
Abstract
Background:
Alzheimer’s disease (AD) is a neurodegenerative disease that imposes economic and societal burden. Biomarkers have played a crucial role in the recent approval of aducanumab and lecanemab as disease-modifying therapies which marked a significant milestone for the treatment of AD. The inclusion of biomarkers in AD trials facilitates precise diagnosis, monitors safety, demonstrates target engagement, and supports disease modification.
Objective:
This study analyzed the utilization state and trends of biomarkers as endpoints in AD trials.
Methods:
In this retrospective study, trials were collected by searching clinicaltrials.gov using the term “Alzheimer”. Primary and secondary outcomes were analyzed separately for each phase.
Results:
Among the 1,048 analyzed trials, 313 (29.87%) adopted biomarkers as primary endpoints and 364 (34.73%) as secondary endpoints, mainly in phases 1 and 2. The top three biomarkers adopted as primary endpoints in phases 1, 2, and 3 were amyloid-PET, tau-PET, and MRI. The top three biomarkers adopted as secondary endpoints, in phase 1, were cerebrospinal fluid (CSF) amyloid-β (Aβ), blood Aβ and amyloid-PET; in phase 2, they were MRI, CSF Aβ, and CSF phospho-tau; and in phase 3, they were amyloid PET, MRI, and blood Aβ. There was a statistically significant increase in the adoption of biomarkers as primary endpoints in phase 2 trials (p = 0.001) and secondary endpoints in phase 3 trials (p = 0.001).
Conclusions:
The growing recognition of the importance of biomarkers in AD trial’ design and drug development is evident by the significant steady increase in biomarkers’ utilization in phases 2 and 3.
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative cognition that is characterized by a progressive decline in cognitive and functional abilities, along with the manifestation of neuropsychiatric symptoms [1, 2]. Its distinctive hallmarks include the accumulation of amyloid-β (Aβ) plaques and the presence of hyperphosphorylated tau protein, which forms neurofibrillary tangles [2, 3].
Despite the increasing prevalence of AD and its socioeconomic impact, effective treatments to cure or reverse the disease’s underlying causes remain elusive [4–6]. However, recent developments, including the approval of disease-modifying therapies (DMTs) such as aducanumab and lecanemab, have brought new hope to the field [3, 6–8]. The approval of these DMTs represents a significant milestone and was made possible through the incorporation of biomarkers such as alterations in cerebrospinal fluid (CSF) Aβ and tau levels, as well as amyloid and tau positron emission tomography (PET) scans. These biomarkers played a crucial role in evaluating the effects of DMTs such as aducanumab in clinical trials [9–15].
Biomarkers play a significant role in the planning and implementation of AD trials. They enable an accurate diagnosis, monitor safety and adverse events, and demonstrate target engagement. Moreover, biomarkers provide evidence for disease modification, and guide drug development efforts [16–18].
As researchers continue their pursuit of effective therapies and diagnostic tools, the AT(N) classification system, including biomarkers of amyloid deposition (A), pathologic tau (T), and neurodegeneration (N), provides a unified scheme and defines AD progression based on biomarker profiles [19, 20]. Moreover, with the advancement of highly sensitive assays, the Aβ42/Aβ40 ratio, as well as the levels of phosphorylated tau (p-tau) at threonine 181 and 217 and neurofilament light chain (NfL) concentrations in the blood were identified as indicators of Aβ pathology, tauopathy, and neurodegeneration in the brain [19, 21]. Numerous studies have established correlations between plasma biomarkers with cognitive staging, imaging techniques, including amyloid and tau-PET, and CSF biomarkers [22]. The development of the AT(N) blood biomarkers, which potentially surpass the limitations of existing biomarkers, addresses the requirement for widespread use in diagnostic, prognostic, and therapeutic trial applications [23]. The biomarker framework is evolving to include an ATX(N) system, where X represents other pathophysiological biomarkers, such as vascular, inflammatory, or synaptic biomarkers [20]. Although primary studies on these biomarkers have been conducted in the CSF, recent data from plasma studies indicate their potential as diagnostic blood-based biomarkers, offering insights into cognitive performance and disease progression [24].
A previous study analyzed biomarker utilization within the AT(N) framework in ongoing AD trials [25]. However, this approach has encountered challenges in accurately observing trends in biomarker utilization and adoption across trials. Consequently, there remains a gap in the literature regarding a comprehensive analysis of biomarkers in AD trials. Our study addresses this gap by including trials irrespective of recruitment status and analyzing all biomarkers associated with AD adopted as primary or secondary endpoints, categorized by trial phase, without restricting the alignment with the AT(N) framework.
This study aimed to provide insights into the utilization state and trends of biomarkers as endpoints in AD trials. Understanding which biomarkers are commonly used and how they are employed can help researchers refine trial methodologies, and lead to more efficient and effective clinical studies. Moreover, from a public health standpoint, these insights can inform evidence-based decision-making concerning drug reimbursement.
MATERIALS AND METHODS
Search strategy
Clinicaltrials.gov (https://clinicaltrials.gov/), managed by the National Institutes of Health, was searched on February 2023 using the term “Alzheimer” [condition or disease] with no restriction on trial phases, status of recruitment, age, sex, date, or location.
Eligibility criteria
The analysis included studies from February 2003 to February 2023. Two authors independently screened the trials and confirmed their compliance with the following criteria: (1) the trial assessed AD, mild cognitive impairment of AD, or AD dementia; (2) the trial start date was between February 2003 and February 2023; and (3) the trial had at least one clinical outcome assessment and/or one biomarker as endpoints.
Trials that adopted clinical outcome assessments as outcome measures, but did not incorporate biomarkers, were not excluded. This allowed for a direct comparison of biomarker adoption with clinical outcome assessment, providing insights into the relative utilization of these outcome measures within the trials.
Outcome definition
In this study, we classified the outcomes into two main categories: clinical outcome assessments and biomarkers. Clinical outcome assessments encompassed evaluations of cognitive abilities (e.g., Mini-Mental State Examination - MMSE), functional capacity, and dependency (e.g., Lawton Instrumental Activities of Daily Living –Lawton IADL), behavioral and neuropsychiatric symptoms (e.g., Neuropsychiatric Inventory –NPI), patient quality of life (e.g., Quality of Life in Alzheimer’s Disease –QoL-AD), and global assessments (e.g., Clinical Dementia Rating –CDR) [26].
Biomarkers were classified based on their association with AD pathology. Biomarkers associated with AD pathology include those measuring β-amyloidosis (such as CSF/blood Aβ42, Aβ42/40 ratio, and amyloid-PET) or tauopathy (such as CSF/blood p-tau levels or tau-PET). Other CSF biomarkers assess different AD pathologies, including chitinase 3-like 1 (also known as YKL-40), the soluble form of triggering receptor expressed on myeloid cells-2 (TREM 2), biomarkers of synaptic dysfunction and loss such as neurogranin, glial fibrillary acidic protein (GFAP), and activated microglia expressing translocator protein (TSPO). Biomarkers that are not specific to Alzheimer’s pathology include those related to neurodegeneration or brain injury, such as magnetic resonance imaging (MRI), CSF/blood t-tau, CSF/blood NfL and Fluorodeoxyglucose PET (FDG-PET). In addition, markers of neuroinflammation, such as biomarkers of pro- and anti-inflammatory cytokines and chemokines, are found in the CSF and blood [2, 27]. Additional details on the clinical outcomes and biomarkers identified in AD trials are provided in (Supplementary Table 1).
Data screening and extraction
Two authors independently retrieved the following data from the selected trials: study title, study status, conditions, interventions, phase, outcome measure (s), national clinical trial number, study start date, first posted date, sample size, study design, sponsor/ collaborators, and study location. Disagreements during the selection or extraction processes were resolved through consensus or by involving a third author.
Data analysis
The primary and secondary outcomes of each trial were separately analyzed. The included studies were categorized according to their respective clinical trial phase. Phase 1/2 trials were considered phase 1, and phase 2/3 trials were considered phase 2 [25]. For trials that did not specify a specific start date, the first posted date was considered the start date.
Statistical analysis
Time series analysis and regression analysis were conducted using the annual proportion of biomarker utilization (dependent variable). This analysis was conducted through SPSS 28.0 (IBM Corp., licensed to Chung-Ang University). Autocorrelation analysis of time series analysis was performed first to determine whether there was any autocorrelation (ACF) or partial autocorrelation (PACF). After confirming the absence of autocorrelation and partial autocorrelation, a simple regression analysis was conducted with the year as the independent variable and assuming that the distribution of the error term was normal. As a result of the simple regression analysis, if the year had a significant effect on biomarker utilization proportion, the data trend was confirmed through a graph representation, including a 95% confidence interval. The significance level was evaluated at a p value of 0.005.
Informed consent
This study did not involve human or animal subjects and, therefore, informed consent was not applicable.
RESULTS
Search results
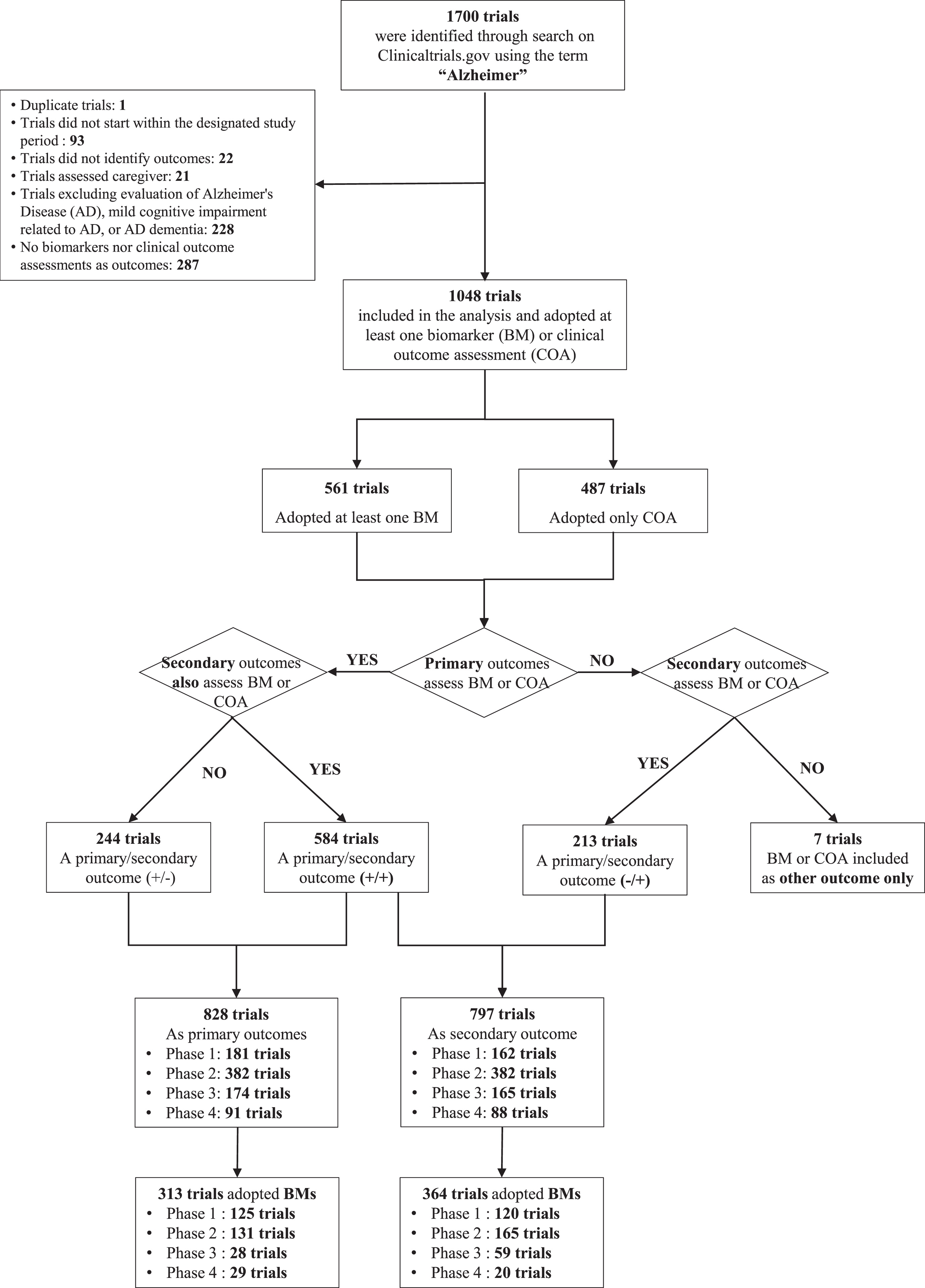
Of the 1,700 trials obtained through the initial clinicaltrials.gov search, 652 were excluded for not meeting the specified eligibility criteria and 1048 trials of phases 1, 2, 3, and 4 were eligible for this study (Fig. 1).
Characteristics of clinical trials included
In total, 239,987 participants were enrolled in the 1,048 trials analyzed, with estimated sample sizes varying from 1 to 8,000 (median, 88) subjects. Most of these trials were conducted in North America (502/1048, 47.90%) and received funding from the biopharma industry (540/1048, 51.53%). The key characteristics of the included trials are summarized in Table 1.
Characteristics of the included clinical trials
In the multi-regional category, clinical trials were conducted in at least two regions. *Trials were conducted in both the northern and southern regions of America. Specifically, only 10 trials were conducted in South America.
Of the 1,048 trials, 561 trials incorporated AD biomarkers, with 165 trials adopting biomarkers as primary endpoints, 211 trials as secondary endpoints, 133 trials as both primary and secondary endpoints, and 52 trials as other endpoints (Supplementary Figures 1 and 2).
Use of biomarkers as endpoints
Overall, 313 trials adopted biomarkers as primary endpoints and 364 trials as secondary endpoints (Fig. 1).
Biomarkers were more commonly utilized as endpoints in phases 1 and 2, whereas phases 3 and 4 mostly relied on clinical outcome assessments as their outcome measures (Fig. 2 for primary outcomes and Supplementary Figure 2 for secondary outcomes).
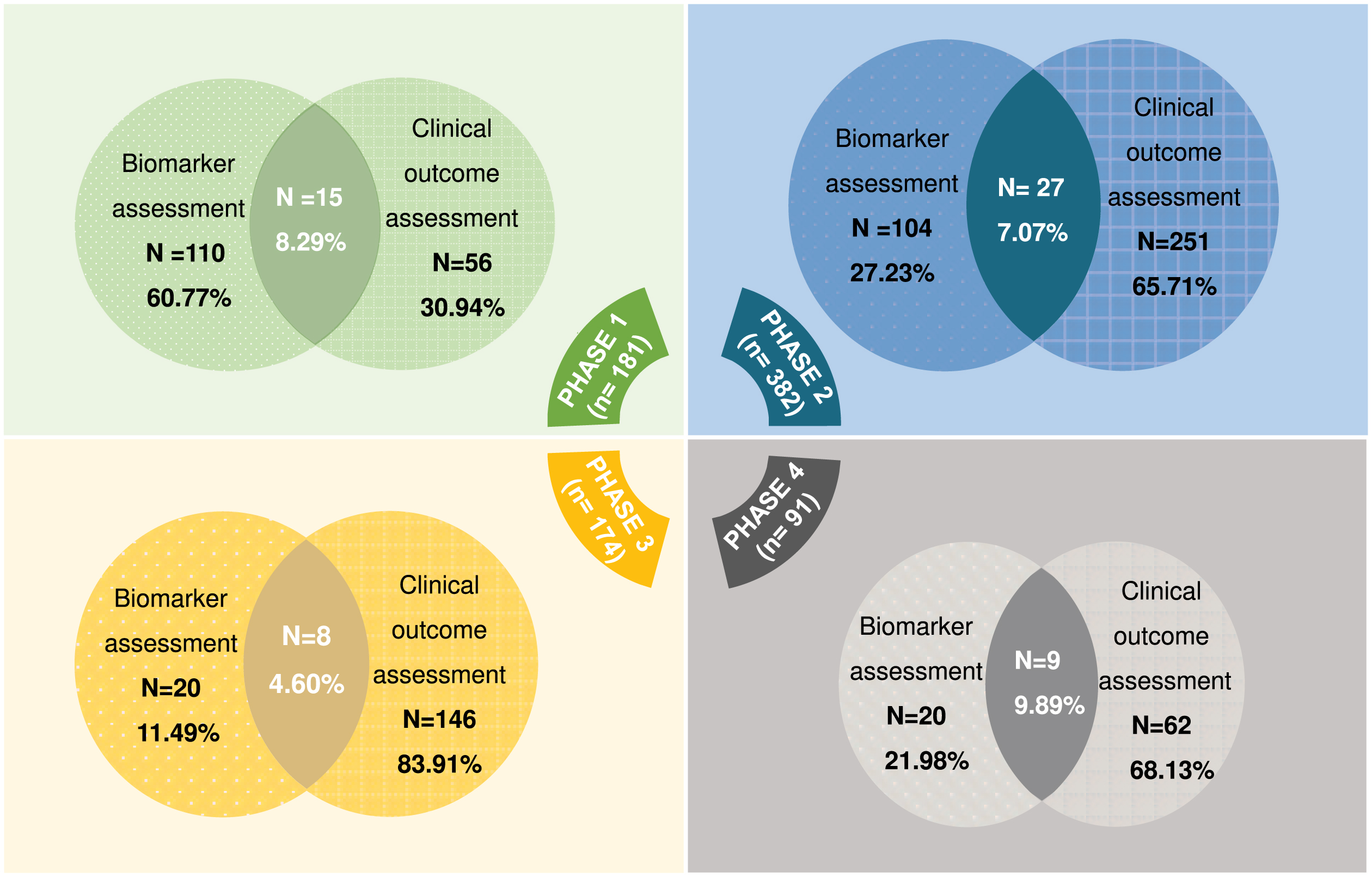
The number and percentage of trials using biomarkers and/or clinical outcome assessments as primary outcomes within each phase.
Statistical analysis further indicated a significant annual steady increase in the utilization of biomarkers as a primary endpoint in phase 2 (p = 0.001) (Fig. 3A) and as a secondary endpoint in phase 3 (p = 0.001) (Supplementary Figure 3A).
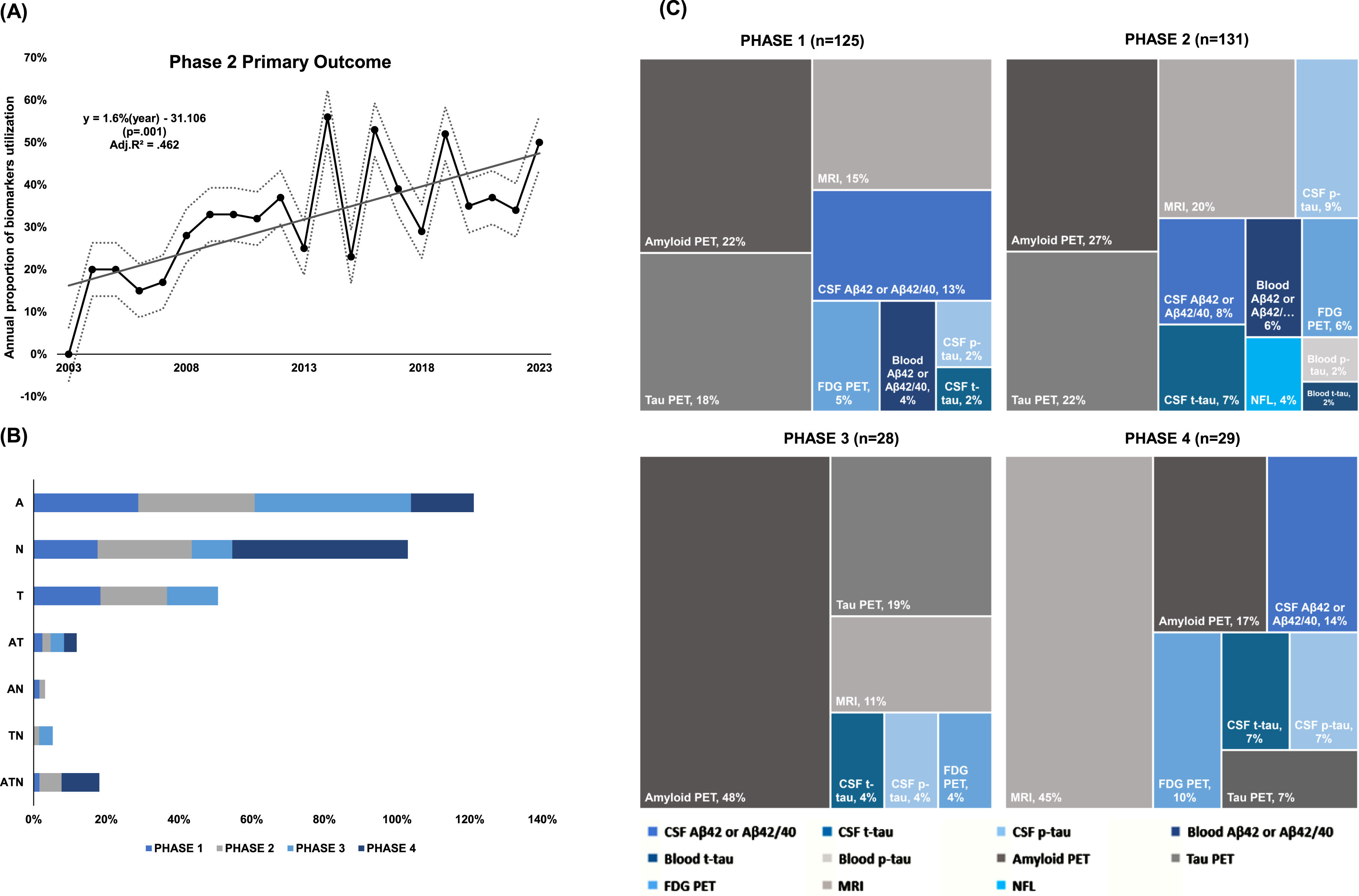
The utilization of AT(N) biomarkers as primary endpoints varied across different phases. For (A) biomarkers, phase 3 trials showed the highest adoption proportion at (12/28, 43%), followed by phase 2 at (42/131, 32%). Meanwhile, (N) biomarkers were most utilized in phase 4 trials at (14/29, 48%), followed by phase 2 at (34/131, 26%). (T) biomarkers, however, showed lower adoption proportions across all phases, with phase 2 trials showing the highest adoption at (24/131, 18%), followed by phase 1 (23/125, 17.6%) (Fig. 3B).
For secondary endpoints, (A) biomarkers were mostly utilized in phase 1 trials at (41/120, 34%), followed by phase 3 at (12/59, 20%). Meanwhile, (N) biomarkers were most adopted in phase 4 trials at (7/20, 35%), followed by phase 2 at (34/165, 21%). (T) biomarkers remained the least adopted across all phases, with phase 3 trials showing the highest adoption at (4/59, 7%), followed by phase 2 at (5/165, 3%) (Supplementary Figure 3B).
The utilization of the AT(N) biomarker combination simultaneously was more prevalent as secondary endpoints, with phase 2 trials demonstrating the highest adoption proportion at 30% (50/165), compared to primary endpoints. (Fig. 3B for primary endpoints, Supplementary Figure 3B for secondary endpoints). In phases 1, 2, and 3, the most adopted biomarkers as endpoints were amyloid-PET, tau-PET, and MRI (Fig. 3 C). However, the top three biomarkers adopted as secondary endpoints varied across the phases. In phase 1, they were CSF Aβ, blood Aβ, and amyloid-PET; in phase 2, they were MRI, CSF Aβ, and CSF p-tau; and in phase 3, amyloid PET, MRI, and blood Aβ were most adopted (Supplementary Figure 3 C).
In the included trials, 70 of 561 trials adopted biomarkers that provided additional insights into various aspects of AD pathophysiology. Among these biomarkers are inflammatory biomarkers such as elevated CSF levels of chitinase-3-like protein 1, TREM 2, and pro- and anti-inflammatory cytokines and chemokines. Other biomarkers were markers of synaptic dysfunction and/or loss such as neurogranin, GFAP, activated microglia expressing TSPO, and exosomal mRNA (Supplementary Table 3).
A schematic that summarizes the historical milestones of biomarkers’ development and the initial incorporation of biomarkers as primary and secondary endpoints in the analyzed trials is provided in Supplementary Figure 4.
DISCUSSION
This retrospective study provided the first comprehensive overview of the state of biomarkers utilization as an endpoint in AD trials, regardless of the trial’s recruitment status, highlighting the increasing acknowledgment of the significance of biomarkers in the process of drug development. Statistical analysis further pinpointed a significant increase in biomarker adoption, both as primary endpoints in phase 2 trials (p = 0.001) and secondary endpoints in phase 3 trials (p = 0.001).
The adoption of tauopathy biomarkers was relatively less frequent compared to biomarkers of amyloid deposition and neurodegeneration across the phases. Changes of amyloid-PET, MRI, and tau-PET were the most frequently adopted biomarkers as primary endpoints across all phases in contrast to other study findings where changes of MRI and FDG-PET were more commonly adopted [25]. Among trials adopting biomarkers as secondary endpoints, the most frequently adopted biomarkers were MRI, CSF Aβ42 or Aβ42/40, and amyloid-PET, which aligned with the other study findings [25].
In our analysis, biomarkers were mainly utilized as endpoints in early-phase trials compared with late-phase trials, where clinical outcome assessments were mostly adopted. Biomarkers such as amyloid or tau proteins play a crucial role in confirming drug-target engagement in early-phase trials, a vital step before progressing to phase 3 [18, 29]. In phase 2 trials, the observation of effects such as reduced CSF tau levels within 3 to 6 months can provide indications of a biological signal, aiding in the selection of doses for phase 3 trials. However, in late-phase trials that focus more on demonstrating clinically meaningful improvements in patient outcomes, such as cognitive function or activities of daily living, clinical outcome assessments are more likely to be the outcome measures, with biomarkers playing a supportive role in providing evidence for efficacy and supporting claims of disease modification [18]. Our findings also indicated that biomarkers of amyloid and tau were mainly used in combination during early-phase trials rather than in later phases.
According to our findings, the (A) biomarkers of the AT(N) framework were widely utilized as both primary (phase 1, 29%; phase 2, 32%; phase 3, 43%; phase 4, 17%) and secondary (phase 1, 34%; phase 2, 16%; phase 3, 20%; phase 4, 10%) endpoints. This may be attributed to amyloid-PET as an endpoint aid for assessing the effectiveness of drugs aiming to reduce amyloid plaque, particularly anti-amyloid monoclonal antibodies [30]. The FDA’s approval of aducanumab in 2021 was largely based on its ability to lower amyloid-PET signal in trials. This approval highlights the significance of amyloid-PET as a surrogate marker for predicting potential clinical benefits. Furthermore, the use of amyloid-PET in the donanemab, an anti-amyloid monoclonal antibody, phase 2 study allowed for treatment dosage adjustment based on imaging results [30–32]. This approach suggests a potential future clinical method for optimizing treatment duration with anti-amyloid monoclonal antibodies, highlighting the importance of amyloid-PET in guiding AD research and clinical decisions [30]. Moreover, in aducanumab trials, other (A) biomarkers such as CSF Aβ42 levels were also employed to assess amyloid pathology [9, 33]. Based on our findings, CSF Aβ42 or Aβ42/40 were commonly utilized as secondary endpoints compared to their adoption as primary endpoints across different phases. Although CSF and PET-based biomarkers offer valuable insights into AD pathology, their invasiveness and high cost limit their widespread adoption in clinical settings [34]. To overcome these limitations, there is a focus on blood-based biomarkers that can offer a less invasive, time-efficient, and potentially more accessible alternative [35]. Although blood-based biomarkers have recently been introduced into clinical trials for AD, our analysis revealed that blood Aβ42 or Aβ42/40 were commonly utilized as secondary endpoints (phase 1, 27%; phase 2, 20%; phase 3, 22%) along with amyloid-PET and CSF Aβ42 or Aβ42/40. Blood-based biomarkers show robust associations with measurements derived from PET or CSF analysis, and effectively estimate cognitive decline and pathological changes of the disease [34]. However, to draw a more generalized conclusion about blood-based biomarkers’ application to the clinical reference, these biomarkers need to undergo examination and validation in extensive, prospective, and longitudinal multicenter cohorts comprising diverse populations, while adhering to a standardized protocol, sample material, and predefined cut-off points [36].
Regarding the biomarkers of neurodegeneration, particularly MRI, were also frequently adopted as primary endpoints and secondary endpoints. Endpoints indicating neurodegeneration offer evidence that a drug alleviates the progression of neurodegeneration [20]. The attenuation of neurodegeneration, which is considered a later stage of the disease, can be illustrated by the changes on volumetric MRI (brain atrophy), CSF t-tau (neuronal injury), and rate of glucose metabolism in the brain as illustrated on FDG-PET [7, 38]. Although not specific to AD, NfL seems promising for the detection of neurodegeneration [20]. Therefore, N biomarkers provide evidence for disease modification when a difference between drug and placebo effects is observed [29]. Furthermore, in the analyzed trials, MRI served also as a safety and monitoring biomarker. Specifically, MRI plays a crucial role in identifying amyloid-related imaging abnormalities in patients receiving anti-amyloid monoclonal antibodies [9].
According to our analysis, (T) biomarkers had relatively less adoption than (N) and (A) biomarkers, especially as secondary endpoints (phase 1, 2%; phase 2, 3%; phase 3, 7%). This relatively low adoption of (T) biomarkers may be influenced by the research focus of different trials. Some trials may prioritize (N) and (A) biomarkers because they align more closely with specific study objectives. Additionally, owing to the limited selectivity and effectiveness of tau tracers, the ability to visualize, map, and quantify tauopathy is restricted [33]. Nevertheless, it is worth mentioning that tau-PET imaging has shown promise in providing valuable insights into disease progression by visualizing tau tangles and predicting cognitive changes, even surpassing the capabilities of MRI and amyloid-PET [39].
This analysis further highlights the exploration of diverse biomarkers beyond Aβ and tau in early-phase trials, including markers linked to synaptic dysfunction (e.g., neurogranin), inflammation (e.g., Chitinase-3-like protein 1, TREM2), and CNS injury (e.g., GFAP and TSPO). These biomarkers, in addition to elevated inflammatory markers and reduced microRNA-125b levels, offer insights into various aspects of AD pathology and are increasingly being recognized for their potential diagnostic and therapeutic relevance [33].
It is important to acknowledge the limitations of this study. We only searched the clinicaltrials.gov database, and although it is comprehensive [40], it may not cover all available literature, potentially leading to gaps in coverage. Additionally, some trials lacked clear information, affecting the unbiased analysis, as the specific biomarkers adopted were not always specified. Furthermore, analyzing biomarker utilization over 20 years posed challenges owing to the dynamic nature of biomarker availability and technological advancements, potentially introducing variability in the types of biomarkers utilized across different periods. Despite these limitations, we provided contextual information on the historical timeline of biomarker development and adoption, and a sub-analysis focusing on the last decade as supplementary material to enhance understanding.
In summary, our findings shed light on the current methodological and clinical approaches employed in AD clinical trials’ outcomes and highlight the increasing recognition of the significance of biomarkers in AD clinical trials, as evidenced by the significant steady increase of biomarker adoption in phases 2 as primary endpoints and phase 3 as secondary endpoints. AD biomarkers play an important role in clinical decision-making, which is especially important with the advancement of anti-Aβ DMTs. By identifying commonly used biomarkers and examining their utilization patterns, our findings contribute to refining trial methodologies, potentially leading to more efficient and effective clinical trials in the future. Future longitudinal studies could compare trends over time and analyze how technological advancements affect biomarker utilization.
AUTHOR CONTRIBUTIONS
Yomna Magdy Elghanam (Conceptualization; Data curation; Formal analysis; Methodology; Visualization; Writing – original draft; Writing – review & editing); EunYoung Kim (Conceptualization; Formal analysis; Funding acquisition; Methodology; Project administration; Supervision; Writing – review & editing); Sujata Purja (Data curation; Visualization; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors express their appreciation to our contributing researchers: Sua Oh, for assistance in structuring the graphical concept, and Manca Slatnar, for extracting information to organize the study characteristics table.
FUNDING
This research received financial support from the South Korean government, specifically from the Ministry of Science and ICT (MICT) under the grant NRF-2021R1F1A1062044, and from the Basic Science Research Program through the National Research Foundation of Korea, funded by the Ministry of Education (Grant Number 2021R1A6A1A03044296). It is important to note that the funding entities played no part in the design of the trial, data collection, interpretation of data, or preparation of the report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available in the supplementary materials.