
Abstract
Background:
The interrelationship of parkinsonism, Parkinson’s disease (PD) and other Alzheimer’s disease (AD) and Alzheimer’s disease and related dementias (ADRD) pathologies is unclear.
Objective:
We examined the progression of parkinsonian signs in adults with and without parkinsonism, and their underlying brain pathologies.
Methods:
Annual parkinsonian signs were based on a modified Unified Parkinson’s Disease Rating Scale. We used linear mixed effects models to compare the progression of parkinsonian signs in 3 groups categorized based on all available clinical evaluations: Group1 (never parkinsonism or clinical PD), Group2 (ever parkinsonism, but never clinical PD), Group3 (ever clinical PD). In decedents, we examined the progression of parkinsonian signs with PD and eight other AD/ADRD pathologies.
Results:
During average follow-up of 8 years, parkinsonian signs on average increased by 7.3% SD/year (N = 3,807). The progression of parkinsonian signs was slowest in Group1 (never parkinsonism or clinical PD), intermediate in Group2, and fastest in Group3. In decedents (n = 1,717) pathologic PD and cerebrovascular (CVD) pathologies were associated with a faster rate of progressive parkinsonian signs (all p values <0.05). However, pathologic PD was rare in adults without clinical PD (Group1, 5%; Group2, 7% versus Group3, 55%). Yet, 70% of adults in Group2 without pathologic PD showed one or more CVD pathologies. In Group2, adults with pathologic PD showed faster progression of parkinsonian signs compared with those without evidence of pathologic PD and their rate of progression was indistinguishable from adults with clinical PD.
Conclusions:
Parkinsonism in old age is more commonly related to cerebrovascular pathologies relative to pathologic PD and only a minority manifest prodromal PD.
INTRODUCTION
Over the past decade, there has been increased recognition that mixed brain pathologies underlying Alzheimer’s disease and related dementias (ADRD) cause not only impaired cognition but also non-cognitive impairments such as parkinsonism. 1 While parkinsonian signs are common in older adults, many but not all older adults may have parkinsonism and even a smaller number have a clinical diagnosis of Parkinson’s disease (PD).2,3, 2,3 PD is a synucleinopathy caused by PD pathology. There is increasing recognition that like pathologic Alzheimer’s disease (AD), pathologic PD develops over many years and during its earliest stages there may be none (preclinical) or mild (prodromal) signs of parkinsonism insufficient for a clinical diagnosis of PD.4 –6
Parkinsonism in older adults is not synonymous with PD but is a heterogeneous syndrome that can be caused by varied medications, medical conditions and diverse brain pathologies including PD, cerebrovascular (CVD), or AD pathology while PD is a synucleinopathy caused by PD pathology. How likely is an older adult with parkinsonism in the community to have preclinical or prodromal PD? On the one hand, clinical PD is uncommon in the general population reported to occur in 3%–5% of adults by age 85.7,8, 7,8 In contrast, investigations of parkinsonian signs in community-dwelling older adults without a clinical diagnosis of PD have reported that up to 50% of older adults may develop parkinsonism by the age of 85 years.2,3, 2,3 However, the pathologic basis for a potential ten-fold difference in the frequency of parkinsonism in community-dwelling older adults with and without clinical PD is unclear.
Previously we reported that a) parkinsonism in older adults is very common and may occur in more than 50% of older adults by age 85, b) parkinsonism is related to postmortem PD pathology, and c) that the progression of parkinsonian signs is related to the burden of mixed-brain pathologies.9 –13 The current study seeks to extend our prior work.14,15, 14,15 First, few studies have compared the progression of parkinsonian signs in older adults with parkinsonism with and without a clinical diagnosis of PD. Second, we develop and provide empiric support for the binary postmortem marker of pathologic PD used in this study. Third, this study examines to what extent progression of parkinsonian signs in older adults with parkinsonism, who never have a clinical diagnosis of PD, varies with and without the presence of pathologic PD. These data have potential to advance the nosology of parkinsonism and PD in older adults and their relationships with other AD/ADRD pathologies and inform on efforts to develop biologic definitions for PD and identify biomarkers.16 –18
METHODS
Study participants
Participants are from one of three ongoing cohort studies of aging and dementia. All three studies employ common ante- and postmortem data collection, allowing combined analyses of data.14,15, 14,15 These studies were approved by the Institutional Review Board of Rush University Medical Center. Written informed consent was obtained from all study participants as was an Anatomical Gift Act for organ donation.
At the time of these analyses, 3,807 participants with valid baseline and one or more assessments of parkinsonism were available for these analyses [Memory and Aging Project (MAP), N = 1,906; Religious Order Study (ROS), N = 1,290, Minority and Aging Research Study (MARS), N = 611].
Assessment of parkinsonism and diagnosis of Parkinson’s disease
Trained nurse clinicians assessed four parkinsonian signs (parkinsonian gait, rigidity, bradykinesia, and tremor) annually using 26 items from a modified Unified Parkinson’s Disease Rating Scale. These assessments have high inter-rater reliability and short-term stability among nurses and compared to a movement disorders physician.11,19, 11,19 In prior work, we found that parkinsonian signs assessed with the UPDRS is also related to other non-motor features including cognition (mild cognitive impairment (MCI) and AD dementia), disability and mortality. 11
Global parkinsonian score: A continuous measure of parkinsonian signs was used to examine the rate of change in parkinsonian signs during follow-up. A score for each of the four parkinsonian signs was based on the sum of the scores for each of its individual items assessed, e.g., 8 items for bradykinesia. The scores for the 4 parkinsonian signs were averaged to provide a continuous global parkinsonian score as previously described. 19 The distribution of global parkinsonian score was positively skewed and was square root transformed prior to ouranalyses.
Parkinsonism category: We constructed a categorical research measure for parkinsonism based on the number of four parkinsonian signs that were present. A parkinsonian sign was present if two or more of its’ items were scored as a mildly abnormal. Parkinsonism was present if at least two of the four parkinsonian signs were present as previously described. 11
Clinical diagnosis of PD: A clinical diagnosis of PD was based on medical history and review of annual medications as previously reported. 10
Demographic covariates
Date of birth and sex were collected through a participant interview. Age in years was computed from self-reported date of birth and date of death.
Neuropathology assessment
Brain removal, tissue sectioning and preservation, and a uniform gross and microscopic examination following a standard protocol with quantification of two post-mortem indices for determining the presence of PD pathology and indices of eight other AD/ADRD pathologies.
Nigral neuronal loss was assessed in the substantia nigra in a hemisection of the mid to rostral midbrain near or at the exit of the 3rd nerve in hematoxylin and eosin stained 6um sections using a semi-quantitative scale (0–3).
Lewy body pathology: Seven regions (substantia nigra, anterior cingulate cortex, entorhinal cortex, midfrontal cortex, superior or middle temporal cortex, inferior parietal cortex and amygdala) were assessed for Lewy bodies using a monoclonal phosphorylated antibody to a-synuclein (1:20,000; Wako Chemical USA Inc., Richmond, VA) Lewy bodies were treated as present or absent in these analyses.
Construction of the PD pathology measure
PD is a synucleinopathy and its pathology is characterized by two components, the loss of nigral dopaminergic neurons and the accumulation of insoluble α-synuclein, Lewy bodies in surviving neurons. Some reports have suggested that nigral neuronal loss links Lewy body pathology with cellular neurodegeneration.20,21, 20,21 We reviewed the distribution of Lewy bodies and nigral neuronal loss in decedents and compared the associations of several groupings of these elements with progression of parkinsonian signs to determine the strongest marker of pathologic PD.
Figure 1 shows the distribution of Lewy bodies and nigral neuronal loss in decedents: a) pathologic PD based on the presence of Lewy bodies as well as moderate or severe nigral neuronal loss as previously published (n = 138, 8%), b) possible pathologic PD was based on the presence of Lewy bodies and mild nigral neuronal loss (n = 185,11%), c) only Lewy bodies were present (n = 138, 8%), and d) a reference group without any elements of pathologic PD (n = 1256, 73%). A small group of (n = 44) of decedents showed only moderate-severe nigral neuronal loss and were not included in any of thegroups.

PD pathology is associated with a faster rate of progressive parkinsonian signs. A) Frequency of one or both elements of PD pathology [Lewy bodies and nigral neuronal loss (NNL)] Elements of PD pathology (X-axis) and Number of decedents (Y-axis). Lewy bodies were present or absent and nigral neuronal loss was rated with a semiquantitative scale [none (0), mild (1), moderate (2), severe (3)]. B) We created four groups of PD pathology based on these combinations: a) No elements of pathologic PD, b) Lewy bodies alone were present, c) Possible pathologic PD if there were Lewy bodies and mild NNL, and d) Pathologic PD based on the presence of both Lewy bodies and moderate or severe NNL. C) The average trajectory for the annual rate of change of parkinsonian signs and the 95% confidence interval (grey area) is shown for each of the four PD pathology groups. Pathologic PD showed a consistently faster rate of progression compared to the three other pathology groups that were not well-differentiated from one another as shown in the 1C.
Other AD/ADRD pathologies collected
Eight other indices of AD/ADRD pathologies were collected at autopsy including Alzheimer’s disease neuropathologic changes (ADNC), limbic predominant-age-related TDP-43 encephalopathy neuropathologic change (LATE-NC), hippocampal sclerosis and five indices of cerebrovascular disease pathologies including macro-and micro-infarcts, atherosclerosis, arteriolosclerosis and cerebral amyloid angiopathy. Additional details are included in prior publications and summarized in the Supplementary Methods. 22 Postmortem interval was 9.8 (SD = 9.66) hours after death.
Statistical methods
While the participants showed some parkinsonian signs during the study, in many the severity was never sufficient to meet our research criterion of parkinsonism and they also never received a clinical diagnosis of PD (Methods). We reviewed all baseline and follow-up assessments of our parkinsonism research criteria and clinical diagnosis of PD during an average of 7.8 years (mean 7.77, SD = 5.57) to categorize all participants into one of three groups. Group1 included adults who never had parkinsonism or a clinical diagnosis of PD (1439, 38%). Group2 included individuals categorized as ever having parkinsonism but who never had a clinical diagnosis of PD (n = 2287, 60%). Group3 included adults who received a clinical diagnosis of PD at baseline or during follow-up (81, 2%).
We employed a series of linear mixed effects models to examine the rate of progressive parkinsonian signs in three groups of older adults. The outcome for these models was based on repeated annual measures of parkinsonian signs summarized as the global parkinsonian scores. Each model included a term, Time, i.e., the number of years in the study, whose coefficient estimates the mean annual rate of change in parkinsonian signs (i.e., slope). Each predictor added to the model included a term for its association with baseline global parkinsonian score and a second term for its interaction with Time for its association with the annual rate of change in parkinsonian signs. All the models included terms for age and sex and their interaction with Time. In a separate model, we included a term for the three groups and its interaction with Time and examined if the rate of progression differed between groups.
One of the goals of these analyses was to examine the association of pathologic PD with parkinsonism in older adults. Pathologic PD is characterized by two components, the loss of nigral dopaminergic neurons and the accumulation of insoluble α-synuclein (Lewy bodies) in surviving neurons. So, we examined several combinations of Lewy bodies and nigral neuronal loss as markers of pathologic PD. We applied a linear mixed effects model adjusting for age and sex, comparing the progression of parkinsonian signs in adults without either of the two elements of PD pathology with three potential markers of pathologic PD: a) Lewy bodies alone, b) possible pathologic PD, or c) pathologic PD.
Next, in the 3 clinical groups who died and underwent brain autopsy, we employed linear mixed effect models similar to those described above to examine the associations of PD and eight other AD/ADRD pathologies with the rate of progression of parkinsonian signs when all the indices were included in a single model.
In further models, we stratified adults in Group2 into two groups based on the presence (2b) or absence (2a) of pathologic PD. We used models similar to those described above to compare the progression of parkinsonian signs in Group2a versus 2b and also to the rate of progression in the other two groups (Groups1, 2a, 2b, and 3).
RESULTS
Characteristics of the analytic cohort
There were 3,807 older adults included in the current analyses and their clinical characteristics are summarized in Table 1. On average, the severity of parkinsonian signs increased in the entire analytic sample (N = 3,807) 7.3% SD/year in all older adults (Estimate 0.101, S.E. 0.003, p < 0.001).
Characteristics of the analytic cohort
Each year above an age of 78 years old at baseline was associated with a 2% SD faster rate of progression per decade (Estimate 0.003, S.E. 0.0003, p < 0.001). Males showed a 1.5% SD per year faster rate of progressive parkinsonism compared to females (Estimate 0.021, S.E. 0.006, p < 0.001), equivalent to someone 7.5 years older at baseline.
Progression of parkinsonian signs in 3 clinical groups
We compared the rate of progressive parkinsonian signs between the three clinical groups. Group2 (parkinsonism never clinical PD) showed a 2.1x faster rate of progression of parkinsonian signs compared to Group1 (Supplementary Table 1, Model A). Group3 (clinical PD), showed 3.6x faster rate of progression of parkinsonian signs compared to Group1 (never parkinsonism or clinical PD) and was 1.7 faster than Group2 (Supplementary Table 1, Model B). Figure 2 illustrates that the rate of progressive parkinsonism was fastest in Group3 and slowest in Group1 and intermediate in Group2.
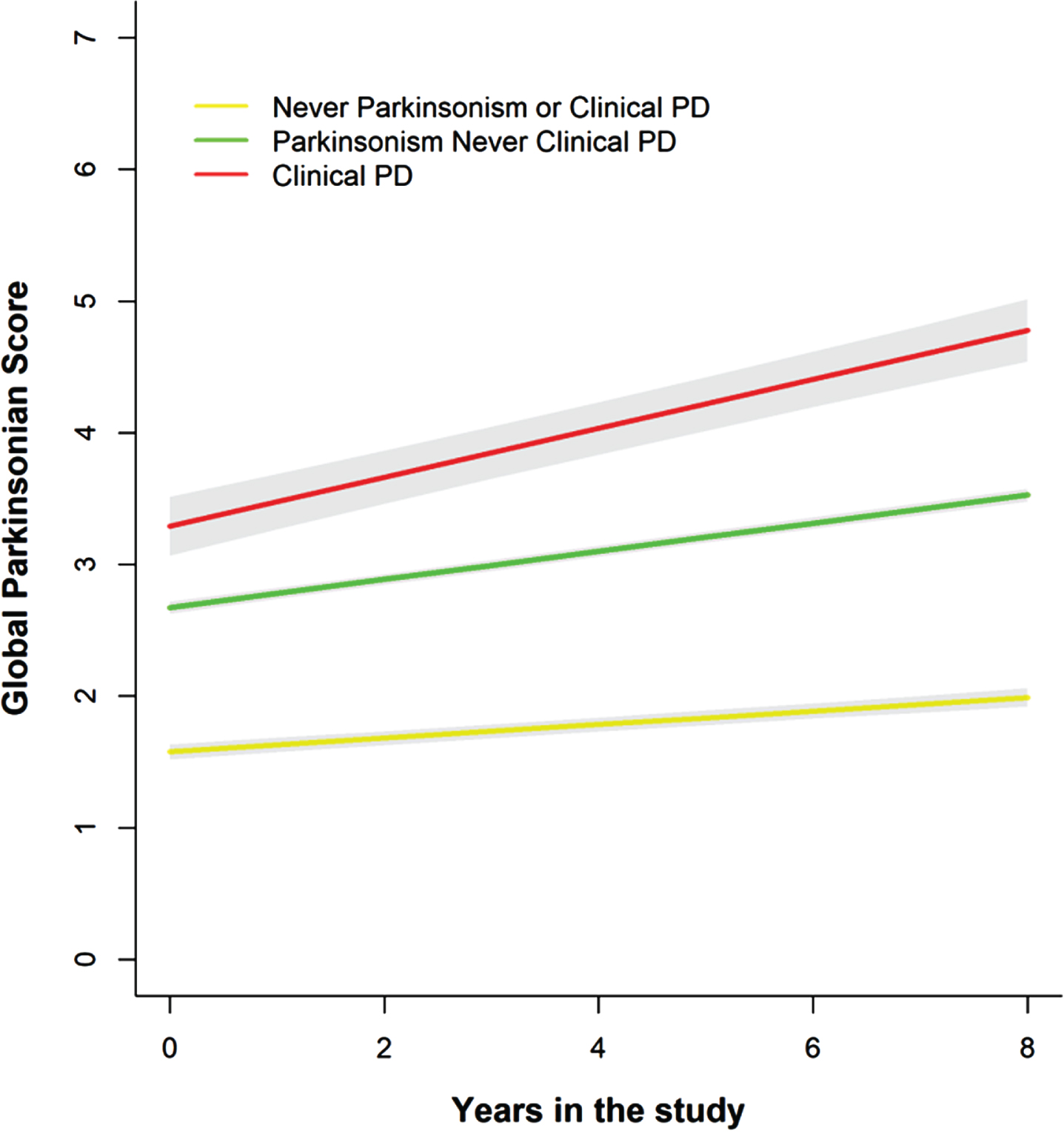
The rate of progression of parkinsonian signs in 3 clinical groups. Model derived trajectories with mean follow-up of eight years for each of the three clinical groups (X-axis) based on repeated annual measures of global parkinsonian score (Y-axis): Group1 (Never parkinsonism or clinical PD, Yellow line), Group2 (Parkinsonism and never clinical PD, Green line) and Group3 (Clinical PD, Red line) with the average trajectory of the progression of parkinsonian signs (colored line) and 95% confidence interval (grey area). The annual rate of change in the progression of parkinsonian signs is fastest in Group3 and slowest in Group1 and intermediate in Group2 (Supplementary Table 3).
Pathologic PD and progressive parkinsonian signs
A subset of 1,717 decedents underwent autopsy, and their postmortem indices are summarized in Table 1. We compared the progression of parkinsonian signs with several potential markers of pathologic PD. We applied a linear mixed effects model adjusting for age and sex, comparing the progression of parkinsonian signs in a reference group of adults without either of the two elements of PD pathology with three potential markers of pathologic PD: a) Lewy bodies alone, b) possible pathologic PD or c) pathologic PD.
Adults with pathologic PD and possible pathologic PD were associated with a faster rate of progressive parkinsonian signs when compared to the adults without any elements of pathologic PD (Supplementary Table 2, Model A). The rate of progression of parkinsonian signs in adults with Lewy bodies alone was not different than the rate of progression in adults without any elements of PD pathology (Supplementary Table 2, Model A). Figure 3 illustrates that adults with pathologic PD showed a consistently faster rate of progression of parkinsonian signs compared to adults with Lewy bodies alone or possible PD pathology or those without any elements of PD pathology (Supplementary Table 2, Model B& C).

Older adults without clinical PD rarely accumulate brain PD pathology, most accumulate CVD pathologies. A) We measured nine AD/ADRD indices of brain pathologies, yet modeling all nine pathologies together showed that only PD and one or more of four cerebrovascular disease pathologies were associated with the annual rate of change in parkinsonian signs (Table 2). The bar plot highlights the heterogeneity of the combinations of PD and CVD pathologies associated with progression of parkinsonian signs in adults without clinical PD. The bar chart in the lower left corner shows the frequency of specific pathologies related to progression of parkinsonian signs. Connected dots on the X-axis indicate the frequency of the combinations of different pathologies that was observed. The bar plot shows the frequencies of the combinations of regions in the Group1 (without parkinsonism no clinical PD, grey) and Group2 (parkinsonism no clinical PD, (blue), ordered by their frequency. The height of each bar corresponds to the number of decedents with the varied combinations of ADRD positivity. B) The second bar plot highlights that most decedents with parkinsonism with or without PD pathology accumulate one or more CVD pathologies and few show PD pathology alone. Even adults who accumulate PD pathology also accumulate one or more CVD pathologies.
PD and AD/ADRD brain pathologies and the annual rate of change of parkinsonian signs
This table shows the results of three linear mixed effects models (column) which examined the association of each pathology (left column) with the annual rate of change in parkinsonism. Each cell shows the term for the interaction of a single pathology shown in the left-hand column with the term, Time, the annual rate of progressive parkinsonism prior to death. Each cell shows the (Estimate, Standard Error, and p-value) for the interaction term shown on the left. Each of these three models also included the following 12 terms (not shown): a term for Time, cross sectional terms for each of the 9 pathologies without the interaction with Time, age, sex and their interaction with Time. Model A includes decedents from all three clinical groups (No parkinsonism, parkinsonism and clinical PD), Model B excludes decedents with a clinical diagnosis of PD and Model C excluded decedents with clinical PD and no parkinsonism. Each model also included demographic terms alone and their interaction with TBD which are not shown.
Including adults with Lewy bodies alone together with adults with Lewy bodies and mild nigral neuronal loss together as “possible pathologic PD” (Supplementary Figure 1 and Supplementary Table 3) and adding another term for “possible PD pathology” did not increase the percentage of variance of progressive parkinsonian signs accounted for compared to a model including a term for pathologic PD alone (Supplementary Tables 4 and 5). So, the marker for pathologic PD used in further analyses was based on the presence of Lewy bodies with moderate or severe nigral neuronal loss.
Distributions of brain pathologies collected in the 3 clinical groups
Most decedents with autopsy (70%) did not have either Lewy bodies or moderate-severe nigral neuronal loss (Fig. 1). Pathologic PD was common (>50%) in decedents in Group3 but rare in decedents who never had a clinical diagnosis of clinical PD (Group1, 5%; Group2, 7%).
The majority of decedents in each of the three groups showed one or more of the other AD/ADRD pathologies measured (Table 1). The heterogeneity of the combinations of varied pathologies measured in each of the three clinical groups is shown in Supplementary Figures 2 and 3. Inspection of the percentages of the other AD/ADRD pathologies collected emphasizes that mixed-pathologies accumulate in decedents from all three clinical groups (Supplementary Figure 4a).
Identifying brain pathologies associated with progressive parkinsonian signs
Prior reports suggest that pathologic PD as well as indices of other AD/ADRD pathologies may be associated with the progression of parkinsonian signs in older adults. 10 A series of linear mixed effects models showed that on average, pathologic PD and/or one or more CVD pathologies including macroinfarcts, arteriolosclerosis and atherosclerosis were associated with the rate of progressive parkinsonian signs (Table 2, Model A; Fig. 3; and Supplementary Figure 4b).
These associations were unchanged when we excluded individuals from Group3 (Table 2, Model B). In a further model we also excluded individuals from Group1 and examined only adults from Group2 and findings were similar (Table 2, Model C). So, although we measured nine different brain pathologies in all autopsied adults (Supplementary Figures 2 and 3) not all of these pathologies were associated with the progression of parkinsonian signs (Table 2 and Fig. 3a).9,23,24 , 9,23,24
Pathologic PD and CVD pathologies showed relatively separate associations with the rate of progressive parkinsonian signs, but together only accounted for a minority (<15%) of the variance of the progression of parkinsonian signs (Supplementary Table 5).
Progression of parkinsonian signs in Group2 with and without pathologic PD
Pathologic PD was rare in adults without clinical PD [Group1(17/357, 5%) and Group2 (92/1,307, 7%)]. Hence, it was much more common for decedents in Group2 (parkinsonism never clinical PD) to show one or more CVD pathologies (928/12,74, 73%) without pathologic PD (Fig. 3).
On the other hand, decedents in Group3 (clinical PD) who commonly showed pathologic PD (33/52, 63%), frequently showed accumulation of one or more CVD pathologies (Supplementary Figures 3 and 4b). Since, both pathologic PD and CVD pathologies show separate effects with the rate of progression of parkinsonian signs (Table 2; Supplementary Table 5) this suggests that the faster rate of progression of parkinsonian signs in Group3 might be due to the presence of both pathologic PD and CVD pathologies.
These data led us to try to identify two subgroups within Group2 based on the presence or absence of pathologic PD whose trajectories of progression of parkinsonian signs might vary. We stratified the Group2 into two subgroups: Group2a (No pathologic PD) and Group2b (Yes pathologic PD). We then compared the rate of progression of parkinsonian signs in the four clinical groups [Group1 (reference group), Group2a (No pathologic PD), Group2b (Yes pathologic PD) and Group3] using a mixed-effect model. The reference Group1 showed the slowest rate of progression of parkinsonian signs as compared to the other three clinical groups (Table 3,Model A).
Progression of parkinsonian signs in no parkinsonism, parkinsonism with and without PD pathology and clinical PD
Few decedents with parkinsonism accumulate PD pathology and most decedents with parkinsonism accumulate one of more CVD pathologies. So, we stratified the Group2 (parkinsonism without clinical PD into two groups: Group2a (parkinsonism without PD pathology) and Group2b (parkinsonism with PD pathology). This table summarizes a mixed effect model comparing the rates of progression of these four clinical groups. Each of the three columns summarizes the rates of progression using a different reference group as shown in each column. Model A-C compared the rate of progression for the four groups head-to-head using a different group as the reference for each model. These data suggest that as hypothesized the Group2b (parkinsonism with PD pathology) shows a faster rate of progression of parkinsonian signs as compared to (Groups1&2a) and is indistinguishable from the rate of progression in Group3 (clinical PD) [Model C]. Moreover, the more common group of adults with parkinsonism without PD pathology (Group2a) shows an intermediate rate of progression between adults without parkinsonism (Group1) and adults with parkinsonism with PD pathology (Group2b Model B). Each model also included demographic terms alone and their interaction with TBD which are not shown.
Group2a (No pathologic PD) show faster progression of parkinsonian signs than Group1, but slower progression compared to Group2b (Yes pathologic PD) and Group3 (Table 3, Model B). Group2b (Yes pathologic PD) showed a faster rate of progressive parkinsonian signs compared with Group2a (No pathologic PD) and their rate of progression of parkinsonian signs was indistinguishable from Group3 (Table 3, Model C).
DISCUSSION
The nature and nosology of pathologic PD, parkinsonism, and clinical PD remains unclear, because the clinical correlates of pathologic PD in older persons without a clinical diagnosis of PD are not well-characterized. Until recently the correlates of pathologic AD and cognition in older adults were also unknown. Recognition of the heterogeneity of cognition associated with pathologic AD required the prospective cognitive assessment of large numbers of older adults undergoing autopsy without case selection based on postmortem findings. This approach led to the reconceptualization of pathologic AD as having an asymptomatic stage (NCI) followed by a MCI stage, with AD dementia being a late manifestation of the disease process. 25 Moreover, although mixed AD/ADRD brain pathologies are common in older adults, these cognitive stages are not distinctive for a specific underlying AD/ADRD brain pathology associated with AD dementia.
The current study leveraged the successful approach that led to the reclassification of pathologic AD and cognitive impairment to characterize the clinical heterogeneity of pathologic PD and parkinsonism in older adults. 25 We deployed the UPDRS to reliably measure parkinsonian signs annually and obtained autopsy in about 85% of decedents that measured both pathologic PD and eight other AD/ADRD pathologies. To avoid truncating the distribution of the clinical spectrum of parkinsonism associated with pathologic PD, we included all cases and did not exclude cases based on their postmortem findings.
Our results are consistent with the notion that clinical parkinsonism in older adults is best conceptualized as a continuum. As illustrated in Fig. 2, adults with parkinsonism but without clinical PD during the study (Group2) showed an intermediate rate of progression of parkinsonian signs compared with adults who never had either parkinsonism or clinical PD (Group1) and adults with clinical PD (Group3). These three clinical groups manifesting varied trajectories of progressive parkinsonian signs during later life are analogous to the cognitive categories of NCI, MCI, and dementia that are recognized as showing varied trajectories of cognitive decline during the protracted clinical course of AD dementia. 25
Pathologic PD was observed in all three clinical groups in the current study (Supplementary Figures 2 and 3). The group of adults with a clinical diagnosis of PD (Group3) in this study was much smaller than the other two categories and we did not quantify the burden of PD pathology, yet, the proportion of decedents with markers of pathologic PD in Group3 was more than 8-fold higher (Supplementary Figure 4b) and they showed the fastest rate of progressive parkinsonian signs compared to Groups 1&2 who never had a clinical diagnosis of PD (Fig. 2). Additionally, Group2 showed an intermediate rate of progression of parkinsonian signs compared to Groups1& 3, similar to the reconceptualization of MCI as an intermediate stage compared NCI and AD dementia.25,26, 25,26
Our data suggest that the clinical association of Lewy bodies with progressive parkinsonian signs was strongest in brains showing Lewy bodies together with moderate or severe nigral neuronal loss. Nonetheless, less severe postmortem findings that we termed “possible pathologic PD” including Lewy bodies alone or adults with Lewy bodies and mild nigral neuronal loss were associated with a faster rate of progressive parkinsonian signs compared to adults without either element (Supplementary Table 2). Yet, the association of pathologic PD with progressive parkinsonian signs was about 5x stronger than the association for possible pathologic PD (Supplementary Tables 3–5). Further work will be needed to determine if the heterogeneity of the accumulation of the elements included in possible pathologic PD, i.e., Lewy bodies alone or with only minimal nigral neuronal loss may be used to identify earlier stages of the accumulation of pathologic PD, i.e., preclinical or early prodromal stages.
There is strong genetic evidence that PD is a synucleinopathy with multiple genetic pathways via alpha synuclein (SNCA).21,27–29 , 21,27–29 Yet, it is possible that oligomeric forms of SNCA that do not form Lewy bodies are injuring neurons and could lead to clinical symptoms without neuronal loss. This study did not measure Lewy neurites, intracellular SNCA or image analysis of SNCA burden that may provide more sensitive markers for SNCA. This conceptualization underscores the importance of further studies to identify the early drivers of SNCA before cell loss to facilitate early treatments.30 –32
A novel aspect of the current study was that we collected not only indices of PD pathology but indices of eight additional AD/ADRD pathologies. Like adults with MCI and AD dementia who rarely show the accumulation of on pathologic AD, the majority of all three clinical groups showed mixed-brain pathologies. Yet, a closer review of the data showed that pathologic PD was uncommon in adults who never received a clinical diagnosis of PD (Groups1& 2) but was common in Group3. Pathologic PD was uncommon (7%) even in adults with parkinsonism (Group2) and more than 70% showed 1 or more CVD brain pathologies associated with progression of parkinsonian signs (Fig. 4).
The rate of progression of parkinsonian signs was faster in Group2b who accumulated pathologic PD compared to Group2a without pathologic PD. Moreover, the rate of progression for Group2b who accumulated pathologic PD was indistinguishable from the rate observed in adults in Group3 (Table 3). This suggests that parkinsonism in most (>70%) community-dwelling older adults is commonly related to the accumulation of one or more underlying CVD brain pathologies even in the absence of pathologic PD (Fig. 3b) and may be amenable to treatments to reduce CVD pathologies. 33 This may explain the large proportion of older adults >50% who have been reported to manifest clinical parkinsonism by age 85, while only, a small minority of older adults (<10%) with parkinsonism may harbor underlying pathologic PD and manifest prodromal PD. These results provide important insights into the nosology of parkinsonism and clinical PD in older adults and may inform on effort to develop a biological classification of PD.16 –18 Moreover, the heterogeneity of mixed-brain pathologies and parkinsonism highlights the potential utility of using serum or fluid biomarker to complement clinical findings to identify adults at risk for specific pathologies or molecular mechanisms.
As reported in our prior studies, mixed-brain pathologies accounted for a small minority (<15%) of the variance of progressive parkinsonian signs.10,34, 10,34 It is likely that the current study underestimated the variance accounted for by PD and CVD pathologies since this study only measured PD and CVD pathologies accumulating in predominantly cognitive regions of brain and limited locations in the upper brainstem and did not assess continuous measures for the burden of PD pathology. Recent work underscores that these both PD and CVD pathologies extend to many locations outside the cerebrum including lower brainstem, cerebellum, spinal cord and peripheral nervous system that may account for additional unexplained variance of progression of parkinsonian signs.35 –37 Additionally, the current study did not assess white mater integrity which may make a substantial contribution to motor phenotypes including parkinsonism in older adults especially given the association of white matter integrity with CVD pathologies. 32 Moreover, our recent work has identified molecular mechanisms in proteome-wide studies of cortical regions that may not manifest a “pathologic footprint” but may be associated with the rate of change of parkinsonian signs in older adults. 38 Further studies are needed to replicate our findings and to determine the full extent to which PD and CVD pathologies and other molecular mechanisms throughout distributed motor pathways may contribute to the progression of parkinsonism in old age.
There are several additional limitations to the current analyses. The clinical diagnosis of PD in these analyses was based on history and medical records and was not based on the clinical assessment by a movement disorder physician. However, even if the clinical diagnosis of PD was suboptimal, since we obtained postmortem indices on all individuals this would not have affected our main findings as the majority of adults developing clinical parkinsonism did not have evidence of pathologic PD and the majority of those with clinical PD showed markers of pathologic PD. The current study was underpowered to study PD and these data highlight the need for further studies to examine the inter-relationship of pathologic PD and other ADRD pathologies in adults with a clinical diagnosis of PD. Decedents in this study were almost all of European descent and better educated than the general population. So, our findings need to be replicated in the more diverse and general populations.
This study has several strengths. One important strength was that by using the same validated instrument to measure parkinsonian signs from prospectively collected data we were able to compare the trajectories of progressive parkinsonian signs in older community-dwelling older adults with and without parkinsonism and also those with and without a clinical diagnosis of PD. In addition, all decedents had a structured brain autopsy which included not only pathologic PD but eight other AD/ADRD brain pathologies allowing us to assess the heterogeneity of AD/ADRD pathologies underlying the progression of parkinsonian signs in old age.
AUTHOR CONTRIBUTIONS
Aron Buchman (Conceptualization; Data curation; Formal analysis; Funding acquisition; Methodology; Project administration; Writing – original draft); Lei S. Yu (Formal analysis; Writing – review & editing); Shahram Oveisgharan (Writing – review & editing); Andrea Zammit (Writing – review & editing); Tianhao Wang (Writing – review & editing); Joshua Shulman (Writing – review & editing); Veronique VanderHorst (Writing – review & editing); Sukrit Nag (Data curation; Writing – review & editing); David Bennett (Funding acquisition; Project administration; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We are deeply indebted to all participants who contributed their data and biospecimens. We are thankful to the staff in the Rush Alzheimer’s Disease Center.
FUNDING
This work was supported by National Institute of Health P30AG10161, R01AG17917, R01AG47976, R01AG56352, R01AG59732, R01AG22018; the Illinois Department of Public Health; and the Robert C. Borwell Endowment Fund. The funding organizations had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
All data included in these analyses are available via the Rush Alzheimer’s Disease Center Research Resource Sharing Hub, which can be found at www.radc.rush.edu. It has descriptions of the studies and available data. Any qualified investigator can create an account and submit requests for deidentified data.