
Abstract
Background:
Alzheimer’s disease (AD) is a progressive neurodegenerative pathology that leads to cognitive decline and dementia, particularly in older adults. It disrupts brain structure and function, with neurotoxic amyloid-β (Aβ) plaques being a primary pathological hallmark. Pharmacotherapeutic trials targeting Aβ and other AD pathological features aim to slow disease progression. Functional magnetic resonance imaging (fMRI) is a non-invasive tool that visualizes brain functional activity, aiding in evaluating the efficacy of AD drugs in clinical trials.
Objective:
This mini-review explores the role of fMRI in evaluating the impact of AD pharmacotherapeutic clinical trials conducted in the past seven years.
Methods:
Literature was systematically searched using two databases. The risk of bias was assessed with the Revised Cochrane risk-of-bias tool (RoB-2) for randomized clinical trials (RCTs).
Results:
Four studies using fMRI to investigate AD drug efficacy were included. Cholinesterase, glutamatergic, and serotonergic drugs showed significant positive effects on brain functional activity, especially within the default mode network. Functional connectivity (FC) changes due to drug intake were linked to cerebellar and cholinergic decline in AD, correlating with improved global cognition and fMRI task performance.
Conclusions:
Recent RCTs demonstrate fMRI’s ability to reveal longitudinal FC pattern changes in response to AD drug treatments across disease stages. Positive FC changes in distinct brain regions suggest potential compensatory mechanisms from drug intake. However, these drugs have limited efficacy, necessitating further research to enhance specific pharmacological interventions for clinical application.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the main cause of dementia among the older populations [1–4]. It is generally described by the deterioration of memory and several cognitive dysfunctions, including attention, learning, and motivation [2, 5]. Due to its increased global prevalence and liability, AD represents a significant socio-economic burden. The pathogenesis of AD is complex and heterogeneous in affected individuals [6]. AD is a multifactorial disease that is pathologically characterized by the deposition of amyloid-β (Aβ) peptides and neuritic plaques on the extracellular level, and intracellular accumulations of hyperphosphorylated tau protein as neurofibrillary tangles (NFTs), and active microgliosis [7]. These changes trigger synaptic damage, neuronal loss, and consequent disruptions in the white matter (WM) integrity [1, 6]. The mechanism underlying the onset and severity of AD are not limited to the ageing process and can include environmental and genetic factors, adding even more to the complexity of disease [3, 8].
In early onset of AD, the presence of the pathology is identified by the existence of extracellular Aβ plaques in several brain regions of affected individuals, due to either excessive or obstructed clearance of Aβ peptides, or possibly both [5, 7]. Pathophysiological studies have confirmed the association of amyloid-β protein precursor (AβPP) and the pathogenesis of AD [7, 9]. Evidence has shown that dysfunction in processing AβPP may result in the production of insoluble neurotoxic Aβ peptides. The two main forms of Aβ peptides that are formed exclusively in AD are Aβ40 and Aβ42 which are accompanied by 40- and 42-aminoacid deposits, respectively [9]. These Aβ peptides tend to accumulate to formulate oligomers of Aβ (oAβ), then accumulate even further to form insoluble amyloid plaques or senile plaques [7]. In the case of sporadic or late-stage AD, the apolipoprotein E4 (APOE4) gene has been reported to be a major contributor to AD pathogenesis. Moreover, individuals expressing APOE4 have increased Aβ deposition and compromised memory [9, 10].
Another critical indication of AD is the presence of intracellular NFTs in the AD brain [11–13]. Tau is a microtubule-related protein that functions to maintain the stability of neuronal microtubules [3]. When Aβ42 accumulates up to excessive concentrations in the brain cells, the risk of hyperphosphorylation of tau increases [14]. As such, the microstructure of the neuron is damaged to become unstable, and the microtubular units are disjointed in the absence of tau support [13]. The phosphorylated tau proteins then accumulate to form insoluble fibrillary tau strings, which clump together in the cytoplasm to form neurotoxic deposits called NFTs [13, 14]. This process leads to synaptic damage and the signaling ability of neurons is disrupted.
Both Aβ plaques and NFTs can stimulate microglia to migrate in close proximity to the plaques and block the clearance of both Aβ and NFTs [11, 16]. Excessive accumulation of reactive microglia induced by Aβ can expose neuronal cells to extensive oxidative damage and progressive neuroinflammation, leading to neuronal cell death [11, 17].
In the past 30 years, Aβ has been the target for the development of drugs for the treatment of AD with mixed results. Tau has received further attention owing to the failure of several Aβ-targeting treatments in clinical trials. At present, a majority of tau targeting therapies being investigated in humans are immunotherapies that showed promising results in animal studies [3, 17–19].
Neuropathological studies have shown that the basal forebrain is the source of cholinergic neurons, which provide the human cerebral cortex with the necessary cholinergic composites involved in several cognitive processes, including memory and attention [2, 6]. AD has been found to be associated with a reduction in the synthesis of acetylcholine, a neurotransmitter in the basal forebrain that is involved in several cognitive trajectories, including memory, attention, arousal, and motivation [5, 20]. Drugs targeting the cholinergic system have proven effective in delaying AD symptoms and AD-related cognitive dysfunction [2, 21].
Recognized global authorities, e.g., The United States Food and Drug Administration (US-FDA), have approved selected AD pharmacotherapeutic drugs, including 3 cholinesterase inhibitors: galantamine, donepezil, and rivastigmine [3, 22]. This approval also included a drug that targets the glutamatergic system, an N-methyl D-aspartate (NMDA) antagonist named memantine [23]. Based on the progression of the disease, the latest treatments for AD are categorized into two main classifications: mild to moderate, and moderate to severe cases. In mild-to-moderate AD cases, acetylcholinesterase (AChE) inhibitors are used to provide short-term symptomatic relief for affected individuals. AD impairs the cholinergic neurons, thereby reducing the amount of acetylcholine in the system. AChE inhibitors block the activity of acetylcholinesterase [7, 22]. This attenuates the loss of acetylcholine concentrations to help compensate for neuronal loss [22]. In moderate-to-severe cases, glutamate NMDA-receptor antagonists are used to regulate stimulation and preclude excessive glutamate secretion [23, 24]. These compounds have been mainly developed to selectively target proteins separately, nonetheless, a mixed treatment approach of both cholinesterase and glutamatergic drugs has been applied [7].
In both clinical and scientific research, magnetic resonance imaging (MRI) has become one of the primary tools in the diagnosis of AD progression [25]. Structural MRI is used to assess volumetric brain changes linked to the degenerative process of AD and can be easily employed in routine clinical investigations. In addition to whole brain volumetry, structural MRI methods such as T1 and T2 weighted images offer insights into anatomical changes and atrophy in particular brain regions such as the hippocampus, lateral ventricles, amygdala, medial and lateral temporal lobes, and grey matter, which have been widely studied. Although this has emerged as a research hotspot of clinical importance, these MRI modes only measure the structural changes in the brain tissue, neglecting the impact of AD progression on brain’s functional activity.
Based on the paramagnetic characteristics of oxygenated and deoxygenated hemoglobin, fMRI provides in vivo visualization of spatiotemporal maps of neural activities based on changes in low-frequency oscillations of blood-oxygen-level dependent (BOLD) signals [26–28]. Two approaches of BOLD-fMRI are commonly used in functional neuroimaging studies: task-based and resting-state (rs-fMRI) examinations [26]. During task-based fMRI, the BOLD signal is triggered by a specific task that is performed during an imaging session of a pre-defined experimental design, which stimulates neural activation within corresponding brain areas of interest [26]. In rs-fMRI sessions, the BOLD signal is detected from the intrinsic neural activation of brain regions without using task demands, which facilitates data-driven exploration of brain’s functionality without the need for implementing complex experimental designs [29, 30]. fMRI represents a comparatively recent addition to AD biomarker research methodologies. Its non-invasive nature is a significant advantage, particularly in clinical trials, as it avoids radiation exposure and the need for contrast agents [31]. This feature facilitates multiple scanning sessions, which are essential for longitudinal studies. Moreover, fMRI provides superior spatial and temporal resolutions and can be conducted concurrently with structural scanning sessions. The perspective that AD functions as a disconnection syndrome, characterized by the progressive structural and functional disengagement of brain regions throughout the disease’s progression, is now firmly established and supported by substantial evidence [32]. In the sequence of AD biomarkers, changes in the functional connectivity of the hippocampus and posterior cingulate cortex (PCC) appear earlier than cerebrospinal fluid Aβ42 accumulations [33, 34]. Therefore, fMRI may be highly effective in detecting early-stage AD and assists in differentiating AD from other forms of dementia.
Advances in fMRI methodologies have been used to investigate pharmacotherapeutic efficiency in AD treatment trials, with existing research indicating fMRI’s capability to identify immediate pharmacological impacts on memory [32, 35] and the default mode networks [36]. Correlations between functional activation within various brain regions (e.g., PCC, dorsolateral frontal, insula, frontal gyrus, hippocampus, and thalamus) and during different treatment settings, such as type of medication, dosage, and intake periods have been confirmed [32]. Also, FC measures of several brain networks (e.g., the default mode, executive control, dorsal attention, and salience) were found to correlate with different treatment proprieties [35]. These functional responses were found associated with changes in cognitive abilities in AD individuals [32, 35]. Recent fMRI approaches aimed to track the results of AD therapeutic experiments, supporting the notion that fMRI can deliver key findings on brain functionality, neural plasticity, and metabolic processes affected by clinical AD therapy trials [35].
METHODS
Guideline for searching strategy
In the current study, we examined recent developments of using fMRI in AD clinical pharmacotherapeutic trials to assess the efficiency of FDA-approved treatment medications. We explored databases of PubMed and PsychINFO using a set of keywords related to AD: (“Alzheimer’s” or “post*Alzheimer’s” or “Alzheimer’s disease” or “AD”), and fMRI methods: (“fMRI” or “functional magnetic resonance imaging” or “BOLD-fMRI” or “functional connectivity”) and AD clinical trials with pharmacotherapeutics: (“clinical trials” or “therapeutic” or “medication” or “drug” or “cholinergic” or “glutamatergic” or “treatment” or “galantamine” or “donepezil” or “rivastigmine” or “selective serotonin reuptake inhibitors” or “D-amino oxidase inhibitor”). Inclusion criteria was as follows: 1) written in English, 2) human-based study sample, 3) clinical trial study design, 4) published after January 2016, 5) FDA-approved drugs, targeting cholinergic or glutamatergic or serotonergic systems, and 6) at least one functional (task or resting-state) MRI session. We excluded review papers; studies that used conventional structural approaches only or focused on non-imaging evaluation; studies used different modalities other than fMRI; and reports that used none-drug treatment approaches (e.g., behavioral/cognitive training, and therapeutic EEG stimulation) were discarded. A schematic representation of papers identified and assessed are summarized in Fig. 1.
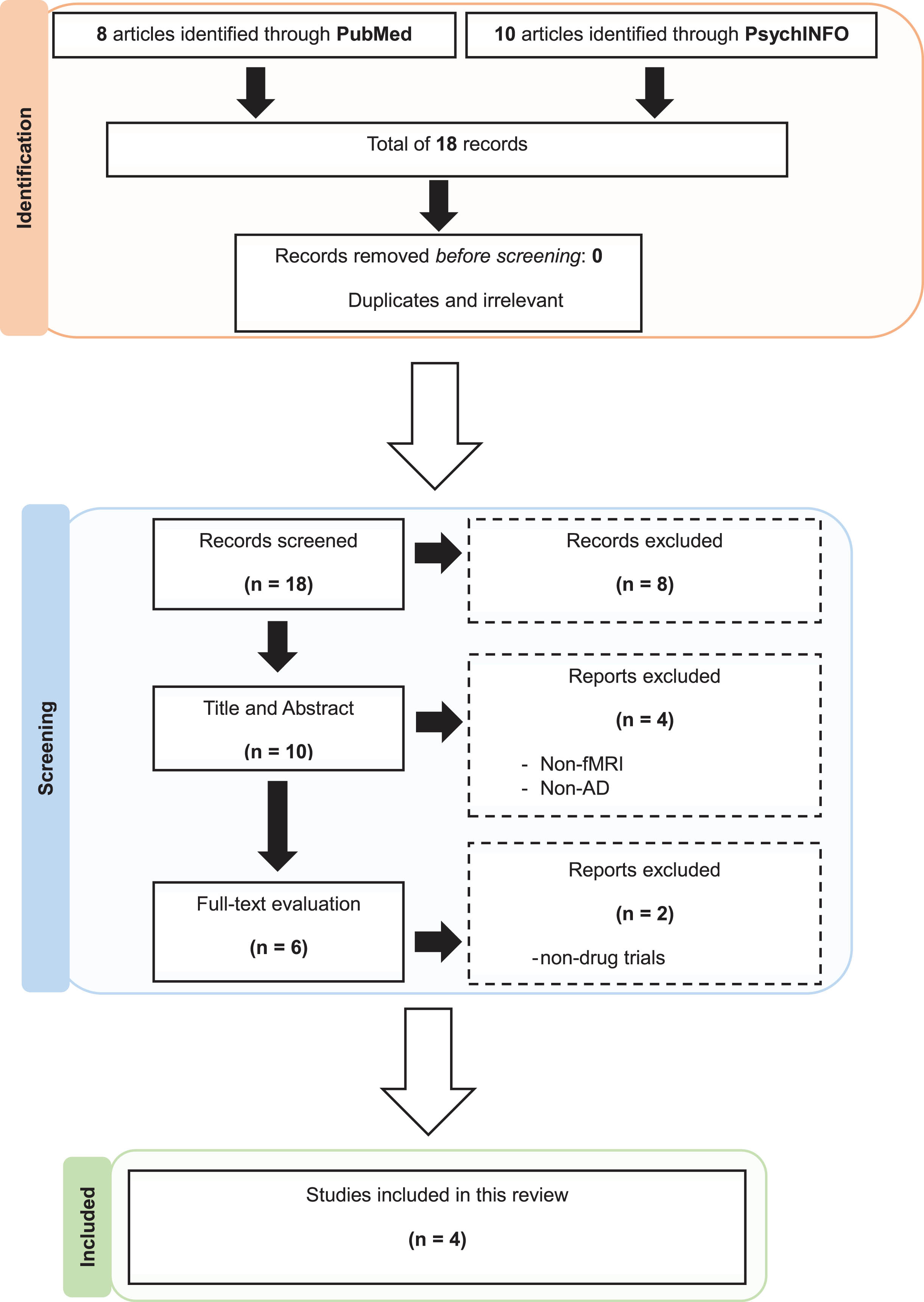
Literature search and article screening results.
Risk of bias assessment
All included trials were assessed for methodological quality using the risk of bias assessment tool 2.0 (RoB-2) developed by Cochrane Collaboration [37]. This tool was developed to assess randomized clinical trials (RCTs) by evaluating 5 domains: randomization process, intended interventions, missing outcome data, outcome measurement, and selective reporting of results. For each of the included trials, domains were classified as low-, some concerns-, or high risk of bias. For an overall low risk of bias, all five domains must have low risk of bias; otherwise, even if one domain showed some concerns or high risk, the overall risk will be judged as some concerns or high risk of bias. Any four domains with some concerns will result in a high overall risk of bias. Authors (MA and NB) independently judged and verified the risk of bias, and any dissimilarities were solved through discussion. A summary of the risk of bias assessment for this review are presented in Fig. 2.
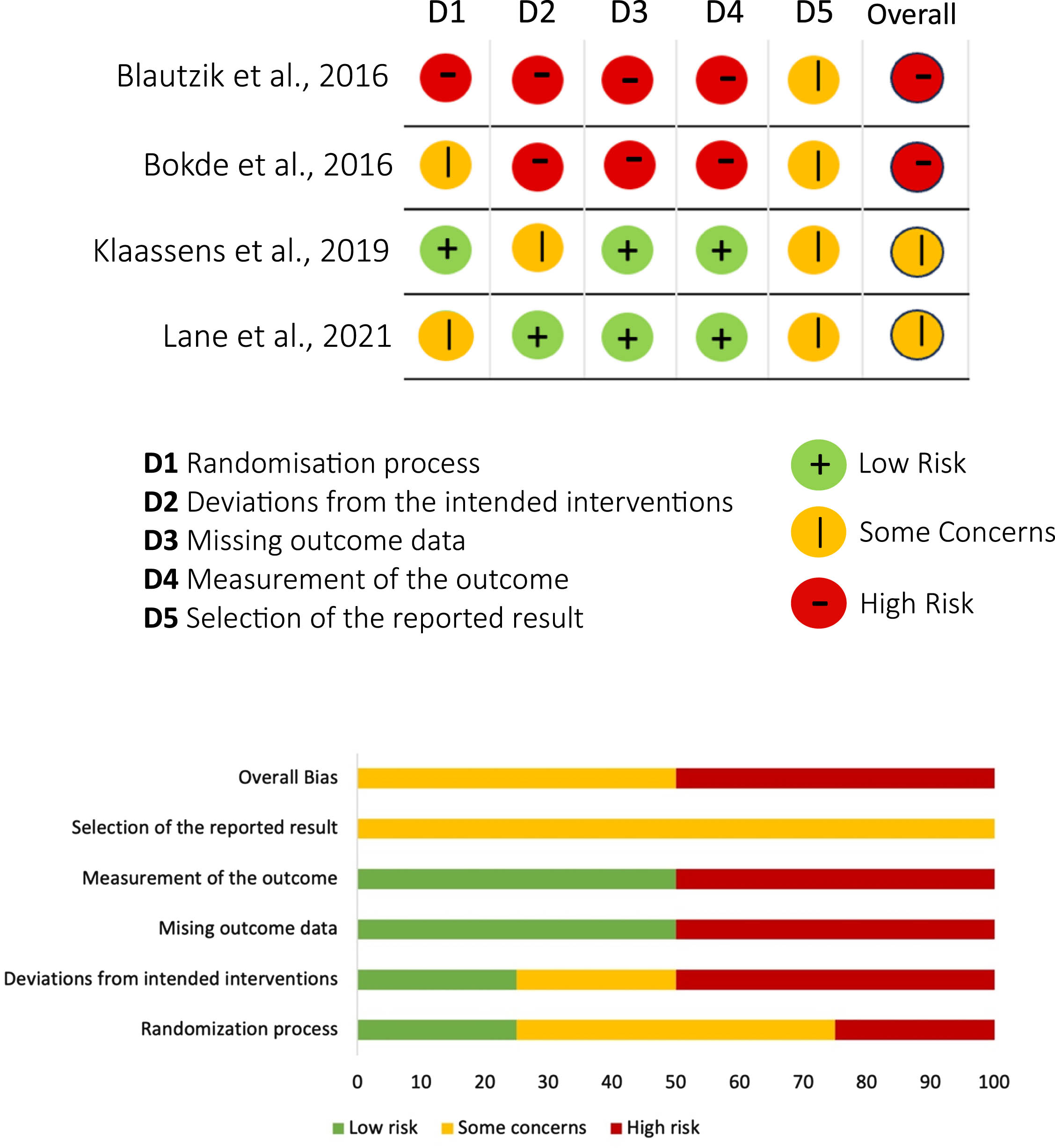
Summary of risk of bias assessment using RoB-2 tool (Traffic light plot and Summary plot).
RESULTS
We located 18 relevant papers, 8 of them were acquired by searching PubMed, and 10 through PsychINFO databases. There were no duplicates, so all reports underwent title inspection. Eight papers were found irrelevant based on title reading and were excluded. For the remaining 10 reports, which were screened based on both title and abstract, 4 records were excluded for not meeting our search criteria. The remaining 6 papers were read in full and evaluated, and 4 articles were included in this review.
We included 4 full-text articles that assessed the efficiency of therapeutic drugs on AD progression using fMRI. All included reports have used different fMRI methodologies in different experimental designs. Three studies have simply used resting-state fMRI approaches, while one study has implemented a task-based experimental design to target pre-defined brain regions that are related to specific cognitive abilities. These studies have used recognized FDA-approved pharmacological medications that target either cholinergic or glutamatergic systems in the brain. All four experiments were conducted longitudinally over periods ranging from a few days up to 12 months with multiple drug doses. The age range of participants range from 50–90 years, as AD onset is expected to exist in older adults. However, the sample size was expectedly low in the reported studies due to the large number of measures used in every experiment (cognitive tests, blood tests, drug intake, imaging), and the lengthy duration of trials that have led to less commitment and participant dropouts. Overall, the feasibility of such experiments showed promising outcomes, supporting the assumptions regarding the benefits of fMRI in delineating AD mechanisms via clinical trials. In our study, rs-fMRI was the preferred method since some individuals were unable to perform tasks due to their medical condition. Detailed descriptions of included studies and key findings are summarized in Table 1.
Summary of reviewed articles used drug-based AD treatment experiment
ADAS-cog, Alzheimer’s Disease Assessment Scale-cognitive subscale; BNT, Boston Naming Test; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; CP, constructional praxis; FC, functional connectivity; HC, healthy controls; MMSE, Mini-Mental Status Examination; PCC, posterior cingulate cortex; RCP, recall of constructional praxis; ReHo, regional homogeneity; VF, verbal fluency; WL, Word List (Learning, Recall, Recognition); WMS-III, Wechsler Memory Scale–Third Edition.
Changes in fMRI connectivity in response to acetylcholinesterase inhibitors
The effect of AChE inhibitors has been investigated in our reviewed studies. Bokde et al. (2016) used working memory and location matching task paradigms in 7 patients (5 treatment and 2 placebo) with mild cognitive impairment (MCI) administered 3–6 months of treatment with rivastigmine (5 treatment and 2 placebo). The study reported significant increases in FC in the frontoparietal pathway [38].
One study tested the effect of cholinergic inhibitors on functional connectivity changes in response to long-term AD treatment. The study found that FC in areas of the default mode network (DMN) showed a significant increase compared to baseline after 12-month post-treatment using galantamine [36]. The clinical trial involved 36 participants (mean age: 70.7 [8.4]) divided into healthy controls, and mild-to-moderate AD participants (subdivided into drug, and drug with placebo participants). Between-group analysis in the same study revealed an increased FC in the PCC and the precuneus in AD group compared to controls. Further, drug-only AD (AD + D) group showed an increased FC in anteromedial temporal lobe compared to the mixed drug/placebo group (AD + GP) [36].
Alterations in cholinergic neurotransmission has been linked with cognitive deficits in AD. One study examined the effect of galantamine in 12 patients with AD and 12 age-matched controls on FC using resting-state fMRI [4]. This randomized, double blind, placebo-controlled crossover study, assessed fMRI scans performed before and after dosing (totaling 432 scans). Connectivity maps of ten functional networks were analyzed using a dual regression method. Multivariate analysis was used to compare the effect of galantamine versus placebo using signals collected from the cerebrospinal fluid and white matter as covariates at the subject level. The study also used baseline and heart rate measurements as confound regressors. The study found that FC within the cerebellar network, and between this network and the thalamus declined significantly post galantamine treatment compared to placebo alone in AD patients, but not in control subjects. The results of this study also confirm a change in cerebellar connections in AD, which is possibly related to cholinergic decline.
Changes in fMRI connectivity in response to other drugs for AD
The study mentioned above [4] also examined the effect of a single-dose of the selective serotonin reuptake inhibitor citalopram in 12 patients with AD and 12 age-matched controls on FC using resting-state fMRI. The study did not find any difference in FC between AD patients and control subjects using voxel-wise network connectivity post citalopram treatment. However, the DMN connectivity with the precuneus and PCC was increased in AD patients, and not present within the control group. As well, mean connectivity within all networks was reduced in control subjects but not in post-citalopram AD patients. The effects of citalopram on the DMN provides evidence for a restoring potential of selective serotonin reuptake inhibitors in AD [4].
Sodium benzoate (a D-amino acid oxidase [DAAO] inhibitor) has been shown to improve cognitive function in patients with early-phase AD/MCI, although the exact mechanism remains unclear [39]. A 24-week, randomized, double-blind, placebo-controlled trial evaluated the effect of benzoate on fMRI in patients with amnestic MCI [39]. The study enrolled 21 patients with amnestic MCI that were randomly allocated to either of 2 treatment groups: 1) benzoate group (250–1500 mg/d), or 2) placebo group. The outcomes examined were working memory, verbal learning and memory, and rs-fMRI and regional homogeneity (ReHo) maps at baseline and endpoint. The study found a reduction in ReHo in the right orbitofrontal cortex after benzoate treatment but not in the placebo group. As well, working memory was positively correlated with the change in ReHo in right precentral gyrus and right middle occipital gyrus, while verbal learning and memory positively correlated with alterations in ReHo in the left precuneus. The pilot study provides support for the role of DAAO inhibitors for the treatment of AD.
Risk of bias
All RCTs included in this review had either some concerns or a high risk of bias in one or multiple methodological domains, hence, the overall risk of bias evaluation for each was classed as either some concerns or high risk according to the guidelines and algorithms of RoB-2. One study was classed as low risk of bias in the randomization process domain [4], one study was classed as high risk of bias [36], while the others were classed as having some concerns [38, 39]. Reasons for randomization bias included an undescribed randomization method, suspected unconcealed allocation sequence before the intervention, and lack of a healthy controls group. Two studies showed high risks of bias in the second domain due to possible deviations from the intended interventions [36, 38], whereas one had some concerns [4]. This bias was mainly due to the previous knowledge of the assigned intervention by either participants or intervention providers (or both) in a way that might affected the outcome.
Most studies followed a mixed open-label/double-blinding approach in different time points, which raised concerns regarding the overall blinding process. Two studies were classified as having a high risk of bias for incomplete outcome data [36, 38], mainly due to serious dropouts of participants, while two studies had low risk [4, 39]. Despite the remarkable role of fMRI as a major outcome for all included trials, two reports were classified as high risk of bias in outcome measurements [36, 38]. This was due to concerns regarding the assessor’s knowledge of the assigned intervention received by participants, which may influence the reported outcomes. Two studies had low risk of bias in the outcome measurements for the relatively safer implementation of randomization and blinding processes [4, 39]. All RCTs have failed to sufficiently describe the pre-intervention intentions, which obstructs methodological comparisons with currently available AD research. As a result, even with the absent answers for the other signaling questions in this domain, RoB-2 algorithms will classify the domain as having some concerns or even a high risk of bias in the selection of the reported results.
DISCUSSION
Several AChE inhibitors have been investigated including galantamine and rivastigmine. Other drugs have also been investigated, including citalopram and sodium benzoate. However, studies comparing the effects of various pharmacological treatments are lacking. We only found one study comparing the effect of citalopram and galantamine on FC patterns [4]. However, the intensity and duration of treatment were not consistent. Functional MRI studies identified significant positive effects of these drugs on brain activation during cognitive task performance and/or resting state in patients with AD and early phase AD (MCI). These changes were reported following acute and chronic exposure to cognitive enhancing agents. Short-term RCTs [4, 39] have proved the rapid effects of AD drugs on brain’s functionality, denoting the superior capability of fMRI in detecting early signs of AD before the irreversible neuron damage [40]. This allows for potential interventions before conversion to AD. Unlike fMRI, structural MRI detects AD at later stages, where the disease is progressed to irreversible neuronal loss [40]. This restricts the focus of trials to later AD stages or increases the possibility of failing the therapeutic objectives of clinical trials in early AD stages.
The necessity for long-term treatment to modulate efficacy raises the problem of the treatment costs. As well, the effects of these drugs on FC were observed in several regions of the brain associated with AD, and non-AD regions as well. In most cases, these changes occurred parallel to improved global cognition and fMRI task performance. However, owing to the heterogeneity of AD pharmacotherapeutics, and diverse cognitive paradigms utilized in fMRI tasks, developing a standardized result remains a challenge.
When evaluating the effect of AD therapeutics on brain function using fMRI, an appropriate definition of the clinical population is crucial. Patients receiving treatment should be classified as prodromal or probable AD with a clinical diagnosis verified using clinical biomarkers. Potential methods to stratify the appropriate target population have been implemented in several large international consortiums including Alzheimer’s Disease Neuroimaging Initiative (ADNI) and include abnormal tau and Aβ42 cerebrospinal fluid levels, baseline MRI atrophy, and AP ∘E4 status. These strategies should be implemented to define an early phase AD (MCI), or at-risk asymptomatic subjects. However, none of the reviewed studies used biomarkers in their inclusion policy. As well, the clinical features of the MCI population (i.e., amnesic, or non-amnesic) were not available. When reviewing the study sample, the absence of appropriate clinical definitions and clinical biomarkers affect the accuracy and reliability of findings. Brain atrophy is common in patients with AD and MCI. Nonetheless, cortical atrophy and grey matter volume was assessed in only one trial of our reviewed studies [36]. Disturbances in brain volume may interfere with the voxel intensities detected using fMRI and affecting group comparisons.
In the articles included in our mini-review, the randomization procedure was not accurately performed due to absence of a healthy group of controls in 2 out of 4 studies [38, 39]. While these studies report differences in effect in FC in the treatment groups, it is difficult to confirm that these observed finds are related to the specific efficacy of the treatment itself or part of the clinical intervention. The confounding factor in these 2 studies remains that the participants and personnel are unblinded. Moreover, the other 2 studies that have adopted a randomized study design, failed to adequately disclose the method for subject randomization or a priori bias (e.g., a priori stratification of the sample group by gender) that may influence the neutral distribution of the enrolled subjects in the experimental groups.
The main challenge when comparing the efficacy of specific treatments is translating the findings from the laboratory into the clinic. fMRI is advantageous because it identifies the brain regions that are affected in response to treatment and can predict the benefits of treatment on routine everyday activities. However, interpreting fMRI data engenders several challenges. For instance, cognitive behavioral fMRI studies that assess behavioral changes longitudinally can be biased by learning effects since the time interval between pre- and post-treatment assessment is short. Many of the tasks used to examine the efficacy of pharmacological interventions are disease-driven. While this approach reflects our current knowledge of AD pathology, it may potentially limit information collected on treatment efficacy. For example, compensatory mechanisms and brain reorganization in regions unaffected by AD pathology are not assessed. A potential solution is to implement task-related fMRI and assess activation of non-memory related brain circuits, i.e., those associated with selective attention, distracter inhibition, etc., to detect potential improvements in the encoding process by specific AD pharmacotherapeutics.
Furthermore, the stability of MRI data over various time intervals is crucial in long-term longitudinal MRI studies. For instance, it is essential for the same MRI scanner to be used by all subjects at consistent time points across the entire duration of the study. The resting and task-based fMRI signal has reported only modest reproducibility in longitudinal studies comparing FC between young and old individuals. Some studies, not examined in this review, have adopted pretraining MRI brain scans. This allows the assessor to distinguish between brain changes associated with repetition, and those related to treatment. However, the inability to have a control group using this study design has limited the implementation of this strategy to identify brain changes in FC. Moreover, direct comparison between resting-state and task-based fMRI on brain FC changes is nascent in the current literature. However, there is a growing body of evidence indicating that resting-state fMRI yields higher reproducibility across different scanners, and over various time points, since the methodology does not require the subject to undertake a cognitive task.
A limitation of this mini-review is the relatively small number of studies included after placing a restrictive criterion. Therefore, our findings should be considered preliminary and require confirmation using a larger number of studies. By restricting the inclusion criteria in this manuscript, the intention is to give clarity to the outcomes under investigation. Without this, it is difficult to come to a conclusion using literature over a broader time frame since no limits have been defined on research available in the literature on AD drugs and fMRI in clinical trials.
Conclusions
This review provides an update on current literature on the effects of selected pharmacological treatments on brain fMRI in AD and MCI. Both task-based and resting-state fMRI have been adopted to identify changes in FC in the brain with promising results. However, these findings are limited, and further work is required to substantially reliability of these findings. This includes but is not limited to increasing the sample size, improving patient selection, enhancing the soundness of the methodology, and developing more appropriate study design that favors comparison across time and different scanners. Additional studies are necessary to increase the value of specific pharmacological interventions to increase the clinical translation of these agents in the clinic, and more broader methods to assess both pathological and compensatory mechanism.
While there is a growing body of knowledge implicating the importance of task and resting fMRI in understanding the neurobiology of AD [41], further studies are needed to validate fMRI as a potential biomarker in clinical trials for AD. Recent studies have shown that task-based fMRI may yield greater efficacy in early “Proof of Concept” studies [38], to detect an optimal efficacy signal over a short period of time. Studies using resting state fc-MRI suggest its feasibility in multi-centered clinical trials since the setup does not require special equipment [4, 39]. As the field of AD research and drug discovery expands to the development of diagnostic tools and early intervention therapy prior to the onset of clinically evident symptoms, the combination of amyloid biomarkers and fMRI may be beneficial for the detection of early AD pathology and AD-related cognitive decline, and to monitor response to interventions.
AUTHOR CONTRIBUTIONS
Mohammed Ali Alghamdi (Data curation; Formal analysis; Investigation; Methodology; Software; Writing – original draft; Writing – review & editing); Nady Braidy (Conceptualization; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This research was supported by a scholarship from Prince Sattam bin Abdulaziz University, Ministry of Education, Saudi Arabia.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article.