
Abstract
Background:
Accumulating evidence has demonstrated that hyperglycemia is a possible risk factor for mild cognitive impairment or Alzheimer’s disease. Diabetic retinopathy (DR) has been identified as a risk factor for dementia in patients with diabetes.
Objective:
This study aimed to investigate the causal relationships between DR and brain structure, cognitive function, and dementia.
Methods:
We performed bidirectional two-sample Mendelian randomization for DR, brain structure, cognitive function, and dementia using the inverse-variance weighted method.
Results:
Inverse-variance weighted analysis showed the association of DR with vascular dementia (OR = 1.68, 95% CI: 1.01–2.82), and dementia was significantly associated with the increased risk of non-proliferative DR (NPDR) (OR = 1.76, 95% CI: 1.04–2.98). Furthermore, better cognitive performance was significantly associated with a reduced risk of NPDR (OR = 0.85, 95% CI: 0.74–0.98). No association was observed between DR and brain structure.
Conclusions:
These findings suggest that the association of DR with vascular dementia. The reciprocal effect of cognitive performance and dementia on NPDR risk highlights the potential benefits of dementia prevention for reducing the burden of DR.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) and all-cause dementia are major public health issues [1]. Currently, dementia affects more than 46 million older adults worldwide; experts predict that the figure will be nearly tripled 2050 [2, 3]. Accumulating evidence has demonstrated that hyperglycemia is a possible risk factor for mild cognitive impairment or AD [4–6]. Numerous hypotheses have been proposed to explain why patients with diabetes have a high prevalence of dementia, including the direct consequences of both chronic and acute hyperglycemia, cerebral microvascular dysfunction, and cerebral insulin resistance [7–9]. Diabetic retinopathy (DR) is a common complication of diabetes and was suggested to be associated with dementia. Studies have showed that DR shared similar pathological processes, including progressive neurodegeneration, special amyloid-β deposits, and chronic microvascular disorder [10]. Furthermore, a few studies have identified DR as a risk factor for dementia in individuals with diabetes. A retrospective study [11] demonstrated a higher incidence of dementia/AD in DR patients after accounting for diabetes severity, and two meta-analyses reported consistent results [12, 13]. However, there are concerns about the impact of brain structure, cognition, and dementia on the occurrence of DR [14], and no conclusive evidence is available on the relationship between brain structure, cognition, dementia, and DR.
Mendelian randomization (MR) allows for a strong causal inference between a risk factor and disease by employing genetic variants as instrumental variables [15]. Compared with standard observational studies, MR is less prone to bias caused by confounders and reverse causation because alleles are randomly assigned at birth and are not affected by diseases [16]. Exploration of the bidirectional relationship between DR and dementia/AD may be particularly valuable for improving the scientific understanding of the shared pathophysiology between the brain and retina. Previous studies have relied primarily on observational designs to elucidate the relationship between DR and dementia/AD. The MR approach, which has not been previously applied to this specific association, is a powerful tool for making causal inferences. Therefore, in this study, we aimed to use MR analysis to evaluate the bidirectional causal association between DR and dementia/AD.
MATERIALS AND METHODS
Study design and data sources
We conducted a comprehensive bidirectional MR analysis to investigate the relationships between DR and both dementia and AD. In addition, we examined the effects of DR on cognitive performance. Our analysis was also extended to explore the association between DR and cerebral structure, specifically focusing on surface areas and mean thicknesses across 34 cortical regions, as defined by the Desikan–Killiany atlas, as well as hippocampal volume. Our analysis was based on three core assumptions: instrumental variants 1) strongly predict exposure, 2) are not associated with known confounders, and 3) influence outcomes only through exposure. DR and its subtype statistical data were obtained from a genome-wide association study (GWAS) of DR using liability threshold modeling of diabetes and glycemic control [17]. This study included four DR GWAS datasets accounting for the duration of diabetes and glycemic control (adjusted model), DR versus no DR, proliferative diabetic retinopathy (PDR) versus no PDR, non-proliferative diabetic retinopathy (NPDR) versus no DR, PDR versus no DR, and four DR GWAS datasets without adjustment (no adjusted model). The GWAS data contained the following cohorts: Age, Gene/Environment, Susceptibility-Reykjavik Study (AGES), Atherosclerosis Risk in Communities Study (ARIC), Australian Genetics of Diabetic Retinopathy Study (AUST), Blue Mountains Eye Study (BMES), Cardiovascular Health Study (CHS), Family Study of Nephropathy and Diabetes-Eye (FIND-Eye), and Multiethnic Study of Atherosclerosis (MESA). None of these cohorts were covered by the outcome sample. Dementia/AD statistical data were obtained from FinnGen (adjusted for age, sex, and top principal components), the International Genomics of Alzheimer’s Project (IGAP) (adjusted for age, sex, and principal components), the Alzheimer’s Disease Genetics Consortium (ADGC) (adjusted for age at evaluation, sex, and principal components), and other recently published GWAS datasets. Statistical data on cerebral structure were obtained from the ENIGMA Consortia (49) (adjusted for age, sex, total intracranial volume, site, or scanner effects to account for multicentric data collection and principal components) (Supplementary Table 1). The protocols of the original studies were approved by the institutional review boards of the participating sites, and informed consent was obtained from all participants.
Mendelian randomization
Using the related GWAS datasets, we employed two-sample MR to investigate the bidirectional relationship between DR/DR subtypes and dementia/AD. To select eligible instrumental variants, we extracted the SNPs associated with dementia/AD at genome-wide significance (based on p < 5×10–8) and DR/subtype at genome-wide significance (based on p < 5×10–6) by considering the relatively small sample of the DR GWAS dataset. To ensure independence among the genetic instruments, we applied linkage disequilibrium (LD) clumping with a clumping distance cutoff of 10000, and an r2 cutoff of 0.001. This was based on a threshold of r2 <0.001 and genotype data from European individuals enrolled in the 1000 Genomes Project as the reference panel [18]. In line with the previous neuropsychiatric MR studies [19, 20] evaluating exposures with few GWAS SNPs, we used a p-value threshold of 5×10–6 to select cortical surface area and thickness instruments. We then extracted the same SNPs from the outcome GWAS results. SNPs absent from the outcome dataset were replaced with matching proxy SNPs (r2 >0.8) when available. We examined the GWAS catalog and eliminated SNPs that were allegedly linked to potential confounders to prevent deviations from the MR assumptions (other types of retinopathy, cerebral disease, and cardiovascular disease) in both DR and dementia/AD [21–23]. In the AD analysis, we excluded SNPs linked to sleep, depression, and education level, all of which may have independent effects on the risk of developing AD [24]. Considering apolipoprotein E (APOE), which may affect the risk of developing dementia/AD, SNPs associated with APOE or SNPs with LD (r2 > 0.1) in ɛ2/ɛ3/ɛ4 APOE genotypes were excluded based on the European 1000 Genomes dataset [25] and the LD link website (https://analysistools.cancer.gov/LDlink/?tab=home) by choosing a European ancestor. Palindromic SNPs with intermediate allele frequencies were also excluded. In addition, we excluded SNPs associated with the outcome (p < 0.01) from the original GWAS. Finally, we assessed the instrument accuracy by deriving F-statistics. Instrumental SNPs with an F-statistic > 10 were excluded because, a low F-statistic suggests a weak instrument bias [26].
Sensitivity analyses
We selected five MR approaches that make different assumptions regarding horizontal pleiotropy to assess the robustness of the results, including the inverse-variance weighted (IVW) method, MR-Egger method, weighted median method, simple mode, and weighted mode estimators. Heterogeneity and pleiotropy were used to determine significant horizontal pleiotropy. Furthermore, we used the MR-PRESSO global test to detect the outliers and subsequently applied distortion tests [27] to determine whether the horizontal pleiotropy decayed after eliminating the outliers. Additionally, we repeated the analyses to explore whether excluding more control participants with dementia would lead to better results.
Statistical methods and power calculation
Analyses were performed using PLINK1.9 and R version 4.2.2, using the two-sample MR, MR-base, Plink2R, MR-PRESSO, and MR packages [28]. As the main statistical technique, we employed fixed-effect IVW to estimate the causal effects. To test the robustness of our results, we estimated the horizontal pleiotropy using four alternative methods: MR-Egger, weighted median, simple mode, and weighted mode estimators. Since we included > 20 cognitive function and dementia-related outcome variables into the analyses, we mainly interpreted our results depending on a two-sided p-value of 0.05 (two sides) to avoid false negative results. Therefore, we demonstrate the strength of the evidence based on the estimated size, 95% CI, and p-value, and report a standard p-value threshold of 0.05. We conducted power calculations for the MR analysis using an online tool (https://sb452.shinyapps.io/power/). We had 20% power to detect an odds ratio (OR) of 1.5 for DR on AD risk, and 83% power to detect an odds ratio of 1.3 for dementia/AD on DR risk.
RESULTS
The primary bidirectional MR studies comprised 3,049 and 488,285 individuals in the DR GWAS and dementia/AD GWAS datasets, respectively. The patients in the included cohorts were of European ancestry. Their ages ranged from 38–69 years, and 48% –54% of the participants were female. We selected 8,11,3,22 SNPs for DR versus no DR, PDR versus no PDR, NPDR versus no DR, and PDR versus no DR, respectively (after excluding one, one, zero, and two SNPs associated with potential confounders, respectively). We selected 14 SNPs associated with AD (after excluding two SNPs associated with potential confounders). Additional information on the selection and exclusion of SNPs is provided in the Supplementary Material (detailed data). Summary-level statistics for the datasets are available in Supplementary Table 1.
Association between genetically predicted DR and dementia, cognitive performance, and cerebral structure
Dementia and AD
Using the IVW method, we found no causal effect of DR on AD, nor did we find causal effect of subtypes of DR on AD (Fig. 1, Supplementary Table 2). We found nominal causal effects of DR on higher risk of vascular dementia (IVW: OR = 1.68, 95% CI: 1.01–2.82, p = 0.046; MR Egger: OR = 0.44, 95% CI: 0.12–1.61, p = 0.26) (Supplementary Table 2, Fig. 5). We found no causal effect of the DR subtype (PDR and NPDR) on dementia/AD (Fig. 1, Supplementary Table 2).
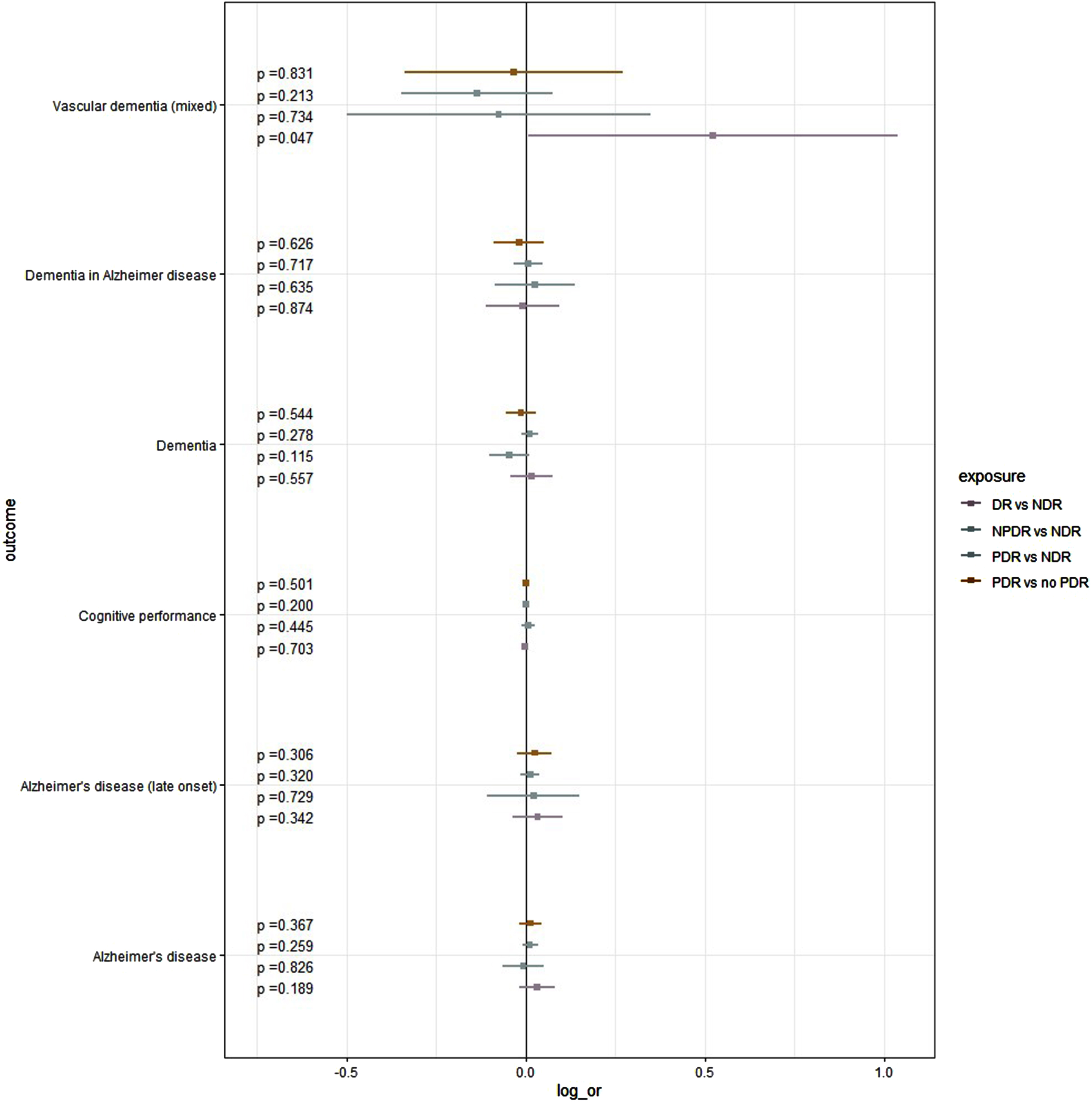
Potential Impact of DR on dementia/AD (log(OR) [95% CI]). All Odds ratios were derived using IVW method. DR, diabetic retinopathy; AD, Alzheimer’s disease; log_or: Logarithmic value of odds ratio; IVW, inverse-variance weighted.
Cerebral structure
To investigate whether DR underlies the changes in the structures of specific cortical regions, we performed MR using DR and subtype DR as exposure variables, and regional surface area and thickness phenotypes as outcomes. The analyses revealed that genetically predicted DR was associated with several cerebral regions associated with advanced cognition (Fig. 3, Supplementary Figure 1, Supplementary Table 3). We found that PDR was the most closely related to cortical structure compared to the other subtypes of DR (fusiform thickness (p = 0.013), isthmus cingulate thickness (p = 0.017), and middle temporal thickness (p = 0.027)). DR and its subtypes showed no genetic causal effect on the mean hippocampal volume (Supplementary Table 6).
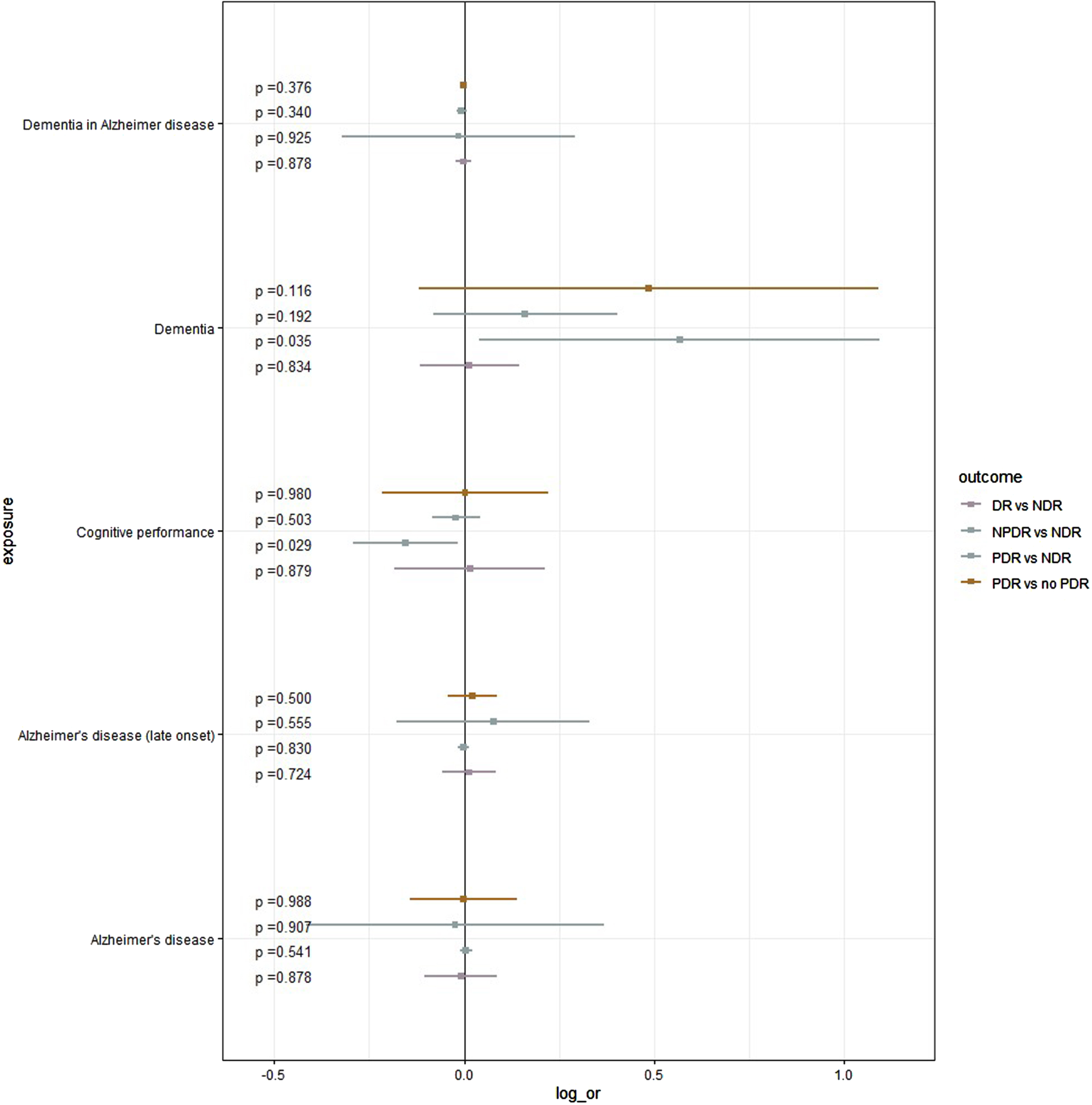
Potential Impact of dementia/AD on DR (log (OR) [95% CI]). All Odds ratios were derived using IVW method. DR, diabetic retinopathy; AD, Alzheimer’s disease; log_or: Logarithmic value of odds ratio; IVW, inverse-variance weighted.
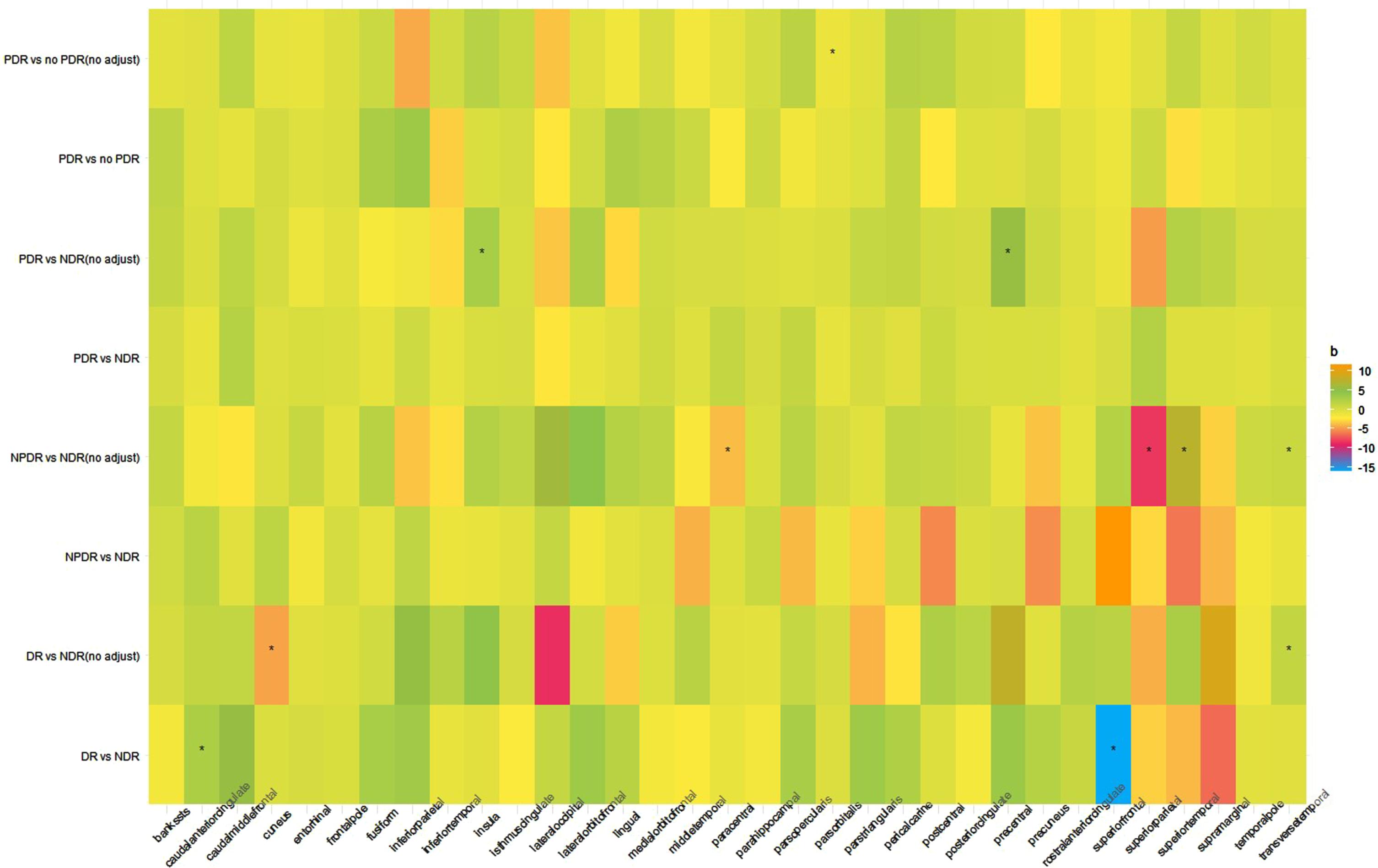
Potential Impact of DR and its subtype on cortical surface areas (beta[95% CI]). All beta coefficient (beta [95% CI]) were derived using IVW method. DR, diabetic retinopathy; IVW, inverse-variance weighted.
Association between genetically predicted AD/dementia, cognitive function, or cortical structure and DR
Dementia and cognitive performance
We found significant causal effects of dementia on higher risk of NPDR compared with NDR in adjusted model (IVW: OR = 1.76, 95% CI: 1.04–2.98, p = 0.034; weighted median: OR = 1.86, 95% CI: 1.02–3.39, p = 0.04) (Fig. 5). We found significant causal effects of better cognitive performance on lower risk of NPDR compared with NDR in the adjusted model (IVW: OR = 0.85, 95% CI: 0.74–0.98, p = 0.029; weighted median: OR = 0.82, 95% CI: 0.69–0.98, p = 0.03) (Fig. 2, Supplementary Table 4).
Cerebral structure
Similar to the direction from DR to cerebral surface areas/thicknesses, our analyses revealed that several genetically predicted cerebral surface areas/thicknesses were associated with DR and its subtype (Fig. 4, Supplementary Figure 2, Supplementary Table 5). The genetically predicted mean hippocampal volume showed no effect on DR or its subtype (Supplementary Table 6).
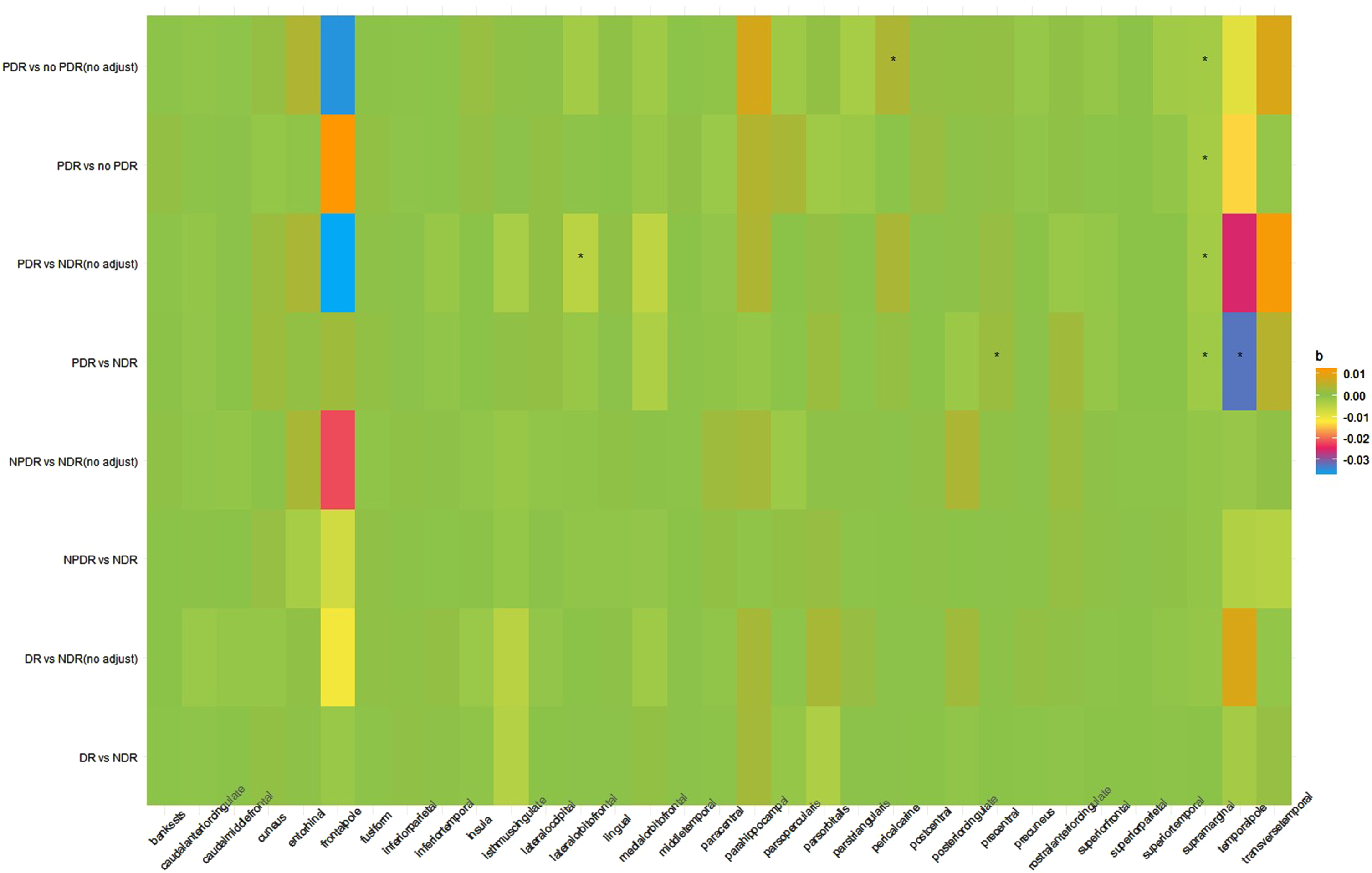
Potential Impact of cortical surface areas on DR and its subtype (beta [95% CI]). All beta coefficient (beta [95% CI]) were derived using IVW method. DR, diabetic retinopathy; IVW, inverse-variance weighted.
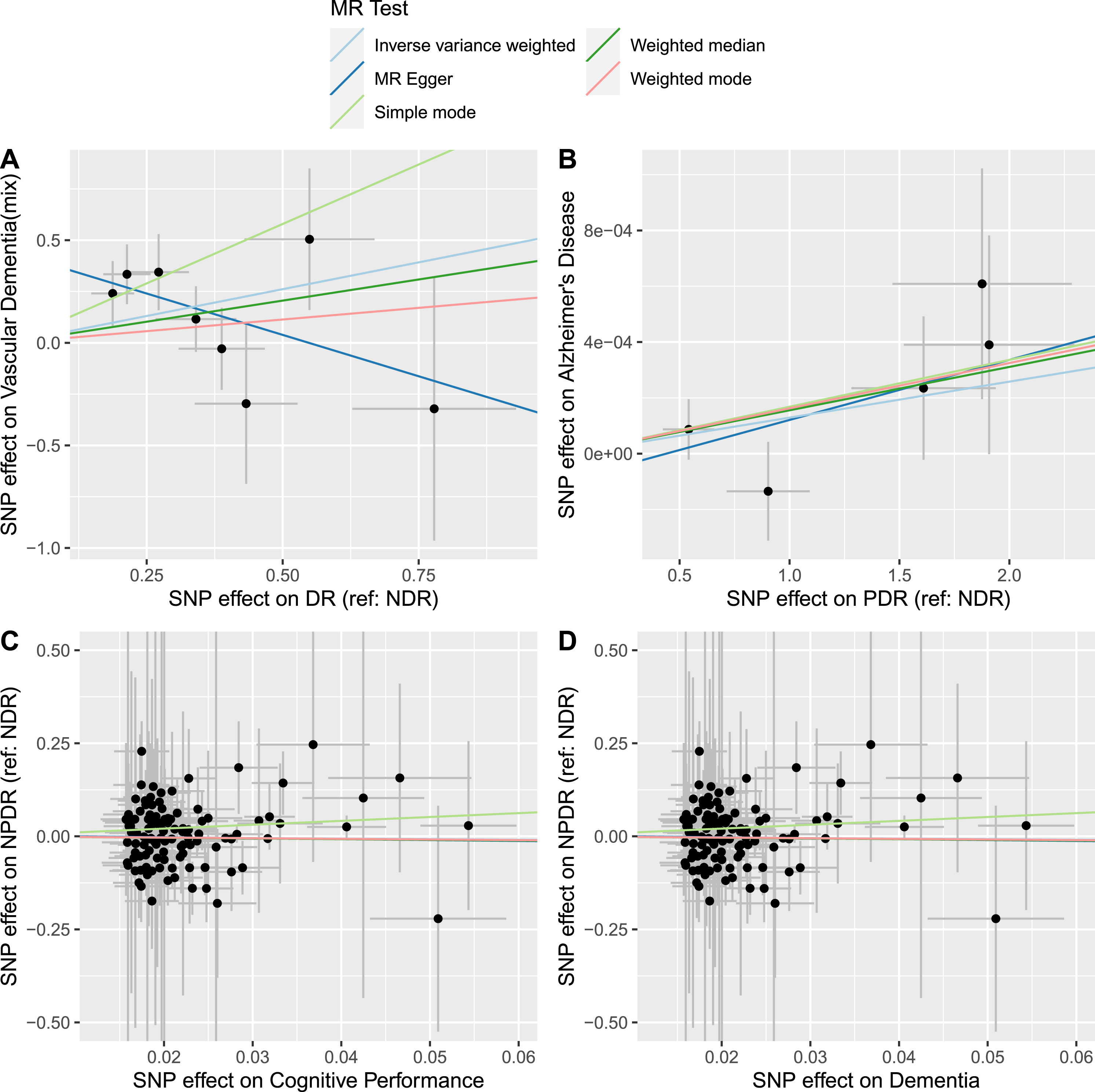
Scatter plot of main bidirectional MR results between DR and dementia/AD or cognitive performance. MR, Mendelian randomization; DR, diabetic retinopathy; AD, Alzheimer’s disease.
DISCUSSION
Our study aimed to explore the relationship between DR and overall dementia/AD using the MR method. Although numerous observational studies have suggested an association between DR and dementia/AD, the potential for confounding factors and reverse causation in such designs cannot be overlooked. To the best of our knowledge, this is the first study to use the MR approach to investigate this association, offering a more robust framework for causal inference. The results of this study suggest a suggestive association of DR with vascular dementia. Dementia is causally associated with a higher risk of NPDR. Better cognitive performance showed a causal relationship with a lower risk of NPDR.
We found that DR and DR subtypes may increase the risk of vascular dementia. Vascular dementia is a form of dementia caused by impaired blood flow to the brain, leading to cognitive decline. The presence of DR, particularly its advanced forms, such as PDR, may serve as an indicator of systemic microvascular damage. The shared pathophysiological mechanisms involving vascular dysfunction and microangiopathy observed in both DR and vascular dementia provide a plausible explanation for this association [29]. DR is characterized by progressive damage to the retinal blood vessels, resulting in ischemia, neovascularization, and, ultimately, vision impairment. Chronic hypoxia and inflammation associated with DR may contribute to the development of cerebral small vessel disease, a key pathology underlying vascular dementia [30]. Retinal microvascular changes, such as arteriolar narrowing, microaneurysms, and hemorrhages observed in DR may mirror similar changes in the cerebral vasculature [31]. Furthermore, individuals with DR are more likely to have other cardiovascular risk factors such as hypertension, dyslipidemia, and obesity. These factors contribute to the development of vascular dementia [32]. The cumulative effects of these risk factors, in addition to the direct effect of DR on cerebrovascular health, may explain the increased risk of vascular dementia in this population.
However, we did not find any causal effects of DR on the risk of AD, which is inconsistent with the findings of many recent studies. Lee et al. [11], in their observational study, found significant associations between DR > 5 years duration with AD (hazard ratio (HR) = 1.80; 95% CI: 1.15–2.82), and the results was not altered by adjusting for estimates of microalbuminuria, long-term glycemia, and renal function (HR = 1.73; 95% CI: 1.10–2.74). Phi et al. [33] reported a study based on medical histories and ICD-9 codes where 3,375 participants from the Cardiovascular Health Study Cognition Study and found DR was associated with vascular dementia/mixed dementia (HR = 2.63,95% CI: 1.10–6.27). Other studies have also reported no relationship between DR and AD/dementia. Chai et al. [11] performed a meta-analysis and found no relationship between DR/subtypes of DR and AD before and after adjustment for sex, age, and type of diabetes. For MR, we focused on the genetics and SNPs of DR, including the vascular endothelial growth factor (VEGF), aldose reductase, advanced glycation end products, and endothelial nitric oxide synthase gene, etc. [34]. VEGF dysregulation has been implicated in various neurological and psychiatric disorders including Alzheimer’s disease, stroke, and depression [35–37]. However, VEGF also plays an important role in promoting angiogenesis and maintaining vascular health, which are critical for retinal function. Owing to variations in the load and influence of VEGF in various tissues, the effects of VEGF on the retina and brain may differ. For example, the negative effects of VEGF on vascular health may outweigh any potential protective effects on the retina, leading to the development of DR. In contrast, the potential neuroprotective effects of VEGF in the brain may outweigh its negative effects, leading to a reduced risk of dementia.
Further, we found that dementia might increase the risk of NPDR. To our knowledge, no study has reported the causal effect of dementia on DR. The observed association between dementia and an increased risk of diabetic retinopathy may be attributed to shared underlying mechanisms. Chronic inflammation, vascular dysfunction, and metabolic disturbances are implicated in dementia and DR [38]. These factors may contribute to the development and progression of retinal microvascular abnormalities in patients with dementia. The expression of energy metabolism genes in the posterior cingulate neurons [39], inherent changes in bioenergetic profiles [40] and insulin-linked metabolic pathways [41] may provide evidence for their shared pathogenesis. However, we did not find a causal effect of dementia/AD on the increased risk of PDR. This may be explained by the fact that the incidence of NPDR is far greater than that of PDR, which may affect the statistical power of the GWAS data. Finally, although our sensitivity analysis consolidated our results, there may be still other confounders may affect both dementia and DR.
The relationship between DR and AD has been reported in several studies, demonstrating a notable link between the presence of DR and an increased risk of developing AD. A robust body of literature has documented the association between AD and alterations in the hippocampus, a brain structure crucial for memory and learning. Hippocampal atrophy is a characteristic feature of AD. However, our study found no causal effect between hippocampal volume and the incidence or progression of DR, and this lack of causality persisted in the reciprocal direction. As few studies have reported the relationship between DR and the hippocampus, further research is needed to clarify these complex interactions and their underlying mechanisms. We found that genetically predicted PDR was associated with cortical areas, such as the fusiform, isthmus cingulate, and middle temporal regions. These cortical areas play a key role in executive functions such as decision-making, working memory, and attention. In summary, chronic hyperglycemia and insulin resistance, which are characteristic features of diabetes, can lead to neuronal damage and impaired cortical thickness in the frontal and parietal lobes. Moreover, DR may be related to alterations in the brain microvasculature, which can lead to reduced blood flow and oxygen delivery to the frontal/parietal lobes, resulting in neuronal damage and impaired cortical thickness. Some evidence to support this idea is available, revealing that individuals with DR have reduced cerebral blood flow and impaired cerebrovascular function [42, 43].
Our study has several limitations. First, only a minor portion of the diversity in DR and AD may be attributed to hereditary factors, whereas the remaining variance is most likely explained by the mechanisms unaffected by genetic variables, as reported by Ridge et al. [44]. This study estimated the heritability of AD to be between 58% and 79% based on twin studies. Second, the results should be interpreted with caution. As with any MR study, there are potential sources of bias that must be considered. For example, the results may be confounded by other genetic or environmental factors associated with DR and dementia/AD, although we adjusted for several known confounders. Furthermore, although we found that genetically predicted DR was associated with several cortical surface areas and thicknesses (particularly the PDR), we did not find a bidirectional causal effect in the same cortical region. Similarly, we found a causal effect of cognitive performance on NPDR; however, we did not find any causal effect of DR/subtype on cognitive performance. Since cognitive function contains many dimensions (attention, perception, memory, executive functions, reasoning and problem solving, emotion, and cognition), further research is needed to validate the association between DR and the dimensions of cognitive function. Finally, our study lacked adequate power. The sample and effect sizes of the associations under investigation may not have been sufficient to detect subtle but clinically significant relationships. As a result, there is a possibility of a type II error, in which true associations might not have been identified. Future research with larger sample sizes is warranted to corroborate and refute our findings.
In conclusion, this study provides genetic evidence of a bidirectional causal relationship between DR and dementia/AD. We found the association of DR with vascular dementia. Our results showed no relationship between DR and AD. In contrast, we found causal effects of dementia on the increased risk of NPDR, suggesting that preventing the onset of dementia may reduce the health burden of diabetic retinopathy. Further research is needed to validate the association between DR and the dimensions of cognitive function, dementia, and AD in larger prospective cohorts.
Footnotes
ACKNOWLEDGMENTS
GWAS summary data, which are non-disclosed results from testing the association of hundreds of thousands to millions of genetic variants with a phenotype, have been routinely collected and curated for several years, and are a valuable resource for dissecting the causal architecture of complex traits [45, 46]. We thank all investigators of the GWAS for making their GWAS summary datasets publicly available. The UK Biobank was founded by the Medical Charity Welcome Trust, Medical Research Council, Department of Health, Scottish Government, and the Northwest Regional Development Agency. We are grateful to all the UK Biobank participants. FinnGen is a large public-private partnership aimed at collecting and analyzing genome and health data from 500,000 Finnish biobank participants. FinnGen aims on one hand to provide novel medically and therapeutically relevant insights and construct a world-class resource that can be applied in future studies. We acknowledge the participants and investigators of the FinnGen study. We are grateful for the resources from the ENIGMA Consortia [![]() ], which have concentrated on discovering genetic variants related to surface area and thickness values in each of the 34 cortical areas defined by FreeSurfer.
], which have concentrated on discovering genetic variants related to surface area and thickness values in each of the 34 cortical areas defined by FreeSurfer.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
All authors declare that they have no conflicts of interest related to this article. Jian-Bo Zhou is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article and/or its supplementary material.