
Abstract
Background:
Lifestyle factors are linked to differences in brain aging and risk for Alzheimer’s disease, underscored by concepts like ‘cognitive reserve’ and ‘brain maintenance’. The Resilience Index (RI), a composite of 6 factors (cognitive reserve, physical and cognitive activities, social engagement, diet, and mindfulness) provides such a holistic measure.
Objective:
This study aims to examine the association of RI scores with cognitive function and assess the mediating role of cortical atrophy.
Methods:
Baseline data from 113 participants (aged 45+, 68% female) from the Healthy Brain Initiative were included. Life course resilience was estimated with the RI, cognitive performance with Cognivue®, and brain health using a machine learning derived Cortical Atrophy Score (CAS). Mediation analysis probed the relationship between RI, cognitive outcomes, and cortical atrophy.
Results:
In age and sex adjusted models, the RI was significantly associated with CAS (β= –0.25, p = 0.006) and Cognivue® scores (β= 0.32, p < 0.001). The RI-Cognivue® association was partially mediated by CAS (β= 0.07; 95% CI [0.02, 0.14]).
Conclusions:
Findings revealed that the collective effect of early and late-life lifestyle resilience factors on cognition are partially explained by their association with less brain atrophy. These findings underscore the value of comprehensive lifestyle assessments in understanding the risk and progression of cognitive decline and Alzheimer’s disease in an aging population.
Keywords
INTRODUCTION
The global demographic shift towards an increasingly older population presents a pressing need to develop validated tools that provide a comprehensive assessment of life-course determinants of brain health and risk of Alzheimer’s disease and related dementias (ADRDs) [1–3]. Such assessments are essential for enabling more effective early interventions and personalized prevention strategies. In the spectrum of brain aging outcomes, cognitive resilience plays a pivotal role, not only in the context of clinical conditions such as mild cognitive impairment (MCI), often considered a prodromal stage of neurodegenerative dementias like ADRDs, but also in ‘normal’ cognitive aging.
In fact, older age is a common factor in the majority of MCI cases and is considered the single greatest risk factor for ADRDs [4, 5]. Even in ‘normal’ cognitive aging, declines in aspects of cognitive abilities, in particular processing speed, attention, and executive functioning become apparent [6–8], which can impact daily functioning and wellbeing, albeit in more subtle ways than overt cognitive impairment [9–11]. Yet the extent of these ‘normal’ age related cognitive changes are greater for some individuals than they are for others [12, 13]. Understanding why some individuals experience more pronounced age-related cognitive changes than others is important given that these variations in normal cognitive aging may signal increased vulnerability to ADRDs.
Characteristic age-related cortical atrophy over the lifespan are well documented [14–17]; changes most strongly associated with changes in cognitive abilities [18, 19]. Numerous studies have recognized the important role of lifestyle factors in influencing age and ADRD related brain changes [1, 20–23]. Related concepts such as ‘cognitive reserve’ and ‘brain maintenance’ are frequently used to explain heterogeneity in age and ADRD related brain changes, including increase variability in normal age-related cognitive decline and differences in ADRD prevalence and symptom presentation [23–26]. According to the Stern et al. (2023) framework on brain maintenance, protective lifestyle factors (healthy diet, exercise, etc.) may lead to better brain health (i.e., slower brain atrophy with aging), thereby supporting cognitive function and is distinct from ‘cognitive reserve’ which refers to the active and dynamic neural capacity to maintain cognitive function in the presence of brain pathology (e.g., cortical atrophy due to Alzheimer’s disease) until a certain threshold of underlying disease pathology is met [27, 28].
Proxy measures of cognitive reserve and brain maintenance capture life course related behaviors—most commonly used include educational attainment, occupational complexity, engagement in leisure activities (in the case of cognitive reserve) [28–30], physical activity, diet and stress reduction activities (in the case of brain maintenance) [31–33]. Given the numerous life course/lifestyle factors linked to variability in age-related brain health outcomes [34], a comprehensive assessment of an individual’s global resilience may provide a better picture of their brain and cognitive resilience, yet are sparse as highlighted by a recent review [35].
In recognition of this gap, our group recently developed and validated the Resilience Index (RI) [36]. The RI is a comprehensive but brief measure of lifestyle factors calculated as the sum from six different scales that assess social engagement, physical activity, proxies of early and later life cognitive reserve (educational and occupational attainment, leisure activities), diet and mindfulness stress reduction. The RI demonstrated excellent discrimination between cognitively intact (n = 39) and cognitively impaired individuals (n = 75), AUC = 0.836. Higher RI scores were also associated with better cognitive, functional, and self-reported quality of life scores. In a subset of individuals (n = 53) with MRI data, greater resilience scores were also associated with larger hippocampal volumes [36, 37]. Given its potential value as a clinical tool for brain-health assessment, there is a need to examine this index in relation to more general and global characteristics of brain aging and underlying disease using an independent and larger sample.
To that end, the current study aimed to test the Stern et al. [28] resilience framework using the RI. Specifically, we hypothesized that the positive association between higher scores on the RI and cognition would be in part explained by its association with better brain health and/or may attenuate the negative association between global cortical atrophy and cognitive function. By examining these relationships, our findings aim to contribute to the broader understanding of how early and later life cumulative lifestyle resilience factors collectively relate to brain health and function; important for deepening understanding lifestyle related risk for ADRDs.
METHODS
Participants
The data for the current study were obtained from the baseline visits of an ongoing longitudinal study referred to as the Health Brain Initiative (HBI) which is focused on the comprehensive assessment of cognitive, medical, physical, and brain health of South Florida residents aged 50 years and older. A total of 113 participants with full baseline data on the measures used for the current study were included. Exclusion criteria for this study include: under age 50 years, refusal to consent for data/specimen storage, lack of a study partner, a diagnosis of moderate or severe ADRD (CDR≥2), inability to provide clinical, cognitive, behavioral, or functional data, have significant medical conditions which would affect neuroimaging participation or obscuring cognitive outcomes, such as metastatic cancer, major psychiatric disorders, unstable chronic diseases, or substance abuse within the past 5 years. Informed written consent was obtained from all participants enrolled in the HBI following full IRB approval by the University of Miami. Full details of the study procedures have been previously published [38].
Measures
Resilience Index
The RI, developed by Galvin et al. [36], represents the sum of six scales, namely the cognitive reserve unit scale [39], the Social Engagement Scale [40], the Quick Physical Activity Rating [41], the Cognitive & Leisure Activity Scale [40], the Mediterranean-DASH Intervention for Neurodegenerative Delay Diet Score [42], and the Applied Mindfulness Process Scale [43]. Thereby, this index measures various behaviors including cognitive activity, physical activity, social engagement, dietary patterns, mindfulness, and cognitive reserve (i.e., calculated based upon the individual’s educational and occupational attainment). The RI ranges from 1–378, with higher scores indicating greater resilience. Full details of the subscales are included in the Supplementary Material.
Global cognition
The cognitive performance of participants was assessed using Cognivue®, an FDA-cleared global computerized cognitive screening tool to aid in assessing for the presence of cognitive impairment [44, 45]. Cognitive domains assessed including motor speed, visuospatial skills, verbal and visual episodic memory, attention, executive function, and reaction time are assessed using adaptive psychophysics, to tailor task difficulty in accordance with the individual’s real-time responses. The assessment procedure takes approximately 10 minutes to complete. For the purposes of this study, the primary outcome was the composite score derived from performances across the mentioned cognitive domains. Scores range from 0–100, with higher scores indicative of better cognitive performance. For sensitivity analysis, the Montreal Cognitive Assessment (MoCA) [46] total score was used as a separate measure of global cognition. This is a widely used cognitive screener for the detection of dementia. Scores range from 0–30 with higher scores indicating better cognitive function. Individuals with a score of 26 or above are considered to be within normal range, while scores between 18 and 25 are suggestive of MCI, and below 18 is suggestive of dementia.
Cognitive status
An initial ‘research’ diagnosis of cognitively normal or MCI using the NIA-AA [47] criteria was rendered for each participant following their baseline HBI cognitive assessments, medical history, and Clinical Dementia Rating (i.e., global score of 0.5 indicative of MCI) by licensed nurse practitioners with specialized training in cognitive assessment. Monthly consensus conferences were conducted to review initial diagnosis by a board-certified neurologist (JG) and licensed neuropsychologist (DOS) to confirm or amend diagnosis. A total of 35 individuals included in the current study were classified as having MCI and 78 were classified as cognitive normal (CN). No individuals in the current sample had a diagnosis of dementia.
Covariates
Sex/gender (male, coded as ‘1’, females coded as ‘2’), age (years) and years of education were self-reported.
Magnetic resonance imaging (MRI) procedures
All participants underwent structural brain MRI using a GE 3 Tesla 750 W scanner at baseline. High-resolution 3D sagittal Magnetization-Prepared Rapid Gradient-Echo (MPRAGE) images were captured, followed by axial and coronal reconstructions. Several corrections were applied to the raw MRI images to ensure quality: including correction for geometric distortion of gradient nonlinearity, field inhomogeneity correction, histogram-peak sharpening, and correction for site-specific scanner features/field strength.
Image analysis and derivation of cortical atrophy measure
Cortical volumes were derived using the Combinostics® cNeuro Suite, an FDA-cleared quantitative analysis tool. This suite harnesses artificial intelligence (AI) technology to optimize the speed, accuracy, precision, and robustness of imaging analysis, thereby enhancing research data quality. The AI-driven Combinostics cMRI suite demonstrates comparable performance to manual segmentation, evidenced by Pearson coefficients ranging between 0.84 and 0.99 [48, 49].
Global cortical atrophy
The Cortical Atrophy Score (CAS) is a z-score estimate of global cortical atrophy. It was developed using the Global Cortical Atrophy visual rating scale, a widely used rating metric in European clinical radiology. The CAS is an age, sex, and head size adjusted estimate using a reference sample of individuals aged between 50 to 90 years. Previous studies have shown that the CAS outperforms measures of cerebral cortex total volumes (AUC = 0.823) as well as the combined volume of cerebral gray and white matter (AUC = 0.833) in distinguishing early-stage AD from cognitively normal individuals, achieving an AUC of 0.873. CAS scores in the current sample ranged from -1.01 to 3.98, with higher scores indicating greater global cortical atrophy [49]. Cortical atrophy was selected as the primary MRI measure to estimate global changes potentially attributable to various factors such as aging, ADRD, lifestyle and a marker with established relevance to cognitive function [50].
Statistical analysis
Descriptive statistics were generated prior to the mediation analysis to evaluate the sample characteristics and distributions of variables. For continuous variables means, standard deviations (SD) and ranges are reported and frequencies and percentages for categorical variables. Due to unequal samples sizes between men and women, Mann-Whitney U tests were employed to compare differences between male and female participants across continuous variables due to its robustness in handling non-normally distributed data and unequal sample sizes. Additionally, the Two-Sample Kolmogorov-Smirnov Test was used to assess differences in the distributions of these variables between genders, offering a comprehensive analysis of both median values and overall distribution shapes.
Pearson’s bivariate correlation (r) analysis was conducted among the RI, cognitive performance, and CAS to examine associations between variables. To test whether the association between the RI and cognition was explained in part by its association with cortical brain atrophy mediation analysis was conducted with the SPSS PROCESS macro version 4.2 [51] with the RI as the independent predictor, Cognivue® scores as the dependent variable and CAS as the mediator. PROCESS is a path analysis modeling tool that uses ordinary least squares (OLS) regression-based procedures. Mediation models we re-run to adjust for age and sex (Model 2). In Model 3, we further adjusted the RI for earlier and mid-life factors, namely education and occupation to better assess understand associations with current lifestyle resilience factors. We did this by regressing RI on CRUS (education and occupation scale) and used the standardized residual as the adjusted RI measure (higher scores indicated greater resilience) and reran the mediation models (controlling for sex and age again). All variables were converted to z-scores based on the mean and standard deviation (SD) of the current study sample prior to mediation analyses to facilitate interpretation. The indirect effect (also referred to as the mediation effect) was quantified using 10,000 bootstrap samples in order to generate bias-corrected confidence intervals. The direct effect of RI on cognitive performance, the relationship between RI and CAS, and the mediated path from the RI to cognitive performances via CAS were evaluated. The mediation effect was considered significant if the 95% bias-corrected confidence intervals for the indirect effect did not encompass zero [52]. To assess the robustness of our findings, we reran the mediation models using total scores on the MoCA as a separate measure of global cognition as sensitivity analysis. Additional sensitivity analysis examined whether mediation effects differed by sex and cognitive status (cognitively normal versus MCI) with moderated mediation Model 7 in PROCESS. These conceptual models are illustrated in Supplementary Figures 1 and 2, respectively. All statistical analyses were conducted with a significance level set at α= 0.05, two-tailed. Effect sizes were interpreted using standardized coefficients. Confidence intervals were set at 95% for all models.
RESULTS
Descriptive statistics
Characteristics of the study sample are shown in Table 1. The mean (±SD) age was 68.56 (±9.88), education mean years = 16.34 (±12.61), 68% were women, 81% White non-Hispanic, 9% non-Hispanic Black, and 10% Hispanic. The mean (±SD) for RI was 179.20, (±32.10), for Cognivue® scores was 74.35 (±12.61), and for CAS was 1.58,±0.95. Mann-Whitney U Tests indicated no significant gender differences in RI (U = 1374.500, p = 0.847), age (U = 1268.500, p = 0.400), education (U = 1198.500, p = 0.188), and Cognivue Total Score (U = 1317.500, p = 0.588). Similarly, Two-Sample Kolmogorov-Smirnov Tests supported these findings, showing no significant distributional differences between genders for these variables (D values ranging from 0.101 to 0.145, p-values ranging from 0.671 to 0.960).
Sample characteristics, N = 113
Bivariate correlations
As summarized in Table 2, The RI demonstrated a significant negative correlation with CAS (r = –0.26, p = 0.006) and a significant positive correlation with Cognivue® scores (r = 0.32, p < 0.001) indicating that greater resilience is associated with less cortical atrophy and better cognitive performances. CAS was significantly and negatively correlated with Cognivue® scores (r = –0.39, p < 0.001), suggesting that greater cortical atrophy is associated with poorer cognitive performance. Age had a significant negative correlation with Cognivue® scores (r = –0.36, p < 0.001). Point biserial correlations between sex and the other variables were not statistically significant.
Bivariate correlations between variables, N = 113
RI, Resilience Index; CAS, Cortical atrophy score; indicates point-biserial correlations between categorical and continuous variables, *p < 0.05, **p < 0.01, ***p < 0.001.
Mediation analyses
The following results are summarized in Table 3. In the unadjusted model (Model 1), higher scores on the RI were associated with a decrease in CAS (β= –0.26, SE = 0.09, p = 0.006, 95% CI [–0.44, –0.08]), accounting for 7% of the variance (R2 = 0.07). In the overall effect model, the RI and cortical atrophy scores together accounted for 21% of the variance in Cognivue scores (R2 = 0.21). The total effect of RI on Cognivue® (without the mediator) was significant (β= 0.32, SE = 0.09, p < 0.001, 95% CI [0.15, 0.50]). The direct effect of RI on Cognivue scores (with the mediator in the model) was significant (β= 0.24, SE = 0.09, p = 0.007, 95% CI [0.07, 0.41]). The indirect effect of the RI on Cognivue® via cortical atrophy was also significant (β= 0.09, SE = 0.04, 95% CI [0.02, 0.17]). To illustrate these relationships, a mediation figure depicting the betas of the pathways is included (Fig. 1).
Summary of regression analyses for resilience on cognivue® through cortical atrophy scores (CAS)
R2, Variance explained; CAS, Cortical atrophy score; RI, Resilience Index; CRUS, cognitive Reserve units (Education and Occupation).
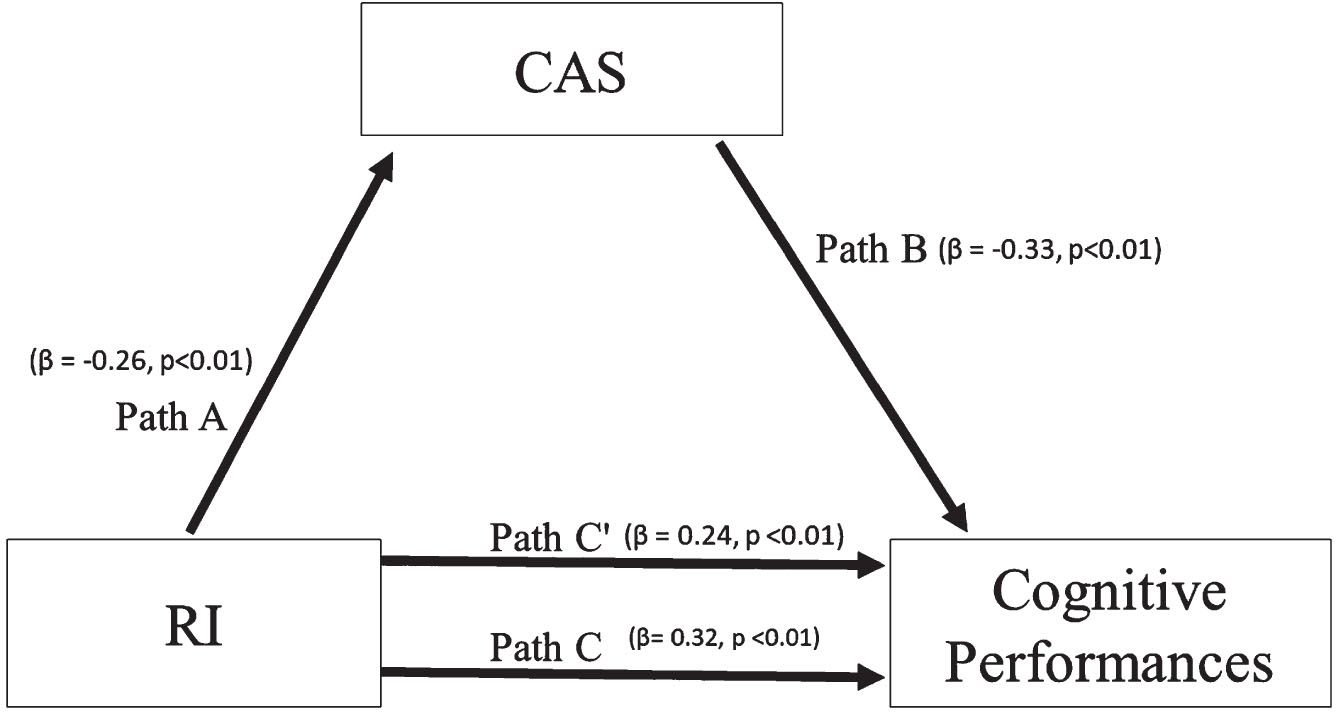
Mediation Model Depicting the Relationship of Resilience Index (RI) with Cognitive Performances, Mediated by Cortical Atrophy Score (CAS). The figure represents the mediation model exploring the effects of the Resilience Index (RI) on cognitive performances, with the Cortical Atrophy Score (CAS) as the mediator. Path A illustrates the effect of RI on CAS, and Path B displays the effect of CAS on cognitive performances. Path C represents the total effect of RI on cognitive performances, while Path C’ depicts the direct effect of RI on cognitive performances after accounting for the mediation effect of CAS. The standardized beta coefficients (β) along with their significance levels (p) are reported for each path, indicating the strength and direction of the associations.
Adjusted model analysis
Table 3 summarizes the subsequent models that were adjusted for age and sex (Model 2). In this model, the associations between RI, CAS, and Cognivue scores remained significant but showed slight reductions in effect sizes. In Model 3, using the residual RI from regressing RI on the CRUS (education and occupation), the direct and indirect effects of RI on Cognivue® were slightly reduced but remained significant.
Sensitivity analysis
Similar associations were observed using MoCA scores, reinforcing the primary analysis results. The results from this mediation analysis are summarized in Supplementary Table 1. Results from moderated-mediation analyses with sex as the moderator (Supplementary Table 2), showed that the indirect effect of RI on cognition through atrophy was significant for females (Effect = 0.060, 95% CI [0.008, 0.136]), but not for males (β= 0.084, 95% CI [–0.003, 0.197]), However, the moderated-mediated index was not significant (β= –0.024, SE = 0.055) 95% CI [–0.135, 0.086]), suggesting that the difference in strength of this difference was not robust. Finally, the indirect effect of RI on cognition through CAS was significant for individuals with normal cognitive status (β= 0.060, 95% CI [0.004, 0.151]) but not for those with MCI (β= 0.031, 95% CI [–0.054, 0.100]). The index of moderated mediation indicated that the difference in the indirect effect between normal and MCI groups was not statistically significant (β –0.029 (95% CI [–0.160, 0.056]).
DISCUSSION
The current study sought to investigate the mediating role of a machine learning derived measure of cortical atrophy in the relationship between a newly validated measure of global cognitive resilience (i.e., RI) and cognitive function. The findings showed that higher scores on the RI were associated with better global cognition and that this association was partially explained by less cortical atrophy in individuals with higher RI, independent of age, sex, and education. Findings from exploratory moderated-mediation analyses indicated that this association may be specific to women and those without overt cognitive impairment, although the strength of these differences was not robust, possibly to the small sample sizes of the subgroups.
Cortical atrophy is a well-documented feature in the progression of Alzheimer’s disease [50, 53], and our study suggests that lifestyle resilience, as measured by RI, may offer a protective mechanism against such neural degeneration. By demonstrating a mediating role of cortical atrophy between resilience and cognitive functioning, this study provides insights into potential pathways for slowing or modifying the progression of Alzheimer’s disease. This is particularly relevant given the limited treatment options currently available for Alzheimer’s and the growing emphasis on preventive measures and lifestyle modifications in managing the disease.
Although numerous studies have shown a positive association between individual lifestyle factors including educational attainment, physical activity, diet and leisure activities and cognitive function, with MRI derived brain volumes [23, 54], a recent review suggested that fewer studies have examined these associations with a composite measure of key brain-health related lifestyle markers, and even less so with validated composite instruments [35].
This is the first known study to examine the association between a recently validated global measure of global resilience that captures well documented measures of early and late life measures of cognitive reserve and healthy brain behaviors and cortical atrophy on cognitive function in a community-based sample of older adults without dementia. This comprehensive approach aligns with the growing understanding in ADRD research that a multifaceted lifestyle intervention may be more effective in maintaining cognitive health and potentially delaying the onset of AD symptoms.
Linking to the concepts of cognitive reserve and brain maintenance
The finding of a direct association of RI on cognition even after controlling for cortical atrophy and age in the whole sample supports the role of cognitive reserve. That is, individuals with higher RI scores compared to lower scores had better global cognitive performances even at similar levels of brain atrophy. On the other hand, a partial mediation effect of cortical atrophy on the RI and cognition suggests that higher lifestyle resilience is associated with less cortical atrophy which relates to better cognitive functioning in line with a brain maintenance perspective [28]. The RI captures both traditional measures of cognitive reserve (i.e., education and occupation) as well as later life measures of cognitive reserve (e.g., leisure activities, social engagement) and brain maintenance related factors (e.g., physical exercise, diet) and therefore is consistent with the expected performance of this measure in demonstrating cognitive reserve and brain maintenance.
Importantly, the current study showed that this relationship was preserved even after adjusting for early and early and mid-life resilience factors (education and occupational attainment), suggesting that the protective effect of RI is robust and operates beyond the cumulative benefits of cognitive reserve from earlier life phases. These findings are consistent with a meta-analysis which showed that a Mediterranean diet and increased exercise can decrease and/or slow conversion from MCI to dementia in later life [55]. Additionally, a more recent review of randomized control trials of lifestyle interventions in MCI and dementia showed that exercise benefits cognition in MCI and dementia, although no significant association was found for stress reduction and there was insufficient evidence for determining the efficacy of a healthy diet [56]. Although these studies did not evaluate the impact of lifestyle on brain variables, a separate randomized clinical trial of 100 adults with MCI (of whom 50 received exercise program while the control group (n = 50) participated in an education program) evaluated the impact of exercise on cognitive function and global cortical atrophy. The findings showed that compared to the control group, the exercise group exhibited significantly higher Mini-Mental State Examination scores, memory performances and reduced whole brain cortical atrophy. Consistent with our findings, lifestyle factors in later life may benefit cognition/brain health.
Utilizing a comprehensive measure of resilience, such as the RI allows for estimating an individual’s overall cognitive and brain resilience. However, it is important to note, that while the RI may serve as a useful component in a more comprehensive assessment framework, its utility in isolation for individual clinical diagnostics or risk prediction requires further investigation, evidenced by a large degree of unexplained variance 70% in our models in cognitive performances. Instead, the RI as a foundational component that, when integrated with additional research and clinical data, can enhance its efficacy and precision in assessing cognitive decline risk.
Moreover, lifestyle and resilience assessments have recently been noted to serve as a pivotal role in clinical brain health services in older adults without significant cognitive impairment for reducing risk for ADRDs [57]. Using only single proxies may lead to under or overestimating one’s brain health status. For example, while one individual may be characterized as low resilience due to low educational attainment, they may be categorized as high resilience based on a separate measure of resilience, i.e., occupational attainment or current physical activity levels and so forth, without a comprehensive assessment of risk and brain health may lead to misidentifying people at high risk for age-related cognitive impairment.
Limitations and future directions
There are several limitations of the current study that are notable. Firstly, due to the cross-sectional design, the directionality of associations cannot be determined. For instance, whether higher global resilience leads to reduced cortical atrophy and improved cognitive function, or whether individuals with better cognitive function and less atrophy tend to report higher resilience. A longitudinal study, with multiple time-points, could offer a more definitive perspective on causality. Another limitation pertains to our sample’s demographics, including the relatively high education levels (mean years = 16; Bachelor level equivalent), which is higher than the national average among adults over the age of 65 whereby only 29% had a Bachelor’s degree [58]. Furthermore, the race/ethnic composition was predominantly White (81%), with only 10% Black and 9% Hispanic. Together these factors narrow the study’s generalizability, as it may not adequately represent the broader population’s socio-economic or cultural diversity.
Additionally, while significant indirect effects of RI on global cognition through cortical atrophy were observed in females and individuals with normal cognitive status, these effects were not evident in males or the MCI group. The non-significant moderated mediation indices indicate that the differences in these indirect effects between sexes and cognitive statuses are not statistically robust. However, the unequal and notably smaller sample size of the MCI group (n = 35) may have limited our ability to detect significant effects, potentially leading to an underestimation in less represented groups. This disparity in group sizes could lead to an underestimation of the effects in less represented groups, such as males and individuals with MCI. These limitations highlight the need for caution in generalizing the findings to these specific groups and underscore the importance of further research with larger and more balanced samples to elucidate the roles of sex and cognitive status in the relationship between RI, cortical atrophy, and cognitive function. Future studies may consider incorporating more detailed brain MRI measures, such as white matter hyperintensity/integrity, gray matter or even specific ADRD biomarkers (e.g., amyloid, tau, etc.) to assess the relevance of lifestyle factors to other biomarkers of health and disease.
Despite the limitations, the current study has several notable strengths. Firstly, our use of the machine-derived and validated cortical atrophy score, normed for age and sex provides a more precise and standardized assessment of cortical health compared to traditionally used manual or semi-automated measures. Furthermore, the utilization of the recently validated RI offers a more comprehensive view of differences in resilience. Unlike many studies that focus on isolated aspects of resilience, the RI integrates a broad spectrum of determinants encompassing both early-life cognitive reserve and later-life lifestyle factors. This comprehensive approach enriches an understanding of resilience and its impact on cognitive health, offering valuable insights into how these factors collectively influence brain aging and risk for ADRDs.
Conclusion
The findings from the current study revealed an association between higher RI scores, diminished cortical atrophy, and better cognitive function. Notably, cortical atrophy appears to play a mediating role in this relationship and suggests that fostering lifestyle resilience might be particularly beneficial for older individuals at risk of cognitive impairment. Enhancing resilience through lifestyle factors is increasingly recognized as a vital component of ADRD management and prevention strategies. These findings contribute to the existing literature on cognitive aging and ADRD by offering insights into how combined early and late-life factors can impact brain health and cognition, in part via reducing cortical atrophy.
AUTHOR CONTRIBUTIONS
Deirdre O’Shea (Conceptualization; Data curation; Formal analysis; Investigation; Writing – original draft; Writing – review & editing); Simone Camacho (Data curation; Writing – original draft; Writing – review & editing); Reem Ezzeddine (Data curation; Writing – original draft; Writing – review & editing); Lilah Besser (Methodology; Writing – original draft; Writing – review & editing); Magdalena I. Tolea (Methodology; Writing – original draft; Writing – review & editing); Lily Wang (Conceptualization; Writing – original draft; Writing – review & editing); Conor Galvin (Data curation; Writing – original draft; Writing – review & editing); Gregory Gibbs (Data curation; Writing – original draft; Writing – review & editing); James E. Galvin (Conceptualization; Resources; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
FUNDING
The Healthy Brain Initiative (HBI) is supported by National Institutes of Health R01AG071514, R01AG071514S1, R01NS101483, R01NS101483S1, RF1AG075901, and R56AG074889 (PI for all grants: JEG) and conducted at the University of Miami – Miller School of Medicine. The HBI was approved by the University of Miami Institutional Review Board. The funders listed had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. DOS acknowledges her support from the Miami Clinical and Translational Science Institute, from the National Center for Advancing Translational Sciences (Grant Number 1K12TR004555).
DATA AVAILABILITY
The dataset used for the current study are available upon request. Other HBI data will be made available upon study completion.
CONFLICT OF INTEREST
JEG is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review. JEG is also a consultant for Cognivue®.