
Abstract
Background:
Recently, subjective cognitive decline (SCD) was proposed as an early risk factor for future Alzheimer’s disease (AD).
Objective:
In this study, we investigated whether accelerated long-term forgetting (ALF), assessed with extended testing intervals than those adopted in clinical practice, might be a cognitive feature of SCD. Using an explorative MRI analysis of the SCD sample, we attempted to investigate the areas most likely involved in the ALF pattern.
Methods:
We recruited 31 individuals with SCD from our memory clinic and subdivided them based on their rate of memory complaints into mild SCDs (n = 18) and severe SCDs (n = 13). A long-term forgetting procedure, involving the recall of verbal and visuo-spatial material at four testing delays (i.e., immediate, 30 min, 24 h, and 7 days post-encoding) was used to compare the two sub-groups of SCDs with a healthy control group (HC; n = 16).
Results:
No significant between-group difference was found on the standard neuropsychological tests, nor in the immediate and 30 min recall of the experimental procedure. By contrast, on the verbal test severe SCDs forgot significantly more than HCs in the prolonged intervals (i.e., 24 h and 7 days), with the greatest decline between 30 min and 24 h. Finally, in the whole SCD sample, we found significant associations between functional connectivity values within some cortical networks involved in memory (default mode network, salience network, and fronto-parietal network) and verbal long-term measures.
Conclusions:
Our preliminary findings suggest that long-term forgetting procedures could be a sensitive neuropsychological tool for detecting memory concerns in SCDs, contributing to early AD detection.
Keywords
INTRODUCTION
Accelerated long-term forgetting (ALF) is a memory deficit characterized by normal information retention up to relatively short intervals (e.g., minutes, hours) but abnormally larger performance decline over more extended periods (e.g., days, weeks). This condition, which is often underestimated in clinical neuropsychological practice due to a lack of assessment tools able to evaluate memory retention beyond 30–60 min, 1 has been widely documented in patients with temporal lobe epilepsy (TLE) who have subjective memory complaints that are not confirmed by common memory tests.2–6
In the past few years, ALF has been reported in patients with other clinical conditions, such as those with traumatic brain injury 7 , minor stroke 8 , and limbic encephalitis 9 and with a higher risk of Alzheimer’s disease (AD).10–14 In this regard, a recent systematic review of the literature 15 reported that ALF is quite a consistent finding in patients in the so-called preclinical stage of AD. By “preclinical stages”, we mean a heterogeneous condition that includes subjective cognitive decline (SCD) individuals, i.e., those who score normally on conventional cognitive tests but complain of subjective memory problems in daily life, 16 with cerebrospinal fluid (CSF) amyloid-β positivity 11 , and are APOEɛ4 and familial AD mutation carriers.10,13,14, 10,13,14 On the contrary, patients with overt memory impairment, e.g., mild cognitive impairment (MCI) and AD, showed an increased forgetting rate at standard delays (typically intervals ranging from 30 min to 2 h) but generally no additional loss at prolonged delays, e.g., 1-day post-encoding or more.17–25 Indeed, as expected, AD patients forgot significantly more than healthy controls already in short intervals, exhibiting instead a parallel decline over longer delays after 24 h. As for patients with MCI, only few studies reported the presence of ALF.16,26, 16,26 These discrepant results may be due to differences in testing methods (among other confounds). A relevant factor to pay attention could be the retrieval of the entire material at each testing interval, which may influence whether or not ALF is found. 27 On the other hand, the failure to find ALF could be due to floor effects on prolonged delays in patients with overt memory problems, already highlighted in conventional testing delays.
At any rate, the presence of ALF in these pre-clinical conditions is very interesting in a research context that is now focused on identifying the earliest and most subtle cognitive changes that occur before the overt diagnosis of cognitive impairment and dementia. In fact, it is currently known that the pathophysiological changes of AD arise a long time before the onset of objectively detectable clinical symptoms 28 and that the subjective feeling of memory concerns may be present several years prior to a clinical diagnosis of MCI or dementia. 29 In this framework, Jessen and colleagues 30 introduced the term ‘subjective cognitive decline’ to identify individuals with a persistent self-experienced decline in memory and other cognitive abilities despite regular performances on standard cognitive tests. Although SCD is often associated with several conditions that do not necessarily imply an underlying neurodegenerative cause (e.g., personality or psychiatric traits, general medical conditions, substance use, medication etc.), longitudinal studies have documented that individuals with SCD have a greater risk of MCI and AD dementia.29,31,32, 29,31,32
As memory concerns and worries in SCD subjects could hide the true mnesic deficit that is not adequately explored by standard memory tests, in the last few years a great deal of experimental research has been focused on the investigation of novel memory paradigms able to objectify in SCDs deficits not otherwise detectable with conventional neuropsychological tools (see, for example33–37). In this regard, only two studies thus far have investigated long-term forgetting in SCD. Manes and colleagues 16 evaluated the possible presence of ALF in participants with SCD by adopting a free recall task for verbal and visuo-spatial material delivered at standard (30 min) and prolonged (6 weeks) delays. These subjects showed normal recall at standard delays, but a significantly increased memory loss at the prolonged interval compared to healthy people. More recently, Tort-Merino and colleagues 12 investigated whether ALF was present in 52 cognitively unimpaired individuals using a novel memory procedure. They found that ALF was present in patients with high ratings of memory complaints, especially in those with abnormal CSF Aβ42 levels. However, the conclusions reached by both studies are questionable due to some methodological issues. For example, the sample size in Manes et al.’s study 16 was small (overall 10 individuals with SCD and 7 with MCI) and the experimental procedure did not equate initial learning rates in SCDs and HCs in order to avoid scaling problems in the interpretation of performance at various delays. Furthermore, it is uncertain whether the participants in Tort-Merino et al.’s study 12 really fit the inclusion criteria for SCD. In fact, despite higher scores on a self-report questionnaire, they did not actively seek medical help due to their concerns. 29 In addition, the lack of a healthy control group and memory assessment by standard intervals raises doubts regarding the possibility of early memory loss cannot be ruled out.
One concern in studying ALF is the neurobiological underpinning of the increased forgetting. Neurophysiological mechanisms underlying memory storage include an early synaptic consolidation phase, during which the hippocampus is the site of structural changes through new protein synthesis and new synapse formation, followed by a reorganization phase during which neocortical large-scale representations are configured.38–40 As the temporal scale of the two consolidation phenomena is largely unknown, it is unclear whether hippocampal or, alternatively, neocortical changes are mainly implicated in ALF (for a discussion of this topic, see Cassel and Kopelman 41 ). Moreover, neuroimaging research on the neural bases of ALF is sparse and controversial. Among these few studies, most of which refer to TLE populations, one reported the structural involvement of the hippocampus in patients with ALF 42 whereas others described a correlation between hippocampal volume and forgetting at shorter delays but not at prolonged ones.43,44, 43,44 In a study with TLE patients that investigated the involvement of resting state hippocampal connectivity in ALF, Audrain and colleagues 45 reported an inverse correlation between forgetting rate on a recognition task and resting-state connectivity between the anterior hippocampus and the lateral temporal cortex, a finding indicative of a disruption of hippocampal-neocortical interactions.
Investigating the relationship between forgetting rates and neurobiological changes in individuals with SCD could shed some light on this controversial issue. Recently, literature on SCD has focused on the investigation of brain structural damage as well as resting-state functional connectivity. Neuroimaging studies that investigated volumetric changes in patients with SCD reported inconsistent results: some studies documented decreased volume in the mesial temporal lobes46–48 or in some subcortical regions,49,50, 49,50 whereas others did not report significant changes51–54 (for a review, see Arrondo et al. 55 ). Interesting results were obtained by studies that analyzed resting-state functional connectivity and that showed alterations in the networks also involved in AD, such as the default mode network 56 , the salience network 57 and the executive control network58,59, 58,59 (for a review, see Wang et al. 60 ).
The main aim of the present study was to evaluate if ALF might be a feature of individuals who meet the criteria for SCD. With respect to previous studies that investigated this issue, our study has two important strong points. First, based on the diagnostic criteria suggested by Jessen and colleagues 29 which emphasizes medical help seeking as a significant feature of SCD linked more to the presence of AD biomarkers compared to non-help-seeking community SCD, we specifically included subjects with SCD who spontaneously approached our memory clinic because of their memory complaints. Moreover, to control for various confounding variables that are known to potentially hide or falsely exalt the observed forgetting rate, we adhered closely to the methodological recommendations proposed by Elliott and colleagues 4 (see below in the Methods section).
Given the lack of evidence on the neural underpinnings of ALF in SCDs, an additional goal of this study was to make an exploratory investigation of structural and functional patterns associated with this process by performing morphological and functional connectivity (FC) MRI analyses. We expected FC to be more sensitive than the structural studies in detecting early brain changes and identifying possible associations with ALF. Indeed, FC modifications are considered as a proxy measure of brain changes and can be observed several years before structural changes. 60
For these purposes, we compared a group of SCD individuals with a group of healthy controls using a long-term forgetting procedure that included recall and recognition tasks for verbal and visuo-spatial material assessed at standard (30 min) and extended (1-day and 1-week later) intervals. We stratified the SCD sample into two distinct sub-groups (i.e., mild SCDs and severe SCDs) according to the severity of their self-referred complaints, which was assessed with a self-report questionnaire. This stratification was consistent with previous findings which demonstrated a positive association between a higher level of complaints and worries and a greater amyloid burden.12,61, 12,61 Therefore, employing this stratification approach allowed us to identify patients at higher risk of progressing to MCI and effectively discriminating them from individuals at lower risk.
Moreover, to carry out an exploratory investigation of the brain structural and functional changes associated with increased forgetting rates, SCD participants were submitted to a 3T MRI exam. This allowed us to perform voxel-based morphometry (VBM) and resting-state functional connectivity (RS-FC) analyses.
MATERIALS AND METHODS
Subjects
Subjective cognitive decliners
We recruited a total of 31 individuals from the Alzheimer’s disease Unit and Neuropsychology Unit of IRCCS Santa Lucia Foundation where they had been referred because of a self-report of memory impairment. According to Jessen’s recommendations, 30 we established the following inclusion criteria for the enrolment of SCD individuals: (a) complaint of self-experienced memory decline; (b) normal age-, gender- and education-adjusted performance scores on all standardized cognitive tests of the screening neuropsychological battery; (c) exclusion of co-existing psychiatric or neurological diseases or acute events related to memory concerns; (d) over 50 years of age; (e) no history of drugs or alcohol abuse.
We split the sample of SCD individuals into two sub-groups based on the memory complaints score obtained on the Everyday Memory Questionnaire (EMQ) 62 (see below).
Healthy controls (HC)
We also recruited 16 age- and education-matched healthy subjects. The inclusion criteria were the following: (a) no referred self-experienced memory decline; (b) normal age- gender- and education-adjusted performances on the standardized cognitive tests of the neuropsychological screening battery; (c) no current or anamnestic report of psychiatric or neurological disease; (d) over 50 years of age; (e) no history of drugs or alcohol abuse.
In agreement with the Declaration of Helsinki, all participants provided their informed consent to take part in the study. The protocol of the present study was approved by the Ethical and Scientific Committee of IRCCS Santa Lucia Foundation.
General neuropsychological evaluation
All participants were submitted to a neuropsychological assessment to obtain a measure of their overall cognitive functioning. The administered tests are described below, according to the cognitive domain examined: Verbal episodic memory: 15 word-list immediate and 15-min delayed recall.63,64, 63,64 Attention and executive functions: Modified Card Sorting Test,
65
Trail Making Test parts A and B,
66
Phonological verbal fluency.
63
Reasoning: Raven’s colored progressive matrices.
63
Language: objects naming subtest of the Batteria per l’Analisi dei Deficit Afasici (BADA).
67
Global cognitive functioning: Mini-Mental State Examination (MMSE).
68
For all tests (except for object naming from the BADA), we used Italian normative data to adjust scores based on sex, age and education and to define normality cut-off scores (see corresponding references).
Everyday Memory Questionnaire
To obtain a measure of subjective experience of memory decline, all participants were administered the self-report “Everyday Memory Questionnaire” by Thompson and Corcoran. 62 The questionnaire consists of 18 statements about memory concerns in daily life (e.g., “Forgetting where you have put something, like losing things around the house”; “Having to go back and check whether you have done something you meant to do”; “Failing to relay important information to someone, perhaps forgetting to pass on a message or remind someone of something”). For each of the 18 items, participants were requested to indicate how often they had memory problems on a 6-point Likert scale (1 = never; 2 = about once in the past three months; 3 = about once a month; 4 = about once a week; 5 = about once a day; 6 = many times a day). A total score (EMQ-tot) was calculated by adding the response scores to each question (possible score range between 18 and 108) with higher scores indicating more memory complaints in daily life.
Long-term memory forgetting assessment
The experimental procedure for assessing long-term forgetting was administered at least one month after the standard neuropsychological evaluation. This time window was adopted to avoid any possible interference between the two evaluation sessions. The overall procedure was conceived so as to fully comply with the guidelines proposed by Elliott and colleagues. 4 In particular, i) we tested memory for both verbal (short story) and visuo-spatial (Rey complex figure) material; ii) we employed both recall and recognition procedures for memory testing; iii) we took into account ceiling and floor effects; iv) we equated the immediate recall level among participants by adapting stimulus exposure on an individual basis; v) we prevented rehearsal by not informing patients of subsequent re-testing sessions; vi) we avoided any short-term memory contribution to forgetting through rehearsal preventing tasks delivered between encoding and immediate recall. Moreover, to fit the first of Elliott et al.’s criteria, 4 we matched the participant groups for age and educational level and did not change any of the tests of the neuropsychological screening battery (see below).
For both tests, the sessions were administered in-person for the learning phase and the 30-min. recall, but by phone for the 1-day and 1-week sessions.
The experimental material for the Short story test consisted of a brief passage, i.e., three- sentences long; it included 26 elements (i.e., characters, plot, setting, time, consequences and other details). 69 For the free-recall task, participants were required to spontaneously recall as many elements of the story as possible. For each verbatim unit recalled or expressed with appropriate synonyms, one point was given (maximum score: 26). Differently, the multiple-choice recognition task consisted of ten questions (e.g., “What was the name of the main character in the story?), each with three alternative responses, one that was correct (e.g., Anna Pesenti) and two that were incorrect (e.g., Anna Polacco, Teresa Polacco). The maximum score was 10.
During the learning phase, the experimenter read the prose passage. Immediately afterwards the participant was involved in counting backward for approximately 30 s to prevent recall from short-term memory. At the end of the distractor task, the participant was required to recall as many elements of the story as possible. To ensure that the material was stored, he/she was exposed to at least two readings, even if the criterion was reached after the first reading. If he/she failed to recall 21 elements out of a total of 26 (i.e., 80% of all the material), the experimenter re-read the short story for a maximum of 8 trials. If the subject did not achieve the 80% accuracy criterion even at the eighth attempt, he/she was excluded. After the learning criterion was achieved, subsequent free recall tests were administered after 30 min (standard recall), 1-day, and 1-week (extended recall). The experimenter administered the multiple-choice recognition task only at the 1-week telephone testing session, after the free recall test.
The experimental material for the visual-spatial task consisted of Rey’s complex figure B (ROFC-B), a non-meaningful figure composed of 11 main elements. The maximum score in reproducing the ROFC-B is 31, which is obtained by adding the scores of the following four parameters: the presence of the elements (max score 11), the proportion between the elements (max score 4), the overlaps (max score 8) and the precision in execution (max score of 8) (for more details see Luzzi et al. 70 ). The free-recall task consisted of the spontaneous reproduction of the figure from memory. The recognition task, instead, required participants to identify the correct detail of the figure out of three similar alternatives (maximum score: 10).
In the study phase, the experimenter presented the participant with the ROCF-B and asked him/her to copy the figure as accurately as possible on a separate sheet of paper. At the end of the copy phase, the figure was removed, and the participant was asked to complete a distractor visual task, exactly as in the verbal test. In this case it consisted of cancelling “paper and pencil” stimuli (e.g., numbers, letters) for 30 s. Afterwards, the participant was given a blank sheet of paper and instructed to draw the figure from memory. Also in this case, the subject had a minimum of two and a maximum of eight trials to reach the 80% accuracy score (25 out of 31). Once the learning criterion was reached, the first recall was set at 30 min (standard recall). For the two extended intervals (1-day and 1-week), three closed, numbered envelopes containing a blank sheet of paper were handed out (two for the 1-day and 1-week free recall and one for the 1-week recognition task). When they were delivered, no instructions were given regarding the contents. The experimenter only advised the participant to leave the envelopes unopened until the telephone meeting. During both the 1-day and 1-week tests, the experimenter instructed the participant to open the envelope and to draw the figure from memory on the sheet of paper. During the 1-week test, the participant was also asked to complete the Recognition task. Finally, the experimenter instructed the participant to return the paper sheets by postbox or via telephone (e.g., Whatsapp).
To obtain an index of memory saving along the four testing intervals (i.e., learning, 30 min, 24 h, and 7 days) for each patient we calculated the proportion of the retained material after a specific delay compared with the previous one using the following formula: test session score x100/previous session score. In this way, we obtained the following three saving indexes: 30m-L (i.e., percentage of learned material retained after 30 min.) 24h-30 m (i.e., percentage of material retained after 24 h compared to 30 min) 7d-24 h (i.e., percentage of material recalled after 7 days compared to 24 h).
Image acquisition and processing
Regarding the overall SCD sample, 7 severe SCDs (age = 64.43±9.73; years of education = 10.43±5.97 years) and 10 mild SCDs (age = 57.9±9.73; years of education = 13.3±2.50 years) were submitted to a 3T MRI examination (Philips Achieva). These 17 participants were selected from the overall SCD sample with the constraint that they could not wear non-MRI-conditional devices and could not be claustrophobic. Moreover, in order to reduce the heterogeneity in the MRI data, they had to be right-handed as assessed by the Edinburgh Handedness Inventory. 71 A total of 14 participants were excluded from the MRI exam (5 because they were claustrophobic, 1 due to lens prosthesis implantation, 3 due to long-standing cholecystectomy, 3 because they had undergone operations involving the insertion of prostheses and screws with dubious compatibility with 3T MRI and 2 because they were left-handed). Written informed consent was obtained from each subject.
The acquisition protocol included: (1) a resting-state fMRI (RS-fMRI) scan using an echo planar imaging (EPI) sequence (TR = 2100 ms, TE = 30 ms, TSE factor = 10, matrix = 400×250×28, slice gap = 1.25, field of view [FOV] = 236×236×152.5 mm 3 , slice thickness = 2.5 mm, total number of slices = 41) during which participants were required to keep their eyes closed but not fall asleep and to not think of anything in particular, (2) an isotropic 3D fast fluid-attenuated inversion recovery (FLAIR) scan (TR = 4800 ms, TE = 125 ms, Inversion Time = 2800 ms, TSE factor = 182), and (3) a T1-weighted ultra-fast gradient echo (TR = 11 ms, TE = 5.3 ms, flip angle = 8°, matrix = 256×228×190, FOV = 230×234.33963×171 mm3, voxel size = 0.9×0.9×0.9 mm 3 ).
To obtain grey matter (GM) volumetrics, the T1-weighted volumes were first pre-processed using the VBM toolbox72,73, 72,73 implemented in the SPM12 software package (Statistical Parametric Mapping, http://www.fil.ion.ucl.ac.uk/spm/) running under MATLAB. The processing includes a repeated combination of segmentations and normalizations that are useful for generating GM probability maps for each subject72,73, 72,73 in standard space (Montreal Neurological Institute, or MNI coordinates). To compensate for the compression or expansion that might occur when warping the images to match the template, the GM maps were modulated by multiplying the intensity of each voxel in the final images by the Jacobian determinant of the transformation, which corresponded to its volume before and after warping. 72 GM, white matter (WM), and CSF values were then obtained for each individual and added together to compute the total intracranial volume. Data were finally smoothed using a 12-mm FWHM Gaussian kernel.
The RS-fMRI data were processed using SPM12 (Statistical Parametric Mapping 12; http://www.fil.ion.ucl.ac.uk/spm). In order to allow for T1 equilibration effects the first 4 volumes of each fMRI time series were discarded and then the following pre-processing steps were carried out: slice timing, head motion correction (by using the SPM12 realignment algorithm), co-registration with the corresponding anatomical images and spatial normalization to a standard stereotaxic space (MNI). Finally, EPI images were filtered using a phase-insensitive band-pass filter (pass band 0.01–0.08 Hz) to reduce low frequency drift and high frequency physiological noise effects and were then smoothed with an 8 mm 3 FWHM 3D Gaussian Kernel. Independent Component Analysis (ICA; Group ICA Toolbox; http://mialab.mrn.org/software/) was employed to identify 20 independent components by using GIFT, a MATLAB toolbox that uses a data-driven method to achieve a data-driven parcellation of brain activation. GIFT first concatenated the individual data across time, then produced a computation of subject specific components and time courses. The toolbox then performed the following analysis in 3 steps for all subjects grouped together: (1) data reduction, (2) application of the FastICA algorithm, and (3) back-reconstruction for each individual subject. We carefully inspected the resulting maps for all group-level ICA spatial maps, then we sorted out networks mainly reported in previous studies55–58 across the SCD individuals: the default mode network (DMN), the executive control network (ECN), the left and right fronto-parietal network (l-FPN and r-FPN), and the salience network (SAL).
Data analysis
Personal and neuropsychological data
Statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS, Version 22.0; Inc., Chicago, IL, USA). To detect differences in age and education between groups, as well as in standard neuropsychological test, results and EMQ scores, one-way analyses of variance (ANOVA) were run. Differences in gender distribution as well as in the number of learning trials needed to reach the criterion in the long-term memory procedures were assessed using the Chi-square test. To compare the accuracy scores of the three groups on the recall tests at the four delays of the experimental procedure, a repeated-measures ANOVA was used, with Group (HC versus mild SCD versus severe SCD) as between factor and delay (learning score versus 30-min recall versus 24-h recall versus 7-days recall) as within factor. Saving indexes between recall tests as well as recognition scores were analyzed by means of one-way ANOVAs. Post hoc analyses were performed using the Tukey test for multiple comparisons.
To evaluate the usefulness of the memory saving indexes in discriminating severe SCDs from mild SCDs and healthy controls, receiver-operating characteristic (ROC) curves were generated. Areas under the curves (AUCs) were used as a measure of the overall performance of the ROC curves (with a 95% Confidence Interval – CI) and specificity and sensitivity were reported.
Finally, possible associations between long-term saving indexes and the degree of subjective memory complaints (measured by EMQ scores) were explored using Pearson’s correlation test.
MRI analysis
We performed statistical analyses of regional GM volumes on SPM-12, using smoothed GM maps within the framework of the general linear model.
A two-sample t-test model was performed to assess GM volume differences between the mild SCD and severe SCD groups. We also investigated the relationship between GM volumes and long-term memory (accuracy scores and saving indexes) by using one-sample t-test models in both the whole sample and in the two subgroups (mild SCDs vs severe SCDs separately). Intracranial volumes were entered in all analyses as covariates of no interest. Statistical significance was set at p < 0.05 FWE-corrected at the cluster level.
The RS-fMRI second level analysis was performed in SPM12 using a two-sample t-test model to assess FC differences between mild and severe SCDs in the different brain networks extracted (DMN, ECN, r-FPN, l-FPN, SAL). Moreover, a series of one sample t-test models were used to investigate associations between changes in FC and experimental recall scores, as well as derived saving scores. These analyses were conducted on both the entire sample and the two SCD sub-groups. Statistical significance was set at p < 0.05 FWE-corrected at the cluster level.
RESULTS
SCD group split based on the EMQ score
On the EMQ, on average the HC group scored 35.2 (SD = 7.8; range 23–54). We subdivided patients in the SCD group based on the severity of their memory complaints: 18 patients who scored ≤ 54 (the highest score obtained by any individual in the HC group) were included in the “mild” SCD group (M = 42.1; SD = 9.6; range 25–54); the remaining 13 patients who reported ratings ≥ 54 were included in the “severe” SCD group (M = 71.0; SD = 7.8; range 58–84).
Demographic and screening neuropsychological data
As reported in Table 1, no significant differences were found between the HC and the two SCD groups for age and educational level. However, the Chi-Square test showed a statistically significant difference in gender distribution. Indeed, quite surprisingly, no male was included in the severe SCD group. Table 2 reports the adjusted mean scores obtained by the three groups on each test included in the neuropsychological screening battery. For BADA object-naming, raw scores were reported because normative data for score adjustment are unavailable. Also, for the MMSE, we used raw scores due to the lack of normative data for the age of our sample. Statistical analyses revealed no significant between-group differences on any of the tests employed.
Demographic data of HC, mild SCD and severe SCD individuals
Mean scores with standard deviations in parenthesis. HC, healthy controls; Mild SCD, mild subjective cognitive decline; Severe SCD, severe subjective cognitive decline.
Adjusted mean scores (and SDs) of the three groups of HC, mild SCD and severe SCD individuals on the tests of the screening neuropsychological battery (due to the unavailability of normative data for the BADA object naming test and the MMSE, raw data are reported)
Mean scores with standard deviations in parenthesis. HC, healthy controls; Mild SCD, mild subjective cognitive decline; Severe SCD, severe subjective cognitive decline; MMSE, Mini-Mental State Examination; WL, Word-list test; MCST, Modified Card Sorting test; TMT, Trail Making Test.
Long-term forgetting assessment
Short story
All participants completed the experimental procedure for all testing delays administered. No difference was observed in the number of trials needed by the three groups to reach the pre-set criterion (HC: M = 2.50, SD = 0.44; mild SCD: M = 2.38, SD = 0.79; severe SCD: M = 2.46, SD = 0.8; χ 2 3.47; p = 0.18). Results of the two-way Group x Delay ANOVA on recall scores across the four delay intervals (Fig. 1) revealed a Group effect that approached significance, F (1, 43) = 3.07; p = 0.056, and a significant Time effect, F (1, 43) = 77.53; p < 0.01, due to the progressively lower accuracy of the overall group across successive testing delays. A significant interaction between the two factors, F (2,43) = 2.65; p < 0.05, was also found. Planned comparisons made to qualify this interaction revealed that the recall of severe SCDs was significantly poorer than that of HCs at both extended delays, i.e., 24 h and 7 days (p < 0.05 in both comparisons), but not at the standard 30 min interval (p = 0.33). No significant difference was found between the HC and the mild SCD groups or between the mild and the severe SCD groups at any interval considered (p consistently >0.10).
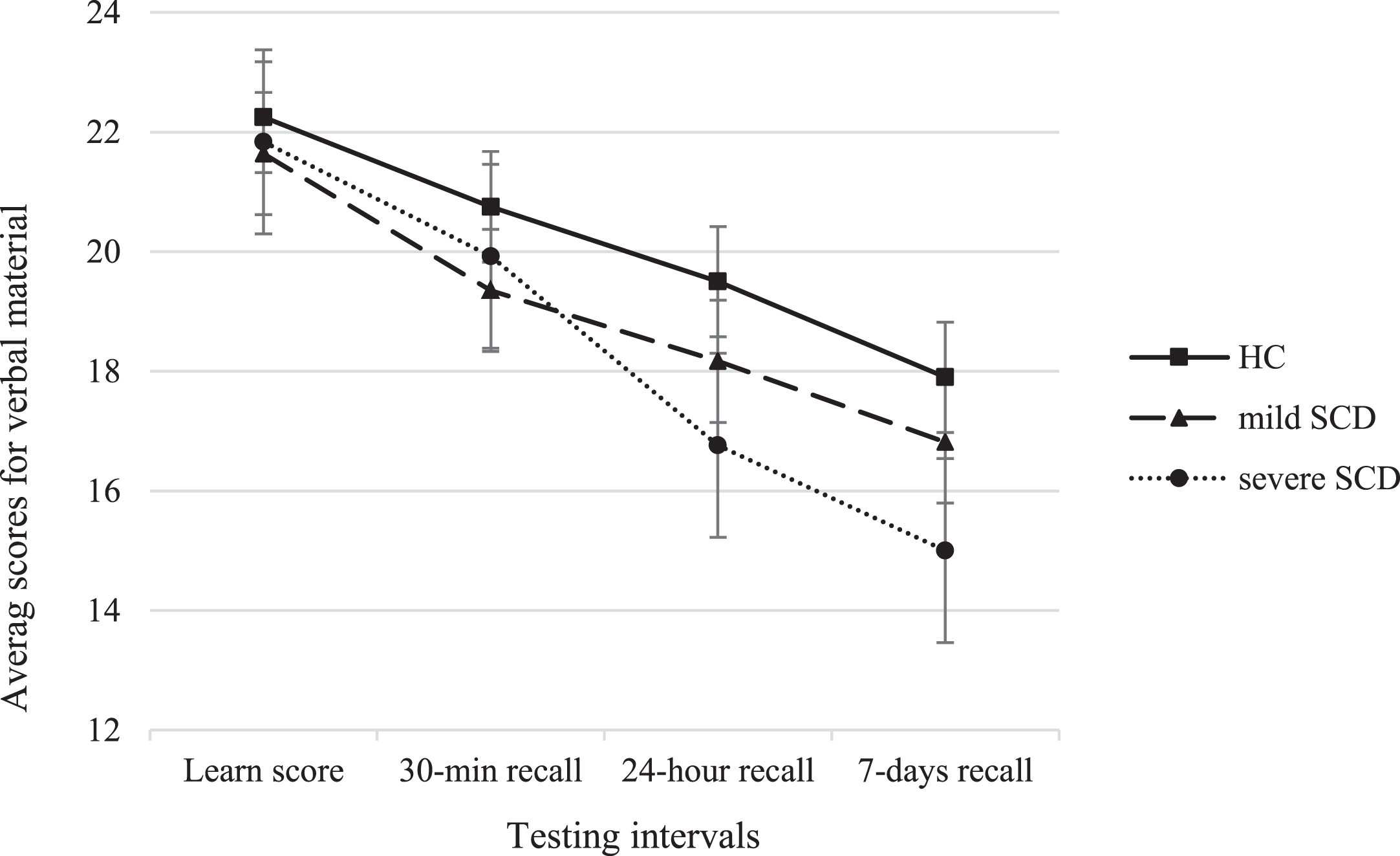
Average recall scores of the HC, mild SCD and severe SCD groups across the four delay intervals of the Short story test (bars represent standard errors). HC, healthy controls; severe SCD, severe subjective cognitive decline; mild SCD, mild subjective cognitive decline. Maximum score = 26.
The pattern indicative of ALF in the severe SCD group was reinforced by the between-group comparisons of saving indexes (Table 3). Indeed, on 24h-30 m index severe SCDs retained significantly less information than HCs and mild SCDs. By contrast, on the 30m-L and the 7d-24 h, the three groups exhibited similar saving indexes. Thus, the only interval at which the performance of the severe SCD group declined more than that of the other two groups was between 30 min and 24 h.
Verbal material saving indexes in the HC, mild SCD and severe SCD groups
Mean scores with standard deviations in parenthesis. HC, healthy controls; Mild SCD, mild subjective cognitive decline; Severe SCD, severe subjective cognitive decline; 30m-L, 30 min recall×100/learning; 24h-30 m, 24 h recall×100/30 min; 7d-24 h, 7 days recall×100/24 h; ¤significantly different from HC; †significantly different from mild SCD.
ROC curves were calculated to evaluate the diagnostic utility of the computed indexes. It emerged that only the 24h-30 m saving index discriminated severe SCDs from mild SCDs (AUC = 0.77; CI 95% [0.59–0.94], p = 0.01, maximum sensitivity and specificity = 78% and 69%).
Analysis of the recognition scores between groups showed a trend toward significance, F (2, 44) = 2.6; p = 0.08, due to the lower scores of severe SCDs (M = 9.08; SD = 0.95) compared to those of HCs (M = 9.7; SD = 0.75; p = 0.03), whereas the recognition scores of the mild SCD group (M = 9.28; SD = 0.95) did not differ from those of the other groups (p > 0.05 in both cases).
Finally, the results of Pearson’s correlation analyses showed a significant negative association in the SCD group between the EMQ total score and the 24h-30 m saving score (r = –0.458; p < 0.01). Correlations between EMQ and all other retention indexes were far from significance (i.e., r ranged between 0.11 and –0.33; p consistently >0.10). Thus, higher memory complaints predicted lower retention scores at 24 h.
Complex figure
All participants completed the experimental procedure for all testing delays administered except for one mild SCD who failed to return the testing material for the 24 h and 7-day recall. Also in this case, the three groups of participants needed a similar number of trials to reach the learning criterion (HC: M = 2.06, SD = 0.44; mild SCD: M = 2.39, SD = 0.7; severe SCD: M = 2.46, SD = 0.87; χ 2 = 1.65; p = 0.44). The two-way ANOVA on recall scores across the four delay intervals (Fig. 2) showed a significant Time effect, F (1, 41) = 28.8, p < 0.01, also in this case it was the expression of a gradual decline in accuracy across delay intervals, but not a significant Group effect, F (2, 41) = 1.38, p = 0.26, due to the similar overall performances of the three groups. The Group x Time interaction was also nonsignificant, F (2, 41) = 0.86, p = 0.53.

Average reproduction scores of the HC, mild SCD, and severe SCD groups across the four delay intervals of the ROCF-B test (bars represent standard errors). HC, healthy controls; severe SCD, severe subjective cognitive decline; mild SCD, mild subjective cognitive decline. Maximum score = 31.
Associations between brain networks FC and experimental verbal long-term memory measures in the SCD group
DMN, default mode network; FPN, fronto-parietal network; SAL, salience network; FC, functional connectivity; GM, grey matter; 24h-30 m, percentage of material retained at 24 h compared to 30 min; V1 BA17, Primary Visual Cortex (Brodmann Area 17); V2 BA 12, Secondary Visual Cortex (Brodmann Area 18); Side, hemisphere; Size, volume; T, T-value for each peak (peak intensity).
The saving indexes of the three groups did not significantly differ at any of the delay intervals (p consistently >0.10). The same was true for the recognition scores (HC: M = 9.62, SD = 0.5; mild SCD: M = 9.00; SD = 1,37; severe SCD: M = 9.38; SD = 0,77), F (2, 44) = 1.73, p = 0.19.
Finally, in the SCD group no significant correlation was found between saving indexes at any delay and EMQ scores (r ranging between 0.02 and –0.02; p consistently >0.10).
Neuroimaging data
VBM analysis did not show any GM volume differences between severe and mild SCD. Moreover, no significant associations between GM volumes and experimental memory scores were found, either when the entire sample was considered or when the mild and severe sub-groups were considered separately.
Similarly, when we examined the association between the brain networks’ functional connectivity and experimental memory scores, we did not find any significant differences between the two groups (severe and mild SCD). However, significant associations were observed when we considered the entire SCD sample (Table 4). In particular, when we examined specific brain networks, we observed significant positive relationships between experimental memory scores on the Short Story task (24 h delayed recall and 24h-30 m saving index) and FC in the left DMN, left FPN and SAL networks (see Table 4 for details).
In the left DMN, we found a significant positive association between the 24 h delayed recall score and FC in the following brain regions: the left lateral occipital cortex, the left middle temporal gyrus, the left inferior parietal lobule, and the left angular gyrus (Fig. 3).
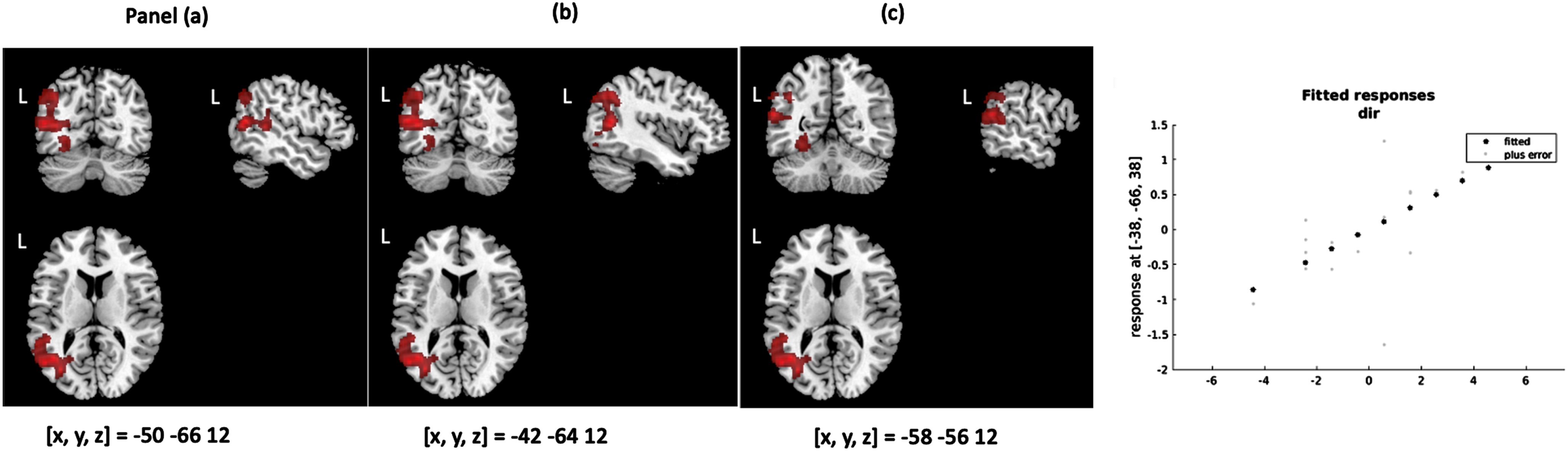
Associations in whole SCD sample between FC into DMN and 24 h delayed recall of the short story. Direct association between 24 h delayed recall and FC in the Lateral Occipital Cortex (a), middle temporal gyrus, inferior parietal lobule, and lateral occipital cortex (b), angular gyrus (c) within the DMN in the left hemisphere. Scatter plot also reported the association between 24 h delayed recall and FC in the maximum peak. SCD, subjective cognitive decline; FC, functional connectivity; DMN, default mode network; L, left.
Regarding the left FPN, direct associations were observed between the 24h-30 m saving score and FC in the following areas: the left postcentral gyrus, the left superior parietal lobule, and the right precuneus. Finally (Fig. 4), regarding the SAL, we found a direct association between the 24h-30 m saving score and the FC in the left visual cortex and the lingual gyrus (Fig. 5).

Associations in whole SCD sample between FC into FPN and 24h-30 m saving index of the short story. Direct association between 24h-30 m verbal saving index and FC in the left postcentral gyrus, left superior parietal Lobule (a) and right precuneus (b) within the FPN. Scatter plot also reported the association between 24h-30 m saving index and FC in the maximum peak. SCD, subjective cognitive decline; FC, functional connectivity; FPN, fronto-parietal network; 24h-30 m, percentage of material retained at 24 h compared to 30 min; L, left.

Associations in whole SCD sample between FC into SAL and 24h-30 m saving index of the short story. Direct association between 24h-30 m verbal saving index and FC in the Visual Cortex V1 BA17 (a), the Lingual Gyrus and Visual Cortex V2 BA18 (b) within the SAL in left hemisphere. Scatter plot also reported the association between 24h-30 m saving index and FC in the maximum peak. SCD, subjective cognitive decline; FC, functional connectivity; FPN, fronto-parietal network; SAL, salience network; 24h-30 m, percentage of material retained at 24 h compared to 30 min; L, left; V1, Primary Visual Area; BA17, Brodmann Area 17; V2, Secondary Visual Cortex Area; BA18, Brodmann Area 18.
No significant associations were found between the ECN or r-FPN and the experimental memory scores or saving indexes.
Finally, no significant associations were found between FC and recall scores or saving indexes on the Complex Figure task.
DISCUSSION
Individuals with SCD are currently a primary target in clinical research on Alzheimer’s disease. Although the self-perceived cognitive changes of these individuals are not yet objectively detectable, they impact their daily life to such an extent that they seek medical help. In fact, these changes are likely predictors of future overt cognitive decline, making it crucial to address this population for early intervention.32,74,75, 32,74,75 Thus, it is essential to identify the cognitive phenotype of this clinical condition and develop neuropsychological methods able to sensitively capture these subtle difficulties. This could lead to enhanced secondary prevention strategies.
To undertake this major challenge, we set out to determine whether ALF was present in a group of subjects with SCD. Notably, this is the first study that has aimed to assess whether ALF is present in individuals who spontaneously seek medical assistance because of their memory concerns, a factor known to boost a dementia progression risk. 29 To ensure methodological rigor and minimize any potentially confounding effects, we designed a procedure that is consistent with the recommended guidelines for investigating forgetting.4,15, 4,15 Furthermore, given that a higher level of memory complaints and concerns is associated with greater amyloid burden findings, 61 we stratified the clinical sample according to the intensity of the subjective symptomatology. This allowed us to identify patients who were at higher risk of progression. Based on these considerations, we compared mild SCDs and severe SCDs (all of whom sought medical care in our clinic) with a group of HCs on verbal and visuo-spatial memory procedures, including early (30 min) and prolonged (24 h and 7 days) testing intervals.
As expected, we found that the three groups performed comparably on all tests of the neuropsychological screening battery, which assessed global cognitive functioning and specific cognitive domains such as memory, executive functioning, attention, language and reasoning. Interestingly, the mean scores of both the mild and the severe SCD groups were well above the cut-off values for each task administered, confirming the almost complete lack of sensitivity of standard neuropsychological assessments in capturing subjective complaints.
The main finding of the present study is that in the verbal long-term memory procedure, severe SCDs displayed a significant ALF compared to the other two groups, despite having comparable scores on immediate and 30 min delayed recall. This abnormal memory decline was actually the expression of a higher forgetting rate in the severe SCDs passing from the 30 min to the 24 h interval. Conversely, in the subsequent 7 days the forgetting slope exhibited by severe SCDs paralleled that of the other two groups, as demonstrated by comparable saving scores.
The presence of a verbal ALF in individuals with SCD is consistent with the findings of a few previous studies available on preclinical AD. Indeed, based on an extensive review of the literature, we previously reported that although the presence of ALF is controversial in MCI (due to heterogeneous results) and typically absent in patients with AD, it is a consistent finding in individuals considered, for one reason or another, to be in the preclinical stages of AD. 15 In particular, verbal ALF has been observed in individuals with positivity for CSF AD biomarkers,11,12, 11,12 with increased genetic risk for sporadic AD13,14, 13,14 and familial forms of AD.10,75,76, 10,75,76
Further reinforcing the view of an association between ALF and rate of subjective memory complaints, in the overall SCD group the ability to retain verbal material from 30 min to one day (24h-30 m index) was more impaired the more pronounced the subjective referral. An association between ALF and subjective report of memory loss was reported by Weston and colleagues 10 in a group of individuals who had an autosomal dominant pathogenic mutation of AD. Interestingly, although these patients were not recruited because they worried about memory difficulties spontaneously, they disclosed a high rate of memory complaints when assessed on a self-report questionnaire. In the same vein, Tort Merino and colleagues 12 stratified a sample of cognitively unimpaired individuals in low and high SCDs, based on their self-report rate of memory concerns. They found a significant association between higher rates of worrying and neuropsychological indexes of ALF, especially in those with abnormal Aβ42 levels. Furthermore, the authors observed that amyloidosis did not seem to influence long-term forgetting in individuals without memory worries, suggesting that ALF is a suitable procedure to use with SCD patients able to catch subjects at higher risk of amyloidosis and subsequent progression.
The normal decay of memory traces in mild SCD (with EMQ scores similar to those of HC) suggests that the detection of ALF in these patients could depend on the disease staging, i.e., as suggested by Schwarz and colleagues, 61 the severity of memory complaints is likely linked to greater neurodegeneration indexes, correlating with higher ALF and proximity to symptom onset. Obviously, since a biomarker-based or follow-up based diagnostic characterization of reported symptoms in SCD patients is lacking, these considerations are just speculative.
The observed dissociation between verbal and visual material, with the finding of normal forgetting on visual-spatial memory tests in individuals who, instead, exhibited ALF on verbal tests, is not uncommon in the literature on TLE patients77–81. This asymmetric pattern could indicate that verbal tests are more sensitive in detecting the ALF profile. Obviously, further studies are needed to confirm this suggestion.
Consistent with the methodological guidelines, 4 the results of our recall procedure were not confounded by ceiling/floor effects. Conversely, accuracy on the 7-day recognition test of both the verbal and visuo-spatial procedure was close to ceiling in most of the participants (47%). This could have been due to the relatively easy multiple-choice recognition paradigm in comparison with the challenging free recall task in individuals with very subtle memory difficulties, such as SCDs. However, despite this procedural pitfall on the verbal test the average recognition accuracy in the severe SCD group was almost significantly lower than that of the HC group, in substantial agreement with the results of the recall task.
As a secondary aim, in this study was conducted an exploratory MRI investigation to investigate the neural underpinning of the ALF pattern in individuals with SCD. The results, which should be considered preliminary due to the limited sample size, did not reveal significant differences between the severe and mild SCD groups in terms of either GM volume or FC. This lack of distinction suggests that neuroimaging measures employed may not have been sensitive enough to detect subtle differences between the two groups, which were categorized based solely on the severity of their reported cognitive complaints. However, when we considered the whole SCD sample, we found associations between long-term (but not early) verbal forgetting and FC in some critical cortical networks, such as DMN, FPN and SAL.
DMN’s key role in the episodic memory process has been widely documented 82 as has the fact that it represents a particularly sensitive network for early prodromal neurodegenerative changes associated with the AD continuum.56,83,84, 56,83,84 In line with this state of the art, we found a direct association between extended memory (1-day recall of the story) and FC of areas belonging to DMN: the left lateral occipital cortex, which is involved in the reactivation of a schema representation and in associative memory performances, 85 the left middle temporal gyrus, which is implied in control of semantic retrieval, 86 the left inferior parietal lobule, and in particular the left angular gyrus, which is suggested to be a crucial region for episodic memory.87,88, 87,88 This finding suggests that, because of to its role in memory consolidation, a reduced FC within the DMN could lead to an ALF at 24 h after the learning phase, thus affecting the ability to effectively consolidate and retain information.
Interestingly, we found FC associations that were not restricted only to the DMN regions but that also involved areas belonging to FPN and SAL. Indeed, our results showed positive associations between the 24h-30 m saving score and the FC in left FPN areas (left postcentral gyrus, left superior parietal lobule, and right precuneus), thus supporting its involvement in consolidating memories over time.89,90, 89,90 Moreover, taking into consideration the SAL, the 24h-30 m index is positively associated with FC in the left visual cortex and lingual gyrus. Previous studies91,92, 91,92 proposed the existence of a visual compensatory mechanism as one of the early modifications in response to subtle cognitive decline. These studies found associations between subjective memory complaints and the FC of the visual cortices, including the cuneus and lingual gyrus. Moreover, increased RS-FC in the medial visual network were found by Hafkemeijer and colleagues 46 in older adults with SCD. Together, these FC findings suggest that variations in neural connectivity within these networks may contribute to the observed ALF in individuals with SCD. However, this association transcended the classification between mild and severe SCD.
The associations between memory indexes and FC (but not volumetric measures) in individuals with SCD were previously described in a recently published study, 93 where the authors hypothesized that early functional alterations might precede and potentially drive structural changes in the progression from SCD to manifest cognitive impairment. Longitudinal studies are needed to clarify the temporal dynamics and casual relationship between these two mechanisms in SCD.
Our cognitive findings shed light on a crucial time frame during which the greatest oblivion occurs in SCDs, i.e., between 30 min and 24 h after the initial encoding of information. This temporal segment might constitute a critical window for ALF in SCDs. At a speculative level, the observation that, in an extended time frame, a group of memory disordered patients show steeper a forgetting curve than that of healthy subjects at a given temporal segment but a parallel one in a later segment is at a variance with the hypothesis of Cassel and Kopelman 41 , i.e., that ALF is substantially a bias resulting from progressively greater difficulty in retrieving episodic information as the retention interval increases. In fact, according to this hypothesis the forgetting curve in the patients and in the healthy groups should progressively diverge, with statistically significant differences appearing belatedly and becoming stronger as the retention interval increases. 41 The forgetting profile exhibited by the severe SCD group in the verbal paradigm is, instead, consistent with the alternative hypothesis that ALF reflects the derangement of a specific mechanism in the overall consolidation process. 94 Interestingly, our neuroimaging investigation provides evidence of an association between ALF in the specific 30m–24 h time delay and reduced FC within important brain networks. We might speculate that the specific derangement in the overall consolidation process put forward by Mayes and colleagues 94 is underpinned by impaired FC in important cortical regions in SCD individuals, and thus reflects the disruption of neural communications between crucial cortical and subcortical regions, possibly involving hippocampal-neocortical connections. While MRI results showed associations with ALF only when considering the whole sample, on cognitive tasks we observed a significant ALF in the severe SCD group when compared to both the mild SCD and healthy control groups. This discrepancy between neuroimaging results and cognitive performance underscores the complexity of the relationship between neural mechanisms and behavioral outcomes in SCD.
Several limitations of the present study should be considered. First, the relatively small sample size could affect the generalizability of our findings. Replication of these results in a larger sample is needed, certainly by including, for MRI investigation, a control group for comparison. Second, the questionnaire used for assessing memory complaints (i.e., the EMQ) 62 has not been validated for the Italian language; thus, due to the lack of a cut-off value, we proposed a differentiation of the SCDs sample based on HCs scores. Third, we did not assess participants’ sleep, despite its essential role in memory consolidation.95,96, 95,96 This aspect is critical because the oblivion in SCDs concerns precisely one-day post-encoding; thus, it could be helpful to evaluate sleep quality. Fourth, as much as possible we tried to comply with methodological guidelines, even if some issues (such as rehearsal or ceiling/floor effect) were challenging to control. Fifth, using the same material for all testing sessions could influence the results due to repetition of information.27,97,98, 27,97,98 It would be appropriate, in future studies, to address this issue by employing different prose passaged in different recall intervals. Furthermore, although we ruled out anxiety or depressive disorders at the time of recruitment, we did not collect psychological data in the clinical group, which could potentially exert confounding effects in long-term forgetting performances. In future works, it may be crucial to assess their impact. Finally, the neuroimaging investigation was largely exploratory and lacked strong predictions. Future work could capitalize on the results of the present study to investigate connectivity changes that might underlie deranged consolidation mechanisms in the long-term frame).
Therefore, in future studies we plan to replicate our cognitive and neuroimaging results in a larger sample, to make longitudinal evaluations during clinical follow-ups and to potentially combine the cognitive data with AD-related biomarkers. We also plan to collect normative data to devise standardized ALF procedures and subjective memory questionnaires that are suitable for use in clinical practice.
In summary, we suggest that verbal long-term forgetting procedures might be sensitive in capturing higher rates of subjective memory complaints of SCD patients. We highlight the importance of extending the time frame of the memory assessment, comprising prolonged delays of at least one day. Finally, we also suggest that functional analysis of resting-state connectivity involving the DMN, FPN, and SAL areas offers a new perspective on the neural bases of ALF. Interruptions in functional interactions within these networks can lead to inefficient consolidation processes which could manifest with ALF.
AUTHOR CONTRIBUTIONS
Marta Rodini (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review & editing); Sabrina Bonarota (Data curation; Formal analysis; Investigation; Writing – original draft); Laura Serra (Supervision; Writing – review & editing); Carlo Caltagirone (Funding acquisition); Giovanni Augusto Carlesimo (Conceptualization; Methodology; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We would like to thank Flavia Loreto for helping us in the initial conceptualization of the study, our participants for their time and the reviewers for their feedback.
FUNDING
This research was funded by the European Union - Next Generation EU - NRRP M6C2 - Investment 2.1 Enhancement and strengthening of biomedical research in the NHS under the grant PNRR-MAD1068 2022-12376889 – CUP J83C22002120007.
CONFLICT OF INTEREST
The authors have stated explicitly that they have no conflicts of interest in connection with this article.
DATA AVAILABILITY
Data that support the findings of this study are available on request from the corresponding author (MR). The data are not publicly available due to privacy or ethical restrictions.