
Abstract
It has been reported that social engagement may be associated with dementia risk. We searched PubMed, EMBASE, PsycINFO, CINAHL, LILACS, Biomed Central, Scopus, and Web of Science from January 2012 – May 2017, supplemented by extraction from previous reviews. We included cohort and case-control studies examining the association between social engagement or loneliness and dementia risk, pooling data using a random-effects model. Registered: PROSPERO (CRD42017067074). We included 31 cohort and 2 case-control studies comprising 2,370,452 participants. Poor social engagement indices were associated with increased dementia risk, including having a poor social network (RR = 1.59, 95% CI 1.31–1.96; I2 = 0.00%) and poor social support (RR = 1.28, 95% CI 1.01–1.62; I2 = 55.51%). In long-term studies (≥10 years), good social engagement was modestly protective (RR = 0.88, 95% CI 0.80–0.96; I2 = 0.00%). Loneliness was non-significantly associated with increased risk (RR = 1.38, 95% CI 0.98–1.94; I2 = 45.32). Our findings encourage interventions targeting social isolation and disengagement for dementia prevention.
Keywords
INTRODUCTION
Alzheimer’s disease and other dementias are increasing globally, particularly as the population ages. The estimated lifetime risk of Alzheimer’s disease at age 45 is 10.3% for men and 19.5% for women [1, 2], and the worldwide cost of the dementias in 2015 was an estimated US$818 billion, a 35% increase since 2010 [3]. Research has primarily focused on the identification of novel biomarkers for Alzheimer’s disease, as well as therapies which may delay or halt disease progression. However, Alzheimer’s disease drugs such as γ- and β-secretase inhibitors and anti-amyloid immunotherapies have not been shown to be clinically efficacious in Phase III clinical trials [4–7].
Consequently, the focus has shifted toward preventive strategies for the dementias. A delay in onset of dementia of just a few years has the potential to dramatically reduce its prevalence. Physical activity, cognitive training, and dietary modification are among the potentially beneficial strategies to attenuate cognitive decline, although what combination of these factors is most effective is unclear [8, 9]. Over the past two decades social engagement has been investigated as a potential protective factor against cognitive decline and dementia [10, 11]. A previous meta-analysis of 19 longitudinal studies, which synthesized evidence up to July 2012, found that low social participation, less frequent social contact, and greater loneliness were all associated with an increased risk of dementia [12]. The present systematic review and meta-analysis has been necessitated by the substantial expansion of literature in the past five years. We systematically reviewed the evidence of associations between social engagement, loneliness, and dementia risk from observational studies, and performed meta-analyses to produce quantitative risk estimates.
METHODS
Search strategy and study selection
The protocol for this review was registered at PROSPERO (CRD42017067074). We performed a systematic review of the relationship between social engagement and cognitive decline or dementia; the present manuscript reports on our findings only for the subset of studies relating social engagement and loneliness to dementia. We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [13, 14]. First author RP performed a systematic search of the databases PubMed, EMBASE, PsycINFO, CINAHL, LILACS, Biomed Central, Scopus, and Web of Science, supplemented by a manual search of reference lists, limited to the period 01 January 2012 – 26 May 2017. We also extracted references from previous systematic reviews [11, 12] covering identified published cohort studies up to July 2012. Our search strategy was thus designed to capture all published longitudinal observational studies to late May 2017. Search terms are detailed in Supplementary Table 1.
Studies were included that: 1) were case-control or cohort studies; 2) included any social engagement assessment at any age; relating it to 3) dementia diagnosis; and, 4) were published, full-length, English-language journal articles. Studies not meeting all inclusion criteria were excluded. Additionally, studies were excluded from the meta-analysis if they reported on similar associations derived from the same cohorts, to prevent duplication of data. In these cases, data were derived from the articles with the longest follow-up times.
Data extraction
For all included studies, RP used a standardized data extraction form to extract: study title, date, authors, location, mean age at baseline, gender, sample size, mean/median/maximum years of follow-up, adjustment for important covariates (age, sex, education, depression, physical activity), method(s) of social engagement and dementia assessment, effect sizes (ESs) for associations between social engagement and dementia risk, confidence intervals, and p-values for statistical comparisons.
Data synthesis
Meta-analysis was performed using a random effects model [15] with the metafor package [16] in R (version 3.4.1), using RStudio (version 1.0.153) [17]. Odds ratios (ORs), risk ratios (RRs), and hazard ratios (HRs) were all pooled in the same analyses, in a similar protocol to that used in a previously published meta-analysis on this topic [12]. The robustness of this pooling decision was investigated by performing subgroup analyses by ratio used in reporting the result. Pooled risk ratios were calculated with 95% confidence intervals (95% CIs). We investigated the associations with dementia risk for good social engagement, poor social engagement, and loneliness. ‘Good’ and ‘poor’ social engagement each captured any facet of social engagement that could be considered positive or negative. For example, good social engagement included strong social networks, high levels of social support, and high social satisfaction, while poor social engagement included social isolation, lack of social support, and having few social contacts. For the purpose of this review, loneliness is defined as the subjective perception of having insufficient social networks or contacts. This is distinct from structural social isolation or lack of social support, which may be measured objectively; an individual may be isolated but not lonely, and vice versa, and as such it is important to consider these variables separately. We also performed analyses based on specific aspects of social engagement and dementia risk: marital status, living situation, social network size, degree of social support, degree of social satisfaction, frequency of social contacts, and frequency of participation in social activities.
We quantified heterogeneity using the I2 statistic, where I2≥75.00 indicated substantial heterogeneity, with p < 0.05 defined as statistical significance. Results with substantial heterogeneity are reported, but not used to draw conclusions. We performed subgroup analyses based on study quality, follow-up time, geographical region, sample size, and adjustment for depression, to investigate for potential sources of heterogeneity. We used Egger’s regression test with funnel plots to assess potential publication bias, where p < 0.05 indicates significant publication bias [18] in which case, we used the Rosenthal approach to calculate the fail-safe N. Generally, if the fail-safe N is greater than 5n+10, where n is the number of studies included in the meta-analysis, it is unlikely that there were enough studies missing from the literature to nullify the observed result to statistical non-significance [19].
Quality and bias assessment
RP performed study quality and bias assessment using the Newcastle-Ottawa Scale (NOS) [20], which rates studies via a star system of up to nine stars. We considered studies that achieved scores of ≤5 stars to be poor quality, 6–7 stars to be adequate to good quality, and of 8–9 to be excellent quality. Subgroup analyses were pre-planned, stratifying by quality.
Inter-rater reliability
For the wider review from which this sub-study is derived, A-NC independently performed a search of the databases PsycINFO and CINAHL. Inter-rater reliability for study selection was calculated using Cohen’s kappa (κ) statistic, using McHugh’s guidelines to interpret strength of agreement [21]. For the 3,343 titles mutually reviewed, the unweighted Cohen’s κ was 0.83 (95% CI 0.72–0.93), which by McHugh’s criteria can be considered strong agreement. All discrepancies were resolved by consensus. Similarly, A-NC performed the quality assessment with the NOS on a subset of fifteen articles selection for inclusion. Agreement was again strong, with an unweighted Cohen’s κ of 0.89 (SE = 0.042, 95% CI 0.81–0.98) for quality assessment.
RESULTS
Study selection
The study selection process is illustrated in Fig. 1. In brief, our search yielded 32,189 potentially relevant citations, of which 87 studies were included in the broader review, and for the current review we included the 33 studies in which the outcome was clinical diagnosis of dementia [11, 22–53].

Study selection flow chart, with reasons for exclusion.
Study characteristics
Study characteristics are shown in Table 1, including 31 cohort studies and two case-control studies. Approximately one-half of the studies were conducted in Europe (18/33, 55%), with the remainder in North America (8/33, 24%) or Asia (7/34, 21%). More than one-half of the studies (18/33, 55%) were published after 2012, confirming the significant expansion in the literature since the previously published systematic review [12]. The follow-up times ranged from one to 32 years, median 7 years. Sample sizes ranged from 220 to 2,288,489 with a median of 1,609.
The social engagement measures and criteria used for dementia diagnosis for each study are summarized in Supplementary Table 2. Only eight of the 33 studies (23%) used validated scales to assess social engagement or loneliness, such as the Berkman-Syme Social Network Index, [54] the Lubben Social Network Scale, [55] and the de Jong-Gierveld Loneliness Scale [56, 57]. Dementia diagnosis was most often done in accordance with validated, reliable criteria, such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria from the revised third (DSM-III-R) [58] or fourth editions (DSM-IV) [59]. Among the studies included, 24 (73%) diagnosed dementia via a structured interview with independent clinicians, while 9 (27%) used other methods, such as extraction of diagnostic codes from databases, computer-assisted protocols, or self-or informant-report of diagnosis.
Studies included in systematic review reporting on social engagement or loneliness in association with risk of dementia
n, number of participants; Edu, education; Dep, depression; PA, physical activity; RR, relative risk; 95% CI, 95% confidence interval; NR, not reported; HR, hazard ratio; OR, odds ratio; AD, Alzheimer’s disease; VaD, vascular dementia; MCI, mild cognitive impairment. *Split up into two studies, one in the community (top row), and one in institutionalized individuals (bottom row).
Four studies reported specifically on the association between loneliness and dementia risk [22, 38]. For these, the median follow-up time was 5.9 years (range 3.0–10.0). Generally, loneliness assessed with single questions in questionnaires, with only Wilson et al. in the Rush Memory and Aging Project using a validated scale [27].
Quantitative synthesis
Table 2 summarizes the results of the meta-analyses performed. In a meta-analysis of 15 studies, poor social engagement was associated with increased dementia risk (RR = 1.41, 95% CI 1.21–1.65), with substantial heterogeneity (I2 = 94.34), but no publication bias (p = 0.13). Considering specific components of poor social engagement, being unmarried (see Supplementary Figure 1A; 8 studies; RR = 1.63, 95% CI 1.37–1.94; I2 = 90.90) and having a poor social network (6 studies; RR = 1.59, 95% CI 1.31–1.93; I2 = 0.00) were associated with the greatest magnitude increase in dementia risk. Four studies reported on the association between loneliness and risk of dementia, with a non-significantly increased risk of dementia seen in meta-analysis (see Supplementary Figure 1B; 5 studies; RR = 1.38, 95% CI 0.98–1.94; p = 0.063; I2 = 45.32).
Meta-analysis results
n, number; RR, relative risk; N. America, North America; CCS, case-control study; NOS, Newcastle-Ottawa Scale; N/A, not applicable. No heterogeneity result was calculable for the association ‘being married’, as only one study was included. This result is just reported; it was not included in a meta-analysis.
Overall, in a meta-analysis of seventeen studies, good social engagement was protective against dementia (RR = 0.81, 95% CI 0.74–0.88; I2 = 68.06). This result had significant publication bias (p < 0.001). However, the calculated fail-safe N of 393 was larger than the 5n+10 value of 100 studies, indicating it is unlikely that any potentially missed or unpublished studies could substantially impact our finding. Examining more specific measures, we found that being married (one study only; RR = 0.68, 95% CI 0.47–0.99), having many social contacts (8 studies; RR = 0.85, 95% CI 0.77–0.93; I2 = 69.15), and having a high level of social activity (6 studies; RR = 0.62, 95% CI 0.48–0.82; I2 = 60.21) were all protective against dementia. An extensive social network, strong social support, or high social satisfaction conferred no protection. No associations had substantial heterogeneity (I2 > 75.00).
Subgroup analyses
We performed pre-planned subgroup analyses; full results are available in Table 2. In brief, we found geographical differences in risk estimates. Good social engagement was more protective against dementia in studies conducted in Asia (see Fig. 2A; RR = 0.54, 95% CI 0.35–0.84; I2 = 30.79) and North America (RR = 0.60, 95% CI 0.49–0.73; I2 = 0.00) than in Europe (RR = 0.90, 95% CI 0.85–0.95; I2 = 37.36). Poor social engagement was not associated with dementia risk in North American studies (RR = 1.16, 95% CI 0.84–1.62; I2 = 35.28), but was for European (RR = 1.40, 95% CI 1.22–1.61; I2 = 87.69) and other (RR = 2.04, 95% CI 1.14–3.65; I2 = 58.38) cohorts.
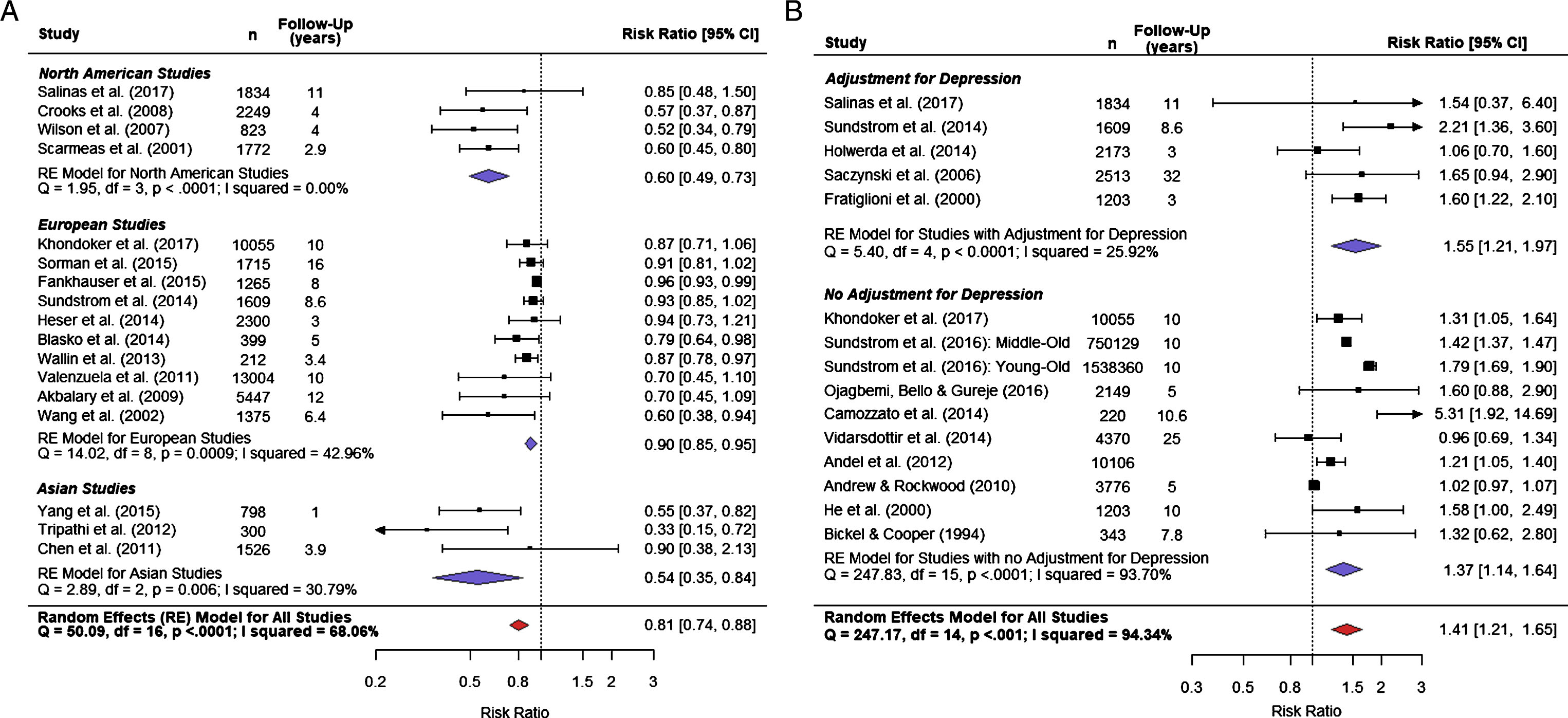
(A) Good social engagement is protective against dementia (Pooled RR = 0.78, 95% CI 0.71–0.86), with some differences based on geographical location; and (B) In studies which adjusted for the important confounder of depression, poor social engagement was associated with an increased risk of dementia (Pooled RR = 1.56, 95% CI 1.29–1.88, p < 0.001).
Studies which adjusted for depression found that good social engagement was still protective against dementia (RR = 0.87, 95% CI 0.79–0.96; I2 = 59.91), though with a somewhat attenuated estimate of protection compared to those studies which did not adjust for depression/depressive symptoms (RR = 0.74, 95% CI 0.63–0.87; I2 = 66.17). In contrast, when considering whether poor social engagement was a risk factor for dementia, those studies which adjusted for depression/depressive symptoms found a greater magnitude of increased risk (see Fig. 2B; RR = 1.57, 95% CI 1.21–1.97; I2 = 25.92) than those which did not adjust for depression (RR = 1.37, 95% CI 1.14–1.64; I2 = 96.25). Thus, the presence/absence of depression as a co-morbid condition appeared to account for some of the benefits of good social engagement, but exaggerate the harms of poor social engagement.
There were no substantial differences in ESs noted in the subgroup analysis for follow-up time in the analysis of poor social engagement and dementia risk. However, for good social engagement and dementia risk, studies with a longer follow-up of ten or more years found an attenuated but still significant protective benefit (RR = 0.88, 95% CI 0.80–0.96; I2 = 0.00) when compared to studies with a shorter follow-up (RR = 0.80, 95% CI 0.681–0.94; I2 = 74.60).
Quality and bias assessment
The median NOS score was seven stars out of a possible maximum of nine, indicating the generally high quality of included studies. Thirteen studies scored eight or nine, indicating excellent quality. Fifteen studies scored six or seven, indicating adequate or good quality. Five remaining studies scored less than six stars, indicating poor quality. We performed subgroup analyses, stratifying studies into those with excellent quality (eight or nine stars) and those with poor or adequate quality (fewer than eight stars). For poor social engagement and dementia risk, we found that excellent quality studies showed a stronger risk estimate (see Supplementary Figure 1C; RR = 1.55, 95% CI 1.17–2.05) with only mild, non-significant heterogeneity (I2 = 44.44; p = 0.14), while other studies had a more attenuated risk estimate (RR = 1.37, 95% CI 1.14–1.64) with substantial heterogeneity (I2 = 95.83; p < 0.001). By contrast, for good social engagement and dementia risk, we found a somewhat attenuated estimate of protective effect for excellent quality studies (RR = 0.85, 95% CI 0.78–0.93; I2 = 68.27) compared to others (RR = 0.72, 95% CI 0.60–0.88; I2 = 51.47).
DISCUSSION
Summary and significance of findings
In this review, the weight of the evidence supports an association between poor social engagement and dementia risk; however, the evidence for a protective effect against dementia derived from good social engagement is tenuous. While good social engagement overall was associated with an approximately 19% reduction in risk of dementia, the presence of moderate heterogeneity and significant publication bias precludes firm, unbiased conclusions. By contrast, we found that living alone, having a limited social network, low frequency of social contact, and inadequate social support were all risk factors for dementia, without substantial heterogeneity or publication bias. In subgroup analyses, we found that in studies which adjusted for the potentially important confounding factor of depression, overall poor social engagement was associated with an even greater 56% increased risk of dementia with no heterogeneity or publication bias. Similarly, when considering only those studies of the highest quality (NOS≥8), the association between poor social engagement and dementia risk was maintained at approximately 55% increased risk, with only mild heterogeneity (I2 = 44.44). This is strong evidence for poor social engagement as a risk factor for dementia. Furthermore, the finding that the combination of depression and poor social engagement magnified the risk of poor engagement has important clinical implications, as it supports the view that poor social engagement is not simply a marker for depressive symptoms, and there is additive risk for dementia when both are present. It cannot be assumed that addressing only one of these two is sufficient to optimally reduce dementia risk. By contrast, the findings suggest that good social engagement and fewer depressive symptoms may overlap in individuals, and are thus not entirely independent protective factors for dementia.
There is increasing evidence supporting the notion that loneliness should be considered separately to structural social isolation in epidemiological studies on socialization. It is entirely possible for an individual to have a complex and highly interconnected social network, but to still feel lonely, or conversely for a socially isolated individual to feel contented with their level of socialization. For this reason, we included loneliness as a separate parameter for investigation in the meta-analysis. We noted a non-significant trend toward increased risk of dementia associated with loneliness (p = 0.063). However, relying on only four included studies, this meta-analysis does not provide conclusive evidence for or against loneliness as a risk factor for dementia. This is particularly true considering that only one of the four included studies examining loneliness used a validated scale to do so; the remaining studies relied on single or a few questions in questionnaires, which may not be effective in fully assessing an individual’s degree of loneliness. In future studies investigating social engagement and dementia, a validated scale for loneliness such as the UCLA Loneliness Scale and De Jong Gierveld Loneliness Scale should be included in addition to typical scales on structural and functional aspects of socialization in order to fully elucidate each participant’s holistic social experience.
Neurobiological hypotheses: The social causation model
The social causation model proposes that socialization directly or indirectly causes cognitive changes and modulates dementia risk via a neurobiological mechanism [10]. For example, the stress hypothesis postulates that hypersecretion of glucocorticoids in the stress response causes accelerated hippocampal degeneration and hence predisposes to cognitive deficits or dementia [60]. The vascular hypothesis argues that social engagement, by minimizing cardiovascular risk factors, attenuates the risk of neurodegenerative disease. These hypotheses have some evidential support, but are not as compelling as a third model, the cognitive reserve hypothesis. This model postulates that neuropathological and atrophic changes which may manifest as cognitive deficits in some individuals may not cause symptoms in individuals with higher cognitive reserve [61–64]. This was potently demonstrated in the Nun Study, in which almost one-third of cognitively normal nuns at autopsy were found to have high levels of neuropathology consistent with Alzheimer’s disease [65, 66]. Social activities, particularly complex ones such as lifelong commitment to communal religious life in the Nun Study, may stimulate cognition and hence expand cognitive reserve. In another example, in the Rush Memory and Aging Study, in those with more extensive social networks, more extensive neuropathology was associated with less deleterious changes in working and semantic memory compared to those with limited social networks [66, 67]. These studies thus demonstrate potential links between socialization and cognitive reserve which warrant further neuropathological investigation.
Association directionality: The health selection model
The health selection model, an alternative explanation for the observed associations between poor social engagement and dementia risk, suggests that the cognitive decline in prodromal dementia causes individuals to re-structure and begin to restrict their social environment, re-evaluating the importance of peripheral social relationships [68]. Memory has been described as a “social glue”, in that memory impairments may necessarily lead to social dysfunction [69]. As a result, the early stages of dementia may cause social disengagement, rather than the reverse. Thus, even in prospective cohort studies, the finding that poor social engagement apparently precedes dementia may, in fact, be due to reverse causation, as prodromal dementia is insidious and difficult to define.
Most studies included in this review have assumed unidirectional causality, that is, that social engagement is associated with subsequent dementia risk. The only study in our review which directly addressed reverse causation found that with the implementation of a three-year lag-time, the association between social engagement and risk of dementia was nullified to statistical non-significance [53]. We attempted to overcome the methodological weakness of the studies eliminating potential reverse causation bias by stratifying by follow-up time. As studies with a longer follow-up time should, in principle, have had a greater chance of measuring social engagement at a timepoint before any effects of the dementia prodrome took hold. However, we found no significant difference in the results between studies stratified in this manner. If reverse causation drove our findings, one would expect the association to be significantly attenuated in studies with a long follow-up time. We have thus provided evidence suggesting, but not proving, that the association is unlikely to be entirely the product of reverse causation.
Consideration of directionality as a mutually exclusive dichotomy may be fallacious. Diverse social networks and social activity may improve health outcomes, including cognitive outcomes, while simultaneously health decline may cause withdrawal from health networks. In this way, a vicious cycle may develop between social isolation and poor health outcomes [70]. Thus, while understanding of the directionality of the association remains unclear, (and noting that no definitive statements about causation can be made), the potential exists that interventions to improve poor social engagement may reduce incident dementia. This potential warrants experimental trials to test this hypothesis empirically.
Limitations
The publication bias and heterogeneity present are major limitations in some analyses to drawing more generalized conclusions. Publication bias was particularly noted in the association between good social engagement and dementia risk. Many included studies reported analyses based on only one or two questions from a much longer questionnaire, suggesting that social engagement was not a focus of the longitudinal study defined a priori. It appears likely, for at least some studies, that social engagement as a risk or protective factor for dementia risk was only reported when such an association was significant, and thus selective publication bias favoring positive studies may have occurred. Heterogeneity is a separate problem that plagues many meta-analyses, and limits confidence in the robustness of conclusions. Beyond clear methodological differences in assessment of social engagement, we found that geographical location, study design, adjustment for depression, and follow-up time may all have contributed to heterogeneity in some analyses. A major strength of our quantitative synthesis and review methodology is that we declined to draw firm conclusions about results with significant publication bias or heterogeneity.
A further limitation of this meta-analysis was our inability to control for confounders, other than depression, due to lack of reporting in the studies reviewed. Exploring the effects of adjustment for physical activity, cognitive activity, physical health, hypertension, diabetes mellitus, alcohol use, smoking, and personality would have been of great interest, but unfortunately was not possible as such factors were generally not reported.
Future directions
Potential preventive interventions may be most beneficial if they combat social isolation and provide support to older individuals lacking social engagement, rather than further bolstering the socialization of those who already have average or better social support and integration. Importantly, depression added to the risk of poor social engagement, with this combination of characteristics identifying individuals at the highest risk of incident dementia. Thus, screening for, and targeting of, this particularly vulnerable group with interventions aimed at both risk factors may be particularly effective. Furthermore, the potential for reverse causation bias should be investigated. This requires a two-pronged approach: identification of a neurobiological causative mechanism, and effectively designed observational studies with long follow-up times and lag times implemented between social engagement assessment and dementia diagnosis. Randomized, controlled trials (RCTs) testing social interventions may assist, if of adequate duration to modify socialization. The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), a two-year multidomain RCT which included dietary, exercise, and cognitive training components, found significant, but modest, improvement in cognitive scores [9]. While these interventions involved group activity and improved social activity, it is not possible to conclude what were the effects on cognition of the socialization component alone. Future studies could study similar lifestyle interventions delivered with and without such group activities, to attempt to isolate the contribution of the socialization itself. Such robustly designed studies with cognitive function outcomes would substantively advance this field.
Public implications
It is likely that social disengagement increases dementia risk. This emphasizes the importance of promoting an interconnected, social lifestyle. However, several factors remain unclear. Firstly, social engagement may occur organically, for example in the context of socializing with friends, or inorganically, by placing individuals in contrived social situations. It is inevitable that social interventions applied through randomized, controlled trials would be of the inorganic variety. Whether or not this is as effective as spontaneous, organic social engagement is uncertain. Secondly, how social engagement at different points of the lifespan influences dementia risk has not been well elucidated. Social engagement initiatives for seniors may occur too late in the lifespan, rendering them ineffective in altering cognitive trajectories. Finally, it is unclear as to whether some forms of social engagement are superior to others in terms of their cognitive effect. For example, video calls may be less cognitively stimulating than face-to-face conversations. Socializing within a group may have different effects on cognition when compared to socializing person-to-person. Despite these issues, the evidence of this meta-analysis supports the general concept of social engagement as a health-promoting activity which should be encouraged in our society.
Conclusions
In this systematic review and meta-analysis, we found evidence that poor social engagement was associated with an increased risk of dementia. Good social engagement could not be conclusively associated with reduced dementia risk, and there was a non-significant trend for loneliness conferring an increased risk. Well-designed experimental studies, including investigation of potential neurobiological, behavioral and social mechanisms are required to test the hypotheses generated by these observational cohort studies.
CONFLICT OF INTEREST
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/18-0439r1).