
Abstract
Background:
The current application effects of computerized cognitive intervention are inconsistent and limited to hospital rehabilitation settings.
Objective:
To investigate the effect of mobile intelligent cognitive training (MICT) on patients with post-stroke cognitive impairment (PSCI).
Methods:
This study was a multicenter, prospective, open-label, blinded endpoint, cluster-randomized controlled trial (RCT). 518 PSCI patients were stratified and assigned to four rehabilitation settings, and then patients were randomized into experimental and control groups in each rehabilitation setting through cluster randomization. All patients received comprehensive management for PSCI, while the experimental group additionally received MICT intervention. Treatment was 30 minutes daily, 5 days per week, for 12 weeks. Cognitive function, activities of daily living (ADL), and quality of life (QOL) were assessed before the treatment, at weeks 6 and 12 post-treatment, and a 16-week follow-up.
Results:
Linear Mixed Effects Models showed patients with PSCI were better off than pre-treatment patients on each outcome measure (p < 0.05). Additionally, the improvement of these outcomes in the experimental group was significantly better than in the control group at week 6 post-treatment and 16-week follow-up (p < 0.05). The rehabilitation setting also affected the cognitive efficacy of MICT intervention in improving PSCI patients, and the degree of improvement in each outcome was found to be highest in hospital, followed by community, nursing home, and home settings.
Conclusions:
Long-term MICT intervention can improve cognition, ADL, and QOL in patients with PSCI, with sustained effects for at least one month. Notably, different rehabilitation settings affect the cognitive intervention efficacy of MICT on PSCI patients. However, this still needs to be further determined in future studies.
Keywords
INTRODUCTION
Stroke, characterized by cerebrovascular-induced neurological impairment [1], has been described as a significant source of high morbidity, mortality, and disability rates worldwide [2]. Likewise, studies have shown that more than 20% –80% of patients experience varying degrees of cognitive impairment after a stroke, and some may even develop severe dementia [3, 4]. Post-stroke cognitive impairment (PSCI) refers to a heterogeneous group of diseases that cause or lead to cognitive decline after stroke, classified as a clinical cerebrovascular event [5]. The main manifestations are memory, attention, executive dysfunction, and hemispatial neglect [6], especially working memory, short-term memory, decision-making, planning and organization ability [7]. Unfortunately, these seriously affect patients’ activities of daily living (ADL) and quality of life (QOL), further exacerbating the functional disability caused by stroke [8]. Furthermore, one study has indicated that the pathogenesis of PSCI is diverse, including cerebral infarction, neuronal injury, white matter injury, and small vessel disease [9]. Therefore, proactive treatment for PSCI patients is vital.
Post-stroke cognitive rehabilitation is usually based on functional neuroplasticity [10] and specific learning strategies [11] to restore or compensate the function of damaged brain regions. In recent years, clinical cognitive rehabilitation, in addition to drug therapy, manual cognitive training, and occupational therapy (OT), computered cognitive training intervention has received increasing attention. However, it is mainly based on the perspective of cognitive education, lacking systematic framework and pertinence, and is limited to the hospital rehabilitation setting [12]. Consequently, about 65% of PSCI patients are discharged from the acute phase and referred to home, community, and nursing home [13]. Currently, due to the lack of professional practitioners and intervention methods in out-of-hospital rehabilitation settings, cognitive training of patients is often interrupted, thereby affecting their rehabilitation outcomes [14]. There is also a lack of research on out-of-hospital cognitive rehabilitation at this stage, which cannot provide guidance for PSCI patients’ out-of-hospital rehabilitation.
Based on computer information technology, we have developed and iteratively optimized a mobile intelligent cognitive training application that can be applied to different rehabilitation settings and put into hospitals, communities, homes, and nursing homes for effectiveness studies. This application not only has the advantage of self-adaptive adjustment of training difficulty but also can break through the limitation of time and space, extending cognitive rehabilitation from the hospital to different rehabilitation settings outside the hospital, which is conducive to the continuity of rehabilitation treatment for PSCI patients. Mobile Intelligent Cognitive Training (MICT) is a new type of cognitive intervention with a background in cognitive neuroscience and rehabilitation medicine. Notably, it adopts the information processing theory and provides online training with the help of an internet platform [15]. Based on the theory of cognitive reserve [16] and central nervous system plasticity [17], MICT intervention can activate the release of the patient’s original cognitive reserve or establish new neural circuits through repeated cognitive task stimulation, improve the efficiency of neural synapses, and promote the reconstruction of the cerebral cortex to improve cognitive impairment.
The study aims to explore the short- and long-term effects of MICT intervention on PSCI and whether there are efficacy differences in cognitive interventions in different rehabilitation settings (hospital versus community versus home versus nursing home).
METHODS
Study design
This study was a multicenter, prospective, open-label, blinded endpoint, cluster-randomized controlled trial (RCT) in which all participants provided written informed consent. The study was approved by the Medical Ethics Committee of the China Rehabilitation Research Center (2020-082-1) and registered in the China Clinical Trials Registry Register (ChiCTR2000040598). The study adhered to the CONSORT guidelines for reporting randomized trials.
Participants
Participants with PSCI were recruited from four different rehabilitation settings: hospital, community, home, and nursing home between March 1, 2021, and December 1, 2023. The patients’ screening, randomization, allocation, and completion are shown in Fig. 1.
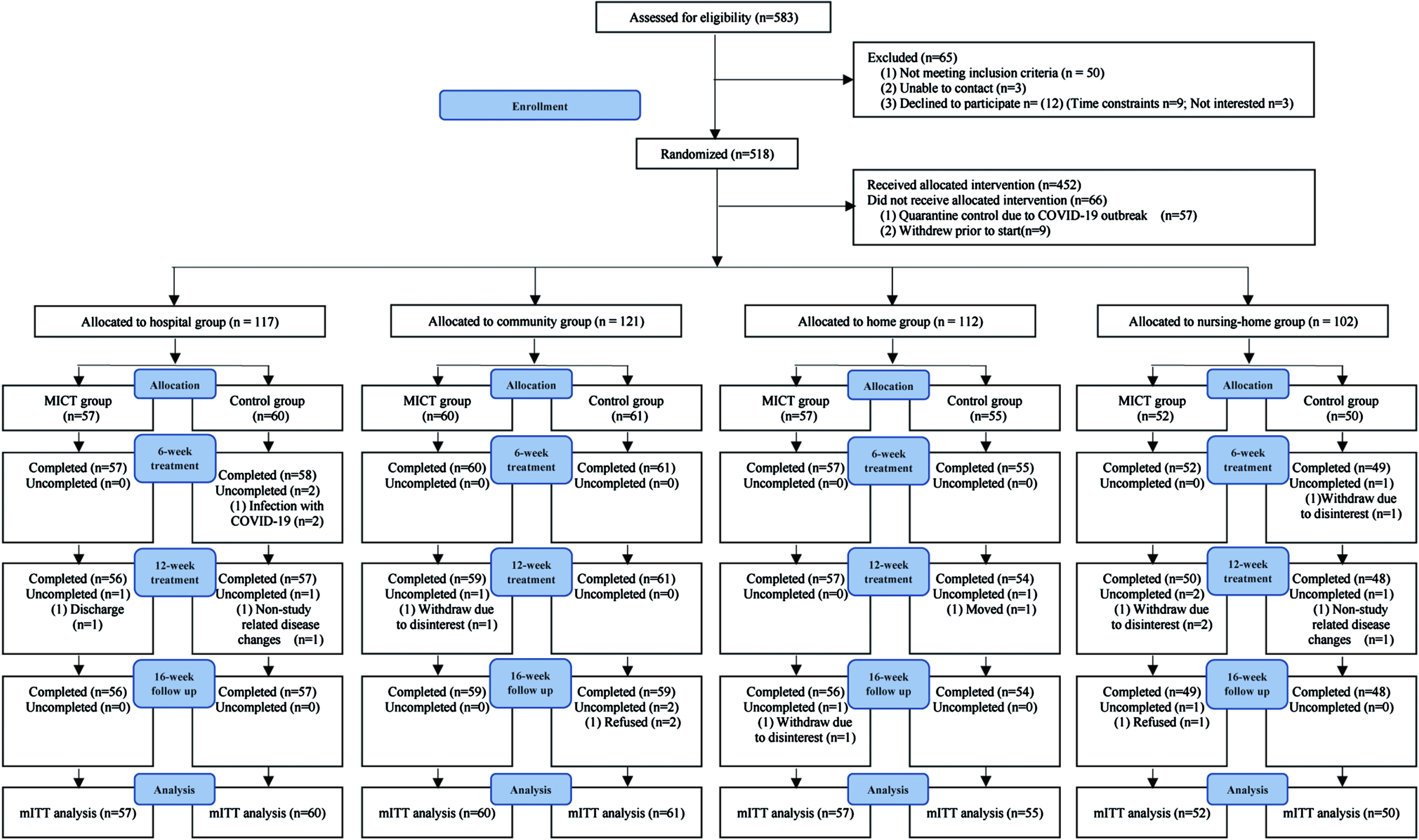
Flow diagram of the study population. MICT, mobile intelligent cognitive therapy; mITT, modified intention-to-treat.
Inclusion criteria were as follows: 1) meeting the diagnostic criteria for stroke [18, 19] and confirmed by computed tomography (CT) or magnetic resonance imaging (MRI); 2) stroke duration of 1 month or more and stable vital signs; 3) age 45 years and older, gender not limited; 4) mild or moderate cognitive impairment (Montreal Cognitive Assessment (MoCA) score < 26 or Mini-Mental State Examination (MMSE) score < 27 and MMSE score ≥10) [20, 21]; 5) can cooperate with the completion of relevant assessments and treatments; and 6) signed informed consent.
Exclusion criteria were as follows: 1) illiteracy; 2) pre-stroke diagnosis of cognitive dysfunction due to diseases other than stroke such as mild cognitive impairment, Alzheimer’s disease, frontotemporal dementia, Lewy body dementia, vascular dementia, Parkinson’s disease dementia, traumatic brain injury; 3) impaired consciousness; 4) severe comprehension aphasia and audiovisual dysfunction; 5) severe psychiatric disorders; 6) severe primary diseases of the circulatory, respiratory, digestive, urinary, endocrine, and hematopoietic systems that cannot be controlled with conventional medications; 7) had a history of drug or alcohol abuse; 8) concurrently participating in another clinical research trial; and 9) other abnormalities that, in the judgment of the investigator, do not qualify for the trial.
Sample size
Patients were stratified into four rehabilitation setting groups with weights of 25%, 25%, 25%, and 25%. Patients were clustered by wards, after which the clusters were randomized into experimental and control. Note that each cluster was allocated to either the experimental or control and that the number of experimental and control clusters was balanced within each stratum. Pre-experimental results showed that the probability of treatment success after receiving the intervention was 0.82 and 0.66 for the experimental and control groups, respectively. The intracluster correlation coefficient (ICC) and the odds ratio are set to 0.1 and 1.9, respectively. The significance level is set to 0.05 (two-sided), and the power is set to 0.8. Based on these conditions, the Cochran-Mantel-Haenszel test module in PASS version 21.0.3 (NCSS LLC, Kaysville, UT, USA) was used to calculate a sample size of 414, which was obtained from 136 clusters. Assuming a drop-out rate of 20% [22], the final sample size was 518 patients.
Randomization and masking
Stratified cluster randomization was used to stratify the overall sample according to different rehabilitation settings (hospital, community, home, and nursing home). Two clinics in each rehabilitation setting participated in recruiting patients, and multiple separate clusters from each clinic participated in this study. Furthermore, the clusters within each clinic were randomized by a statistician of the leader unit using a computer-generated randomization table with a 1 : 1 ratio.
The leader unit communicated the group assignment information to one randomly assigned researcher at each clinic via an encrypted folder. The study was confidential to patients and their caregivers, and we asked them not to discuss the intervention during the trial. This study also enforced confidentiality for recruiters, assessors, data collectors, and statistical analysts.
Intervention
All patients received comprehensive management of PSCI, including health education, routine care, and health management for PSCI. The management plan was set at 30 minutes per day, 5 days per week, for 12 weeks.
Based on comprehensive management, patients in the experimental group also received MICT intervention, administered for 30 minutes per day, 5 days per week, over 12 weeks. MICT intervention utilized the Mobile Intelligent Cognitive Training Application (modified version) developed by Hangzhou Ultimate Medical Technology Co., Ltd. (available at http://service.jizhiyiliao.com/), which was chosen as the intervention method because of its portability, intelligence, and self-adaptability. It is a downloadable, computerized cognitive training tool for portable use on an iPad, specifically tailored for patient cognitive therapy. It includes six rehabilitation modules: memory, attention, execution, calculation, thinking, and perception, with different difficulty levels set for cognitive training tasks in each module. Based on the principle of individualization, the patient’s cognitive impairment domains were first determined according to the results of the patient’s cognitive function assessment. Then, the appropriate cognitive training tasks were selected by the treatment personnel. The training time for each task was determined according to the patient’s cognitive function level. During the training process, the application automatically adjusted the task difficulty level from easy to difficult according to the patient’s training situation to ensure the rationality and feasibility of the training plan. A complete list of MICT cognitive tasks is described in Table 1 and excerpted Figures are shown in Supplementary Figures 1–7.
Complete list of cognitive domains and associated MICT tasks
Uniformly trained rehabilitation therapists, community therapists, social workers, and rehabilitation nurses guided patients to conduct cognitive training in hospitals, community health service centers, patients’ homes, and nursing homes. The researchers were able to understand and supervise the patients’ training anytime and anywhere through the application’s network platform.
Outcomes measurements
Each patient was assessed neuropsychologically by the same blinded, trained assessor at each clinic before the treatment, at weeks 6 and 12 post-treatment, and the 16-week follow-up (T0, T1, T2, and T3, respectively), including assessments of cognitive function, ADL ability, and QOL.
Cognitive function assessment
Montreal Cognitive Assessment (MoCA), as the primary outcome measure, is an assessment tool for rapid screening of mild cognitive impairment [23]. The cognition assessed includes seven domains of visuospatial and executive function, naming, memory, attention, language, abstraction, and delayed recall, with a total score of 30. The higher the score, the better the cognitive function.
Mini-Mental State Examination (MMSE) is a commonly used neuropsychological test to assess cognitive decline, and it consists of 11 items covering 5 domains: orientation, memory, attention and calculation, recall, and language abilities [24]. The total score is 30, with higher scores indicating better cognitive function. Prospective and Retrospective Memory Questionnaire (PRMQ) is a questionnaire tool used to assess patients’ prospective and retrospective memory performance in the short and long term [25]. This questionnaire contains 16 items with a total score of 64, with lower scores indicating stronger memory ability.
ADL assessment
Modified Barthel Index (MBI) is a tool to assess patients’ ADL ability, including 10 items: eating, bathing, grooming, dressing, bowel control, bladder control, toileting, transferring, walking, and movement up and down stairs [26]. The total score is 100; higher scores indicate better daily living ability.
Functional Activities Questionnaire (FAQ) is a tool used to assess the self-care ability of older adults, covering basic life skills (e.g., dressing, eating, and hygiene), household activities (e.g., shopping, cooking, and cleaning), and more advanced cognitive tasks (e.g., managing money, using the telephone, and planning trips) [27]. The total score is 30, with lower scores indicating greater self-careability.
QOL assessment
Quality of Life Index (QLI) is an indicator used to assess the QOL of an individual or community in 5 domains: activities, daily living, health, support, and outlook [28]. The total score is 10, with higher scores indicating a better QOL.
Statistical analysis
All data in this study were analyzed using modified intention-to-treat analysis (mITT), in which statistical analyses were conducted after excluding the following from all patients who underwent randomization: (1) no intervention was received after randomization, and (2) ineligible for enrollment after randomization. Missing values were input by last-observation-carried-forward (LOCF).
All analyses were performed using IBM SPSS statistics 26.0 (IBM Corp. Armonk, NY, USA) and R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria) software. All statistical tests were two-tailed with a significance level of 5%, and p < 0.05 was considered statistically significant.
Baseline balance analysis
Descriptive analysis was conducted to present patients’ demographics, clinical characteristics, and baseline scores, and these data were compared between the experimental and control groups in each rehabilitation setting. Normally distributed continuous variables were presented as mean and standard deviation (SD). In contrast, skewed distributed, continuous variables were presented as the median and interquartile range (IQR). The comparisons between the two groups were conducted using Student’s t-tests or Wilcoxon rank-sum tests, respectively. Furthermore, categorical variables were presented as frequencies and percentages, and between-group comparisons were performed using chi-square or Fisher’s exact tests.
Clinical efficacy analysis
This study used Linear Mixed Effects Models to analyze the efficacy of the intervention. The model consisted of fixed and random effects, and the Akaike Information Criteria (AIC) and Bayesian Information Criteria (BIC) were applied to select variables and models. Finally, the variables included in the fixed effects were rehabilitation setting (0 = hospital, 1 = community, 2 = home, 3 = nursing home), group (0 = intervention group, 1 = control group), time (0 = baseline, 1 = week 6 post-treatment, 2 = week 12 post-treatment, 3 = 16-week follow-up), first-order interaction terms for them (group * time, group * environment, time * environment), second-order interaction terms for them (group * time * environment), and confounders (age, gender, handedness, education, stroke duration, stroke type, stroke location, hypertension, dyslipidemia, diabetes); the variables included in the random effects were subjects. Multiple comparisons of post hoc analysis were performed using the package (“emmeans”), and the p-value after Tukey correction was used to determine whether there was statistical significance in the efficacy.
RESULTS
Study population
According to modified intention-to-treat analysis (mITT) principles, 452 PSCI patients were included in this study for data analysis. Among them, 117 PSCI patients were assigned to the hospital setting, of whom 2 withdrew due to infection with COVID-19, 1 dropped out due to discharge, and 1 withdrew due to disease change unrelated to this study; 121 PSCI patients were assigned to the community setting, of whom 1 withdrew due to disinterest in this study, and 2 dropped out due to refusal to participate in follow-up assessment; 112 PSCI patients were assigned to the home setting, of whom 1 dropped out due to moving, and 1 dropped out due to refusal to participate in follow-up assessment; 102 PSCI patients were assigned to the nursing home setting, of whom 3 withdrew due to disinterest in this study, 1 withdrew due to disease change unrelated to this study, and 1 dropped out due to refusal to participate in follow-up assessment.
This study conducted a descriptive analysis of the demographic, clinical characteristics, and baseline scores of 452 patients with PSCI (Table 2). The results showed no statistical difference in the above aspects between the two groups in each rehabilitation scenario (p > 0.05).
Demographics, clinical characteristics, and baseline scores of patients
Data are presented as mean±standard deviation, or number (%), or median (interquartile range). MICT, mobile intelligent cognitive therapy; MoCA, Montreal Cognitive Assessment; MMSE, Mini-Mental State Examination; PRMQ, Prospective and Retrospective Memory Questionnaire; MBI, Modified Barthel Index; FAQ, Functional Activities Questionnaire; QLI, Quality of Life Index. a Since Handness is a constant, no statistics are calculated.
Primary efficacy outcome
The results from Linear Mixed Effects Models showed that for each outcome index, the first-order interaction between group and time and the second-order interaction between group, time, and rehabilitation setting were statistically significant (p < 0.05). This indicates that MICT intervention in PSCI patients was effective, and the rehabilitation setting affected the efficacy.
At baseline, there was no significant difference in MoCA scores between the two groups in each rehabilitation setting (p > 0.05). The MoCA scores in the experimental group were significantly higher than those of the control group at week 12 post-treatment and the 16-week follow-up for each rehabilitation setting (p < 0.05). Notably, the MoCA scores of the patients in the experimental group were significantly higher than those of the control group at week 6 post-treatment in the home and nursing home settings (p < 0.05) (Fig. 2).
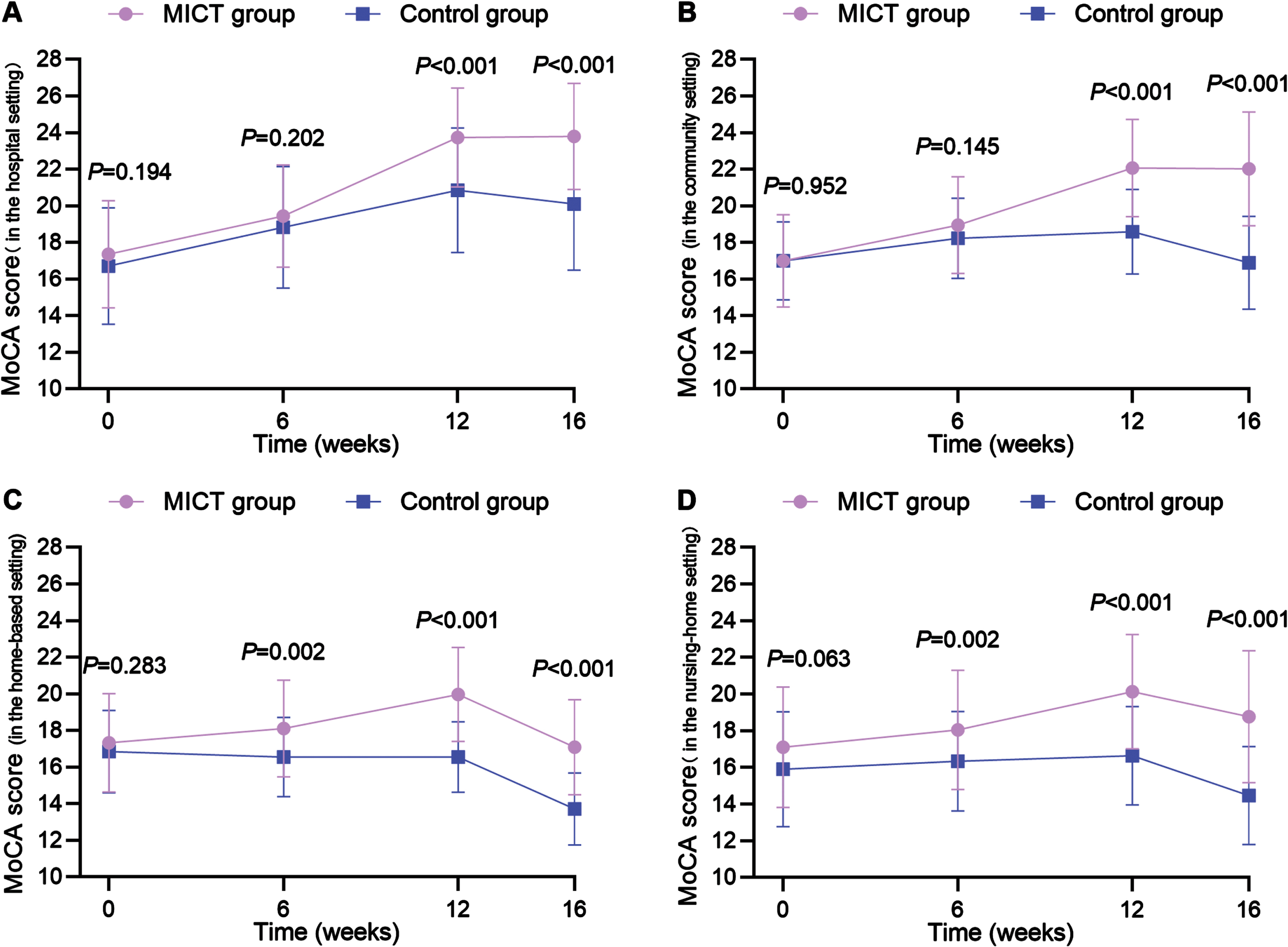
Statistical differences in MoCA scores in Intergroup and Intagroup at baseline, week 6 and week 12 post-intervention, and 16-week follow-up (mITT analysis). p-values are from a linear mixed effects model after adjusting for confounders. (A) in the hospital setting, (B) in the community setting, (C) in the home setting, and (D) in the nursing home setting.
Intra-group comparisons revealed that both the experimental and control groups in the hospital setting, as well as the experimental group in the community and nursing home settings, showed a significant increase in MoCA scores compared to baseline (p < 0.05) at each assessment (T1, T2, and T3, respectively) (Supplementary Table 1).
Based on the statistically significant second-order interaction, we performed multiple comparisons of MoCA scores among the experimental groups in the four rehabilitation settings. No significant differences in MoCA scores were noted at baseline among the four experimental groups (p > 0.05). The MoCA scores at week 6 post-treatment were hospital > community>nursing home > home, only with a statistical difference between hospital and home settings (19.44±2.79 versus 18.11±2.64, p = 0.021). At week 12 post-treatment, MoCa scores were hospital > community>nursing home > home, only with no statistical difference between nursing home and home settings (20.13±3.12 versus 19.96±2.57, p = 0.884). At the 16-week follow-up, scores were hospital > community>nursing home > home, with all having statistically significant differences (p < 0.05) (Supplementary Table 2).
Secondary efficacy outcome
MMSE
At baseline, there was no significant difference in MMSE scores between the two groups in each rehabilitation setting (p > 0.05). There was a significant difference in MMSE scores between the two groups at week 12 post-treatment and the 16-week follow-up for each rehabilitation setting (p < 0.05). Likewise, significant differences were observed at week 6 post-treatment in the home and nursing home settings (p < 0.05) (Fig. 3). Intra-group comparisons revealed that both the experimental and control groups in the hospital setting, as well as the experimental group in the community and nursing home settings, showed a significant increase in MMSE scores compared to baseline at each assessment (p < 0.05) (Supplementary Table 1). Additionally, there was no significant difference in MMSE scores among the experimental groups in the four rehabilitation settings at baseline (p > 0.05). MMSE scores at week 12 post-treatment were hospital > community>nursing home > home, only with a statistical difference between hospital and home settings (26.00±2.34 versus 24.30±2.74, p = 0.006). Furthermore, at 16-week follow-up, the scores were hospital > community>nursing home > home, only with no statistical difference between hospital and community settings (26.35±2.10 versus 25.12±2.33, p = 0.052) (Supplementary Table 2).

Statistical differences in MMSE scores in Intergroup and Intagroup at baseline, week 6 and week 12 post-intervention, and 16-week follow-up (mITT analysis). P-values are from a linear mixed effects model after adjusting for confounders. (A) in the hospital setting, (B) in the community setting, (C) in the home setting, and (D) in the nursing home setting.
PRMQ
At baseline, there was no significant difference in PRMQ scores between the two groups in each rehabilitation setting (p > 0.05). However, there was a significant difference in PRMQ scores between the two groups at week 12 post-treatment and the 16-week follow-up for each rehabilitation setting (p < 0.05) (Fig. 4). Intra-group comparisons revealed that both the experimental and control groups in the hospital and community settings, as well as the experimental group in the home and nursing home settings, demonstrated a reduction in PRMQ scores compared to baseline at each assessment (p < 0.05) (Supplementary Table 1). Additionally, there was no significant difference in PRMQ scores among the experimental groups in the four rehabilitation settings at baseline (p > 0.05). PRMQ scores at 16-week follow-up were hospital < community<nursing home < home, with significant differences for hospitals or communities, respectively, compared to nursing home or home settings (p < 0.05) (Supplementary Table 2).
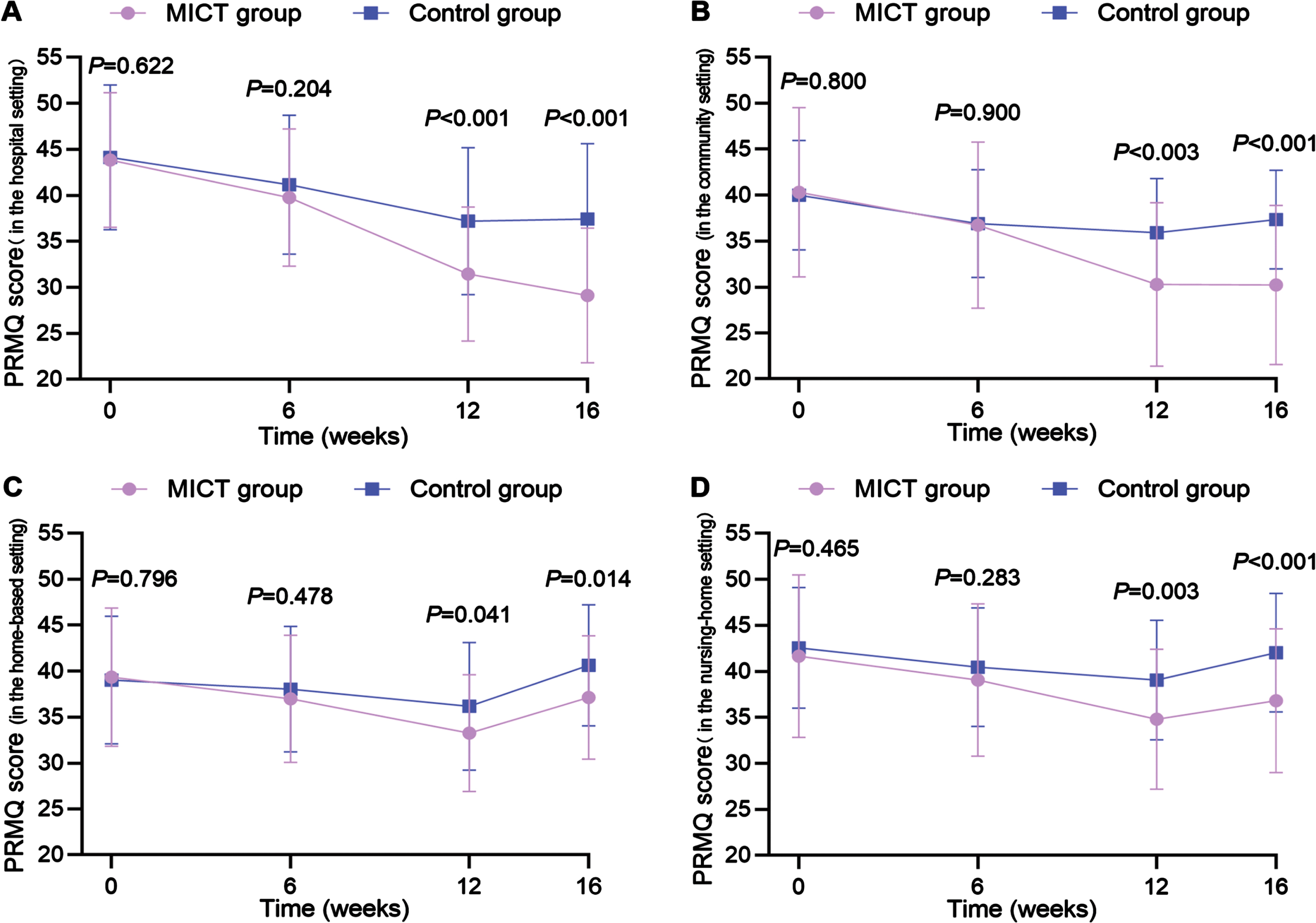
Statistical differences in PRMQ scores in Intergroup and Intagroupat baseline, week 6 and week 12 post-intervention, and 16-week follow-up (mITT analysis). p-values are from a linear mixed effects model after adjusting for confounders. (A) in the hospital setting, (B) in the community setting, (C) in the home setting, and (D) in the nursing home setting.
MBI
At baseline, there was no significant difference in MBI scores between the two groups in each rehabilitation setting (p > 0.05). There was a significant difference in MBI scores between the two groups at week 12 post-treatment and the 16-week follow-up for each rehabilitation setting (p < 0.05). Additionally, significant differences were noted at week 6 post-treatment in the hospital and nursing home settings (p < 0.05) (Fig. 5). Intra-group comparisons revealed that both the experimental and control groups in the hospital and community settings, as well as the experimental group in the home and nursing home settings, showed a significant increase in MBI scores compared to baseline at each assessment (p < 0.05) (Supplementary Table 1). Moreover, there was no significant difference in MBI scores among the experimental groups in the four rehabilitation settings at baseline (p > 0.05). MBI scores at week 12 post-treatment and the 16-week follow-up both showed hospital > community>nursing home > home. Furthermore, both groups showed statistical differences for hospitals or communities, respectively, compared to nursing home or home settings (p < 0.05) (Supplementary Table 2).
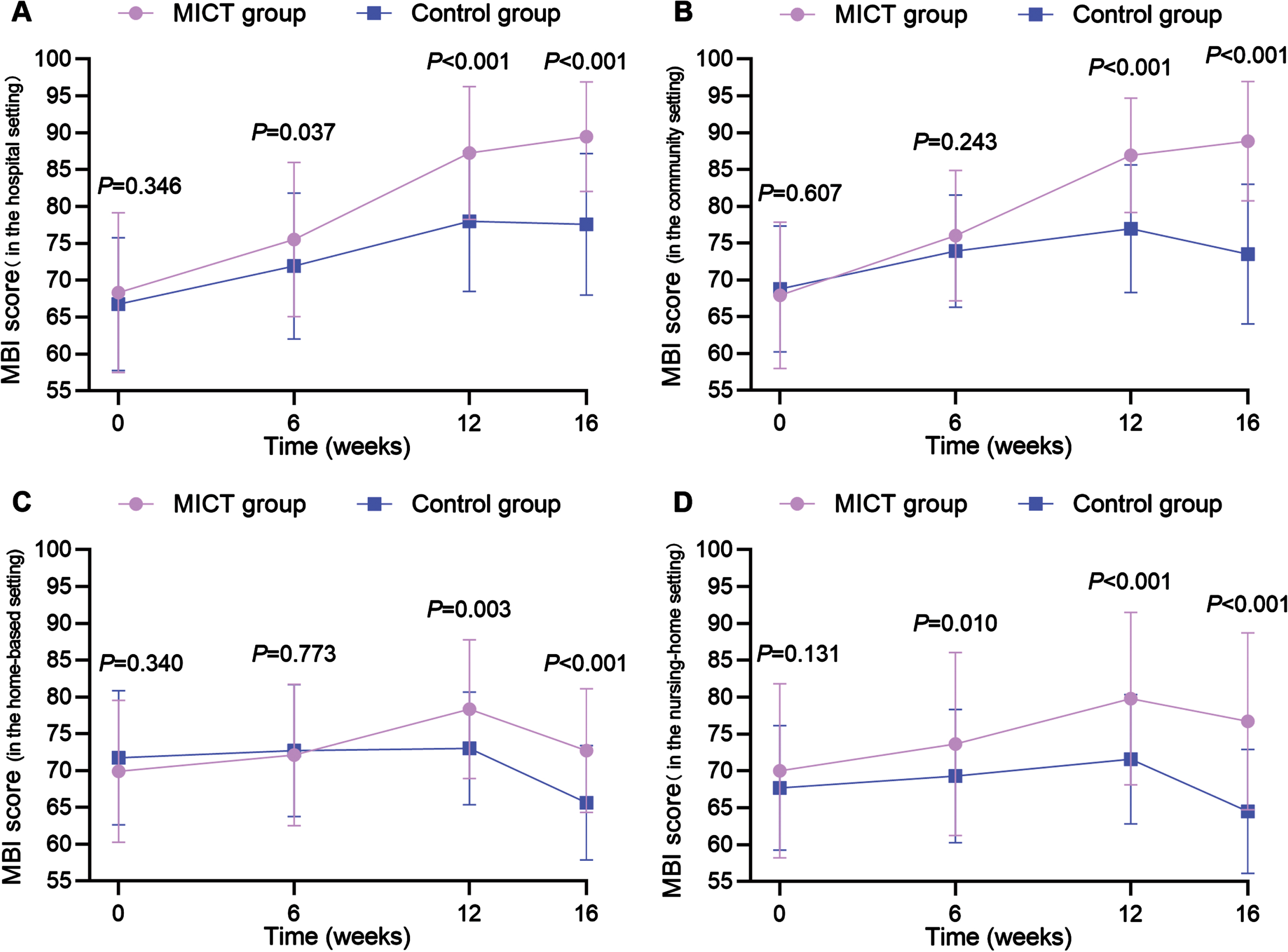
Statistical differences in MBI scores in Intergroup and Intagroup at baseline, week 6 and week 12 post-intervention, and 16-week follow-up (mITT analysis). p-values are from a linear mixed effects model after adjusting for confounders. (A) in the hospital setting, (B) in the community setting, (C) in the home setting, and (D) in the nursing home setting.
FAQ
At baseline, there was no significant difference in FAQ scores between the two groups in each rehabilitation setting (p > 0.05). There was a significant difference in FAQ scores between the two groups at week 12 post-treatment and the 16-week follow-up for each rehabilitation setting (p < 0.05). Likewise, significant differences were noted at week 6 post-treatment in the hospital setting (p < 0.05) (Fig. 6). Intra-group comparisons showed that the FAQ scores in the experimental group for each rehabilitation setting improved compared to baseline at each assessment (p < 0.05) (Supplementary Table 1). Additionally, there was no significant difference in the FAQ scores among the experimental groups in the four rehabilitation settings at baseline (p > 0.05). The FAQ scores at week 12 post-treatment and the 16-week follow-up both showed hospitals < community<nursing home < home, both also with no statistical difference between nursing home and home settings (p > 0.05) (Supplementary Table 2).
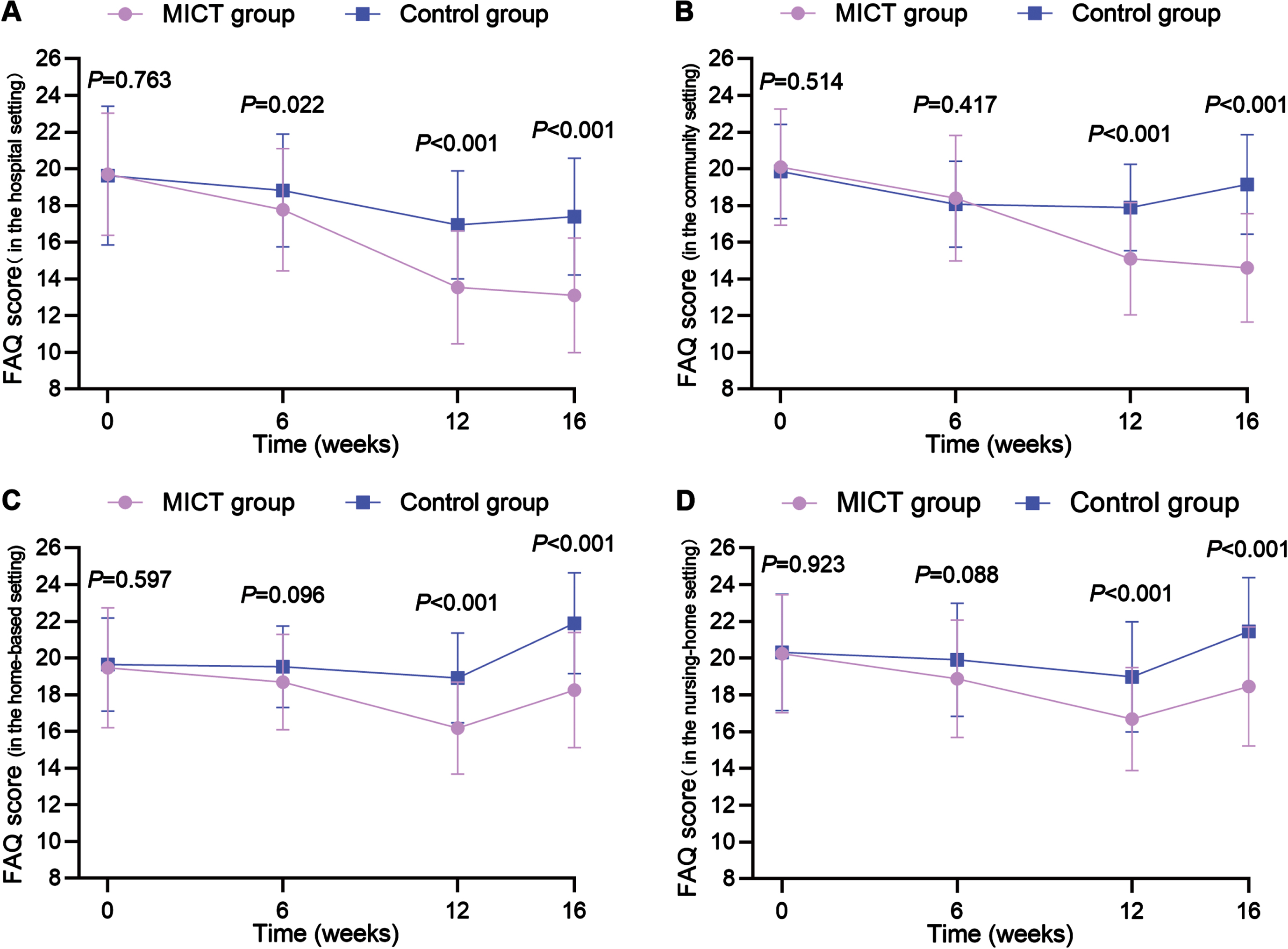
Statistical differences in FAQ scores in Intergroup and Intagroupat baseline, week 6 and week 12 post-intervention, and 16-week follow-up (mITT analysis). p-values are from a linear mixed effects model after adjusting for confounders. (A) in the hospital setting, (B) in the community setting, (C) in the home setting, and (D) in the nursing home setting.
QOL
At baseline, there was no significant difference in QOL scores between the two groups in each rehabilitation setting (p > 0.05). There was a significant difference in QOL scores between the two groups at week 12 post-treatment and the 16-week follow-up for each rehabilitation setting (p < 0.05). Likewise, significant differences were noted at week 6 post-treatment in the hospital and home settings (p < 0.05) (Fig. 7). Intra-group comparisons revealed that both the experimental and control groups in the hospital setting, as well as the experimental group in the community and nursing home settings, showed a significant increase in QOL scores compared to baseline at each assessment (p < 0.05) (Supplementary Table 1). Additionally, there was no significant difference in QOL scores among the experimental groups in the four rehabilitation settings at baseline (p > 0.05). Moreover, the QOL scores at week 6 post-treatment were hospital > community>nursing home > home, only with the statistical difference between hospital and community or home, respectively (p < 0.05). At week 12 post-treatment and the 16-week follow-up, both groups showed hospital > community>nursing home > home, where both groups showed no statistical difference between nursing home and home settings (p > 0.05) (Supplementary Table 2).
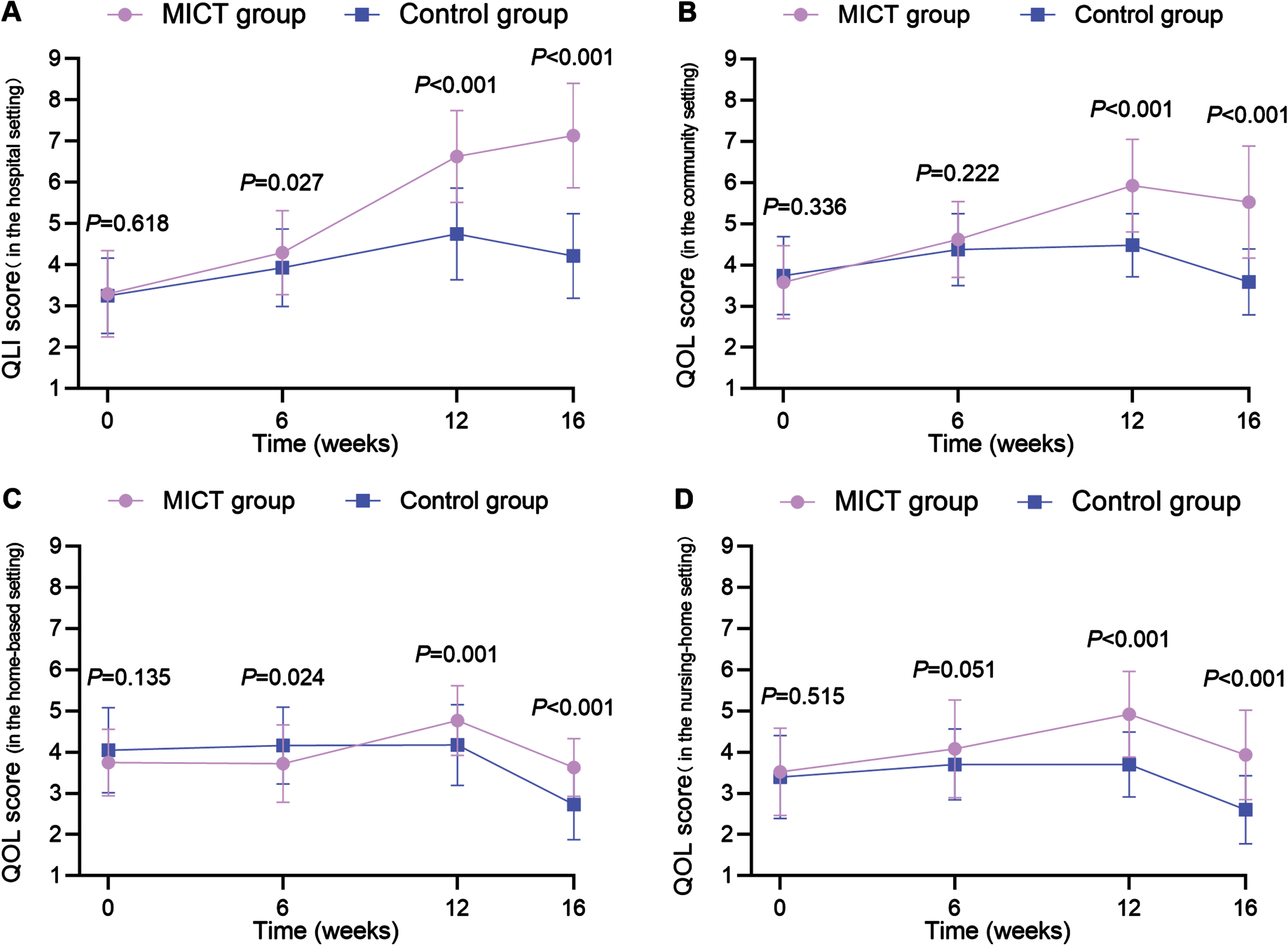
Statistical differences in QOL scores in Intergroup and Intagroup at baseline, week 6 and week 12 post-intervention, and 16-week follow-up (mITT analysis). p-values are from a linear mixed effects model after adjusting for confounders. (A) in the hospital setting, (B) in the community setting, (C) in the home setting, and (D) in the nursing home setting.
DISCUSSION
Cognition is one of the advanced functions of the brain, and brain tissue damage following a stroke is prone to cause cognitive impairment in patients [29]. With the development of cognitive neuroscience, neuroimaging, computer technology, and VR technology, MICT has become a development trend for cognitive rehabilitation training of PSCI patients [30, 31]. This 12-week, multicenter, cluster-randomized controlled study explored the short- and long-term effects of MICT on PSCI. The results demonstrated that compared to the control group, 6-week MICT did not significantly improve the cognitive function of PSCI patients. However, 12-week MICT improved the cognitive function, ADL ability, and QOL of PSCI patients and lasted for at least one month.
Compared with this study, Wentink et al. [32] conducted an RCT to investigate the effects of an 8-week computer-assisted cognitive rehabilitation (CACR) program (Lumosity Inc.®) on stroke patients, in which the experimental group received an 8-week brain cognitive training program, while the control group also received only comprehensive management of stroke disease. Consistent with our 6-week MICT intervention results, the 8-week brain cognitive training had no significant effect on cognitive function, QOL, and self-efficacy in stroke patients. Considering the possible reasons, this is likely related to the time effect hypothesis [33]. As a desirable cognitive rehabilitation model, MICT also relies on functional neuroplasticity [10] and specific learning strategies [11], affecting the functional recovery of PSCI patients through repeated stimulation of multisensory cognitive tasks over a set period. Another study has shown that the brain follows the law of competition internally and that the plasticity of neural networks often requires a sufficient number of repeated stimuli [34]. Brain cognitive learning is using internal language to repeat learning materials or stimuli in the brain, integrating the intrinsic relationship between old and new knowledge to enhance and maintain cognitive learning [35]. In a study by Withiel et al. [36], the use of cognitive learning strategies increased significantly over time. This suggests that the therapeutic effect of MICT may have a “time-accumulation effect”, and short-term MICT intervention is not sufficient to improve the dysfunction of PSCI patients.
In the 12-week RCT conducted by van de Ven et al. [37], stroke patients were randomly divided into intervention, active, and waiting-list control groups. From this study, the intervention group received computerized cognitive training, the active control group received mocking training, and the waiting control group received no additional treatment. As such, changes in cognitive function were compared among the three groups before and after treatment. Consistent with our 12-week MICT intervention results, patients in the intervention group significantly improved their performance on the cognitive training task and still improved 4 weeks after the end of training. Different from the study by Milman et al. [38], which utilized a 12-week computered cognitive training on 18 patients with Parkinson’s disease and demonstrated that the patients’ global cognitive function and mobility improved significantly, with still a certain sustained effect 4 weeks after training. However, both trials also suggested that these study results and the exact mechanism of cognitive impairment improvement still need further verification due to various factors, such as the small sample size.
One study has also suggested that computerized cognitive training may be involved in modulating brain regions associated with cognitive function [39]. For example, the medial prefrontal lobe is engaged in integrating sensory-perceptual and extracting situational memory [40], the dorsolateral prefrontal lobe is involved in processing working memory, cognitive control, and execution [41], and the medial temporal lobe is involved in encoding memories, processing visuospatial information, and cognitive flexibility [42, 43]. Furthermore, the execution of cognitive functions acts as a brain network and is not limited to a single brain region [44]. The function of the brain region is a network-like structure in which the default mode network (DMN) and dorsal attention network (DAN) are closely related to cognitive functions [45]. Animal experiments have also demonstrated that rich environmental stimuli can thicken the cerebral cortex of mice [46], and the effects on PSCI patients are similar. In post-stroke rehabilitation, MICT intervention has multiple potential benefits of multisensory stimulation and repeatability of cognitive tasks. MICT intervention may also take advantage of these features to stimulate cognitive-related brain regions, increase the release of relevant trophic factors in vivo, and enhance functional network connectivity of the DAN, DMN, and the posterior cingulate cortex and inferior parietal cortex for which the DMN is responsible [47]. Additionally, degeneration of central cholinergic neurons is considered an important pathological factor of PSCI [48]. Based on a previous study [49], we hypothesized that the mechanism by which MICT improves cognitive impairment may be related to the regulation of acetylcholine and acetylcholinesterase content. In the neocortex and hippocampus, acetylcholinesterase can be decomposed into acetylcholine, which is not only involved in neuronal activity but also in regulating synaptic plasticity to improve cognition [50].
MICT intervention also has the advantage of adaptively adjusting the difficulty of cognitive tasks. Currently, studies have explored the efficacy of difficulty-adaptive computerized cognitive training only in hospital patients with cognitive impairment [51] and community older adults [52, 53], and there is no clear conclusion yet. However, this study was the first to apply MICT intervention in different rehabilitation settings, including the hospital, community, home, and nursing home. Furthermore, it revealed that the cognitive efficacy of MICT intervention in improving PSCI patients is affected by the rehabilitation setting, and the improvement degree of each outcome was found to be highest in hospital settings, followed by community, nursing home, and home settings. Considering the possible reasons, this study was a multicenter clinical trial, the standardization of MICT intervention, the comprehensive management of PSCI, and the cooperation of patients may be better assessed in the hospital setting despite our strict quality control. Previous studies have shown that age and stroke duration can have an impact on the rehabilitation of PSCI patients [3]. In contrast, the longest stroke duration in this study was in the nursing home, followed by home, community and hospital settings, and the age of the nursing home patients was older. Compared with interventions in other rehabilitation settings, home-based rehabilitation is susceptible to environmental interference, which can affect the quality of patient training [54]. Fortunately, the cognitive functions of the patients improved in the experimental group in each rehabilitation setting compared with the pre-treatment. This finding suggests that MICT intervention with a certain intensity and repetition can continuously stimulate the central nervous system, promoting the recovery, substitution, and compensation of damaged brain areas, significantly improving the integrity of the cerebral white matter. Furthermore, it can increase connectivity between brain cortices and induce the advanced brain networks to produce alterations in neural functional connectivity [55], improving the cognitive function of patients to a certain extent.
Additional studies have also reported transfer phenomena related to training tasks in computerized cognitive interventions [56, 57], such as MICT intervention. In this study, near transfer refers to the improvement in performance observed in similar, untrained tasks within the same cognitive domain after task training in a specific cognitive domain. Additionally, far transfer refers to improving performance on tasks in a different cognitive domain after training in a specific cognitive domain [58]. Consistent with Barnett et al. [59], patients with PSCI in this study showed correlations in changes in global cognition, memory, and ADL abilities.
This multicenter clinical trial is our a preliminary exploratory study, and it has some limitations. First, this study did not include stroke patients with severe cognitive impairment, so the findings do not apply to all patients with PSCI. Second, the outcome measurements used in this study did not involve the various cognitive domains due to the consideration of completion among all patients in different rehabilitation settings. Third, there is still a lack of standardized guidelines for clinical use and unified training prescriptions of MICT intervention at this stage. Although this study’s results indicate a statistical difference in the cognitive intervention efficacy of MICT for PSCI patients in different rehabilitation settings, the factors influencing the efficacy may be various. For example, the patient’s age, gender, education level, history of smoking and alcohol consumption, stroke location and size, stroke duration, and underlying medical condition may have a certain impact on the credibility of the results. Moreover, there is still uncertainty about the correlation between cognitive efficacy and various factors. Despite the limitations, however, it is through the conduct of this study that we have gained insight into the current status and challenges of cognitive therapy in different rehabilitation settings, and likewise provide valuable references for the future development of cognitive rehabilitation, which is precisely the significance of this study. It is also through this study that we have identified shortcomings and made corresponding modifications. In the future, we hope to further explore the clinical efficacy of the MICT intervention through a more rigorous study design, as well as a randomized controlled trial with a larger sample size, higher quality, and follow-up, to provide evidence for improving the quality of long-term survival of patients with PSCI.
In conclusion, this prospective, multicenter, cluster-randomized controlled study demonstrated that long-term MICT intervention can improve cognitive function, ADL ability, and QOL in patients with mild to moderate PSCI, with sustained effects for at least one month. Notably, different rehabilitation settings affect the cognitive intervention efficacy of MICT on PSCI patients. However, this still needs to be further determined in future studies.
AUTHOR CONTRIBUTIONS
Kaiyue Han (Conceptualization; Methodology; Writing – original draft); Guangliang Liu (clinical trials); Nan Liu (clinical trials); Jiangyi Li (clinical trials); Jianfeng Li (clinical trials); Lihua Cui (clinical trials); Ming Cheng (clinical trials); Junzi Long (data analysis); Xingxing Liao (graph preparation); Zhiqing Tang (Data curation); Ying Liu (Data curation); Jiajie Liu (Data curation); Jiarou Chen (data analysis)l Haitao Lu (data analysis)l Hao Zhang (Conceptualization; Methodology; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We are very grateful to the Capitals Funds for Health Improvement and Research for supporting this study. And we thank all researchers and participants for their contributions to this multicenter clinical trial.
FUNDING
This research was funded by the Capitals Funds for Health Improvement and Research (grant number: 2020-1-6011).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on reasonable requests from the corresponding or first author.