
Abstract
Background:
Loneliness, dementia, and mortality are interconnected.
Objective:
We aimed at understanding mediating pathways and interactions between loneliness and dementia in relation to mortality risk.
Methods:
The study tested bi-directional relationships between dementia, loneliness, and mortality, by examining both interactions and mediating effects in a large sample of older US adults participating in the nationally representative Health and Retirement Study. Out of≤6,468 older participants selected in 2010, with mean baseline age of 78.3 years and a follow-up time up to the end of 2020, 3,298 died at a rate of 64 per 1,000 person-years (P-Y). Cox proportional hazards and four-way decomposition models were used.
Results:
Algorithmically defined dementia status (yes versus no) was consistently linked with a more than two-fold increase in mortality risk. Dementia status and Ln(odds of dementia) were strongly related with mortality risk across tertiles of loneliness score. Loneliness z-score was also linked to an elevated risk of all-cause mortality regardless of age, sex, or race or ethnicity, and its total effect (TE) on mortality was partially mediated by Ln(odds of dementia), z-scored, (≤40% of the TE was a pure indirect effect). Conversely, a small proportion (<5%) of the TE of Ln(odds of dementia), z-scored, on mortality risk was explained by the loneliness z-score.
Conclusions:
In sum, dementia was positively associated with all-cause mortality risk, in similar fashion across loneliness score tertiles, while loneliness was associated with mortality risk. TE of loneliness on mortality risk was partially mediated by dementia odds in reduced models.
INTRODUCTION
Worldwide, around 50 million people have dementia and this is projected to increase to 152 million in 2050, with a greater increase in low-and middle-income countries, with Alzheimer’s disease remaining the most common sub-type [1]. Additionally, 4.7% individuals aged 60 years and older are projected to be affected with dementia, with 4.6–7.7 million additional cases worldwide per year [2]. Dementia is characterized as a progressive loss of global functions, with an emphasis on memory loss and on deficits in executing everyday life activities [3]. The World Health Organization (WHO) recognized the importance of addressing dementia globally through a global action plan responding to dementia over the period of 2017–2025, highlighting key action areas in health and social systems [4]. Despite recent advancements in drug development [5] there are limited treatment options. Therefore, increasing research on dementia prevention and risk reduction remains critical, along with identifying modifiable lifestyle and risk factors linked to dementia risk.
In 2020, the Lancet commission identified potentially modifiable risk factors that accounted for 40% of dementia risk; these include education, hearing loss, traumatic brain injuries, hypertension, alcohol use, obesity, smoking, depression, social isolation, physical inactivity, air pollution, and diabetes [6]. The same study also highlighted social contact as a protective factor against dementia, with the potential to improve late-life cognitive functioning [6]. In 2020 the National Academies of Science, Engineering and Medicine report identified how social isolation and loneliness are risk factors for depression, anxiety, cognitive deficits, dementia, poor cardiovascular health, and early mortality [7]. The same report also summarized the pathways which link social isolation and loneliness with health outcomes ending with risk for mortality; along with mediators that are behavioral (e.g., lifestyle, medial adherence), psychological (e.g., stress), and biological (blood pressure, gene expression) suggesting that social connection influences morbidity and mortality [7]. Several cross-sectional studies have identified feelings of loneliness to be predictive to dementia onset [8, 9] one even concluding feelings of loneliness to be more predictive than social isolation [10]. Recent studies have also shown dementia and poor cognitive performance to be predictive of higher mortality risk [11, 12]. At the same time, loneliness in older adults has recently become a public health concern associated with cardiovascular disease [13, 14], psychiatric morbidities [15, 16], hospitalization [17, 18], and mortality [19, 20]. A recent systematic review and meta-analysis of 144 studies identified loneliness to be associated with adverse health outcomes, especially on mental health and overall well-being, with a stronger effect on men [21]. Another recent meta-analysis of 36 studies not only concluded that loneliness was associated with mortality but also a small social network size was also associated with mortality [22], providing a possible objective aspect to addressing subjective feelings of loneliness in older adults. Nevertheless, most studies have either examined the association between loneliness and mortality (e.g., [19, 22–27]) or loneliness and dementia (e.g., [8, 28–35]).
Given that loneliness, dementia, and mortality are interconnected, understanding the pathways, along with the potential interaction between loneliness and dementia in predicting mortality, provides a relevant area of research to be developed. To our knowledge, no known study has comprehensively examined the mediating and moderating role of loneliness, dementia, and mortality risk among older adults using a nationally representative sample. Therefore, we test whether dementia and loneliness are related to mortality risk, independently of potential confounders and across sex and race groups, and their 2-way interactions. We then simultaneously test how loneliness and dementia odds interact to determine mortality risk and bidirectional mediation of “loneliness”-mortality and “dementia”-mortality through dementia status and loneliness, respectively, using four-way decomposition models.
MATERIALS AND METHODS
Database
Repeated every two years since 1992, the Health and Retirement Study (HRS) collects data on a nationally representative sample of US individuals over the age of 50 years [36, 37]. The National Institute on Aging (grant number U01AG009740) and the Social Security Administration fund the prospective cohort study. The core data contains a long list of variables that are obtained every two years from all HRS participants, covering a variety of domains related to health and retirement. This core data is made available in a curated manner in the RAND longitudinal dataset used in this study. In 2006, the Enhanced Face-to-Face Interview (EFTF) was launched for the HRS to incorporate physical (i.e., performance tests & anthropometric measures), biological (i.e., blood and saliva samples), and psychosocial (i.e., self-administered psychosocial questionnaires) measures. Throughout the primary sampling units (PSUs), nearly half of homes with one or more living respondent were included for an EFTF interview.
From the 2006 HRS wave, a random half sample of respondents were used for EFTF interviews. In 2008, the second half of the sample was examined. Likewise, for 2010 new cohort families were assigned at random to one of these two groups, beginning in 2010 or 2012 for EFTF data collection. Ensuring the same request was sent to both household members, the household level was chosen as the sample. New spouses of respondents who were marked for an EFTF interview were asked to do the same. In coupled families, both members were chosen. A few EFTF sample participants were not required to complete physical or biomarker measures. Those respondents a) were questioned by a proxy, b) were in a nursing home, or c) refused face-to-face interview but agreed to a phone interview. In this study, EFTF psychosocial data was used for the years 2006 and 2008combined.
Standard protocol approvals, registrations, and patient consents
All procedures followed the ethical standards of the institutional or regional committee on human experimentation. Approval was obtained from the committee of human subjects at a local universities Institutional Review Board (IRB). For the current prospective longitudinal cohort analysis, approval was obtained from the parent IRB-approved study, from a government agencies research program, while the ethics board determined that participant consent was not required or waived.
Study sample
A total of 43,561 HRS particpants (1992–2018) were included in the initial RAND file for the longitudinal study (randhrs1992_2018v2). Based on the participant flowchart (Supplementary Figure 1), in 2010, those who were included and alive were 22,034. Among them, those aged > 50y were 20,695. Additonally, those with data on dementia status or probability in 2010 were 7,677. In the final sample, we accounted for missing data on loneliness, including 6,468 participants > 50y in 2010 with dementia status or probability and loneliness data who were followed up until 2020 for mortality from all causes using the HRS latest tracker file available (trk2020tr_r). The mean age in 2010 was 78y. Around 5.5% of this sample reported being in a nursing home over the past 2 years.
All-cause mortality
The present study had the outcome variable all-cause mortality between 2010 and 2020, which was documented from 2010 for both the loneliness exposure and dementia status or probability measurement. Deaths were identified in the HRS using data linkage from the population registry and interviews [38]. Variables to 2020 (verson 2) were used from the tracker file. During the follow-up period from 2010–2020, 6,468 participants were used in our final sample. Among those who died from any cause with a known date of death (month and year), 3,298 were counted. Time-to-death or censoring was calculated from time elapsed (measured in years) between age in 2010 and age at death or age at censoring.
Dementia status and probability
The data file (hrsdementia_2021_1109.sas7bdat) which is publicly available includes dementia probabilities and classifications projected for 2000–2016 HRS respondents 60 + in 2006. Several new algorithms were developed. Those included a modified version from Hurd and colleagues (Modified Hurd Model) who originally developed the model, along with a new expert-informed logistic model (Expert Algorithm) and the Least Absolute Shrinkage and Selection Operator (LASSO) algorithm were trained and tested using HRS data along with data from all four waves of the Aging, Demographics, and Memory Study (ADAMS; http://hrsonline.isr.umich.edu/index.php?p=shoavail&iyear=XB). This process achieved 77–83% sensitivity, 92–94% specificity, and 90–92% accuracy overall in out-of-sample performance. The Supplementary Material and Supplementary Methods File contain further information regarding these algorithms. In summary, two forms of these variables were available, one being dichotomized as 0 = no dementia versus 1 = dementia and another being a predicted probability from each of the models, which was then transformed into Ln(odds of dementia).
Loneliness score
Loneliness was operationalized using 3 items from 2006 and 2008, each measured on a Likert scale of 1–3. These items were KLB020A, KLB020B, KLB020 C, LLB020A, LLB020B, and LLB020 C, which were reverse coded to reflect greater loneliness with higher scores and can be obtained from the Leave-Behind Questionnaires section LB, for the 2006 wave of data (public use data, wave K). The three items from 2006 were combined with those in 2008 creating a total loneliness score from 1–3 with 3 indicating greater loneliness. The general formulation of these items was as follows: In 2006: Item 1: “How often do you feel you lack companionship?”; Item 2: “How often do you feel left out?”; and Item 3: “How often do you feel isolated from others?”
In 2008: Item 1: “You lack companionship?”; Item 2: “Left out?”; and Item 3: “Isolated from others?”. Initially scaled from 1–3, items were combined together by taking the mean if at most 1 item is missing out of 3 [39, 40]. This resulted in a score ranging between 1 and 3, which was then multiplied by 3. Subtracting 3 from the resulting product, we then obtained a potential range of 0 to 6, with “0” reflecting no or little loneliness and “6” reflecting “extreme loneliness”. Details and code are provided in the Supplementary Methods 2 and in (https://hrs.isr.umich.edu/sites/default/files/meta/2006/core/codebook/h06lb_ri.htm). The loneliness score ordered data was also split into thirds or tertiles using the final selected sample (T1, T2, and T3). Furthermore, also within the final selected sample, a z-score of the loneliness total score was estimated with a unit increase denoting a 1 standard deviation increase in that score. In summary, three forms of the loneliness exposure were used alternatively: (A) The raw form ranging from 0–6; (B) The loneliness score tertiles; (C) The loneliness standardized z-score calculated within the final selected sample, as deemed most appropriate for each type of analysis.
Covariates
Socio-demographic characteristics
The following socio-demographic variables were considered: sex (male, female), age measured in 2010, self-reported race/ethnicity (White versus Black/Hispanic/Other), marital status (never married, married/partnered, separated/divorced, widowed), education (no degree, GED, high school graduate, some college, college degree or higher) work status (working, not working) and total wealth (in US dollars) (<25,000, 25,000–124,999, 125,000–299,000, 300,000+).
Lifestyle factors
Factors falling in the category of lifestyle were also measured in 2010, including smoking status (never smoker, past smoker, current smoker) and frequency of moderate/vigorous exercise (never, 1–4 times per month,>1 times per week).
Health characteristics
The following health characteristics measured in 2010 were considered: self-rated health (excellent/very good/good versus fair/poor), self reported weight and height measures along with existing cardiometabolic risk factors and chronic illness determined by a physician and depressive symptoms measured by an 8-item Centers for Epidemiologic Studies-Depression (CES-D) scale total score. To enhance the sample size, multiple imputation was used with these variables.
Statistical analysis
Data taken from the HRS were analyzed with Stata 18.0 (StataCorp, College Station TX) [41] and sampling design complexity was accounted for [42] using PSU, stratifications, and sampling weights. Multiple imputation using chained equations [43, 44] were used for covariates only, specifically with 5 imputations and 10 iterations. Stata commands mi register, mi stset, mi svyset, mi impute, mi passive and mi estimate were used among others. Missingness ranged between 0% and 1.3% for all variables that were imputed, with up to 270 observations imputed out of over 21,000 in the case of BMI. To estimate population means, proportions, and regression coefficients we used the survey (svy) command. Taylor series linearization were used to adjust standard errors [42]. To compare means and proportions of primary variables across sex and race groups, svy:reg and svy:mlogit commands were used, stratifying on sex and race.
Age at entry > 50 years (i.e., delayed entry) until last age when the event of concern or censoring (loss to follow-up or end of follow-up) occurred is how we defined time-to-event (in years). We defined loss to follow-up as the age respondents were not present for a wave but were alive and responded in the previous wave. Only respondents alive in 2010 were included in the final sample analysis. The time variable used in this analysis was the number of years elapsed between age at the end of 2010 (age at entry), and age at death, censoring or by December 31, 2020. Across the loneliness tertiles and dementia status groups, Kaplan-Meier survival curves were used, along with a log-rank test to evaluate differences in survival functions.
We implemented race- and sex-stratified Cox proportional hazards (PH) models to evaluate the relationship between loneliness, dementia, and all-cause mortality using both reduced (Model 1) and fully adjusted models (Model 2). Age in 2010, sex and race were included in Model 1 while Model 2 further adjusted for education, total wealth, marital status, smoking status, physical exercise, self-rated health, body mass index categories, cardiometabolic risk groups, and CES-D total scores. The main exposures were loneliness as a continuous measure and each “dementia probability” [Ln(odds) (Pr/(1-Pr) transformed; Hurd, Expert and LASSO] (Analysis A) for models 1 and 2. Loneliness and Ln(odds of dementia)’s associations with mortality risk by sex and race were tested for heterogeneity effects by adding 2-way interactions between each exposure and sex or race. Binary dementia status variables and loneliness tertiles as main exposures were applied with a similar analysis (Analysis B).
To test the association of Ln(odds of dementia), Analysis A) or dementia status (Analysis B) and mortality risk across loneliness tertiles, an additional set of models were used (reduced—i.e., Model 1—and fully adjusted—i.e., Model 2) with a similar analytic process as before. Using Cox PH models, each dementia exposure was entered separately with all-cause mortality of all causes as the outcome of interest, while stratifying by loneliness tertile. Loneliness tertiles were tested for heterogeneity in an unstratified model with 2-way interaction terms for each exposure of interest, considering loneliness tertile was an ordinal variable.
Next, we used four-way decomposition to decompose TE into four distinctive components: (1) no interaction or mediation, or controlled direct effect (CDE); (2) interaction is present rather than mediation or reference interaction (INTREF); (3) both an interaction and mediation are present, or INTMED; and (4) mediation is present but not an interaction or Pure Indirect Effect (PIE) (see the Supplementary Methods File) and a summary in Table 1. These models were recently operationalized in Stata using the Med4way command [45] [https://github.com/anddis/med4way]. We considered three alternative potential mediator/moderators, the Ln(odds of dementia) (i.e., Hurd, expert, and LASSO), in the total effect (TE) of loneliness on all-cause mortality risk between 2010 and 2020 and evaluated these relationships using four-way decomposition models. In each of the four-way decomposition models, standardized z-scores for exposures and mediator/moderators were utilized. Mediation and interaction effects of the TE of loneliness z-score on all-cause mortality were tested, along with three Ln(odds of dementia), z-scored, measures utilized as different potential mediator/moderators. In these four-way decomposition models, Cox PH regression was estimated for the exposure/mediator/moderator versus all-cause mortality outcome equation, and OLS regression for each mediator/moderator as predicted by the exposure of interest. Main four-way decomposition models were applied to the total sample, using a reduced set of exogeneous covariates, namely age in 2010, sex and race; with additional models tested stratifying by sex and by race, separately. Consideration of the full model was also used as a secondary analysis. In a similar analytic approach, a four-way decomposition for the TE of Ln(odds of dementia), z-scored, on mortality risk [Ln(odds of dementia, z-scored)-mortality risk analysis] was decomposed using the loneliness z-score as a potential mediator/moderator. As a sensitivity analysis, the TE of loneliness z-score and Ln(odds of dementia), z-scored, in four-way decomposition models were compared with addition of each exogenous variable aside from those included in the reduced model, to test confounding effects of those variables. A type I error of 0.05 was set for all analyses, except for the 2-way interaction terms whereby 0.10 was set [46]. To address multiple testing, we adjusted the type I error using familywise Bonferroni correction accounting for multiplicity in dementia algorithms[47], assuming all other analyses to be independent hypotheses. Thus, the type I error was reduced to 0.017 for main effects and 0.033 for interaction terms, similar to what was done in previous studies (e.g., [48–50]).
Summary of four-way decomposition models
Details are provided in the technical appendix: loneliness-dementia-four-way-decomposition-models.pdf
RESULTS
Of the 6,468 participants that were selected in the final analytic sample, 2,718 were male, 3,564 were female, 5,135 were White and 1,147 were “Black/Hispanic/Other ethnic groups” adults, with an average age of 78.3 years. The mortality rate in this sample was 64 per 1000 person-years (P-Y), overall (Supplementary Figure 1), with a median survival time of 9.9 years and a maximum of 11.2 years. Weighted proportions and means±SE of key characteristics are presented in Table 2, overall, by sex and by racial minority status groups. Male older adults were significantly more likely than female older adults to be married/parternered (74.9% versus 40.4%, p < 0.001). They also were more likely to be currently working (17.6% versus 9.8%), to have a college degree or higher (27.8% versus 15.9%), and less likely to have a total wealth ($)<25,000 (25.3% versus 46.6%). In terms of lifestyle factors, females had a higher proportion of never smokers (53.5% versus 30.4%), though their phyiscal activity level was significantly lower, with 43.9% among females versus 53.2% among males reporting > 1 times/week of physical exercise. BMI within the normal range was a more likely outcome among male adults (46.1% versus 34.0%, p < 0.001). While self-rated health did not differ across sex; male older adults reported≥3 cardiometabolic factors and conditions to a greater extent than their female counterparts (15.4% versus 11.1%, p < 0.001). In contrast, female older adults had on average a higher level of depressive symptoms compared to male older adults (mean±SE: 1.5±0.0 versus 1.0±0.0, p < 0.001). Similarly, loneliness scores, proportion with dementia based on the 3 algorithms, and dementia probabilities were higher among female older adults compared to their male counterparts.
Study sample characteristics: overall, by sex and by race/ethnicity groupsa,b
Abbreviations: LASSO = Least Absolute Shrinkage and Selection Operator; NHW = Non-Hispanic White; SE = Standard Error. aValues are means±SE column percentages for overall and fixed sample characteristics, across sex and race/ethnicity groups, accounting for sampling design complexity. All covariates are measured in 2010. bBased on linear or multinomial logit models using sex or race as main predictors for both continuous and categorical variables, accounting for sampling design complexity. cNumber of chronic conditions among hypertension, diabetes, heart problems and stroke. dLoneliness score had a mean of 1.33 and a standard deviation of 1.56 in the unweighted and unimputed sample. Loneliness tertiles 1, 2 and 3, had means±SD of 0.00±0.00 (n = 2,902), 1.45±0.50 (n = 2,010), and 3.68±1.00 (n = 1,556) in the unweighted and unimputed sample, N = 6,468.
In terms of racial disparities, “Black/Hispanic/Other ethnic groups” older adults had a greater likelihood of dementia based on all 3 algorithms, higher scores on loneliness and depressive symptoms, and significantly higher proportion reporting fair/poor self-rated health or≥3 chronic condition compared to their White counterparts. Furthermore, lower level of physical exercise, current smoking and lower SES in terms of education and income were also more prevalent among “Black/Hispanic/Other ethnic groups” older adults compared to their White counterparts.
Figure 1 presents survival probabilities across loneliness score tertiles and by dementia status (3 algorithmic definitions). Loneliness score tertiles were directly associated with a higher mortality rate, with a dose-response relationship. Notably, dementia status was consistently and strongly associated with all-cause mortality risk.
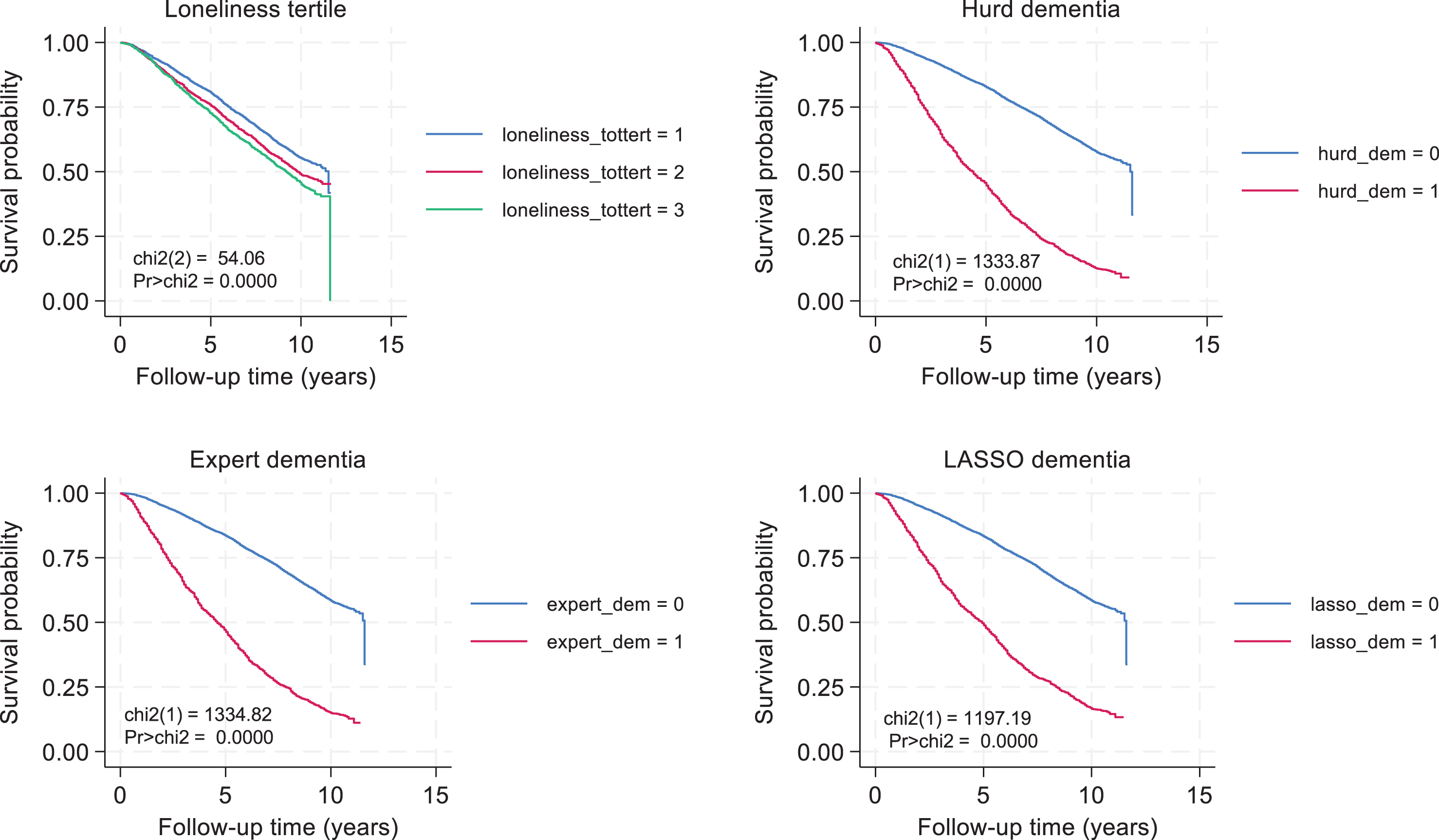
Loneliness score tertile, dementia status, and all-cause mortality: K-M survival curves. Abbreviations: chi2 = Chi-square test, Log-rank test; K-M = Kaplan Meier; dem = Dementia; tert = Tertile.
Table 3 presents Cox PH models that included “Loneliness score” as the main ordinal exposure and the outcome being all-cause mortality risk, displaying adjusted Ln(HR) with their SEs on multiple imputed data. In these Cox PH models, a unit increase on the “loneliness” score was associated with a 1.09-fold increased risk of all-cause mortality [HR = 1.09, 95% CI: 1.06–1.10, p < 0.001] adjusted only for age, sex and race/ethnicity (Table 3). This association was detected among all sex and race sub-groups, without any significant heterogeneity. Nevertheless, upon adjustment for other covariates, including socio-economic, lifestyle and health-related factors, the “Loneliness” score was no longer associated with mortality risk, with an overall HR = 1.01 (0.99–1.02) per unit increase (p > 0.05). In models with the loneliness score tertile as the exposure of interest (Analysis B), each tertile increase in the loneliness score measure was associated with a 16% increase in mortality risk overall and specifically in the reduced model. In the full model, a tertile increase in the loneliness score was not associated with mortality risk (p > 0.05), overall or within any of thesub-groups.
Loneliness, [Ln(odds of dementia), Analysis A] or dementia status (Analysis B) and all-cause mortality: Cox PH models, overall, by sex and by race, HRS 2010–2020a,b
Abbreviations: HRS = Health and Retirement Study; LASSO = Least Absolute Shrinkage and Selection Operator; PH = Proportional hazards; SE = Standard Error. aValues are β±SE, with β representing Ln HR from Cox PH model for each exposure-outcome relationship. Cox PH models were conducted overall and across sex or race/ethnicity groups, accounting for sampling weights and sampling design complexity in multiple imputed data. bAll covariates are measured in 2010 unless stated otherwise. Analysis A included continuous forms of dementia probability (Ln(odds of dementia) and ordinal Loneliness score, while Analysis B included binary dementia status (3 algorithms) and Loneliness tertile. cp < 0.010; dp < 0.001 for null hypothesis that β= 0. eReduced models (Models 1A-1D) were adjusted for age in 2010, sex and race/ethnicity. Full models (Model 2A-2D) further adjusted the reduced model by all covariates described under the Covariates section, including socio-demographic, socio-economic, lifestyle and health-related factors. fp-value associated with 2-way interaction term between sex or race and the main exposure (loneliness score or dementia odds), in a model not stratified by sex or race.
In Table 3, we included three different algorithms to estimate the odds of dementia, which were then entered into a Cox PH model for all-cause mortality risk, using a similar modeling approach to as for the “Loneliness” exposures. The Ln(odds of dementia) were consistently associated with higher mortality risk, with up to 22% higher risk for the LASSO algorithm (reduced model). Upon further covariate adjustment, the association between dementia odds and mortality risk was attenuated for most algorithms, even though the relationship retained its statistical significance at type I error of 0.05. In all these models, a unit increase in the Ln(odds of dementia) corresponded to dementia probability moving from 0% to 73%. Similar patterns were observed for the binary dementia exposures (0 = no, 1 = yes), whereby having a probable dementia diagnosis based on each algorithm was linked to approximately a two-fold increased risk of all-cause mortality in the reduced model, an association that was markedly reduced in the full model though retaining statistical significance (HR 1.5), with no detectable sex or racialdifferences.
Table 4 displays findings from Cox PH models for the relationship between Ln(odds of dementia) and all-cause mortality, stratified by loneliness score tertile. In the fully adjusted and reduced models, there was no heterogeneity detected across loneliness levels, of the association between dementia and mortality, regardless of the algorithm or the definition of the dementia exposure. Thus, dementia status and Ln(odds of dementia) were both associated with mortality risk with comparable strength across loneliness score tertiles.
[Ln(odds of dementia), Analysis A] or dementia status (Analysis B) and all-cause mortality across loneliness tertile: Cox PH models, HRS 2010–2020a
Abbreviations: HRS = Health and Retirement Study; LASSO = Least Absolute Shrinkage and Selection Operator; PH = Proportional hazards; SE = Standard Error. aValues are β±SE, with β representing Ln(HR) from Cox PH model for each exposure-outcome relationship. Cox PH models were conducted overall and across sex or race/ethnicity groups, accounting for sampling weights and sampling design complexity in multiple imputed data. bAll covariates are measured in 2010 unless stated otherwise. Analysis A included continuous forms of dementia probability (Ln(odds of dementia); while Analysis B included binary dementia status (3 algorithms). cp < 0.010; dp < 0.001 for null hypothesis that β= 0. eReduced models (Models 1A-1 C) were adjusted for age in 2010, sex and race/ethnicity. Full models (Model 2A-2C) further adjusted the reduced model by all covariates described under the Covariates section, including socio-demographic, socio-economic, lifestyle and health-related factors. fp-value associated with 2-way interaction term between loneliness tertile entered as an ordinal variable and the main exposure Ln(odds of dementia), in a model not stratified by loneliness score tertile.
Four-way decomposition of the TE of loneliness, z-scored, on mortality risk through Ln(odds of dementia), z-scored, is presented in Table 5, by displaying findings from both a reduced and a fully adjusted model and for all 3 dementia algorithms. In the reduced models, the TE was > 0 and statistically significant for all algorithms and strata, indicating that loneliness was associated with increased risk of mortality independent of age, sex and race/ethnicity. This TE was partially mediated by Ln(odds of dementia), z-scored, with PIE explaining about 21–40% of the TE, depending on the algorithm, indicating that a significant proportion of the TE of loneliness on mortality risk is accounted for pure mediation without interaction. This pattern was observed across all socio-demographic strata. Nevertheless, the TE was markedly attenuated when other exogenous variables were accounted for [e.g., from+0.15±0.020 (p < 0.001) to 0.027±0.021 (p = 0.43), for Hurd algorithm], including other socio-demographic, socio-economic, lifestyle and health-related factors. The PIE remained statistically significant among female and White participants between the fully adjusted and the reduced models, explaining a large portion of the TE (>20% up to 100% of TE).
Loneliness z-score and all-cause mortality: four-way decomposition models by Ln(odds of dementia), z-scored, overall, by sex and by race
Abbreviations: CDE = Controlled Direct Effect; HRS = Health and Retirement Study; INTMED = Mediated Interaction; INTREF = Reference Interaction; LASSO = Least Absolute Shrinkage and Selection Operator; PIE = Pure Indirect Effect; SE = Standard Error; SD = Standard Deviation. aCox PH regression models with mortality as the main outcome and loneliness score (z-scored, 1SD = 1.56 unit increase) as the exposure. [Ln(odds of dementia), z-scored] using Hurd, expert and LASSO algorithms were potential mediators/moderators allowed to interact with the main exposure, sample size N = 6,079 (full model) and 6,468 (reduced model), four-way decomposition analysis. 1 SD for each Ln transformed odds of dementia was 3.8, 3.0, and 2.3, for Hurd, Expert and LASSO algorithms, respectively. bExogenous variables are the ones included in Table 2, Models 1A-2D, as covariates for the reduced and full models, respectively. See Covariates section for detail.
Four-way decomposition of the TE of Ln(odds of dementia), z-scored, on mortality risk through the loneliness z-score is shown in Supplementary Table 1. First, looking at the Hurd dementia algorithm and specifically the reduced model, the positive TE of Ln(odds of dementia), z-scored, on mortality (TE:0.411±0.020, p < 0.001) consisted mainly of a controlled direct effect, CDE (+0.389±0.020, p < 0.001). Nevertheless, around 3.6% of this TE was mediated through a positive association between Ln(odds of dementia), z-scored, and mortality risk (PIE:+0.015±0.003, p < 0.001), another 1.1% was due to both mediation and interaction (INTMED:+0.005±0.002, p = 0.028). After adjustment for other potentially confounding factors, the TE of loneliness z-score retained its statistical significance (p < 0.001), as did the CDE for all 3 algorithms, while PIE became markedly atenuated (p > 0.05).
A sensitivity analysis was carried out to determine the most influential potential confounder in each of the four-way decomposition models, starting from the reduced model. When loneliness z-score was considered as the exposure of interest (as in Table 5), the TE on mortality risk was most influenced by self-rated health and the CES-D score, for all dementia algorithms. When Ln(odds of dementia), z-scored, was the exposure of interest (as in Supplementary Table 1), the most influential potential confounders were physical activity, self-rated health and the CES-D score. Those attenuations in the TE on mortality risk are shown in more detail in Supplementary Figure 2.
DISCUSSION
Summary of findings
This is to our knowledge, the first study to examine bi-directional associations of dementia, loneliness, and mortality, while testing both interactions and mediating effects in a large sample of older US adults using the nationally representative Health and Retirement Study. Among 6,468 individuals with mean age of 78.3 years in 2010 followed up until 2020, we found that female older adults had higher loneliness scores, dementia prevalence, and dementia probability than male older adults. Black/Hispanic/Other ethnic groups among older adults had higher scores on loneliness and depressive symptoms, a greater likelihood of dementia, and a significantly higher proportion of fair or poor self-rated health or chronic conditions than their White counterparts. Among key findings, probable dementia was consistently linked to a two-fold increased mortality risk. The presence of and Ln(odds of dementia) were equally strongly related with mortality risk across tertiles of the loneliness score. The study also found that the loneliness z-score was linked to an elevated risk of mortality regardless of age, sex, or race or ethnicity, and that its TE on mortality was partially mediated by Ln(odds of dementia), z-scored, with up to 40% of TE being a pure indirect effect. In contrast, a very small proportion (<5%) of the TE of Ln(odds of dementia), z-scored, on mortality risk was explained by the loneliness z-score.
Previous studies
Dementia and mortality
The mechanisms underlying these connections between poor cognitive performance assessed in mid- [51] to late-life [52] and an increased risk of death are poorly understood. The intricate interactions between genetic and environmental influences throughout life, which may also affect health and mortality trajectories, are most likely the source of cognitive function. In addition to the social and physical consequences, problems in cognitive function may indicate underlying biological abnormalities or hereditary issues that go beyond neurodegenerative illnesses. Importantly, a meta-analysis of over 60 studies revealed that cognitive impairment, including overt dementia, was linked to a higher risk of death from all causes [53]. In a systematic study, dementia was also linked to higher mortality among COVID-19 patients [54]. It is also well known that the mortality rates of various dementias vary. Particularly, it has been demonstrated that dementias other than Alzheimer’s disease have a higher death rate [55]. Further research is needed to disentangle stages of dementia, cognitive performance, and their mechanistic pathways to mortality risk.
Loneliness and mortality
This study’s findings contribute to existing research that demonstrated loneliness remains a risk factor for mortality in older adults, irrespective of suboptimal lifestyle-related behaviors, underlying biological aging processes, and chronic health problems often associated with natural aging [22]. Prior research has shown that even in European and Asian countries where people tend to live longer than in the US, loneliness increases the risk of mortality [23], underscoring the need for targeted interventions for this age group [24]. Whereas many reports have found that feelings of loneliness were robust predictors of excess risk of death, others have found additional possible pathways wherein these associations are explained by other psychosocial factors or chronic conditions [19, 25]. A study using HRS data from 2002 to 2008 found that the associations of loneliness and increased mortality risk were influenced by health outcomes such as depressive symptoms, self-rated overall health, and functional capabilities [26]. Because older adults are more likely to experience cognitive and physical decline and other aging-related neurocognitive disorders that are risk conditions for mortality, additional work is needed to understand the interplay between loneliness and dementia [27].
Loneliness and dementia
Studies show that feelings of loneliness may be a precursor to diminished cognitive function and dementia in older adults [28–30]. A systematic review including ten studies with adult samples of mean ages 60 years and older reported that loneliness was associated with cognitive decline [31]. Although studies’ neuropsychological test batteries differ, and broad cognitive domains appear to be affected [32], the causal mechanisms remain unclear. In much of this literature, a wide array of measurements has been used to conceptualize loneliness, including the loss of a spouse or partner, living alone and lack of social connections, and perceptions of feeling alone [33]. Loneliness can affect memory recall, executive function (planning, visual cognition), and underlying neuroendocrine and genetic mechanisms that affect brain chemistry and matter [8, 35]. Our study contributes to current body of work that not only might loneliness affect mortality risk by way of poorer health outcomes [21], but dementia may be a plausible pathway as well. Future research should explore how the progression of cognitive decline and impairment influences the strength of these associations.
Strengths and limitations
Our study has several strengths. First, this is the first study to explore the potential bi-directional mediational effects between loneliness and dementia in determining mortality risk. It is also the first to do so in a nationally representative study of older individuals with up to 14 years of follow-up. We may test a wide range of hypotheses using a wealth of data from the HRS while considering any potential confounding effects of unrelated variables. The current study additionally included cutting-edge methodologies, such as multiple imputation applied to variables, Cox proportional hazards models accounting for the complexity of the sampling design, and four-way decomposition models to simultaneously examine mediation and interaction. Our study does, however, have several important limitations. First, even though date of death was known, the analysis contained some measurement error because the date of birth’s precision was only at the month and year levels. Second, a small number of questions that were not verified against other measures, like a full scale with many items, were used to measure loneliness. Third, even though some of these algorithms were based on the comprehensive ADAMS sub-study, measurement error in the algorithmically defined dementia result could not be evaluated. Given the observational nature of the study, selection biases and lingering confounding cannot be ruled out. In fact, we were not able to adjust for diet quality indices or dietary behavior given the limited data available in the HRS on a sub-sample and with few waves available compared with the core data. In addition, we did not include alcohol use among potential exogenous variables, given the strong suggestion of it being a consequence rather than a cause of loneliness. Finally, we cannot rule out the possibility of exposure-induced mediator-outcome confounding given that many of the assumptions of the four-way decomposition models are not empirically testable (see Supplementary Methods File) [56]. We also acknowledge that, to our knowledge, med4way does not account for this potential [56].
Conclusions
In sum, dementia was positively associated with mortality risk, in similar fashion across loneliness score tertiles, while loneliness was associated with mortality risk in the overall sample. The TE of loneliness on mortality risk was partially mediated by dementia probability, particularly when models were only adjusted for age, sex, and race/ethnicity. Future research should further investigate the pathway explaining how loneliness, dementia, and mortality are related to each other. Our findings underscore the potential importance of intervening both on loneliness and dementia to reduce mortality risk.
AUTHOR CONTRIBUTIONS
Michael F. Georgescu (Study concept, plan of analysis, assistance with data management and statistical analysis; literature search and review, write-up of parts of the manuscript, revision of the manuscript); May A. Beydoun (plan of analysis, data management, statistical analysis, literature search and review, write-up of the manuscript, revision of the manuscript); Jason Ashe (Plan of analysis, literature search and review, write-up of parts of the manuscript, revision of the manuscript); Christian A. Maino Vieytes (methodology, literature search and reviews, write-up of parts of the manuscript, revision of the manuscript); Hind A. Beydoun (Literature search and reviews, write-up of parts of the manuscript, revision of the manuscript); Michele K. Evans (Data acquisition, write-up of parts of the manuscript, revision of the manuscript); Alan B. Zonderman (Data acquisition, write-up of parts of the manuscript, revision of the manuscript).
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the HRS staff, investigators and participants and the NIA/NIH/IRP internal reviewers of this manuscript.
Dr. Hind A. Beydoun worked on this manuscript outside her tour of duty at the U.S. Department of Veterans Affairs.
FUNDING
This work was supported in part by the Intramural Research Program of the NIH, National Institute on Aging, National Institutes of Health project number AG000513.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
While the data is owned by the University of Michigan Ann Arbor and HRS is public use data, this work is owned and funded by the National Institute on Aging at the NIH. Scripts used in this analysis will be made available on a GitHub repository: baydounm/HRS_Loneliness_dementia_mortality (github.com). For additional information please contact the corresponding author by e-mail contact at E-mail: