
Abstract
Background:
Social networks and social participation have protective effects on cognitive function maintenance and Alzheimer’s disease and general dementia development.
Objective:
We aimed to investigate the association between conversations and dementia incidence in older adults.
Methods:
This longitudinal prospective cohort study used population data from the National Center for Geriatric and Gerontology–Study of Geriatric Syndromes (NCGG–SGS) from September 2015 to February 2017. The database included 4,167 individuals in Japan aged ≥60 years who were generally healthy and without major cognitive impairment. Participants were classified into two groups according to six daily conversation measures at baseline. The conversation index was calculated as a composite score for these measures. Participants were tracked monthly over 60 months for new-onset dementia.
Results:
Data from 2,531 participants were analyzed (72.7±6.7 years; range: 60–96 years). Dementia incidence per 1,000 person-years was 15.7 (95% confidence interval, 13.6–18.1). The Youden index determined the cut-off point for dementia incidence, with a conversation index of 16/17 points. The low conversation group included more participants with new-onset dementia. Cox proportional hazards regression crude models showed remarkable relationships between dementia onset and specific conversation measurements, including conversation index. According to the Cox regression adjusted model, the cut-off point of the conversation index showed only a remarkable relationship with dementia onset.
Conclusions:
Dementia risk was extensively associated with low daily conversation statuses. The assessment of conversational factors may be useful as a risk indicator for the development of Alzheimer’s disease and general dementia.
INTRODUCTION
In 2022, the older population (≥65 years of age) amounted to 36.2 million, accounting for 29% of the total population [1]. The structure of the disease is changing as the population ages, and dementia, which is particularly prevalent among the older population, is becoming a social concern. The world population is aging, and the World Alzheimer Report estimated that 46.8 million people worldwide lived with dementia in 2015. This number will almost double every 20 years and is estimated to reach 74.7 million in 2030 and 131.5 million in 2050 [2]. The most prevalent cause of dementia is Alzheimer’s disease, accounting for approximately two-thirds of the cases.
Although there is no strong evidence to prevent the onset of dementia-related conditions, including Alzheimer’s disease, potentially effective methods have emerged. The development of the first World Health Organization guidelines for reducing the risk of cognitive decline and dementia was a milestone in dementia risk reduction [3]. The guidelines highlighted the importance of evidence-based healthy lifestyle modifications in delaying or preventing cognitive decline and dementia [3]. However, the WHO’s guidelines on risk reduction for cognitive decline and dementia did not include social participation [3]. Furthermore, social participation, along with cognitive health and dementia risk, has emerged as a potential contributor to general health and well-being. This is because social participation may promote an active lifestyle, reduce stress, and build general health [4]. An extensive systematic review found that low social participation, less frequent social contact, and increased loneliness were considerably associated with new-onset dementia [5]. Additionally, a meta-analysis revealed that poor indicators of social engagement, including poor social networks and inadequate social support, were associated with an increased risk of dementia [6].
Successful social interactions often involve constructing a dynamic mental model of another person’s beliefs, expectations, emotions, and desires, along with the ability to stay focused, solve problems, and pursue goals in distracting environments while inhibiting inappropriate behavior. Many of these tasks require executive functions such as working memory, attention/cognitive control, and inhibition [7]. Furthermore, language skills and executive functions can facilitate social interactions during conversations.
Social isolation, with a lack of social interaction and conversation, is closely associated with psychological health problems, including depression, decreased life satisfaction, and decreased psychological well-being [8], and it can have detrimental effects on physical health, causing cardiovascular, neuroendocrine, and cognitive disorders and mortality [9]. Social isolation has also been associated with biological stress markers such as cortisol response [10], accelerated cellular senescence [11], elevated inflammatory marker levels [12], and sympathetic nervous system activation [13], suggesting that social isolation influences dementia risk through the pathological effects of stress. The important role of systemic inflammation in the etiology of dementia is becoming increasingly recognized [14].
Numerous epidemiological studies have identified that social isolation is associated with negative health outcomes, such as frailty [15], cardiovascular diseases [16], cognitive decline [17], dementia [5], depression [18, 19], disability [20], and mortality [9, 22]; however, limited information is available about how daily conversation affects the health of older adults. Previous research has found that older adults who engage in daily conversation have a significantly lower risk of new onset dementia than those who do not [23]. Dodge et al. conducted a pilot behavioral trial to improve cognitive function in older adults without dementia by enhancing their social interaction through Internet-based conversation. The results indicated high adherence to the protocol, and the intervention groups showed improvements in language-based executive functions within a short period during the trial [24]. The evidence suggests that daily conversation affects cognitive function in older adults. However, it remains unclear how factors, such as the number of different individuals they converse with daily, the duration of their conversations, and the individuals with whom they converse, influence cognitive function maintenance.
Thus, this study aimed to examine the association between daily conversation and the incidence of dementia in older adults.
MATERIALS AND METHODS
Participants
Among those recruited from Takahama, Japan, 4,167 community-dwelling older participants aged ≥60 years participated in the National Center for Geriatric and Gerontology–Study of Geriatric Syndromes (NCGG–SGS) [25]. Participants were selected for this study using the database. The inclusion criteria were residence in Takahama and age ≥60 years at the time of examination (September 2015 to February 2017). The exclusion criteria were as follows: individuals certified by the Japanese public long-term care insurance system to receive routine care (n = 76) and inability to perform activities of daily living, such as eating, dressing, bathing and showering, functional mobility, climbing up and down stairs, personal hygiene and grooming, and toilet hygiene (n = 9); participants with a history of dementia, Parkinson’s disease (n = 16), stroke (n = 219), or depression (n = 97); participants who scored <21 on the Mini-Mental State Examination (MMSE) [26] (n = 67); and participants whose responses contained missing data for the conversation and other measurements (n = 1,145). Informed consent was obtained from all participants before their inclusion in the study. The study protocol was approved by the National Center for Geriatrics and Gerontology Ethics Committee (No 770-1).
Measurements of daily conversations
We assessed the participants’ daily conversations by asking them questions regarding the number of people they interact with daily, conversation durations, speaking durations, frequency of their conversations with family members living together, frequency of conversations with their remote family members, and frequency of conversations with their friends. We created survey items that focused on the frequency of daily conversations because we considered it difficult to simply assess the content of conversations through a questionnaire survey. The questions were as follows: 1) “On an average day of the week, how many people do you talk to, including family members and phone calls?”; 2) “On an average day of the week, how many minutes do you spend talking to someone?”; 3) “How many minutes of this conversation do you speak?”; 4) “How frequently do you have conversations, including phone conversations, with family members who live together and relatives?”; 5) “How frequently do you have conversations, including phone conversations, with remote family members and relatives?”; and 6) “How many conversations, including phone conversations, occur with friends?” For questions 4–6, the frequency of conversation was assessed using the following choices: 1) none; 2) several times monthly; 3) several times weekly; and 4) almost daily. Scoring was performed in this order, from 1 to 4 points. Items 1–3 were scored from 1 to 4 points according to quartiles Q1–Q4.
Measurement of the incidence of dementia
Participants who did not have dementia at baseline and were diagnosed with dementia during the 60-month follow-up period were considered to have new-onset dementia, and data were collected from the Japanese National Health Insurance System and Japanese Long-Term Care Insurance System. In Japan, all adults aged ≥65 years have public health insurance, which includes one of the following: health insurance for employed individuals (Employees’ Health Insurance), national health insurance for unemployed and self-employed individuals aged <75 years (Japanese National Health Insurance), or health care for individuals aged ≥75 years (Later-Stage Medical Care). In the present study, the participants were followed up monthly for new-onset dementia (Alzheimer’s disease, vascular dementia, frontotemporal dementia, or other dementia subtypes) as recorded by the Japanese National Health Insurance and Later-Stage Medical Care. Participants were considered to have dementia based on a diagnosis made by physicians according to the International Classification of Diseases-10. We identified cases of dementia from the NCGG–SGS data according to the corresponding International Classification of Diseases-10 codes (Table 1). The diagnosis of dementia from the UK Biobank inpatient data, which have similar criteria to the NCGG–SGS (Table 1), has been previously validated and showed a positive predictive value of 87.3% for any dementia compared with the clinical expert adjudication of full-text medical records [27].
ICD-10 codes used to identify dementia cases in UK Biobank and NCGG–SGS
ICD10, International Classification of Diseases-10; UKB, UK Biobank; JNHI, Japanese National Health Insurance; LSMC, Later-Stage Medical Care; AD, Alzheimer’s disease; VaD, vascular dementia; FTD, frontotemporal dementia; O, other dementia subtype; N, no subtype specified.
The Long-Term Care Insurance System is a mandatory form of social insurance to support the daily lives of older adults with disabilities [28, 29]. In Japan, all individuals aged ≥65 years are eligible for institutional or community-based services depending on their disability level, and those aged ≥40 years with disabilities related to aging, such as cerebrovascular disease, are also eligible to access benefits. The disability certification process consists of two parts: (i) the degree of disability based on a questionnaire developed by the Ministry of Health, Labor and Welfare of Japan and (ii) a physician’s written opinion prepared by the attending physician [30]. We identified dementia based on the level of independence in the daily living of older adults with dementia in the disability certification process. The level of independence is classified into five ranks from mild to severe (I, II, III, IV, and M), and individuals who had moderate dementia-related behavioral disturbance and cognitive impairment with slight dependence were classified as rank II. We defined dementia as the determinant of rank II or higher symptoms derived from a primary care physician’s written opinion. The criteria were the same as those used in previous studies in Japan [31–34].
Potential confounding factors
Dementia results from a combination of various factors occurring over time, including demographics and chronic conditions. All multivariate-adjusted models reported include the following covariates unless otherwise noted: age at enrollment, sex, educational level, presence of chronic conditions, and cognitive impairment as defined by an MMSE score of ≤23. The following self-reported chronic conditions were included in the model: hypertension, heart and lung disease, osteoarthritis, and diabetes mellitus [35, 36].
Statistical analyses
Participants were classified into four groups according to quartiles: number of people involved in daily conversations, conversation times, speech times, conversations with family members living together, conversations with remote family members, and conversations with friends. Conversation scores were calculated by assigning 1–4 points to Q1 through Q4 and 1–4 points for conversation frequency, with higher scores indicating increasing frequency of conversations. These total scores were used as the conversation index score (range 6–24 points). Curves for receiver operating characteristics were examined to identify cut-off points for the conversation score that best discriminated between those with dementia development and those without. Cut-off points for maximizing the sensitivity and specificity for each test were determined using the Youden index [37]. Participants were classified into those with low conversation scores (low conversation group) and those with high conversation scores (high conversation group) based on the cut-off points of the conversation score. Analysis of variance, Student’s t-test, and Pearson’s chi-squared test were performed to assess differences in baseline characteristics between participants with and without dementia. A chi-squared test with adjusted standardized residuals was used to determine whether daily conversations significantly affected dementia. The residuals followed the t distribution: t > 1.96 was accepted as an indication of p < 0.05 and t > 2.56 as an indication of p < 0.01. In the univariate analyses of the incidence of dementia, participants who moved away or died were excluded.
We calculated the cumulative incidence of dementia during follow-up according to baseline conversation status grouping. Associations between conversations and dementia incidence were analyzed using Cox proportional hazard regression models. Crude and multivariate models adjusted for demographic variables, primary diseases, and cognitive impairment were used as potential confounders. HRs for the incidence of dementia were estimated, and 95% CIs were calculated. SPSS (version 25.0; IBM, Armonk, NY, USA) was used for all statistical analyses. Statistical significance was set at p-values of <0.05.
RESULTS
Among the initial 4,167 participants, 1,636 were excluded, and data from 2,531 participants were analyzed (1,024 males and 1,507 females) (Fig. 1). The mean age of the participants was 72.7±6.7 years (range: 60–96 years).
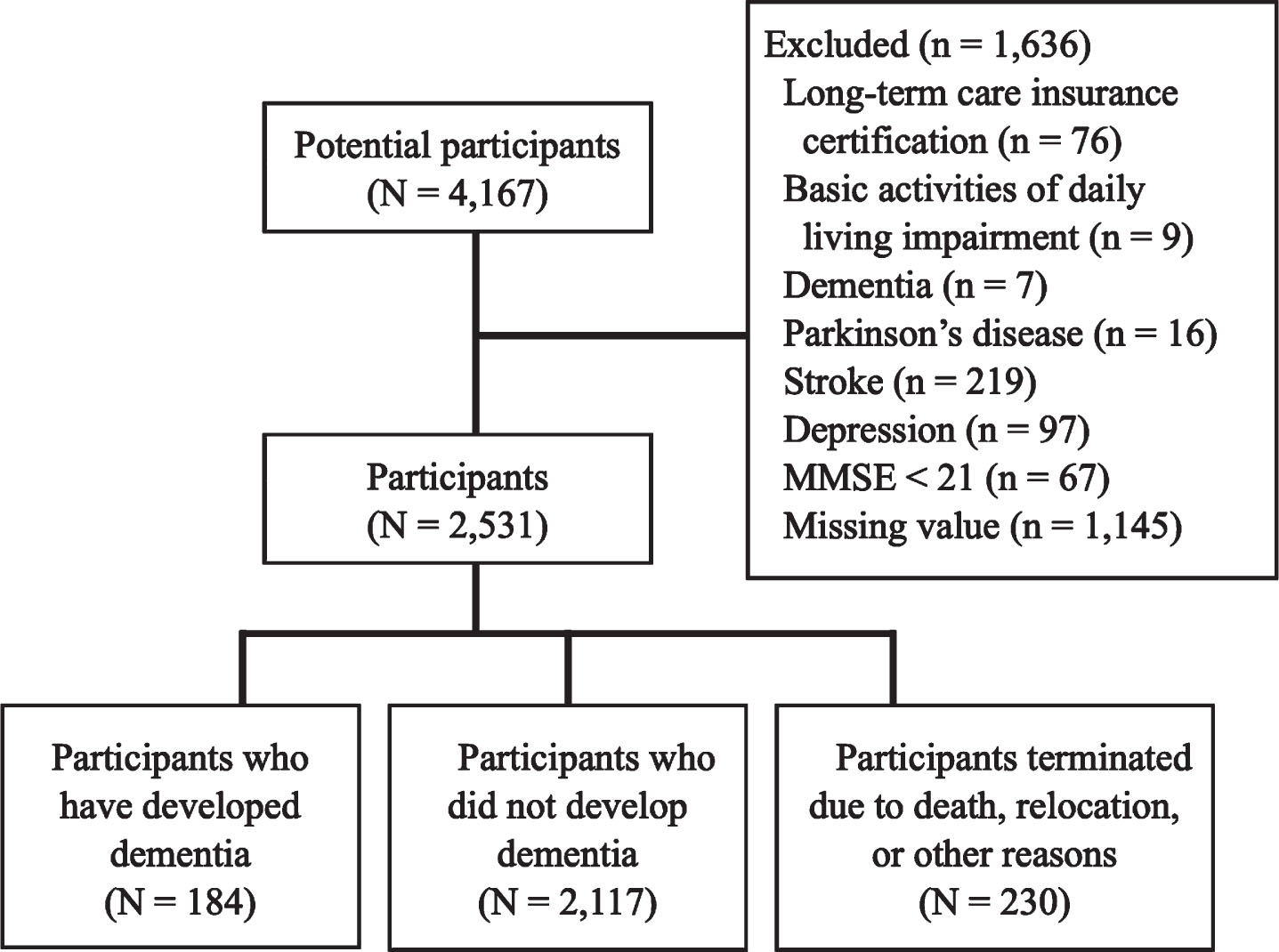
Flow chart of participant enrollment. MMSE, Mini-Mental State Examination.
One hundred eighty-four participants (7.3%) were diagnosed with dementia; 29 (1.1%) moved away from Takahama City, 140 (5.5%) died during the follow-up period, and 61 (2.4%) were terminated for other reasons. The incidence of dementia per 1,000 person-years (95% CI) among all participants was 15.7 (13.6–18.1).
Table 2 presents the possible confounding factors for dementia incidence in the participants grouped according to the presence or absence of dementia. Significant differences (p < 0.05) were found in age; educational level; presence of hypertension, osteoarthritis, or diabetes mellitus; cognitive impairment; number of people spoken to daily; conversation times; speech times; frequency of talking with family at home; talking with family outside of home; talking with friends; and conversation index (Table 2).
Baseline characteristics of study participants stratified by the development of dementia
*: n (%).
The Youden index was used to determine the cut-off point for dementia incidence, resulting in a conversation index of 16/17 points. The incidences of new-onset dementia diagnoses per 1,000 person-years were 20.7 (95% CI, 17.3–24.8) and 11.0 (95% CI, 8.7–14.0) for the low and high conversation groups, respectively. Notably, more participants with new-onset dementia were reported in the low conversation group (p < 0.01).
Cox proportional hazards regression models were used to analyze the association between conversations and the incidence of dementia (Table 3). Regarding the crude model, compared with the Q1 group or the participants who did not talk with family or friends per HR and 95% CI, a significantly higher dementia incidence was found in Q3 and Q4 regarding conversation times (Q3 : 0.51, 0.28–0.93, Q4 : 0.49, 0.32–0.77); in Q2, Q3, and Q4 regarding speech times (Q2 : 0.67, 0.46–0.98, Q3 : 0.60, 0.41–0.89, Q4 : 0.46, 0.30–0.70); in Q4 regarding talking with family at home (Q4 : 0.57, 0.37–0.87); and in the cut-off point of the conversation index determined using the Youden index (0.53, 0.39–0.72) (Fig. 2, left panel). In the adjusted model, the cut-off point for the conversation indexes remained only significantly related to dementia incidence (0.67, 0.49–0.91) (Table 3, Fig. 2, right panel).
Hazard ratios for dementia incidence in the crude and adjusted models

Cox survival estimates for dementia incidence according to high and low conversation volumes. Left panel: Hazard estimates of dementia incidence in the crude model. Right panel: Hazard estimates of dementia incidence in the adjusted model (age, sex, education, chronic medical conditions, and cognitive impairment).
DISCUSSION
In this prospective study, dementia risk was extensively positively associated with conversation times, speech times, talking with family at home, and conversation indexes. Previous results from our longitudinal study indicated that the risk of dementia was considerably lower in participants involved in daily conversations, driving, shopping, fieldwork, and gardening, among many other lifestyle activities [23]. This suggests that social interactions, including daily conversations, may act as stimuli to preserve cognition or prevent cognitive decline. Therefore, knowledge of social requirements and interventions to ensure social conversation in older adults may help to reduce older adults’ risk of developing dementia [38].
Poor social relationships are associated with cognitive decline in the general population, according to a meta-analysis of 19 longitudinal cohort studies [39]. In contrast, an active and socially integrated lifestyle appears to be associated with a lower risk of developing dementia [40]. In people with dementia, a good social network protects against rapid cognitive and functional decline [41]. These findings suggest that maintaining social connections in old age effectively reduces functional decline and the onset of dementia.
In this study, we investigated the relationship between the onset of dementia and daily conversation status in six aspects: the number of people in daily conversations, conversation times, speaking times, frequency of conversations with family members living together, frequency of conversations with remote family members, and frequency of conversations with friends. After adjusting for potential confounders, none of the items of daily conversation was found to be associated with the development of dementia, except the total conversation index score. We believe that each daily conversation item captures only one aspect of conversation, and that the total score of each item is associated with the development of dementia, suggesting the importance of measuring the frequency of conversations. Moreover, these findings suggest the need to assess daily conversations from multiple perspectives. In addition, an interventional study on dementia prevention through conversations may require a comprehensive research plan that promotes more conversations.
A behavioral pilot randomized controlled trial designed to improve cognitive function by enhancing social interaction through Internet-based conversations showed that the intervention group had improved language-based executive functions in older adults without dementia [24]. The intervention group had face-to-face interviews with trained interviewers 5 days a week for 6 weeks, 30–35 min per session, using a dedicated video chat-enabled personal computer provided to each participant. Conversations emphasized spontaneous rather than structured responses. This randomized controlled trial clearly showed that conversations with others over the internet can also improve cognitive functions. Therefore, it is necessary to investigate conversations with people other than family and friends in addition to the current survey items. Social contact with others may increase cognitive adaptability, improving an individual’s ability to tolerate neuropathologies [42]. An autopsy study found that the relationship between neuropathology and cognition changed with the amount of social contact a person had before death. This supports the hypothesis that people with more social contact have greater cognitive reserves and higher amyloid burdens and that neurofibrillary tangle density is not more strongly associated with cognitive decline in people with more social contact [43]. Further interventional studies are needed to determine the extent to which conversations effectively preserve cognitive function and prevent dementia in older adults.
Limitations
This study has some limitations. First, the participants were not randomly recruited, which may have resulted in an under representation of cognitive impairment because the participants were sufficiently healthy to undergo health examinations. Second, data were not collected for dementia subtypes (e.g., Alzheimer’s disease, vascular dementia, dementia with Lewy bodies, and frontotemporal dementia). Thus, the data did not allow inferences regarding the correlation between conversations and dementia pathologies. Third, we were unable to contact informants (e.g., family members) to verify the medical records, lifestyle information, or asymptomatic aberrant behavior of some participants. This may have led to an underestimation of the incidence of dementia because of the absence of early-onset dementia. Fourth, information about participants’ medical conditions and comorbidities was collected through self-reports, and because we did not have access to medical records, we could not confirm these reports. Finally, the diagnosis of dementia may have been made by a physician who is not a dementia specialist. Therefore, new-onset dementia may not have been accurately recorded. This problem, together with the presence of patients who are hesitant to visit a doctor, may lead to an underestimation of the diagnosis of dementia.
The strengths of this study are as follows: our findings are consistent with those of comprehensive geriatric assessments designed to identify the status of daily conversations. To the best of our knowledge, this is the first study to use a large population-based sample to examine the correlation between conversations and dementia incidence.
Conclusions and implications
In summary, the risk of dementia was markedly positively associated with a low conversation time, speech time, frequency of talking with family at home, and conversation index. However, none of the daily conversation items were associated with the development of dementia after adjusting for potential confounders. In contrast, the total conversation index score remained considerably associated with new-onset dementia in the multiple adjustment model. These findings indicate that older adults who partook in a low quantity of conversation faced an elevated risk of new-onset dementia compared with those with high total conversation quantities. These findings could influence the health-related guidelines and recommendations for older adults, and the knowledge gained by patients and clinicians could help reduce the incidence of Alzheimer’s disease and other dementia-related conditions. Future studies should collect specific data for each subtype of dementia to provide an in-depth analysis of the effect of conversation on the incidence of the different conditions.
AUTHOR CONTRIBUTIONS
Hiroyuki Shimada (Conceptualization; Formal analysis; Funding acquisition; Project administration; Writing – original draft); Takehiko Doi (Writing – review & editing); Kota Tsutsumimoto (Investigation; Writing – review & editing); Keitaro Makino (Conceptualization; Investigation; Writing – review & editing); Kenji Harada (Investigation; Writing – review & editing); Kouki Tomida (Investigation; Writing – review & editing); Hidenori Arai (Supervision).
Footnotes
ACKNOWLEDGMENTS
The authors acknowledge the substantial contributions of the dedicated and skilled staff to the NCGG–SGS. The authors also appreciate the NCGG–SGS, who volunteered to participate in this study. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
FUNDING
This study was supported by the Japan Society for the Promotion of Science (Grant-in-Aid for Scientific Research (A), 26242059), Ministry of Health, Labor and Welfare (Research project on health and welfare promotion for older people), the National Center for Geriatrics and Gerontology (Research Funding for Longevity Sciences 27-22), Japan Agency for Medical Research and Development (15dk0107003h0003, 15dk0207004h0203), Research Institute of Science and Technology for Society (RISTEX), and Japan Science and Technology Agency (JST) (Japan and Solution-Driven Co-creative R&D Program for SDGs (SOLVE for SDGs): Preventing Social Isolation & Loneliness and Creating Diversified Social Networks:22-221037254). The funding source played no role in the design or conduct of the study; the collection, management, analysis, and interpretation of the data; and the preparation, review, or approval of the manuscript.
CONFLICT OF INTEREST
HS received grants from the Kanagawa Prefectural Government, Nagoya City Local Government, Obu City Local Government, FUJISOFT INCORPORATED, and TOYOTA MOTOR CORPORATION during the study period. TD received grants from the Japan Society for the Promotion of Science. KT received grants from the Japan Society for the Promotion of Science. HA received grants from the National Center for Geriatrics and Gerontology and the Japan Agency for Medical Research and Development during this study. The other authors have no conflicts of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article. The corresponding author can be contacted for further inquiries.