
Abstract

Introduction
Total knee arthroplasty (TKA) is an effective procedural cure for arthritis with more than 1.4 million surgeries performed worldwide [16]. Commonly used implant materials are titanium and cobalt alloys. Moreover, two types of tibial implants viz; a metal-backed modular tray (MBT) and an all-polyethylene (APE) type can be used based on surgical needs. However, both the above type of implants has its own advantages and drawbacks. APE systems have primarily three benefits in comparison with the MBT systems. First, it reduces the risk of osteolysis due to the elimination of metal-insert interface and reduce backside wear [13, 18, 20]. Second, it reduces the surgical cost up to 50% [6, 7, 8, 9]. Lastly, patients with allergy to metal components can be advised for APE systems [11]. Modularity, usage of stems, ease of removal during revision surgery are some of the advantages of MBT systems. Furthermore, many studies have also reported reduced compressive stresses in the periprosthetic region under the base plate leads to a more uniform load distribution in the proximal tibia [1, 10, 19].
Cemented TKA has shown excellent long-term survivorship among various available implant designs [23]. However, aseptic loosening and osteolysis is a common multi-factored failure phenomenon in cemented TKA. Adequate fixation and surface preparation enhance the long-term stability of the implant system. End-of-stem pain is the most common phenomenon in patients undergoing TKA, with cemented implants reporting 9% incidence among successful TKR. However, these incidences have been considerably reduced by using a polyethylene tip at the end of the tibial tray [24]. Fixation strength, tibial component backside wear and undesired levels of micromotion between the implant-bone interface are said to be the primary factors affecting the long term survival of TKR [3, 14, 17, 22]. Reliable fixation depends largely on the type of cementation technique and cement depth. Ideal bone in-growth post TKR have been reported in several studies wherein implant-bone micromotions are in the range of 20–50
Elastic modulus mismatch between the tibial implant and the surrounding bone stock results in accelerated bone resorption and stress shielding. Further, it leads to periprosthetic bone density loss and aseptic loosening in both primary and revision TKA. Reducing the implant stiffness by means of a lower moduli implant material or using an all-polyethylene implant systems have been shown to significantly reduce stress shielding and corresponding bone loss and failure [4, 12, 21].
In the current investigation, we have considered two types of implant material, a metal-backed modular tibial tray (MBT) and an all-polyethylene (APE) implant system and analyzed the effect of implant material on the micromotions at the bone-implant surface during level walking condition, with axial loading.
Materials and methods
Bone-implant model acquisition and reconstruction
The TKA prosthesis used for current study is a commercially available posterior stabilized type implant system, DePuy SIGMA (DePuy Orthopedics, Warsaw, IN, USA). The 3D geometries of implant components were scanned using a 3D scanner (Geomagic Capture, 3D systems, USA) and reverse engineered using Geomagic Design
(a) Isometric view. (b) front view. (c) exploded view of bone-implant assembly.
Bone and implant components were imported in Hypermesh (Hyper works, Altair University,) and initial surface meshing was done for all components with an element size ranging from 0.3 mm–1.5 mm. The element size of different surfaces was chosen, considering the master-slave contact surface relation of the solver and desired precision in results at critical areas of bone-implant system. Triangular surface meshes were converted to volume mesh using tetrahedral C3D10 and C3D4 element type for implant system and bone respectively. Mesh quality check and optimizations were performed considering: Jacobian 0.8–1, skew angle of less than 40
Material properties and boundary conditions
Linear elastic and isotropic properties were assumed for implant components and cement mantle layer. The material properties used in present study are listed in below:
Meshed bone was imported to MIMICS (Materialise, Leuven, Belgium) and calibrated with CT images for assigning its heterogenous properties. Fifteen different sections were considered for property assignment. The correlations between Hounsfield units and bone apparent density (g/cm
And subsequently for corresponding Young’s modulus in MPa are:
The range of Young’s modulus values obtained from Eqs (3) and (4) is from 48 MPa to 14.8 GPa, which is inside the typical scope of bone properties in the knee.
The interface between polyethylene insert -titanium tray, cement mantle layer- titanium tray and bone-cement were assumed to be fully bonded, as per available literatures and other similar studies carried out. The lower part of full tibia bone was fully fixed by constraining all its D.O.F.
For each set of simulation, MB and AP components were separately considered. Properties of titanium and polyethylene was considered for MB and AP implant components respectively, for the tibial tray and the screw. Neutral position of implantation was considered for all arrangements, wherein, neutral position alludes to a tibial level cut made at 0
Comparison of micromotion (Cslip) along 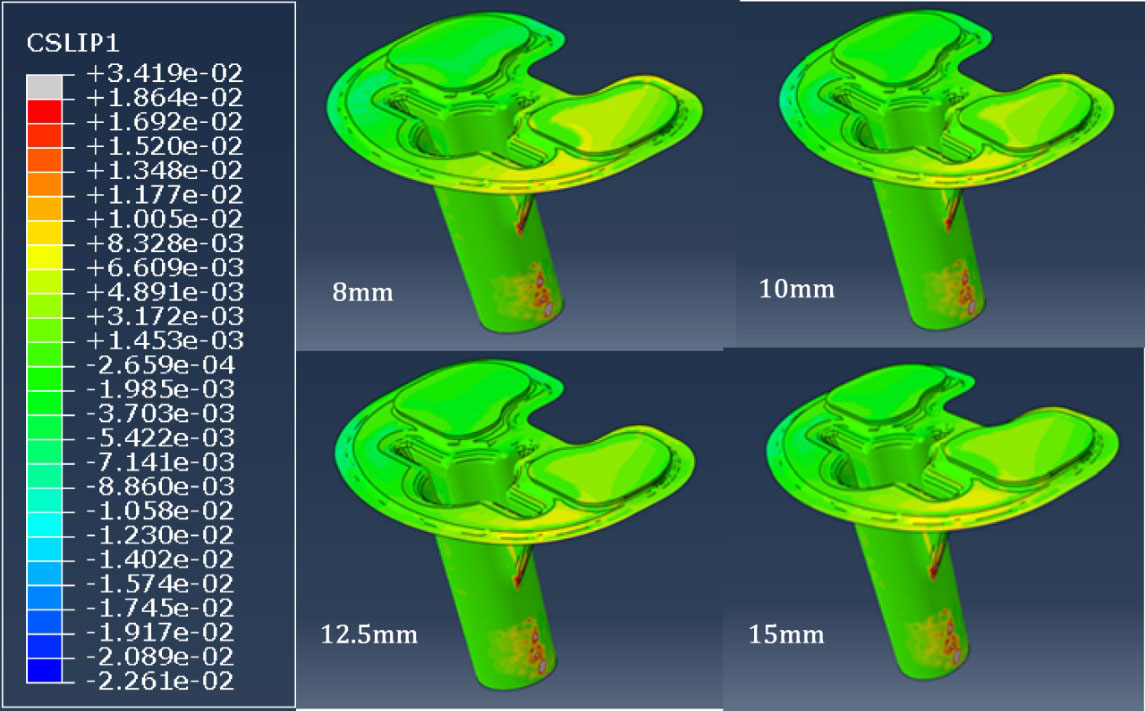
Maximum axial compressive loads of 3360 N, 4108 N and 4261 N during level walking, stair ascending, and stair descending activity respectively were considered, for a high body weight of 100 Kg [34]. The ratio of axial forces was assigned as 50:50 and 55:45 on medial and lateral surfaces of polyethylene insert for level walking and stair ascending and descending respectively [10,35,36]. The non-implanted and implanted tibial models, consisting of C3D10 elements in implant components and C3D4 type of element in bone with about 19,00,000 elements, with sizes ranging from 0.5–2.0 mm, were entered to Abaqus 6.14 (Dassault Systems, USA) for numerical analysis.
The results for all the cases are taken at the location wherein aseptic loosening initiates, i.e the surface surrounding the bone-implant conjunction. This surface along with the tibial surface accounts for 92% of early implant failures due to loosening.
Figures 2 and 3 depict the comparisons in micromotion (in
Comparison of maximum principal strains generated in the bone for different poly thicknesses.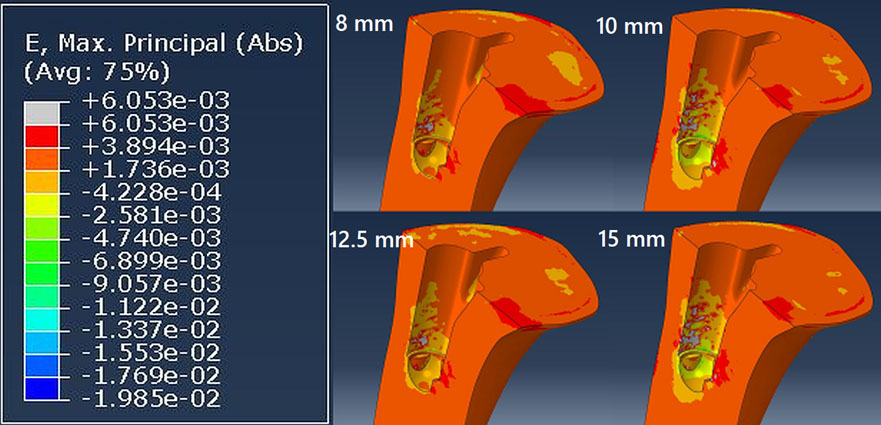
Relationship between micromotions (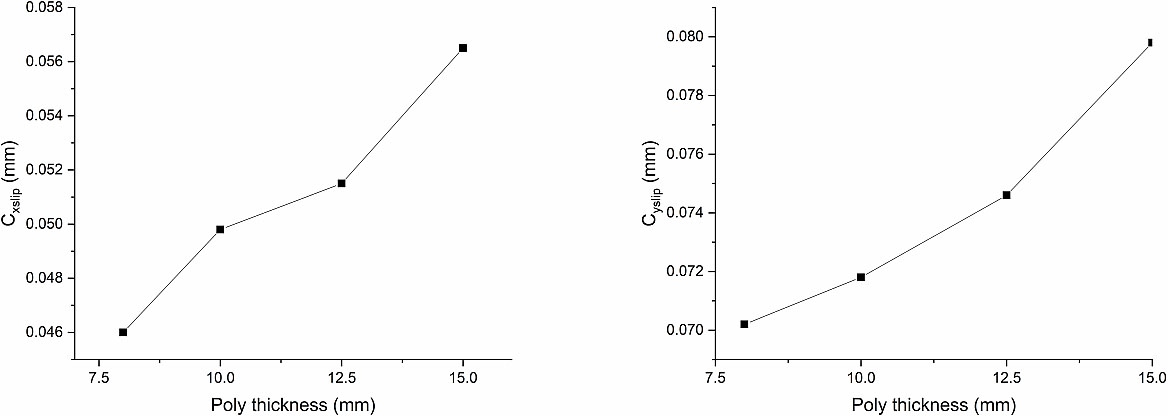
Relationship between micromotions (
Figures 4 and 5 above, depict the variations in micromotions (
MBT shows highest total micromotion (110
Limitations
There are a few limitations in the current numerical investigation. The full-bone tibial FE model developed in the current study was based on the CT images of a healthy male person, aged 35 years, thus the validation of the model was not attempted. Despite this, the trends of obtained results were reasonable with other similar studies considering 100–150 mm of tibia bone. The current assessment was based on just a single subject-specific model. The articular ligament and menisci were not considered for analyses in the intact tibia, where the contact forces on the condyles in an ordinary knee joint will not be the same as that of an implanted knee. The static examinations were completed assuming normal axial joint contact forces during typical walking and stair ascending and descending while the impacts of physiological dynamic load cases were not considered.