
Abstract
Background:
Within older Veterans, multiple factors may contribute to cognitive difficulties. Beyond Alzheimer’s disease (AD), psychiatric (e.g., PTSD) and health comorbidities (e.g., TBI) may also impact cognition.
Objective:
This study aimed to derive subgroups based on objective cognition, subjective cognitive decline (SCD), and amyloid burden, and then compare subgroups on clinical characteristics, biomarkers, and longitudinal change in functioning and global cognition.
Methods:
Cluster analysis of neuropsychological measures, SCD, and amyloid PET was conducted on 228 predominately male Vietnam-Era Veterans from the Department of Defense-Alzheimer’s Disease Neuroimaging Initiative. Cluster-derived subgroups were compared on baseline characteristics as well as 1-year changes in everyday functioning and global cognition.
Results:
The cluster analysis identified 3 groups. Group 1 (n = 128) had average-to-above average cognition with low amyloid burden. Group 2 (n = 72) had the lowest memory and language, highest SCD, and average amyloid burden; they also had the most severe PTSD, pain, and worst sleep quality. Group 3 (n = 28) had the lowest attention/executive functioning, slightly low memory and language, elevated amyloid and the worst AD biomarkers, and the fastest rate of everyday functioning and cognitive decline.
CONCLUSIONS:
Psychiatric and health factors likely contributed to Group 2’s low memory and language performance. Group 3 was most consistent with biological AD, yet attention/executive function was the lowest score. The complexity of older Veterans’ co-morbid conditions may interact with AD pathology to show attention/executive dysfunction (rather than memory) as a prominent early symptom. These results could have important implications for the implementation of AD-modifying drugs in older Veterans.
INTRODUCTION
In 2020, the Veterans Health Administration (VHA) provided medical care for more than 9 million enrolled Veterans, of whom over 50% were age 65 years or older [1, 2]. Within older Veterans, it is estimated that approximately 10% have dementia [3], and this number is forecasted to increase more than 29% by 2033 [4]. Military-related experiences that lead to toxic exposures and combat-related trauma can put one at greater risk for dementia. More specifically, elevated vascular burden (i.e., a greater number of and/or more severe cardio- and cerebrovascular risk factors and diseases), post-traumatic stress disorder (PTSD), depression, and traumatic brain injury (TBI) have all been linked to military exposures, and are associated with increased risk of Alzheimer’s disease and related dementias (ADRD) [5–9]. Given the unique experiences and potentially elevated risk of dementia in older Veterans, it is critical to study early profiles of cognition and biomarkers to better understand the many factors that may be associated with unique presenting phenotypes as well as to better understand prognosis of these presentations.
Data-driven approaches have been used to better characterize subgroups and understand heterogeneity of both cognitive presentations [10–14] as well as biomarker patterns in ADRD [15–18]. Specifically, studies that have used data-driven clustering approaches to understand neuropsychological subtypes have yielded significant heterogeneity both in breadth and severity of cognitive difficulties, including within cognitively unimpaired (CU) participants [13, 14], as well as unique patterns of relative strengths and weaknesses in different cognitive domains. These unique cognitive phenotypes tend to show differences in variables such as sociodemographic, subjective cognitive decline, Alzheimer’s disease (AD) biomarkers, vascular health factors, as well as longitudinal rates of functional decline and progression to dementia [10, 19–21]. Few studies, however, have combined both objective and subjective cognition as well as biomarkers as part of the clustering analysis.
Considering multiple sources of information in the form of neuropsychological testing, subjective cognitive decline (SCD), and amyloid biomarkers is becoming a more common practice in research and even in some clinical settings. While we have significant research on individuals from academic memory clinic settings, within older Veterans, there may be multiple co-occurring factors such as PTSD, that are likely to contribute to particularly complex presentations. More work is needed to understand the cognitive and pathological presentations in older Veterans, particularly given the need for accurate detection of AD- versus non-AD pathologic presentations now that an anti-amyloid therapy has been approved for use at the VHA. Therefore, the aim of our study was to identify cluster-derived subgroups of Vietnam-Era Veterans without dementia based on neuropsychological test data, SCD, and amyloid positron emission tomography (PET) and to compare their baseline characteristics and rates of 1-year change in everyday functioning and global cognition.
MATERIALS AND METHODS
Data used in the preparation of this article were obtained from the Brain Aging in Vietnam War Veterans/Department of Defense Alzheimer’s Disease Neuroimaging Initiative (DoD-ADNI) database (http://adni.loni.usc.edu). DoD-ADNI is directed by principal investigator Dr. Michael Weiner of the San Francisco VA Medical Center and University of California, San Francisco. The overarching goals of DoD-ADNI are to characterize the long-term neural and behavioral consequences of TBI and/or PTSD. The main aims and methods are described in detail elsewhere [22], and up-to-date information can be found at http://www.adni-info.org. This research was approved by the institutional review boards of all participating sites within ADNI and written informed consent was obtained for all study participants.
Participants
Enrollment criteria for DoD-ADNI have been described elsewhere [22]. Briefly, DoD-ADNI excluded participants with a diagnosis of dementia and Clinical Dementia Rating (CDR) score of >0.5. The current study included 228 Vietnam-Era Veterans without dementia from DoD-ADNI. Participants were included if they had neuropsychological, SCD, and amyloid PET data at the first study visit. While participants have varying durations of follow up (up to ∼5 years) [23], we used the 1-year follow-up visit to reduce the risk of selective attrition since there were still 183 participants (80.3% of baseline sample) with everyday functioning data at year 1.
Measures included in cluster analysis
Neuropsychological measures. The cluster analysis included the following neuropsychological cognitive domains: Immediate Memory, Delayed Memory, Language, and Attention/Executive Functioning. Domain scores were calculated by taking the mean of the unadjusted z-scores of the tests in that domain. The Immediate Recall score included the immediate recall scores from the Rey Auditory Verbal Learning Test and Logical Memory; Delayed Recall included the delayed recall scores from the Rey Auditory Verbal Learning Test and Logical Memory; Language included the 30-item Boston Naming Test and Animal Fluency; Attention/Executive Functioning included Trail Making Test Parts A and B. Trail Making Test scores were log-transformed (due to skewness) and multiplied by –1 prior to being averaged so that higher scores represented better performance across all tests.
Once the unadjusted domains scores were created, each domain score was converted to an age-, education-, race-, and ethnicity-adjusted z-score [24]. Sex/gender was not adjusted for given the very small number of women in the sample (n = 2). Adjusted z-scores were determined based on the difference between the observed score and expected score divided by the standard error of measurement. Regression coefficients to determine the expected score were derived from a subset of the larger DoD-ADNI sample who had a CDR = 0 (i.e., cognitively unimpaired) at baseline (N = 230).
Subjective cognitive decline. The Everyday Cognition (ECog) measure was used to measure subjective cognitive decline. The ECog measure is a 39-item measure in which the participants rate their ability to perform everyday tasks relative to 10 years ago on a scale of 1 (“better or no change”) through 4 (“consistently much worse”) in the domains of memory, language, visuospatial, planning, organization, and divided attention [25]. A score of 9 (“don’t know”) was coded as missing. The ECog score is based on the mean of all non-missing items. Higher scores represent more subjective everyday cognitive and functional difficulties. The ECog was log-transformed and z-scored prior to being entered into the cluster analysis.
Amyloid PET. Florbetapir (AV45) PET was used to measure amyloid burden. Specific details of data acquisition and processing of florbetapir PET data are available at adni.loni.usc.edu. A summary standardized uptake value ratio (SUVR) was calculated by dividing the mean uptake across 4 AD-vulnerable cortical regions (frontal, anterior/posterior cingulate, lateral parietal, and lateral temporal cortices) by whole cerebellar (white and gray matter) uptake [26]. Greater binding of florbetapir is consistent with greater cortical Aβ burden. Aβ PET was log-transformed and z-scored prior to inclusion in the cluster analysis.
Additional measures for phenotype characterization
Demographic and sociocultural variables. Age, years of education, sex/gender, race, ethnicity, and preferred language were all used to characterize the cluster-derived subgroups.
Biomarkers. In addition to amyloid PET that was used in the cluster analyses, additional biomarkers were used to characterize the cluster groups. These included Apolipoprotein E (APOE) ɛ4 carrier status, cerebrospinal fluid (CSF) p-tau181, hippocampal volume, and white matter hyperintensity (WMH) volume (residualized for total brain volume). Further, flortaucipir PET imaging was available on a subset of participants (n = 84) and a metatemporal region of interest that was partial volume corrected and normalized to the inferior cerebellar gray was compared across cluster groups [27].
Vascular and health measures. Proportion of Veterans with self-reported diabetes and hypertension were examined. Additionally, pulse pressure was examined as a proxy for arterial stiffening and was calculated by subtracting diastolic blood pressure from systolic blood pressure [28]. TBI history was based on participant report and severity was based on Veteran Affairs (VA)/DoD criteria 2021 Clinical Practice Guidelines [29]. TBI severity was based on the most severe TBI sustained in their lifetime. A TBI was classified as mild if the participant reported a loss of consciousness (LOC) of less than 30 min, or alteration of consciousness (AOC) or post-traumatic amnesia (PTA) up to 24 h. The moderate and severe TBI criteria were combined since the information for PTA of more than 1 day was not available. A TBI was classified as moderate-to-severe if the participants had a LOC greater than 30 min, AOC greater than 24 h, or PTA greater than 1 day. Other health measures included sleep quality based on the Pittsburgh Sleep Quality Index, and pain frequency as measured on the Short Form-12 (SF-12) health survey.
Psychiatric measures. Current and lifetime PTSD symptom severity was measured using the Clinician-Administered PTSD Scale (CAPS-IV). A participant was classified as having PTSD if Criteria A though F were met based on the DSM-IV algorithm [30]. Depressive symptoms were measured using the 15-item Geriatric Depression Scale. History of alcohol or opioid abuse or dependence based on the Structured Clinical Interview for DSM Disorders (SCID) was also examined.
Longitudinal outcome measures
Clinical Dementia Rating –Sum of Boxes (CDR-SB). The CDR is a semi-structured interview that assesses cognitive and functional abilities. Relative to the CDR global score, the CDR-SB provides a greater range of scores (i.e., 0–18), with higher scores indicating more functional difficulty [31].
Global cognition. The Global Cognition composite was derived from the mean of the Immediate Recall, Delayed Recall, Language, and Attention/Executive Functioning scores described above under Neuropsychological measures.
Statistical analyses
A hierarchical cluster analysis that included the neuropsychological domain scores, SCD, and amyloid PET z-scores at baseline was conducted to derive the cluster groups. Next, a discriminant function analysis was conducted to test the extent to which the individual neuropsychological, SCD, and amyloid PET measures could predict cluster-group membership. Analysis of variance, Kruskal-Wallis, and χ2 tests examined demographic, clinical, and biomarker characteristics by group. Linear mixed effects models were used to determine the 1-year change in everyday functioning and global cognition by group membership. Random intercept was included, but random slope did not improve model fit (likely due to the 2 timepoints), so was not included. Fully-adjusted models that included age, education, PTSD symptom severity, APOE ɛ4 carrier status (carrier versus noncarrier), and TBI history (none, mild, moderate-to-severe) as covariates are reported. Unadjusted models are also reported. All variables were z-scored prior to being included in the models.
RESULTS
Cluster analysis
Across the sample, participants had a mean age of 69.73 years (SD = 4.78), mean education of 15.17 years (SD = 2.44), were 99.1% male, 85.5% white and 7.0% Black/African American, and 7.9% Hispanic/Latino. The cluster analysis identified 3 cluster groups that were derived using neuropsychological domain scores, SCD, and amyloid PET: Group 1 had average-to-above average cognition, below average SCD, and the lowest amyloid (n = 128); Group 2 had low memory and language, the highest level of SCD, and average amyloid (n = 72); Group 3 had the lowest attention/executive functioning, slightly low memory and language, average SCD, and high amyloid (n = 28; see Fig. 1). Means and SDs of the neuropsychological, SCD, and amyloid variables are shown in Table 1. A discriminant function analysis using the neuropsychological, SCD, and amyloid measures to predict group membership into these 3 clusters correctly classified 92.0% of the participants. A 4-cluster solution from the cluster analysis was also considered in which Group 1 was split into an average cognition group (n = 89) and a high cognition group (n = 39), both with below average SCD and average amyloid. Groups 2 and 3 remained consistent in both the 3- and 4-cluster solution. A discriminant function analysis predicting group membership into the 4 clusters correctly classified 90.8% of the participants. For parsimony and to maintain a larger sample size of participants who are generally performing within the average range and above on neuropsychological measures, have average to low-average levels of SCD, and have average to low amyloid burden, the 3-cluster solution was selected for further analyses.

Baseline demographic, clinical, and biomarker characteristics of the cluster-derived groups
Data are summarized as mean (standard deviation) or %. aSignificantly different than Group 3 (i.e., p < 0.05); bSignificantly different than Group 2; cSignificantly different than Group 1. MMSE, Mini-Mental State Exam; CDR, Clinical Dementia Rating; AVLT, Rey Auditory Verbal Learning Test; BNT, Boston Naming Test; ECog, Everyday Cognition; APOE, apolipoprotein E; CSF, cerebrospinal fluid; WMH, white matter hyperintensity volume (log-transformed after residualizing for total brain volume and z-scored); CAPS, Clinician-Administered PTSD Scale; GDS, Geriatric Depression Scale; TBI, Traumatic brain injury.
Phenotype characterization
Table 1 shows the demographic, clinical characteristics, and specific raw neuropsychological test scores by cluster-derived group. Briefly, Group 3 was older and had higher years of education than Groups 1 and 2. There were no differences by race, ethnicity, or preferred language, though there was a general pattern in which there was a greater proportion of white and non-Hispanic participants in Group 3 than in Groups 1 and 2. In general, participants in Group 2 had the most cognitive and functional difficulty and the most SCD, while participants in Group 1 had the best cognition and everyday functioning. Group 3 had mean cognitive scores that were mostly in between Groups 1 and 2, but had the worst scores on Trails A and B (attention/executive functioning). In addition to elevated amyloid PET levels compared to Groups 1 and 2, Group 3 had other markers that are most consistent with AD including the highest rate of APOE ɛ4 carriers (50%), lowest hippocampal volume, and the highest levels of CSF p-tau and temporal tau on PET. Group 2 had the highest rates of current PTSD diagnosis and current and lifetime PTSD symptom severity as well as worst sleep quality and greatest pain frequency. There were no differences by group in vascular diseases (diabetes, hypertension) or vascular markers (pulse pressure, WMH volume), depressive symptoms, or history of alcohol or opioid abuse/ dependence. TBI history did not statistically differ by group, but Group 3 had a pattern for greater proportion of participants with a history of TBI, particularly a moderate-to-severe TBI.
Longitudinal analyses
One-year change in everyday functioning and global cognition by cluster group are shown in Fig. 2, and both unadjusted and adjusted model estimates are shown in Table 2. After adjusting for age, education, PTSD symptoms, TBI history, and APOE ɛ4 carrier status, there was a main effect of group such that relative to Group 1, Group 2 had significantly greater everyday functioning difficulties on average (p = 0.004). While the pattern was similar for Group 3, it did not statistically differ from Group 1 (p = 0.066). Groups 2 and 3’s mean level of functional difficulties did not differ across time (p = 0.857). Longitudinally, when the group × time interaction was added to the model, results showed that relative to Group 1, Group 2 showed a faster, but non-significant, increase in functional difficulties (β = 0.212, 95% CI: –0.051 to 0.475, p = 0.114) and Group 3 showed a significantly faster increase in functional difficulties over 1 year (β = 0.552, 95% CI: 0.171 to 0.933, p = 0.005). Group 3 also had a faster increase in functional difficulties relative to Group 2, but this effect did not reach statistical significance (β = 0.340, 95% CI: –0.071 to 0.751, p = 0.104). The pattern of results was the same in the unadjusted model.
Parameter estimates for 1-year change in CDR-SB and Global Cognition by cluster group
CDR-SB, Clinical Dementia Rating-Sum of Boxes; APOE, apolipoprotein E; CAPS, Clinician-Administered PTSD Scale; TBI, Traumatic brain injury.
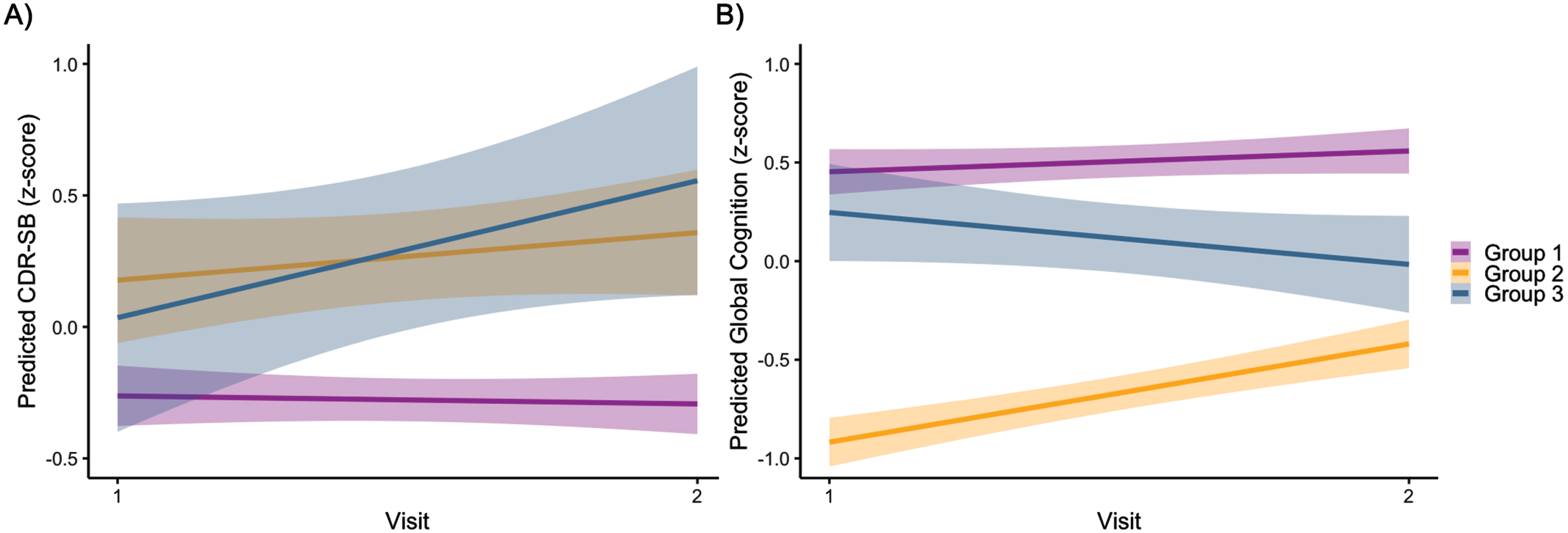
For global cognition, after adjusting for age, education, PTSD symptoms, TBI history, and APOE ɛ4 carrier status, there was a main effect of group such that Group 1 had significantly better global cognition than Groups 2 and 3 across visits, and Group 3 had better global cognition than Group 2 (ps < 0.010). Longitudinally, when the group × time interaction was added to the model, results showed that relative to Group 1, Group 2 showed a significantly faster improvement in global cognition over 1 year (β = 0.393, 95% CI: 0.136 to 0.649, p = 0.003) while Group 3 showed a pattern of greater decline in global cognition over 1 year (β = –0.368, 95% CI: –0.741 to 0.004, p = 0.053). Group 3 had significantly greater rate of decline in global cognition relative to Group 2 (β = –0.761, 95% CI: –1.161 to –0.361, p < 0.001), as Group 2 seemed to regress toward the mean by visit 2. The pattern of results was the same in the unadjusted model.
DISCUSSION
The current study used a data-driven approach that included not only neuropsychological measures, but also a measure of SCD and amyloid PET to determine if there are meaningful phenotypes that emerge in a sample of Vietnam-Era Veterans. Three cluster groups were found. The largest group (Group 1) performed within the average range or above on all cognitive measures, had low levels of SCD, and the lowest levels of amyloid burden. The second largest group (Group 2), however, had the worst cognitive profile with the lowest scores on memory and language measures plus the highest rate of SCD despite average amyloid levels. Group 2 also had the highest rates of PTSD, pain, and poorest sleep quality. Finally, the smallest group (Group 3) had elevated amyloid and performed the lowest on attention/executive functioning but had average SCD. Group 3 was also slightly older, had more years of education, had biomarkers that were most consistent with biological AD, and had the largest proportion of participants with a TBI history.
Longitudinally, Group 3, the group most consistent with biological AD, had the fastest rate of increase in functional difficulties over 1-year, followed by Group 2 and Group 1, despite Group 2 having the worst everyday functioning and memory and language performance at baseline. Given the subjective measurement of the CDR and potential for psychiatric symptoms and physical health to impact the scores, change in global cognition over 1 year was also examined. These results demonstrated a slightly different pattern such that although Group 3 again showed the fastest rate of decline, Group 2 showed improvement in cognitive performance between baseline and the 1-year follow-up visit despite having the lowest cognitive performance on average.
This pattern, consistent with regression to the mean for Group 2, was somewhat unexpected given the initial profile of the lowest memory and language performances in addition to the highest report of SCD. However, this group also had the highest PTSD symptom severity, poorest sleep quality, and highest pain frequency. There is consistent evidence that all of these factors can impact cognition in older Veterans [32–34]. However, while factors such as PTSD may be associated with dementia risk [35], these are also factors that may fluctuate up and down over time depending on medications, therapy and other treatment/activities, and ongoing life stressors. Therefore, it is possible that the associated cognitive difficulties could also fluctuate, and improve on sensitive neuropsychological measures, over time even if the participant is still reporting some everyday functioning difficulties in their everyday life. While Group 2’s global cognition improved by the 1-year follow up, they were still performing below the other groups on the global cognition composite. These longitudinal results emphasize the importance of contextualizing cognitive difficulties, which is likely best done with a multidisciplinary approach that includes a comprehensive neuropsychological evaluation comprising of a thorough clinical interview and considers all psychiatric, health, and other conditions before making a diagnosis and treatment plan. This may be particularly important in the context of the newly approved anti-amyloid drug Leqembi. Notably, Group 2 had the highest rate of CDR = 0.5, which would be considered mild cognitive impairment (MCI) and therefore likely meet the cognitive criteria for Leqembi despite their cognitive difficulties potentially not being due to AD pathology. In fact, Veterans with this profile may benefit from management of psychiatric, pain, and sleep symptoms first, or in combination with other approaches to improve cognition (e.g., learning compensatory cognitive skills, physical activity, managing vascular risks, etc.) [36–38] and then be re-assessed to determine if they still meet criteria for MCI.
Group 3 had the highest rate of amyloid burden and had other biomarkers that were most consistent with biological AD [39], including elevated CSF p-tau and tau PET levels, smallest hippocampal volumes, and a high proportion of APOE ɛ4 carriers. Rather than showing prominent memory difficulties [40], however, this group performed the lowest on attention/executive functioning and did not show the highest rates of MCI (measured as CDR = 0.5). This cognitive profile provides important insights into what may be a unique presentation of biological AD among older Veterans who likely have higher rates of co-occurring psychiatric symptoms, TBI histories, and vascular risks. Specifically, the complexity of older Veterans’ co-morbid conditions may interact with AD pathology to show attention/executive dysfunction (rather than memory) as a prominent early symptom for this group. This cognitive profile also has implications for treatment since despite showing very high levels of amyloid, many in this group would not meet criteria for MCI based on the CDR, which is weighted heavily for memory difficulties. Thus, a more comprehensive neuropsychological assessment would be required to diagnose MCI based on impairments beyond memory.
Unlike previous studies that have largely focused on profiles of either cognition or biomarkers, the current study examined neuropsychological measures, SCD, and amyloid PET together in the same clustering model. Important next steps with a larger sample would be to consider additional biomarkers of AD, including tau, as well as non-AD specific markers such as vascular biomarkers (e.g., WMH volumes, cerebral blood flow) or vascular metrics such as blood pressure and hemoglobin a1c in the clustering model. A next step to making the implications of the current results more accessible and applicable in a clinical setting would be to examine the associations and profiles of cognition and co-morbid conditions with plasma biomarkers, rather that PET imaging, the latter which is expensive and not available in many settings. Plasma biomarkers have not been well-validated in older Veterans, so this work would be a critical next step given the likelihood of increased AD plasma biomarkers availability in coming years.
In addition to the approach of combining cognition and amyloid in the cluster analysis, strengths of this study include the use of the DoD-ADNI data given the multiple AD biomarkers that are available as well as measures of PTSD and depression, multiple domains of cognition, SCD, and everyday functioning as well as longitudinal data, which was particularly critical in interpreting the prognosis for Group 2. At the same time, the data are limited by the lack of women Veterans who are enrolled as well as limited race/ethnicity diversity. Given women and Black/African American and Hispanic older adults are at greatest risk for dementia, improved representation in future research is critical. Further, there was intentional over-sampling of participants with a history of TBI and PTSD in DoD-ADNI and exclusion of Veterans with high levels of vascular burden given the initial goals of the larger study to understand the associations of TBI and PTSD with AD biomarkers. However, the high rate of TBI may make generalization to the overall Vietnam-Era Veteran population more difficult. Importantly, recent work in this cohort has not found associations between TBI or PTSD with AD biomarkers [23], so despite the pattern of higher rates of TBI across the sample and especially in Group 3, it is unlikely that TBI is the cause of the elevated amyloid levels in this group.
These results add to a growing literature demonstrating heterogeneity in early cognitive and pathological presentations of ADRD [10, 42]. Within older Veterans, most participants were performing in the average-to-above average range. The other two cluster-derived groups showed unique cognitive, SCD, and amyloid profiles and were associated with different demographic, psychiatric, pain/sleep, and AD biomarker correlates as well as unique patterns of change in everyday functioning and global cognition, even in the span of only 1 year. These results have important implications for assessment and precision treatment of older Veterans and highlight the need for comprehensive clinical evaluations that include a thorough neuropsychological assessment with clinical interview and biomarker testing when possible.
AUTHOR CONTRIBUTIONS
Kelsey Thomas (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Visualization; Writing – original draft); Alexandra Clark (Conceptualization; Methodology; Writing – review & editing); Alexandra Weigand (Conceptualization; Methodology; Writing – review & editing); Lauren Edwards (Methodology; Writing – review & editing); Alin Alshaheri Durazo (Data curation; Writing – review & editing); Rachel Membreno (Writing – review & editing); Britney Luu (Writing – review & editing); Peter Rantins (Data curation; Writing – review & editing); Monica Ly (Data curation; Methodology; Writing – review & editing); Lindsay Rotblatt (Writing – review & editing); Katherine Bangen (Methodology; Writing – review & editing); Amy Jak (Conceptualization; Methodology; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was supported by the U.S. Department of Veterans Affairs Clinical Sciences Research and Development Service (1IK2CX001865 to KRT, 1I01CX001842 to KJB), National Institutes of Health/National Institute on Aging grants (P30 AG062429 to KRT, R03 AG070435 to KRT, 1RF1AG082726 to KRT, R01 AG063782 to KJB), and the Alzheimer’s Association (AARG-22-723000 to KRT).
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; BioClinica, Inc.; Biogen Idec Inc.; Bristol-Myers Squibb Company; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; GE Healthcare; Innogenetics, N.V.; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Medpace, Inc.; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Synarc Inc.; and Takeda Pharmaceutical Company. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Disease Cooperative Study at the University of California, San Diego. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California. This research was also supported by NIH grants P30 AG010129 and K01 AG030514.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Disease Cooperative Study at the University of California, San Diego. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California. This research was also supported by NIH grants P30 AG010129 and K01 AG030514.
CONFLICT OF INTEREST
Kelsey Thomas and Katherine Bangen are Editorial Board Members of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer-review. The other authors have no conflict of interest to report.