
Abstract
BACKGROUND:
There are certain issues using saliva as a sample for steroid hormone analysis in clinical diagnostics. Therefore, it is important to test whether currently available assays are suitable for this approach in a routine laboratory.
OBJECTIVES:
The analytical performance of two commercially available immunoassays was compared under routine conditions. In addition, salivary steroid hormone levels were compared with serum levels.
METHODS:
Saliva and serum samples were collected from healthy subjects. Afterwards, the concentration of cortisol, testosterone, progesterone and estradiol in saliva was measured by using the ADIVA Centaur® XP platform and commercially available manual ELISA kits. Serum levels of the selected steroid hormones were determined by using the ADVIA Centaur® platform.
RESULTS:
Currently, the ADVIA Centaur® XP platform cannot be used for the quantification of steroid hormones in saliva due to an insufficient calibration range. Commercially available ELISA kits on the other side are well suitable for this application.
CONCLUSIONS:
There are commercially available immunoassays which are sensitive enough for the determination of steroid hormones from saliva and can be used under routine conditions. However, the interpretation of salivary steroid hormone levels stays a challenging task due to the large variability of the results.
Introduction
Saliva is a variable and complex fluid which is mainly produced by three pairs of salivary glands in the mouth, including the parotid, submandibular and sublingual gland [1]. Additionally, saliva contains variable amounts of gingival crevicular fluid, plasma exudates and sometimes also blood from oral abrasions or lesions [1]. Hormones can enter the saliva by a variety of different mechanisms [1]. For neutral steroids the most common way is rapid diffusion through the acinar cells [1]. Therefore, the concentration is not influenced by the saliva flow rate [1]. Other ways for steroids to enter saliva can be through blood or plasma via oral abrasions but also directly from food by contamination with exogenous steroids [1].
From a clinical point of view saliva would be a good sample specimen due to the attractiveness of non-invasive, repeated and simple stress-free sampling [1]. This is especially important in the field of pediatrics. Due to the easy way of sampling, saliva has emerged as a popular sampling fluid for psychobiology, sports medicine, pharmacology and pediatric studies but also in the field of complementary medicine [1]. Salivary progesterone and estradiol for example can be used for assessing the ovarian function [1]. Salivary cortisol is used for the investigation of the adrenal function and there is an application as a screening test for the Cushing‘s disease [1]. Last but not least the testosterone levels in saliva seem to correlate with psychological parameters and so it can be applied in psychobiological studies [1].
Beside the noninvasive way of sampling no special training or equipment is needed and the patients can conveniently collect saliva samples themselves [1]. It is also important that salivary steroid hormones can reflect the circulating levels of free steroid hormones rather than total circulating steroid levels, which are confounded by the presence of circulating high affinity binding proteins, such as sex hormone-binding globulin (SHBG) or albumin [1].
However, there are some problems regarding the use of saliva in clinical diagnostics. These problems concern the collection techniques, the variable matrix of saliva, the sensitivity of the assays, the stability of the analytes as well as the presence of binding proteins and some reference range anomalies [1]. Besides, the circadian rhythm of hormones makes the interpretation of the results quite difficult.
Regarding the collection technique it is important to use collection tubes which do not absorb steroid hormones over time (e.g. glass or polypropylene tubes) [2]. Only by using the right collection tubes the stability of the analytes can be guaranteed. Further, it is also important that no citric acid is used to stimulate saliva secretion because it can interfere with some assays [2]. The second major problem is the low concentration range of steroid hormones in saliva, making it quite difficult to develop a suitable assay.
For the analysis of steroid hormones in saliva mainly immunological methods and chromatographic methods (primarily liquid chromatography, coupled with mass spectrometric detection) are used [2].
Because of the wide variety of different problems, the aim of this work is to investigate whether two currently available immunoassays (Siemens ADIVIA Centaur® XP and IBL International Saliva ELISA kits) are suitable for the routine quantification of steroid hormones from saliva. For this purpose, the steroid hormones cortisol, testosterone, progesterone and estradiol were selected for investigation. In addition, further information about the ratio between salivary steroid hormone levels and serum levels should be collected.
Materials and methods
Sample set
Serum and saliva samples were collected from 14 male and 14 female subjects. In general, the mean age was 27.6 (18.8–61.8) years. In the male group the mean age was 26 (21.6 –53.7) years. On the other side in the female group the mean age was 29.3 (18.8–61.8) years. It is also important that in the female group 11 of the subjects used oral contraceptives (mainly combined preparation with ethinylestradiol and dienogest). The remaining three subjects did not use any hormone medication.
Ethics statement
All serum samples which were used in this study were waste from routine laboratory diagnostics. Therefore, there was no need for an ethic approval. The respective samples were originally collected for routine diagnostic purpose and no collection was done specifically for the purpose of this study. Further, the samples were anonymized prior to the use in this study and no medical or personal data of the subjects was recorded.
Saliva samples on the other side were collected only for the purpose of this study because saliva collection is a non-invasive sampling technique. To compare saliva and serum hormone levels it is essential to collect saliva samples together with serum samples. Therefore, no saliva samples from the routine reserve sample storage of the institute were used. Instead, the samples were collected from subjects shortly after the collection of a serum sample for routine diagnostic purpose. After sampling the saliva samples were anonymized and again no medical or personal data of the subjects was recorded. All subjects were informed about the purpose of this study and gave their informed consent.
Sample collection, preparation and storage
In order to compensate the circadian rhythm of the hormone levels and to get reproducible results all samples were collected at 11 o'clock in the morning.
The blood samples were collected by venipuncture using 7.5 ml tubes with clot activator (Sarstedt, Nümbrecht, Germany). After collection the blood samples were centrifuged at 3000 × g for 10 minutes. Finally, after the routine diagnostic tests were performed, the remaining serum was transferred into 5 ml polypropylene tubes (Kühnle GmbH, Karlsruhe, Germany) and stored at -18°C until analysis.
Saliva samples were collected in saliva collection tubes (IBL International GmbH, Hamburg, Germany). A drinking straw was used to enable an easier sampling process. Approximately 1 ml saliva was collected from every subject. After collection the samples were stored at -18°C. Prior to analysis the samples were centrifuged at 3000 × g for 10 minutes and only the supernatant was used for analysis. In a previous experiment, this has turned out to be the most suitable method for sampling and storing of saliva samples.
Analysis of steroid hormone levels by different immunoassays
For the detection of cortisol, testosterone, progesterone and estradiol from serum samples the ADVIA Centaur® XP platform (Siemens Healthcare Diagnostics GmbH, Erlangen, Germany) was used. The measurement principle is based on direct chemiluminescence and is validated for the use with serum samples. To see whether it works also with saliva, five saliva samples were measured by using this platform.
The detection of the steroid hormones mentioned above from saliva was done by using four commercially available ELISA kits (IBL International GmbH, Hamburg, Germany). These assays are validated by the manufacturer for the use with saliva samples.
Data analysis
Data analysis was performed by using the statistic software R [3]. To compare salivary hormone levels with serum levels a linear regression analysis was performed.
Results
For the performance evaluation of the commercial ELISA kits under routine conditions and to compare the results with the detected steroid hormone levels in serum 28 saliva samples were measured in total. Additionally, five saliva samples were measured by using the ADVIA Centaur® XP platform to see whether this system is also able to quantify steroid hormones in saliva.
By using this platform, a quantitative analysis of salivary steroid hormones was not possible. The results clearly indicate that none of the analytes was detectable in saliva by using this platform because all results are below the limit of quantification (Table 1).
Quantitative measurement of cortisol, testosterone, progesterone and estradiol from saliva by using the ADVIA Centaur® XP platform
Quantitative measurement of cortisol, testosterone, progesterone and estradiol from saliva by using the ADVIA Centaur® XP platform
[a] Subject number, [b] m = male, f = female.
However, by using the IBL ELISA kits it was possible to detect the steroid hormone levels in saliva.
At first the detected cortisol levels in saliva were compared with serum levels (Fig. 1). In saliva as well as in serum, a higher median concentration was observed in females compared with males.
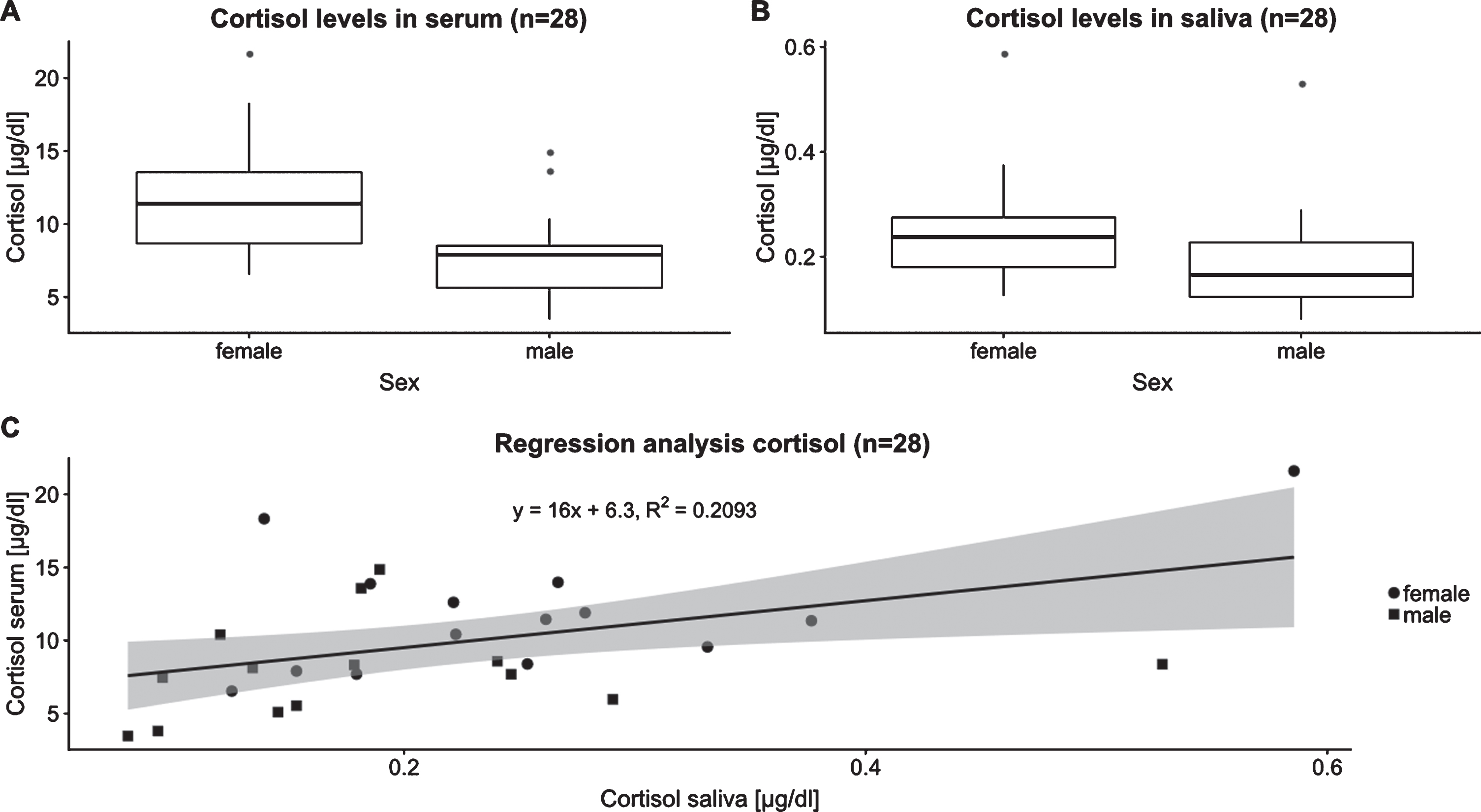
A) Cortisol levels in serum which were quantified in male and female subjects by using the ADVIA Centaur® XP platform. B) Cortisol levels in saliva which were detected in male and female subjects by using the IBL Saliva Cortisol ELISA kit. C) Linear regression analysis to compare salivary cortisol with cortisol levels in serum.
The cortisol levels in serum of male subjects range from 3.45μg/dl to 14.85μg/dl with a median of 7.9μg/dl (Fig. 1A). In female subjects the serum cortisol levels range from 6.53μg/dl to 21.59μg/dl. The median in this group is 11.39μg/dl (Fig. 1A). According to the literature the gender independent reference range for cortisol in the morning (7-10 o'clock) is 4 –22μg/dl [4].
Next, salivary cortisol levels in male subjects range from 0.08μg/dl to 0.53μg/dl and the median is 0.17μg/dl (Fig. 1B). In female subjects the concentration of cortisol in saliva ranges from 0.13μg/dl to 0.59μg/dl. The median is 0.24μg/dl (Fig. 1B). Here, according to the manufacturer of the ELISA kit the reference range is 0.083 –0.574μg/dl [5].
Finally, the linear regression analysis shows a coefficient of determination (R2) of 0.2 for the correlation between serum levels and saliva levels (Fig. 1C).
Regarding testosterone, obviously female subjects show lower concentrations compared with male subjects in saliva as well as in serum (Fig. 2).

A) Testosterone levels in serum which were quantified in male and female subjects by using the ADVIA Centaur® XP platform. B) Testosterone levels in saliva which were detected in male and female subjects by using the IBL Saliva Testosterone ELISA kit. C) Results of the linear regression analysis to compare salivary testosterone with testosterone levels in serum.
In male subjects the testosterone levels in serum range from 2.19 ng/ml to 5.46 ng/ml. The median is 3.84 ng/ml (Fig. 2A). Female subjects on the other side show testosterone levels in serum from 0.15 ng/ml to 0.81 ng/ml. Here, the median is 0.28 ng/ml (Fig. 2A). Of course, the reference range of testosterone is sex dependent. In serum, normally male subjects show concentrations of 3–9 ng/ml [4]. For female subjects a concentration of < 0.45 ng/ml is expected [4].
Finally, in saliva male subjects present a testosterone concentration ranging from 0.04 ng/ml to 0.131 ng/ml with a median at 0.078 ng/ml (Fig. 2B). The concentration of salivary testosterone in female subjects ranges from 0.005 ng/ml to 0.069 ng/ml and the median is 0.019 ng/ml (Fig. 2B). The reference range for salivary testosterone according to the manufacturer of the kit is 0.041–0.142 ng/ml for males and 0.005–0.049 ng/ml for females [6]. With higher age the reference range decreases [6].
Regarding the comparison between salivary and serum testosterone levels the result of the linear regression analysis shows an R2 of 0.5 (Fig. 2C).
Next, the progesterone levels in serum and in saliva are comparable between male and female subjects in our test group (Fig. 3).

A) Progesterone levels in serum which were quantified in male and female subjects by using the ADVIA Centaur® XP platform. B) Progesterone levels in saliva which were detected in male and female subjects by using the IBL Saliva Progesterone ELISA kit. C) Results of the linear regression analysis to compare salivary progesterone with progesterone in serum.
In male subjects the progesterone concentration in serum ranges from < 0.21 ng/ml to 0.85 ng/ml with a median at 0.45 ng/ml (Fig. 3A). For females on the other side the values are distributed from < 0.21 ng/ml to 2.48 ng/ml. The median in this group is 0.34 ng/ml (Fig. 3A). The reference range for males is 0.28–1.04 ng/ml and for females 0.2–25.2 ng/ml dependent on the menstrual cycle [7].
Regarding salivary progesterone the concentration in male subjects ranges from 0.018 ng/ml to 0.15 ng/ml. Here, the median is 0.05 ng/ml (Fig. 3B). In female subjects the salivary progesterone concentration ranges from 0.021 ng/ml to 0.165 ng/ml (Fig. 3B). The median is 0.03 ng/ml, respectively. Again, according to the manufacturer of the ELISA kit the reference range for males is < 0.051 ng/ml and for females it is dependent on the menstrual cycle 0.028–0.446 ng/ml [8]. The linear regression analysis shows an R2 of 0.03 for the correlation between salivary levels and serum levels (Fig. 3C).
Last but not least, the results from the quantification of estradiol in serum and saliva show that the levels are again comparable between males and females (Fig. 4).

A) Estradiol levels in serum which were quantified in male and female subjects by using the ADVIA Centaur® XP platform. B) Estradiol levels in saliva which were detected in male and female subjects by using the IBL Saliva Estradiol ELISA kit. C) Results of the linear regression analysis to compare salivary estradiol with estradiol levels in serum.
The estradiol concentration in serum of male subjects ranges from 24.98 pg/ml to 51.38 pg/ml. The median in this group is 37.56 pg/ml (Fig. 4A). In female subjects on the other side the serum concentration of estradiol ranges from 12.70 pg/ml to 128.56 pg/ml and the median is 40.45 pg/ml (Fig. 4A). According to the current literature the reference range for estradiol in serum is < 52 pg/ml for males and 11–526 pg/ml for females dependent on the menstrual cycle [7].
Salivary estradiol levels range in male subjects from 0.54 pg/ml to 3.55 pg/ml and the median is 1.52 pg/ml (Fig. 4B). In females the concentration ranges from 0.73 pg/ml to 11.91 pg/ml. Here, the median is 1.71 pg/ml (Fig. 4B). For salivary estradiol the reference range according to the manufacturer of the used ELISA kit is 0.6–3.1 pg/ml in males and 0.6–6.3 pg/ml in females [9].
Finally, the linear regression analysis for the comparison of serum and salivary estradiol levels presents an R2 of 0.54 (Fig. 4C).
The aim of this study was to test whether two commercially available immunoassays are suitable for the routine quantification of cortisol, testosterone, progesterone and estradiol from saliva samples.
The results clearly show that the ADVIA Centaur® XP platform, which is based on the direct chemiluminescence immunoassay principle, is currently not suitable for this application because the calibrated concentration range does not match to the concentration range of steroid hormones in saliva. As shown in Table 1 the concentration of the hormones in all saliva samples is below the limit of quantification of this system.
These results are not a surprise because until today the ADVIA Centaur® XP system is not validated for the quantification of steroid hormones in saliva and should only be used for serum samples. In the future maybe there will also be an application for saliva samples because in general the direct chemiluminescence immunoassay technique is sensitive enough to detected steroid hormones in saliva [10]. Further, an automated system would be a great approach because for the routine quantification of steroid hormones in saliva high throughput but also high reproducibility are needed. These requirements can be met by using automated analyzers.
As an alternative to the automated analyzer manual immunoassay kits were tested under routine conditions. The used ELISA tests are all based on the competitive principle.
The results show that nearly all salivary steroid hormone levels which were determined by using the respective ELISA kit (see Figs 1–4) are within the given reference ranges. This value distribution was expected because all test subjects were healthy individuals. However, there are some outliers in each of the four hormone groups which do not fit in the given reference ranges. An explanation for this observation might be the distinct circadian rhythm of steroid hormones. Especially progesterone and estradiol in females are strongly varying over the menstrual cycle [11]. Due to this strong variation of steroid hormone levels it is possible that some of the measured values are outside the reference range. Normally, the best approach in this case is to draw a second sample at another day in order to control borderline test result.
Interestingly, in the current study population female subjects show higher levels of cortisol compared with male subjects in both saliva and serum. Larson et al. made a comparable observation [12]. In their study 1811 men and women in an age group from 30 to 75 years were randomly selected from a Swedish population and salivary cortisol was assessed [12]. The results of this study show that the morning cortisol levels at eight o'clock are significantly higher in women than in men [12]. Additionally, Larson et al. observed a significant association between increasing age and increasing cortisol levels [12].
In the current study, progesterone and estradiol showed comparable levels between men and women (Fig. 3 and Fig. 4). This is probably due to the problem that 79%of the female subjects use oral contraceptives. Oral contraceptives decrease the progesterone and estradiol levels and alter the cycle pattern of a normal menstrual cycle [13]. Therefore, comparable progesterone and estradiol levels might be observed between men and women taking oral contraceptives. As a conclusion for further studies it would be important to include also women without oral contraceptive drugs in the study population. On the other side from an analytical point of view the results indicate that there should be no relevant cross reactivities of the detection antibodies used in the ELISA tests with synthetic steroids such as ethinylestradiol or dienogest.
In a systematic review by Zimmerman et al. it is mentioned that the circulating levels of total testosterone and free testosterone also decrease during the use of combined oral contraceptives [14]. These drugs inhibit the ovarian and adrenal androgen synthesis and also increase the levels of SHBG [14]. In the present study a comparison between women with and without oral contraceptives was not possible because the study population is too small and most female subjects used oral contraceptives. Thus, there is no control group for comparison.
Regarding analytical methods, another technique which is well suitable for the quantification of steroid hormones in saliva is liquid chromatography coupled to mass spectrometry [2]. In general, mass spectrometry is a highly specific analytical method, which can overcome problems of immunoassays such as possible cross reactions [2]. Further, this technique enables the screening of a complete profile of steroids in one sample in a short amount of time [2]. Although this technique has some major advantages, suitable instruments are quite expensive at the moment. Therefore, the application for salivary hormone quantification is not widespread but this might change in the future.
In addition to the evaluation of the immunoassays under routine conditions, the results of the current study were used to compare salivary steroid hormone levels with serum levels using linear regression analysis (Figs 1–4). The results present a positive correlation for cortisol (R2 = 0.2), testosterone (R2 = 0.54) and for estradiol (R2 = 0.54). Progesterone shows a small negative correlation (R2 = 0.03). The results indicate that the concentration of cortisol, testosterone and estradiol in saliva seems to increase with an increasing concentration of the serum levels. However, it is important to consider a possible influence of oral contraceptives on the results of progesterone, estradiol and testosterone in women. Due to this problem the results might be biased. In general, the selected steroid hormones are released into the blood stream in both their inactive form (bound to carrier proteins) and the biologically active free fraction [15]. The free fraction of the steroid hormones can migrate through the salivary gland membrane, while the carrier-protein bound fraction cannot pass through this membrane [15]. Therefore, it is reasonable that with increasing total hormone concentration in serum the concentration of the free hormone fraction in saliva also increases.
Finally, the results of the linear regression analyses show that the connection between salivary levels and serum levels is not totally linear and there are also variations within the four tested hormones. To get even better statistically significant results it might be important to investigate this question in a much larger study population. Also, a possible influence on the ratio between salivary and serum concentrations by oral contraceptives must be considered especially for progesterone and estradiol.
Conclusion
Summarized, the results indicate that commercially available, validated immunoassays are suitable for the quantification of steroid hormones in human saliva. This can be seen from the distribution of the measured values from healthy subjects compared with the given reference ranges. For further evaluation, we took also part in a proficiency testing scheme (also including pathological concentrations) but the results were not yet available when this article was written.
The limitation of this study clearly is the small study population and the high number of female subjects taking oral contraceptives. Further, the results have shown that the interpretation of salivary steroid hormone profiles is quite challenging and salivary levels do not represent directly the serum concentrations. Therefore, it is important that the determination of steroid hormones from serum samples still stays the gold standard. Salivary steroid hormone levels can primarily be used in combination with serum levels or if there is a clear indication for using them on their own.
Conflict of interest
The authors declare no conflicts of interest.