
Abstract
BACKGROUND:
Vascular resistance, and therefore blood pressure (BP), depends on vascular and rheological factors. Microrheological characteristics of red blood cells (RBCs) can affect blood viscosity (BV) and thus be included in the pathogenesis of increased blood pressure in arterial hypertension (AH). Signaling molecules such as gasotransmitters (NO, CO and H2S) regulate vascular tone and RBC microrheological characteristics and thus affect blood pressure and tissue perfusion.
OBJECTIVE:
It was evaluated the changes in the macro- and microrheological characteristics of blood and red blood cells (RBCs) under arterial hypertension in persons with and without COVID-19, as well as the protective effect of NO and H2S donors on the RBC microrheological properties.
METHODS:
Hemorheological profile parameters were recorded in group 1 individuals (n = 18, 9 women and 9 men) without a history of COVID-19; group 2 (n = 16; 11 females and 5 males), hypertensive patients who had COVID-19. As a control, there was a group of healthy individuals (group 3 n = 22). In experiments with red blood cells (RBCs) and their recovered ghosts (filled with an isotonic solution of known viscosity), deformability (RBCD) and aggregation (RBCA) were recorded after incubation of cells with sodium nitroprusside (SNP, 100μM) and sodium hydrosulfide (NaHS, 100μM).
RESULTS:
In patients with AH in both groups, the main parameters of the hemorheological profile were negatively changed, including a decrease in RBCD and an increase in BV, plasma viscosity (PV) and RBCA. SNP and NaHS significantly increased deformability and reduced their aggregation (p < 0.01). However, in healthy individuals, microrheological responses to GT donors (100μM) were more pronounced than in patients with AH, especially in the AH+COVID-19 group (p < 0.05).
CONCLUSION:
Both gasotransmitter donors (NO and H2S) have a positive effect on the RBC microrheological characteristics in healthy and sick individuals. However in hypertensive patients, especially those who had COVID-19, microrheological responses to GT donors were significantly lower. Therefore, on the model of red cell microrheological responses, as on a test object, it is possible to determine the decrease in the sensitivity of cells and tissues to the regulatory action of gasotransmitters.
Introduction
Analysis of the Poiseuille equation shows that volume blood flow depends on vascular, rheological and hemodynamic factors [1, 2]. Therefore vascular resistance and, consequently, blood pressure (BP) are significantly affected by the rheological properties of blood [3], and what is especially important, the red blood cell (RBC) microrheological characteristics correlate with the values of systolic (SBP) and diastolic blood pressure (DBP) [4–7]. It was shown that red blood cell aggregation (RBCA) positively correlated with the severity of arterial hypertension (AH), and their deformability (RBCD) –negatively. Thus blood viscosity alterations mediated by changes in RBCA and RBCD can affect the magnitude of blood pressure and cause microcirculatory disorders [8, 9]. At the level of microcirculation, the RBC microrheological properties have a significant impact on tissue perfusion [10–13]. At the same time, it is important to keep in mind that such biophysical characteristics of these cells as deformability and aggregation change under the influence of signaling molecules [14]. Hydrogen sulfide and nitric oxide are now recognized as important regulators in the cardiovascular system [15–17]. In this regard, the question arises whether these regulatory molecules can prevent the negative effect of mediators of the sympathoadrenal system and are there any violations of this protective effect of gasotransmitters (GT) in pathological conditions? It has been shown that a deficit in the NO/H2S homeostasis is involved in the pathogenesis of various cardiovascular diseases, especially arterial hypertension and diabetes mellitus [18, 19]. This deficiency can be determined on the model of RBC microrheological responses, when they are incubated with standardized concentrations of GT donors, by comparison with control samples without the addition of these active compounds [20]. The aim of the study was to evaluate the changes in the macro- and microrheological characteristics of blood and red blood cells (RBCs) under arterial hypertension in persons with and without COVID-19, as well as the protective effect of NO and H2S donors on the RBC microrheological properties.
Materials and methods
Patients and study design
From the total mass of the examined patients (n = 34; aged 42 to 73 years) with arterial hypertension (AH), two groups were distinguished: group 1 (n = 18, 9 women and 9 men) without a history of COVID-19; group 2 (n = 16; 11 females and 5 males), hypertensive patients who had COVID-19 within six months prior to this study. All patients were diagnosed with grade II AH with mean BP of 103.7±7.1 mm Hg. At the same time, systolic pressure (SAP) was from 134 to 186 mm Hg, and diastolic (DAP) from 80 to 106 mm Hg. As a control, there was a group of healthy individuals (group 3), corresponding in sex and age to the first group (n = 22, 12 women and 10 men). In this group, SAP averaged 122.4±7.6 mm Hg, while DAP was 73.3±4.9 mm Hg. The use of human blood was in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). The study was approved by the local ethical committee of the university (protocol No. 6 dated June 16, 2022) and informed consent was obtained from all study participants. Blood samples were obtained by venipuncture into EDTA vacutainers. RBCs were separated from plasma by centrifugation (15 min, 3000 rpm), washed three times in isotonic NaCl solution, and resuspended in Ringer’s solution.
Hemorheological measurements
Hemorheological profile parameters were recorded: blood viscosity at high (>100 s–1, BV1) and low shear rates (<20 s–1, BV2), plasma viscosity (PV), RBC suspension viscosity (SV) at hematocrit (Hct) 40% and the constant viscosity of the suspension medium (viscosity –1.56 mPa×s), using a rotational viscometer (Brookfield DV2TLV, USA). The hematocrit index was determined on an Elmi SM-70 hematocrit centrifuge (Latvia). The hemorheological efficiency of oxygen transport was assessed by the ratio of hematocrit/viscosity (Hct/BV1) [21, 22]. The red blood cell aggregation (RBCA) was determined using Myrenne M1 aggregometer (Germany). To assess red blood cell deformability (RBCD), the cell elongation index (EI) was recorded in a flow microchamber [20].
Registration of RBC microrheological responses to gastransmitter donors
To study the red blood cell sensitivity to gasotransmitters (GT) in in vitro experiments, their suspension was divided into 3 aliquots and the cells were incubated at 37°C for 30 min with each of the following compounds: NO donor - sodium nitroproprusside (SNP, 100μM); H2S donor, sodium hydrosulfide (NaHS, 100μM); Only in Ringer’s solution (without any compounds) –control samples.
For a more accurate analysis of the influence of gasotransmitters on the molecular RBC targets located in the structure of their plasma membranes, suspensions of their recovered ghosts were prepared. This was done according to the Dodge method [23]. RBCs were destroyed by osmotic shock. To do this, 7 ml of chilled distilled water (at 4°C) was added to 1 ml of cells, followed by washing twice in phosphate buffer. Then the ghosts concentrate was incubated in Ringer’s solution with the addition of 30% dextran-200 (the ratio of buffer and dextran was 7: 3 by volume). The suspension of RBC ghosts was divided into three aliquots and then they were incubated with SNP and NaHS. After incubation for 30 min at 37°C, their deformability (EI2 index in the figures) was recorded in a flow microchamber [20].
The effectiveness of GT donors in three different groups was assessed by microrheological responses –RBCD and RBCA changes. RBC suspension was incubated the same way (duration and temperature) but in a drug-free buffer solution was used as a control sample. All compounds were purchased from Sigma-Aldrich (USA). They were dissolved in distilled water or DMSO. Preliminary experiments with incubation of RBCs in isotonic Ringer’s solution containing DMSO did not reveal significant differences in RBCD and RBCA compared to control samples (without DMSO).
Statistics and data presentation
Statistical processing included obtaining the mean (M) and standard deviation (SD). The sampling distribution was tested using the Shapiro-Wilk test. Nonparametric statistics of the program Statistica 10.0 (StatSoft Inc., USA) was used. When conducting paired comparisons of indicators within groups during repeated measurements, the Wilcoxon test was used. Differences at p < 0.05 and p < 0.01 were taken as statistically significant. The data correlation hypothesis was tested using Pearson’s correlation coefficients.
Results
Change in hemorheological profile parameters in hypertensive patients with and without COVID-19
The main rheological characteristics of blood and RBC microrheology in patients differed significantly from the values of healthy individuals (Fig. 1).

Relative differences (in %) of the hemorheological profile parameters in hypertensive patients (groups 1 and 2) compared to healthy individuals (group 3 as control group) data represented as null line. Note: BV1 –blood viscosity at high shear rate (300 c-1); BV2 –blood viscosity at low shear rate (3 c-1); PV –plasma viscosity; SV –red blood cell suspension viscosity; RBCD –red blood cell deformability; RBCA –red blood cell aggregation; Hct/BV1 ratio –an index of blood transport efficiency.
The parameters of the hemorheological profile in persons of groups 1 and 2 differed by an average of 22–34% from the data of the group 3. At the same time, RBCA changed most significantly, its value in groups 1 and 2 exceeded the value of the control group by 50 and 57% (p < 0.01), respectively. A noticeable increase in RBC suspension viscosity was found, up to 11% (p < 0.05, Fig. 1) in hypertensive patients, compared with the data of the healthy individuals (group 3). Together with a significant decrease in RBC elongation index (p < 0.05), this indicated a negative change in the RBCD in hypertensive patients. It should be noted that blood viscosity in patients with AH and, consequently, its transport potential, significantly depends on the RBC deformability. This was indicated by a rather high correlation between blood viscosity and RBC suspension viscosity (r = 0.75, p < 0.01), as well as a negative correlation between blood viscosity and RBC elongation index (r = –0.58, p < 0.05).
It is known that RBC microrheological characteristics including their deformability and aggregation are critical for tissue microvascular perfusion [24–26] and can be positively corrected by the action of gasotransmitters (GT) [27, 28]. However, the availability of these signaling molecules and the sensitivity of target cells can be negatively altered under arterial hypertension [19]. This can be investigated in models of red blood cell microrheological responses to GT donors.
The red blood cell (RBC) microrheological responses to SNP averaged 17% in the group of healthy individuals. Under these conditions, the deformability of native RBCs and their recovered ghosts increased by 8 and 9%, respectively (Fig. 2a). As for aggregation, it was reduced by 34%. NaHS slightly more changed the RBC microrheological characteristics in the group of healthy individuals (on the average by 19%), than after RBC treatment with SNP. So RBCD of intact cells was increased by 9%, their ghosts by 11% (p < 0.01) and aggregation was reduced by 39% (p < 0.01, Fig. 2b).
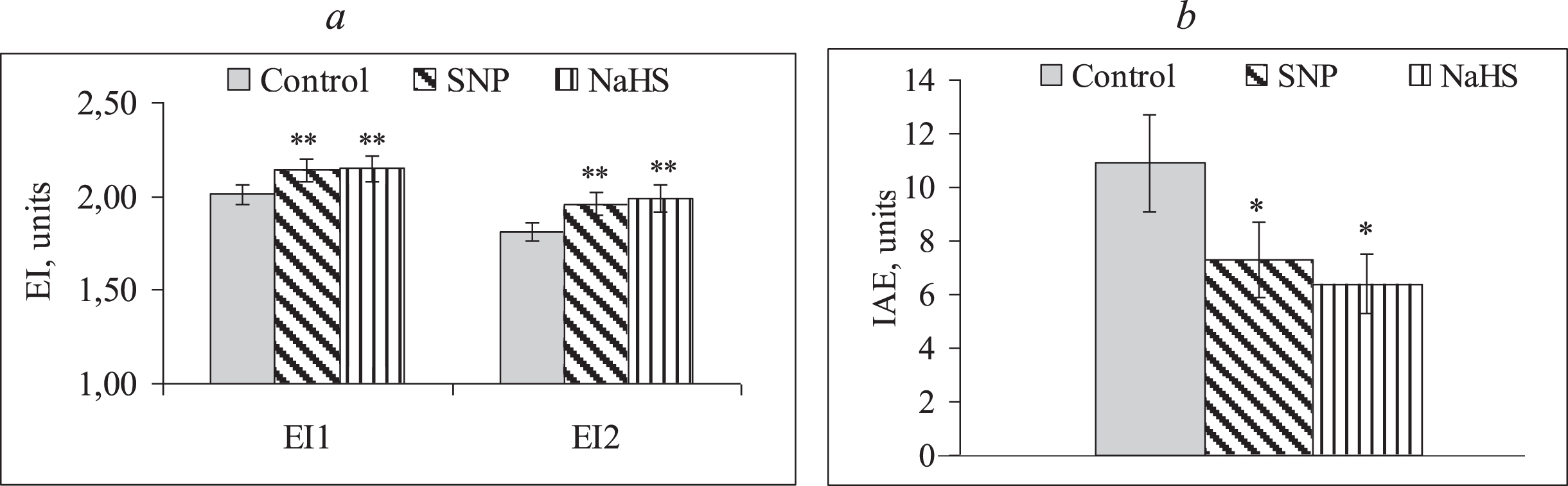
Changes in red blood cell deformability, their ghosts (a) and red blood cell aggregation (b) under the influence of sodium nitroprusside and hydrogen hydrosulfide in healthy individuals. Note: SNP –sodium nitroprusside; NaHS –hydrogen hydrosulfide; EI1 –elongation index of intact red blood cells; EI2 –elongation index of red blood cell recovered ghosts; IAE –index of red blood cell aggregation; *p < 0.05, vs. control; **p < 0.01, vs. control.
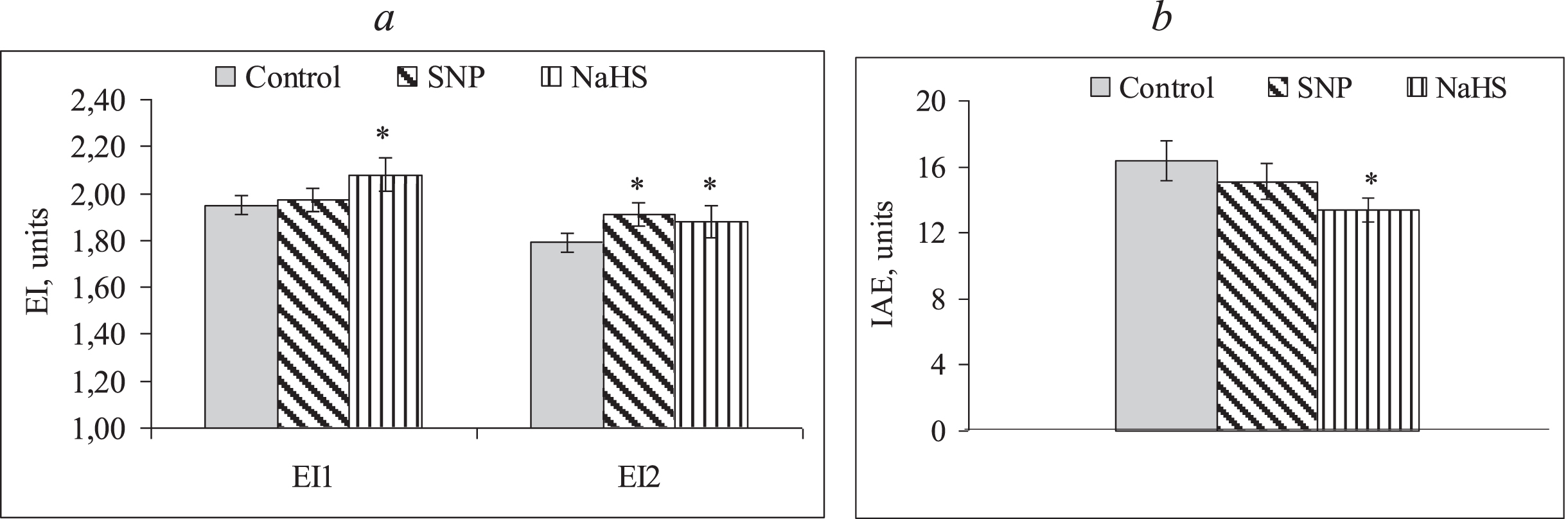
In patients with arterial hypertension without COVID-19, the microrheological responses of RBCs to SNP were significantly less and averaged 7.6% for three characteristics (healthy individuals - 17%). The intact RBCs and their ghosts increased their deformability only by 4.6 and 4.2% (Fig. 3a; p < 0.05), respectively, after incubation with SNP. The RBC aggregation reduction was 14% (p < 0.01, Fig. 3b).

Changes in intact red blood cell deformability, their ghosts (a) and red blood cell aggregation (b) under the influence of sodium nitroprusside and hydrogen hydrosulfide in hypertensive patients without COVID-19. Note: SNP –sodium nitroprusside; NaHS –hydrogen hydrosulfide; EI1 –elongation index of intact red blood cells; EI2 –elongation index of red blood cell recovered ghosts; IAE –index of red blood cell aggregation; *p < 0.05, vs. control; **p < 0.01, vs. control.
Sodium hydrosulfide in group 1 elicited somewhat greater RBC microrheological responses than SNP. The increase in RBC deformability of intact cells and their ghosts was 6% (p < 0.01), and RBCA reduction was 20% (p < 0.05, Fig. 3b). On average, for all three characteristics, the change under the influence of NaHS was about 11%.
Patients with AH+COVID-19 showed the lowest RBC microrheological responses to GT donors. After RBC incubation with SNP, the deformability of intact cells and their ghosts were increased only slightly, by 3–5% (Fig. 4a), respectively. As for RBCA, its decrease by 8% was not significant (Fig. 4b). The mean value of changes in the three RBC microrheological characteristics was only 5.3%, which was significantly less than in the other two groups.
Changes in red blood cell deformability, their ghosts (a) and red blood cell aggregation (b) under the influence of sodium nitroprusside and hydrogen hydrosulfide in hypertensive patients with COVID-19. Note: SNP –sodium nitroprusside; NaHS –hydrogen hydrosulfide; EI1 –elongation index of intact red blood cells; EI2 –elongation index of red blood cell recovered ghosts; IAE –index of red blood cell aggregation; *p < 0.05, vs. control; **p < 0.01, vs. control.
After incubation with NaHS, the average microrheological response (for three characteristics) was 9%. This markedly exceeded the RBC response to incubation with SNP, which was 5.3% in patients of this group only. An increase in the deformability of intact RBCs and their ghosts was by 5% (p < 0.05, Fig. 4a), and a reduction in RBCA was by 13% (p < 0.05, Fig. 4b).
The integral blood rheological characteristic, its viscosity was markedly increased in patients with AH in both groups (groups 1 and 2) compared to healthy individuals. It is known that viscosity depends on a complex of factors, including plasma viscosity, hematocrit, RBC aggregation, their deformability and also the shear conditions [26]. Therefore, in order to determine changes in this complex of blood rheological characteristics, the concept of hemorheological profile can be applied [22]. Its analysis in patients with AH and AH+COVID-19 showed that a higher BV in them was accompanied by increased plasma viscosity. Significant correlation between BV1 and PV was found (r = 0.71, p < 0.01). While in healthy individuals this relationship was less pronounced (r = 0.53, p < 0.05). It is important to note that in persons with AH + COVID-19, a significant negative correlation of viscosity (BV1) and RBCD (r = –0.58, p < 0.05) was found, while in the control group it was only –0.43. Thus, it can be assumed that the decreased RBCD in patients with AH made a significant contribution to the increase in blood viscosity. Moreover, this RBC microrheological characteristic was significantly reduced compared to healthy individuals. The question arises: could this be affected by the reduced sensitivity of the cells of sick individuals to gasotransmitters (NO, H2S), since the positive effects of GT on the RBC microrheological properties are known [28, 29]. This assumption was tested on models of RBC microrheological responses and their recovered ghosts to gasotransmitter donors. Both of these GTs have a vasodilating effect in the circulatory system [28, 30] and also had a positive impact on the RBC microrheological characteristics [28, 31].
It is known that under conditions of pathology, the bioavailability of gasotransmitters may decrease [18, 32]. The obtained data indicate that microrheological responses to dosed concentrations of GT donors were significantly lower in both groups of AH patients than in healthy controls. For the latter the increase in the elongation index of RBC under the influence of SNP was 0.16±0.01 units. Whereas in individuals with AH, the change in EI was 0.11±0.03 units, and the difference with the data of healthy individuals was significant (p = 0.01, Fig. 5a).

Mean values of differences in microrheological responses (RBCD and RBCA) to SNP in patients with AH and AH+COVID-19 compared with those in the healthy individuals (Control is group 3). Note: Data are presented as median (Me) [Q25:Q75].
Also, the decrease in RBC aggregation in response to SNP in groups of patients with hypertension was significantly less than in healthy individuals. The average value of the decrease in the RBCA index under the influence of SNP in healthy individuals was 3.45±0.62 units, while in groups 1 and 2 it was only 1.48±0.53 and 1.59±0.44 units, respectively (p < 0.05). This decrease in the RBC sensitivity to the action of the NO donor in hypertensive patients may be due to impaired signal transduction in the sGC-cGMP-PKG molecular cascade due to oxidative stress based on increased production of superoxide [33].
In addition, in AH, an increased level of angiotensin II leads to a decrease in the expression of sGC [34], as the main molecular target of NO action in cells, including RBCs [35]. Therefore, reduced RBC microrheological responses to the NO donor in hypertensive patients may be evidence of a functional insufficiency of sGC as the first element of the NO-mediated signaling pathway. On the other hand, stimulation of sGC is known to lead to an increase in cGMP concentration [36]. The latter can inhibit the entry of Ca2 + into RBCs which is accompanied by a decrease in their aggregation [14, 37].
Microrheological responses to the H2S donor were similar in magnitude and direction of changes in RBC deformability and aggregation to those observed under the influence of SNP, and in groups 1 and 2 were significantly lower than in healthy individuals. Thus, the difference in the increase in RBCD under the influence of NaHS was 0.090±0.002 units in group 1 and 0.110±0.006 units in group 2, which was significantly less than in healthy individuals (0.172±0.008 units, p < 0.05; Fig. 6). The aggregation response of RBCs in AH patients was also less pronounced to the standard donor dose (NaHS, 100μM) than in the control group (p < 0.01).

Mean values of differences in microrheological responses (RBCD and RBCA) to NaHS in patients with AH and AH+COVID-19 compared with those in the healthy individuals (Control is group 3). Note: Data are presented as median (Me) [Q25:Q75].
ATP-dependent K+ channels (KATP) are considered as a molecular target in cells for H2S [38]. However, it was previously shown that blocking them with glibenclamide does not eliminate the increase in RBC deformability under the influence of NaHS [28]. In addition it is known that hydrogen sulfide has the ability to increase the level of cGMP [39]. To do this, GT must first activate the guanylate cyclase. In doing so, the actions of H2S and NO converge at cGMP; though hydrogen sulfide does not directly activate sGC, it maintains a tonic inhibitory effect on phosphodiesterase 5, thereby delaying the degradation of cGMP [40]. It is quite possible, NO and H2S are mutually required for the physiological control of microrheological responses of red blood cells. Since it is known that changes in microcirculation and blood fluidity in patients with AH are systemic [41] then correction of the identified disorders of RBC microrheology by GT donors could have the potential to reveal therapeutic targets. To solve this problem, it is necessary to study the entire signal cascade associated with positive RBC microrheological changes under the influence of various GT donors, including the phosphorylation status of the cytoskeleton, accompanied by an improvement in RBC deformability [42].
Taken together the results of the study allow us to conclude that in persons with arterial hypertension, increased blood viscosity and, consequently, its reduced transport potential is negatively correlated with RBC deformability. At the same time, gasotransmitter donors (NO and H2S) have a positive effect on the RBC microrheological characteristics in healthy and sick individuals. However, in hypertensive patients, especially those who had COVID-19, microrheological responses to GT donors were significantly lower. Therefore, on the model of RBC microrheological responses, as on a test object, it is possible to determine the alteration in the sensitivity of cells and tissues to the regulatory action of gasotransmitters.
Abbreviations
soluble guanylate cyclase cyclic guanylate monophsphate protein kinase G nitrogen oxide hydrogen sulfide sodium nitroprusside sodium hydrosulfide red blood cell deformability red blood cell aggregation
Footnotes
Acknowledgments
This work was supported by the Russian Science Foundation (Grant No. 22-15-00120) and performed according to the Development program of the Interdisciplinary Scientific and Educational School of Lomonosov Moscow State University < <Photonic and Quantum technologies. Digital medicine> >.
Author contributions
AV Muravyov and AV Priezzhev, supervised the experimental study design, interpretation and wrote the article.
IA Tikhomirova included the patients and conducted the experiments.
PV Mikhailov included the patients, conducted the experiments and performed the data analysis.
AE Lugovtsov worked on the study design and interpretation performed the data analysis.
Conflicts of interest
There is no potential conflict of interest, real or perceived by the authors.