ positive participants (CU+), and 38 cognitively unimpaired and Aβ negative participants (CU–). DEM+ was diagnosed based on ‘probable AD dementia with evidence of the Alzheimer’s pathophysiological process’ [20]. MCI+ was diagnosed based on the criteria of the National Institute on Aging-Alzheimer Association for ‘mild cognitive impairment due to AD with intermediate or high likelihood’ [21]. Aβ positivity was determined using cut-offs derived by Gaussian mixture modelling of FBB uptake [22]. Exclusion criteria were as follows: 1) initially atypical features, such as prominent language or executive dysfunction; 2) focal brain lesions, severe white matter hyperintensity [23], multiple lacunes, or hydrocephalus on brain MRI; 3) parkinsonism, including resting tremor, bradykinesia, rigidity, and postural instability; and 4) other major neurological, psychiatric, or metabolic diseases. Genotyping for apolipoprotein E (APOE) was performed for all subjects. The enrollment flowchart for the study participants is presented in Supplementary Figure 1.
Baseline clinical and neuropsychological characteristics of study subjects
Values are expressed as mean±standard deviation or number (percentage). p-values are the results of analyses of variance. The number in parentheses in each cognitive domain represents the possible maximum score. CDR-SB, Clinical Dementia Rating Sum-of-Boxes; CU–, amyloid-β negative and cognitive unimpaired; CU+, amyloid-β positive and cognitive unimpaired; DEM+, Alzheimer’s disease with dementia; K-MMSE, Korean version of the Mini-Mental State Examination; MCI+, mild cognitive impairment due to Alzheimer’s disease.
This study was approved by the institutional review board of Gangnam Severance Hospital (IRB No.: 3-2014-0286), and written informed consent was obtained from all participants. All procedures performed in this study were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments.
Acquisition of MRI and PET images
T1-weighted brain MR images were acquired on a 3.0 Tesla MR scanner (Discovery MR750, GE Medical Systems, Milwaukee, WI, USA) with a 3D-spoiled gradient-recalled sequence (repetition time = 8.28 ms, echo time = 1.6 to 11.0 ms, flip angle = 20°, 512×512 matrix, voxel spacing = 0.43×0.43×1 mm).
All FBB and FTP PET scans were performed using a Biograph mCT PET/CT scanner (Siemens Medical Solutions, Malvern, PA, USA) for 20 min at 80 and 90 min after 18F-florbetaben and 18F-flortaucipir injections, respectively. The two PET scans were done on separate days. Computed tomography (CT) images were acquired for attenuation correction prior to the PET scan. After the correction for attenuation and scatter, we reconstructed 3D PET images in 256×256×223 matrices with 1.591×1.591×1 mm voxel size by using the ordered-subsets expectation-maximization algorithm.
Image processing and quantitation of FBB and FTP PET
MR images were first processed using the FreeSurfer (version 5.3; Massachusetts General Hospital, Harvard Medical School; http://surfer.nmr.mgh.harvard.edu) software for creating subject-specific volumes of interest (VOIs) and mapping the PET uptake on surface structures as described in our previous stud [24]. In brief, the MR images were segmented into grey and white matter, and then the cortical grey and white matter surfaces were reconstructed. By using the anatomical information and curvature of surface, cortical and subcortical regions were segmented into 112 regions. After merging anatomically related regions across hemispheres, subject-specific composite VOI mask images including 25 cortical regions were created within the FreeSurfer space (256×256×256 matrix with 1 mm isovoxels).
Statistical parametric mapping (version 12; Wellcome Trust Centre for Neuroimaging) and in-house software implemented in MATLAB (version R2019b; MathWorks, Natick, MA, USA) were used to process the PET images and measure regional uptake. PET images were co-registered to individual MR images in the FreeSurfer space. By using the cortical and subcortical segments obtained from FreeSurfer, PET images were corrected for partial volume effects (PVE) with the region-based voxel-wise method [25]. For creating standardized uptake value ratio (SUVR) images, we used the cerebellar crus median obtained by overlaying the template VOI for the cerebellar crus on the spatially normalized PET images [26]. Finally, PVE-corrected regional SUVR values were measured by overlaying the subject-specific composite VOI.
We used meta-regions specific for FBB and FTP PET to measure the individual representative Aβ and tau burden: FBBMETA = superior, middle, and inferior frontal, orbitofrontal, superior and inferior parietal, supramarginal, precuneus, superior, middle, and inferior temporal, fusiform, anterior and posterior cingulate cortices [27], and FTPMETA = entorhinal, amygdala, parahippocampal, fusiform, and inferior and middle temporal cortices [28].
For vertex-wise analyses across the whole cortex, cortical uptake at the mid-point between the grey and white matter surface was mapped on the white matter surface and then corrected for PVE and converted to SUVR surface maps. PVE-corrected surface SUVR maps were spatially normalized and finally smoothed on a 2D surface using a Gaussian kernel with 8-mm full width at half-maximum.
Measuring BF volume
For measuring the BF volume, we used a standard BF VOI, which had been previously designed with postmortem MRI and cytoarchitectonic maps of BF cholinergic nuclei on autopsy brains by transferring to standard Montreal Neurological Institute (MNI) space using a diffeomorphic anatomical registration through exponentiated lie algebra (DARTEL) non-linear registration technique [29]. Likewise, all T1-weighted MR images in this study were segmented into five tissue classes (grey and white matter, cerebrospinal fluid, skull, and scalp), and then, we obtained gray matter density map by transferring gray matter segments to MNI space using an in-house DARTEL template and a DARTEL toolbox in SPM12. Finally, the BF volume was measured by overlaying the standard BF VOI on individual grey matter density map. We used the entire volume of the BF, including all cholinergic subdivisions, as a proxy for overall BF cholinergic system integrity.
Neuropsychological testing
All subjects underwent a standardized and comprehensive neuropsychological battery of tests called the Seoul Neuropsychological Screening Battery (SNSB) [30], which contained tests for attention, language, visuospatial, memory, and executive functions. We included the following tests in the analyses: the digit span forward and backward for the attention domain; the Korean version of the Boston Naming Test (K-BNT) for the language domain; copying item of the Rey-Osterrieth Complex Figure Test (RCFT) for the visuospatial domain; immediate recall, 20-min delayed recall, and recognition items of the RCFT and Seoul Verbal Learning Test for the memory domain; and the semantic and phonemic Controlled Oral Word Association Test and Stroop color reading test for the executive domain.
A composite score was calculated for each cognitive domain by the sum of the raw scores using the following equation [31]: the digit span forward score+the digit span backward score for the attention domain, ranging from 0 to 17; the K-BNT score for the language domain, ranging from 0 to 60; the RCFT copy score for the visuospatial domain, ranging from 0 to 36; [SVLT immediate recall score + SVLT delayed recall score + (SVLT recognition score – 12) + RCFT immediate recall + RCFT delayed recall + (RCFT recognition score – 12)] for the memory domain, ranging from 0 to 144; and (COWAT animal score + COWAT total phonemic score/3 + Stroop color reading score/5) for the executive domain, ranging from 0 to 55. Global cognitive function was assessed using the Korean version of the Mini-Mental State Examination (K-MMSE) and Clinical Dementia Rating Sum of Boxes (CDR-SB).
Statistical analyses
The baseline FBBMETA, FTPMETA, and BF volume of the study participants were compared among the groups. The BF volume was analyzed using an analysis of variance since it was normally distributed, while the FBBMETA and FTPMETA were analyzed using a Kruskal-Wallis test. The post-hoc pairwise group comparison were performed at the same level of significance without adjustment.
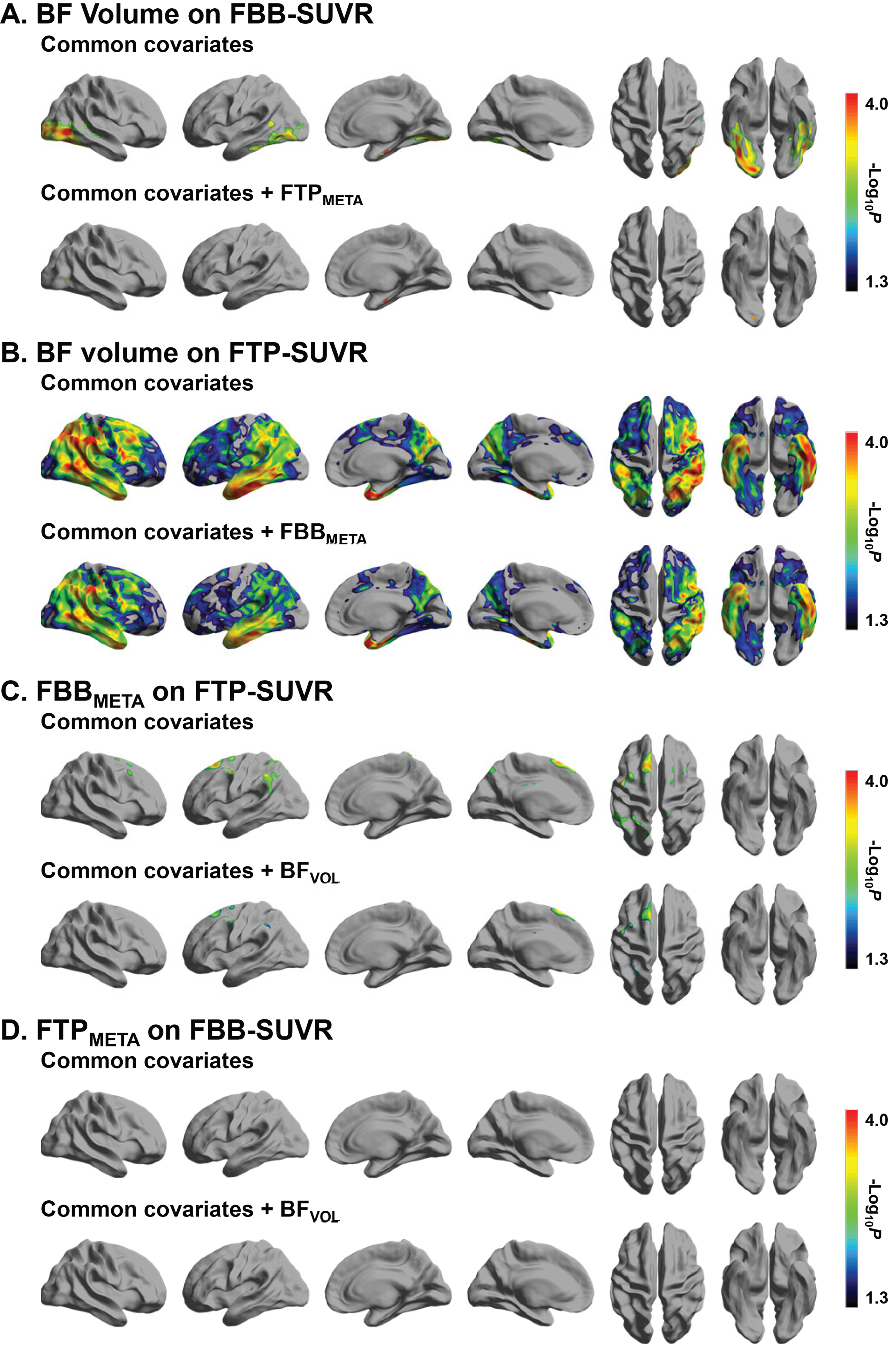
General linear models were used to investigate the baseline association between the BF volume and Aβ and tau burden. We mapped the effect of BF volume of cortical FBB- and FTP-SUVR, the effect of FBBMETA on cortical FTP-SUVR, and the effect of FTPMETA on cortical FBB-SUVR, after adjustment for age, sex, years of education, presence of the APOE ɛ4 allele, total intracranial volume (TIV), and disease group as common covariates. In particular, we included disease group as one of the covariates since we included subjects spanning from CU–to DEM+, and their difference in disease severity should be controlled to avoid spurious associations between variables. Moreover, when investigating the association between the two variables, the other variable was further included as a covariate.
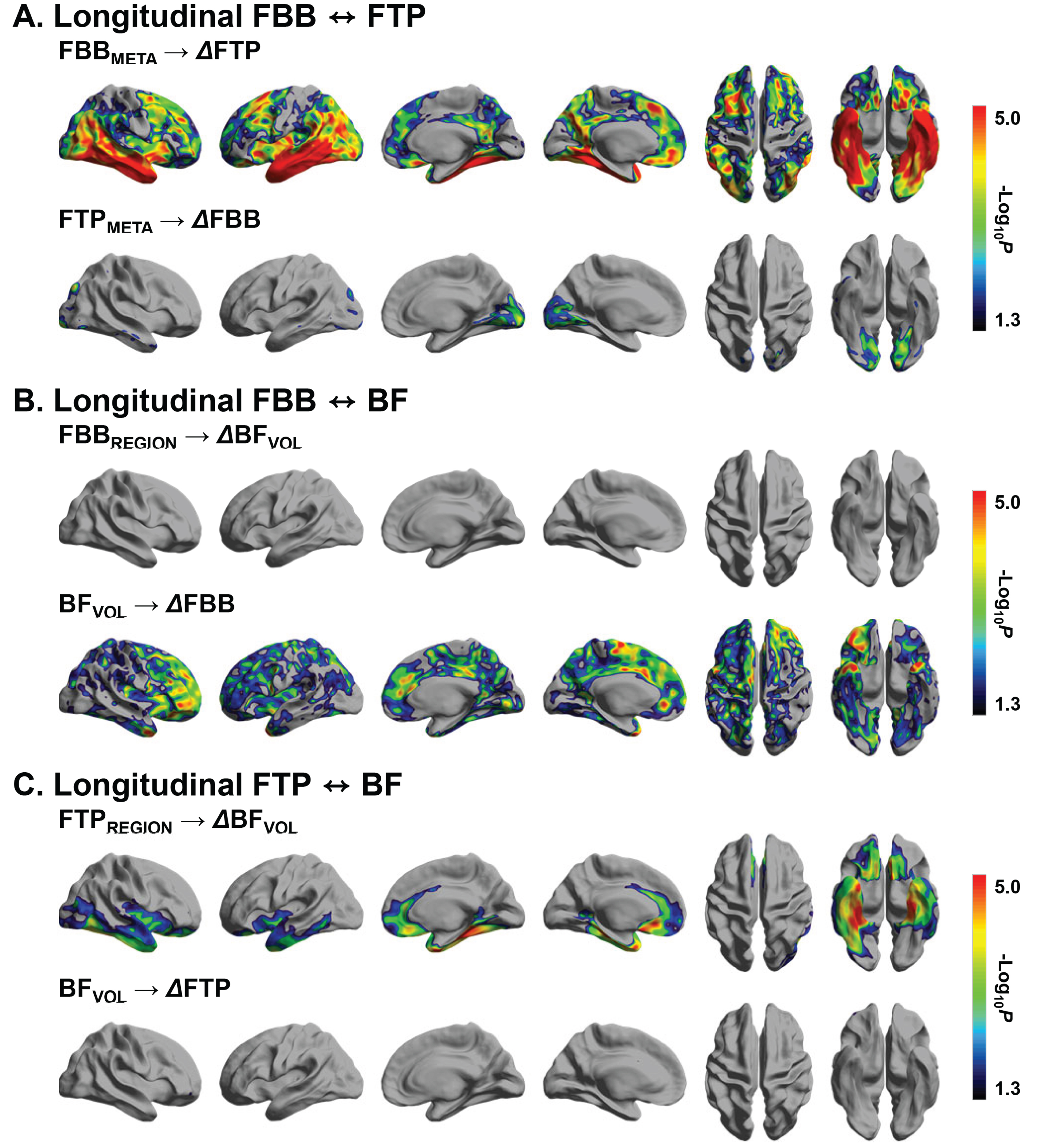
Using R package ‘lme4’, linear mixed models were conducted to examine the effect of baseline BF volume and Aβ and tau accumulation on longitudinal changes in other variables over time, using random effects terms for intercept and slope over time, nested within individuals. We mapped the effect of baseline FBBMETA on changes in cortical FTP-SUVR, baseline FTPMETA on changes in cortical FBB-SUVR baseline BF volume on changes in cortical FBB- and FTP-SUVR, and baseline cortical FBB- and FTP-SUVR on changes in BF volume. When investigating the association between the two variables, we adjusted for the baseline value of the other variable and its interaction term with time as well as the common covariates. We used the intervals between MR scans as a time variable consistently for all analyses.
For example (baseline BF volume on longitudinal FBB-SUVR):
General linear model and linear mixed models were used to investigate the association of the baseline BF volume and Aβ and tau burden with the baseline and longitudinal composite score in each cognitive domain. In the base model, the baseline BF volume, FBBMETA, or FTPMETA was included as a predictor, respectively with the adjustment for the common covariates. In the extended model, the baseline BF volume, FBBMETA, and FTPMETA were included simultaneously in the general linear model and their interaction term with time were also included in the linear mixed model.
For example (baseline BF volume on longitudinal memory function):
SPSS software 24 (IBM, Armonk, NY) and R software package (version 4.2.1, http://www.r-project.org/) were used for statistical analyses. In imaging analyses, a vertex-wise false discovery rate (FDR)-corrected p-value < 0.05 was considered statistically significant, and in the analyses investigating the effect of baseline Aβ burden, tau burden, and BF volume on cognitive function, FDR-corrected p < 0.05 across the five cognitive domains was considered statistically significant.
RESULTS
Clinical, cognitive, and imaging characteristics of study subject
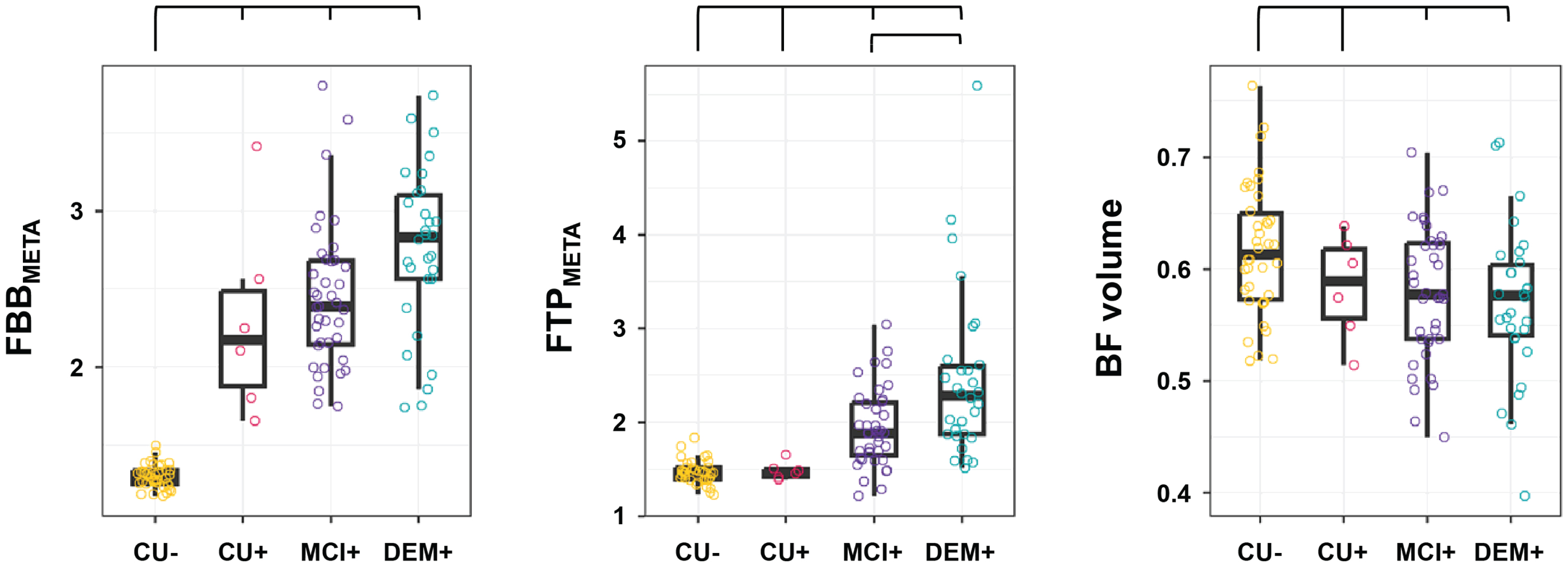
Table 1 describes the baseline demographic characteristics of the participants. As for the imaging findings (Fig. 1), the CU–group had lower FBBMETA than the other groups. All groups had difference FTPMETA between each other except for the CU–and CU+ groups. Regarding BF, The CU–and CU+ group had lower BF volume than the MCI+ and DEM+ groups, respectively, while there were no differences between the CU–and CU+ and between MCI+ and DEM+. Sixty subjects repeated the same assessment once, and 53 did so twice. The average time interval between baseline and last follow-up assessments was 3.6±1.5 years. Detailed data of interval between the MRI, FBB PET, FTP PET, and neuropsychological test are described in Table 1.
Baseline relationship between Aβ burden, tau burden, and BF volume
A lower BF volume was associated with an increase in FBB-SUVR in the occipital cortex, while the area of correlation disappeared after further controlling for FTPMETA (Fig. 2A). A lower BF volume was associated with an increased FTP-SUVR in widespread cortical regions, except the primary motor and sensory, medial frontal and occipital cortices, most prominently in the lateral parieto-temporal, inferior temporal, and lateral prefrontal regions (Fig. 2B). Even after further controlling for FBBMETA, the area of correlation remained largely unchanged. Higher FBBMETA was associated with increased FTP-SUVR in the superior frontal and parietal regions regardless of the covariates (Fig. 2C). Higher FTPMETA was not associated with increased cortical FTP-SUVR regardless of the covariates (Fig. 2D).
Longitudinal relationship between Aβ burden, tau burden, and BF volume
A higher baseline FBBMETA was associated with a faster increase in FTP-SUVR in cortical regions where tau accumulates prominently in AD, while a higher baseline FTPMETA was also associated with a faster increase in FBB-SUVR, mainly in the medial occipital areas (Fig. 3A). A higher baseline FBB-SUVR in any region was not associated with faster BF atrophy, while baseline BF volume was associated with a faster increase in FBB-SUVR in widespread cortical regions, except the lateral parieto-temporal and medial and lateral occipital cortices (Fig. 3B). A higher baseline FTP-SUVR in the orbitofrontal, insular, lateral temporal, inferior temporo-occipital, and anterior cingulate cortices was associated with faster BF atrophy, while baseline BF volume was not associated with cortical changes in FTP-SUVR over time (Fig. 3C).
Association of baseline Aβ burden, tau burden, and BF volume with baseline and longitudinal cognitive function
Regarding the baseline association, the language, memory, and executive composite scores were negatively correlated with FBBMETA and FTPMETA and positively correlated with BF volume, while the visuospatial composite score was negatively correlated only with FTPMETA (Table 2). The significance of all items survived after the FDR correction. The attention composite score did not correlate with any imaging biomarkers. In the extended model, FBBMETA was independently associated with the language and memory composite scores, and FTPMETA with the visuospatial, memory, and executive composite scores, while BF volume was not associated with any cognitive domain composite score. After the FDR correction, the association of FTPMETA with cognition disappeared.
The effect of baseline Aβ burden, tau burden, and BF volume on longitudinal cognitive function
Data are the results of multivariate linear regression models or linear mixed models on baseline or longitudinal composite z-score in each cognitive domain. In the base model, baseline age, sex, years of education, disease group, baseline total intracranial volume, and presence of APOE ɛ4 allele were adjusted as covariates, while in the extended model, in addition to the above covariates, baseline FBBMETA, FTPMETA, BF volume (BFVOL), and their interaction with time were included simultaneously. Asterisk indicates statistical significance after correction for 15 analyses (3 variables×5 cognitive domains) in the base model and for 5 analyses (5 cognitive domains) in the extended model.
Regarding the longitudinal association, baseline FBBMETA was associated with faster decline in the attention, language, and memory function, and baseline FTPMETA was associated with faster decline in all cognitive function, while BF volume was associated with faster decline in the language and memory function. The significance of all items survived after the FDR correction. In the extended model, baseline FBBMETA was not associated with decline in any cognitive domain composite score, while FTPMETA was associated with faster decline in the language and visuospatial function, and BF volume was associated with faster decline in the language and memory function. After the FDR correction, the association of BF volume with cognition disappeared.
Sensitivity analyses
Sensitivity analyses were also conducted to see whether the association between Aβ, tau, and BF remained still after changing the participants or covariates. First, among the common covariates, we changed the disease group to total MMSE score and examined their baseline and longitudinal associations (Supplementary Figures 2 and 3). Second, we changed the participant into those who were Aβ only (CU+, MCI+, and DEM+) while controlling for the same covariates in the original analyses (Supplementary Figures 4 and 5). In both analyses, the main results were not largely changed after full adjustment.
DISCUSSION
We explored the role of BF volume in the context of the AD pathological cascade using imaging biomarkers and detailed neuropsychological testing. The major findings of this study were as follows: First, cross-sectionally, lower BF volume was not independently associated with Aβ burden but with tau burden in widespread cortical area. Second, tau burden in the orbitofrontal, insular, lateral temporal, inferior temporo-occipital, and anterior cingulate cortices were associated with progressive BF atrophy, while lower BF volume was not associated with faster tau accumulation. Third, lower BF volume was associated with faster Aβ accumulation, mainly in the prefrontal, anterior temporal, and cingulate cortices, while Aβ burden was not associated with faster BF atrophy. Fourth, independent of amyloid and tau burden, BF volume was not associated with baseline cognitive function but with progressive decline in language and memory functions, although the significance disappeared after the FDR correction. In summary, BF atrophy follows tau deposition and predicts longitudinal Aβ deposition and cognitive dysfunction in AD.
Independent of the Aβ burden, cortical tau pathology was significantly associated with baseline and longitudinal BF atrophy in AD. To the best of our knowledge, our study is the first to assess the association between BF volume and tau pathology measured by PET. This finding is consistent with previous pathological studies demonstrating that BF is one of the brain regions most susceptible to tau pathology [8, 9]. Notably, tau cytopathology in the BF was observed in elderly with no objective cognitive impairment, as well as in patients with mild cognitive impairment [8]. Imaging studies elucidated that tau pathology initiates with BF degeneration [11], which was an upstream event of entorhinal degeneration [32]. Longitudinal data in our study found that tau accumulation in the intermediate Braak III–IV [24] regions was a strong and independent predictor of BF atrophy over time. Moreover, cross-sectional data in our study revealed that lower BF volume was correlated with tau burden in widespread cortical regions that receive cholinergic innervation from the posterior and intermediate parts of the nucleus basalis of Meynert [33]. Given the evidence of a caudorostral pattern of neuronal loss in the nucleus basalis of Meynert in AD [33], we can assume that degeneration of BF cholinergic neurons from the posterior part is closely associated with tau deposition in the corresponding cortical areas. This interpretation requires caution because BF atrophy differs from BF cholinergic denervation, and baseline BF volume did not predict cortical tau accumulation in our study. Considering the longitudinal data, we can infer that tau accumulation precedes BF atrophy, correlates well with BF atrophy, and accelerates BF atrophy.
The cross-sectional association between Aβ pathology and BF disappeared after controlling for tau pathology, and lower BF volume predicted progressive accumulation of Aβ. The BF cholinergic system is not an early and prominent site of Aβ deposition [34]. In a neuropathological study, there was almost no correlation between the loss of cholinergic fibers and the density of Aβ deposits [35]. In our study, the area of correlation between BF volume and Aβ deposition completely disappeared after further adjustment for tau burden. These results suggested that Aβ may not directly trigger BF degeneration. Contrary to our results, previous experiments have shown that Aβ alters cholinergic transmission and induces cholinergic hypofunction directly [15]. The discrepancy is perhaps due to the facts that we did not measure BF cholinergic function, but rather BF volume, and controlled for tau burden. Intriguingly, the baseline BF volume was associated with faster accumulation of Aβ in widespread cortical regions, especially in the anterior temporal and prefrontal regions. This observation extends previous findings of cross-sectional associations between BF volume and cortical Aβ burden [17, 36], and is consistent with experimental animal studies that demonstrated that cholinergic deficits exacerbated Aβ deposition [16, 37]. Cholinesterase inhibitors influence Aβ precursor protein processing and Aβ neurotoxicity [38]. Therefore, it can be inferred that degeneration of the BF would accelerate the accumulation of Aβ, thus resulting in a vicious cycle of Aβ deposition, tau deposition, and cholinergic dysfunction (Fig. 4).
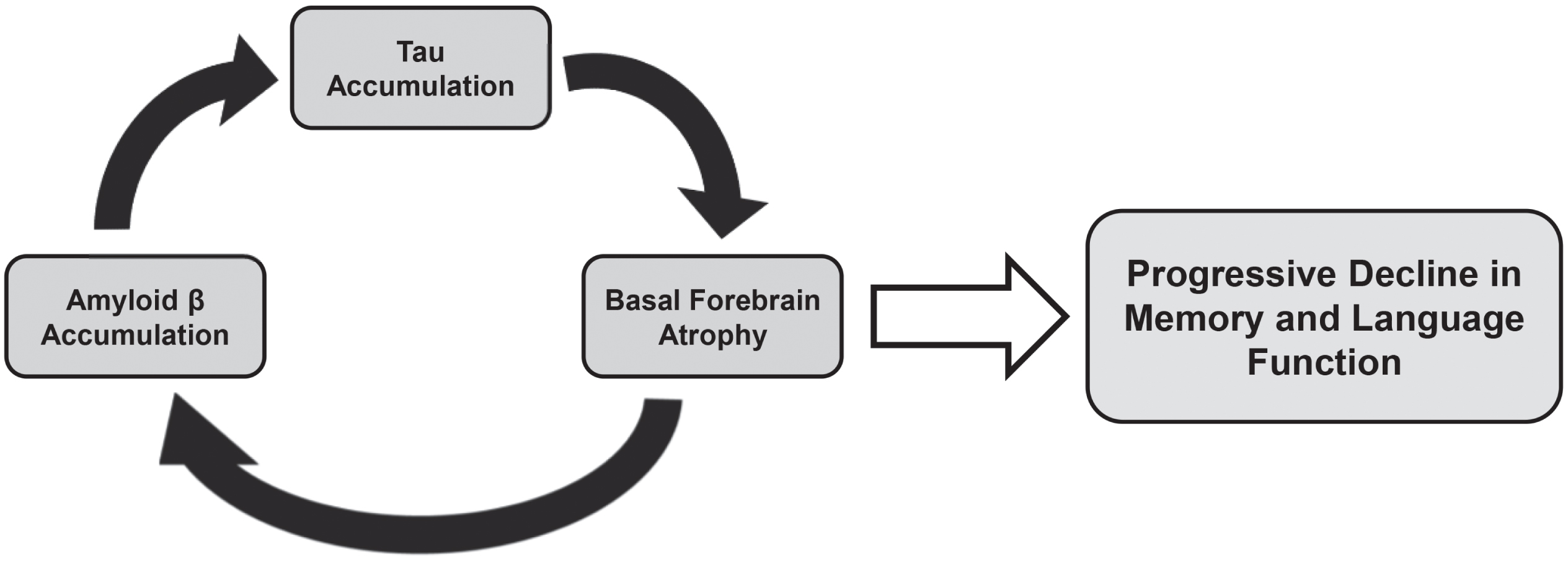
Schematic representation of the proposed role of BF atrophy in Alzheimer’s disease.
After controlling for the effect of Aβ and tau burden, we found that BF volume was not independently associated with baseline cognitive dysfunction but with longitudinal cognitive decline in memory and language function, although the significance disappeared after the FDR correction. Cross sectional and animal studies figured out that BF was associated with memory, attention, and executive function [39, 40]. However, these studies did not consider the effect of Aβ and tau burden simultaneously. Consistent with our finding, longitudinal studies showed a temporal association of preceding BF degeneration with subsequent entorhinal pathology and memory impairment [41]. BF volume, but not hippocampal volume, was a predictor of cognitive decline in AD [42]. Therefore, we can infer that degeneration of the BF which has widespread projection to cortical and limbic regions would have a strong and continuous effect on AD-related cognitive decline. Considering the role of reduced BF volume in driving further Aβ pathology in our study, we can also assume that a vicious cycle of AD-related neuropathological process may exacerbate progressive cognitive decline (Fig. 4). The association between BF cholinergic system and language function has not been elucidated well. However, reduced BF volume in patients with primary progressive aphasia suggested that BF is crucial for language function [43, 44]. Additional supporting data are required to confirm the effect of cholinergic dysfunction and progressive decline in language function.
This study had several limitations. First, a reduced BF volume may not directly reflect cholinergic dysfunction or denervation. Functional imaging studies, such as PET of cholinergic neurotransmission, are required to measure cholinergic dysfunction in relation to AD pathological cascade. Second, despite using a histology-informed cytoarchitectonic map of the BF cholinergic system, measuring BF volume using this template-based method is likely to include non-cholinergic neuron populations. Third, we used the total BF volume in this study, and future studies should perform topographic analyses according to subregional BF volumes to investigate the differential roles of regional cholinergic projections in AD pathogenesis in more detail. Fourth, the number of subjects in the CU+group was too small (13.6%), which was similar to the prevalence in another study conducted in South Korea [45]. That is, the low prevalence of CU+in this study may be attributed to the ethnic difference. Last, the significance of the effect of baseline BF volume on longitudinal memory and language dysfunction disappeared after correction for multiple analyses. Caution is required to interpret the independent association between the BF volume and cognitive decline.
Using in vivo neuroimaging modalities and detailed neuropsychological tests, we elucidated the role of BF volume in the AD pathological cascade. This study suggests that BF cholinergic function should be considered together with Aβ and tau burden when assessing patients with AD. It also suggests that BF cholinergic function plays a central role in the AD pathological cascade, indicating the potential value of cholinergic therapy starting as early as possible during the pathophysiological spectrum of AD.
AUTHORS CONTRIBUTIONS
Han Soo Yoo (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Software; Visualization; Writing – original draft; Writing – review & editing); Han-Kyeol Kim (Data curation; Formal analysis; Investigation; Writing – review & editing); Jae-Hoon Lee (Investigation; Resources; Supervision; Writing – review & editing); Joong-Hyun Chun (Investigation; Resources; Validation); Hye Sun Lee (Data curation; Methodology; Software; Writing – review & editing); Michel Grothe (Methodology; Validation; Writing – original draft; Writing – review & editing); Stefan Teipel (Methodology; Validation; Writing – original draft; Writing – review & editing); Enrica Cavedo (Validation; Writing – original draft; Writing – review & editing); Andrea Vergallo (Validation; Writing – original draft; Writing – review & editing); Harald Hampel (Methodology; Supervision; Validation; Writing – original draft; Writing – review & editing); Young Hoon Ryu (Conceptualization; Investigation; Methodology; Project administration; Supervision; Writing – review & editing); Hanna Cho (Data curation; Funding acquisition; Project administration; Resources; Supervision; Writing – original draft; Writing – review & editing); Chul Hyoung Lyoo (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Visualization; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We thank all the participants for their involvement in this study.
FUNDING
This research was supported by a grant from a faculty research grant of Yonsei University College of Medicine (6-2018-0068, 6-2021-0094), grants of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI) funded by the Ministry of Health & Welfare, Republic of Korea (HI18C1159 & HU20C0164), a 2020 Research Grant of Gangnam Severance Hospital Research Committee, and a grant of Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF2020R1F1A1076154 & NRF2018R1D1A1B07049386). MJG is supported by the “Miguel Servet” program [CP19/00031] and a research grant [PI20/00613] of the Instituto de Salud Carlos III-Fondo Europeo de Desarrollo Regional (ISCIII-FEDER).
CONFLICT OF INTEREST
H.H. has no conflict of interest, but disclose the followings: H.H. is an employee of Eisai Inc. This work has been done during his academic appointment at Sorbonne University in Paris, France. He serves as Reviewing Editor for the Journal Alzheimer’s and Dementia, as Editorial Board Member of the Journal of Prevention of Alzheimer’s Disease (JPAD), and as Scientific Committee Member of the annual Clinical Trials on Alzheimer’s Disease (CTAD) conference. He is inventor of 11 patents and has received no royalties: (i) In Vitro Multiparameter Determination Method for The Diagnosis and Early Diagnosis of Neurodegenerative Disorders Patent Number: 8916388; (ii) In Vitro Procedure for Diagnosis and Early Diagnosis of Neurodegenerative Diseases Patent Number: 8298784; (iii) Neurodegenerative Markers for Psychiatric Conditions Publication Number: 20120196300; (iv) In Vitro Multiparameter Determination Method for The Diagnosis and Early Diagnosis of Neurodegenerative Disorders Publication Number: 20100062463; (v) In Vitro Method for The Diagnosis and Early Diagnosis of Neurodegenerative Disorders Publication Number: 20100035286; (vi) In Vitro Procedure for Diagnosis and Early Diagnosis of Neurodegenerative Diseases Publication Number: 20090263822; (vii) In Vitro Method for The Diagnosis of Neurodegenerative Diseases Patent Number: 7547553; (viii) CSF Diagnostic in Vitro Method for Diagnosis of Dementias and Neuroinflammatory Diseases Publication Number: 20080206797; (ix) In Vitro Method for The Diagnosis of Neurodegenerative Diseases Publication Number: 20080199966; (x) Neurodegenerative Markers for Psychiatric Conditions Publication Number: 20080131921; and (xi) Method for diagnosis of dementias and neuroinflammatory diseases based on an increased level of procalcitonin in cerebrospinal fluid: Publication number: United States Patent 10921330. However, H.H. was not involved in the peer-review process nor had access to any information regarding its peer-review. All other authors have no conflict of interest to report.
None of authors has any conflict of interest to disclose.
DATA AVAILABILITY
Anonymized data used within the article can be shared on reasonable request from qualified investigators.